
Abstract
Introduction:
Different stress radiographs exist to diagnose dynamic scapholunate instability. Using a semi-automated stress CT-based measurement method, we compared the different imaging techniques in unstable wrists and in controls.
Methods:
Scapholunate distance (SLD) was measured on radiographs with and without stress of both wrists of 22 participants without instability (group A) and 21 patients with one symptomatic unstable wrist (group B). All wrists also underwent a CT scan without and with stress to measure CT-SLD and radioscaphoid distance (CT-RSD).
Results:
In both groups, the SLD was greater in the clenched fist plus ulnar deviation views (median 2.2 mm (IQR 1.8 to 2.4) in group A and 2.5 mm (IQR 2.2 to 2.8) in group B) than in clenched fist views alone (median 1.9 mm (IQR 1.7 to 2.2) in group A and 2.2 mm (IQR 2.0 to 2.4) in group B). The SLD was greater in symptomatic unstable wrists than in stable wrists under all stress radiographs. In both groups, no statistically significant differences were measured between both sides during stress radiographs and CTs. The unloaded CT-SLD was greater in symptomatic unstable wrists (median 15 mm (IQR 12 to 17)) than in stable wrists (median 13 mm (IQR 12 to 15)). Under stress, the CT-RSD was greater in symptomatic unstable wrists (median 10 mm (IQR 8 to 13) than in stable wrists (median 6 mm (IQR 5 to 7).
Conclusion:
Adding ulnar deviation to clenched-fist views along with stress CT may help to detect dynamic scapholunate instability.
Level of evidence:
III
Keywords
Introduction
Scapholunate instability typically presents with dorsoradial wrist pain and results in functional impairment. Dynamic scapholunate instability is defined as a condition where the abnormal movement or separation between the scaphoid and lunate becomes evident only during specific movements or manipulations, such as wrist motion or stress. Physical examination often reveals tenderness over the radiocarpal joint and a positive Watson scaphoid shift test (Kitay and Wolfe, 2012; Watson and Ballet, 1984). When treatment is required, the instability should ideally be addressed in the dynamic stage, before a non-reducible malalignment and secondary arthritic changes occur (Bain and Amarasooriya, 2023). Although there is currently no consensus on the optimal detection method, increase in scapholunate distance (SLD) and dorsal scaphoid translation (DST) are usually measured to confirm dynamic scapholunate instability (Bain and Amarasooriya, 2023). Different radiological stress views have been described, including the clenched fist view (Kitay and Wolfe, 2012), pencil grip view (Lawand and Foulkes, 2003) and bilateral ulnar deviation supination stress (BUDS) view (Puig de la Bellacasa et al., 2022). All of the tests aim to assess the increase in SLD during wrist loading. Dorsal scaphoid translation, dorsal radioscaphoid translational alignment or the increase in radioscaphoid distance (RSD), are usually assessed on lateral radiographs or computed tomography (CT) (Gondim Teixeira et al., 2022; Vutescu et al., 2020).
This study compared SLD with different radiographic stress views in individuals with and without dynamic scapholunate instability. All participants also had a CT scan of the wrist in neutral position without loading and a CT scan of the same wrist under BUDS stress conditions. The first aim of the study was to determine which stress radiographs induced the greatest scapholunate widening, and the second aim was to determine whether a CT under BUDS stress conditions revealed an increase in SLD and RSD.
Materials and methods
Study subjects and physical examination
The study was registered as NCT06695260 on clinicaltrials.gov, and ethical approval was obtained from the local ethics committee. Informed consent was provided by all participants. Two groups were evaluated. Participants for both groups were simultaneously recruited by the first author at his institution between January and October 2025. Group A consisted of volunteers without scapholunate instability; none had experienced symptoms of scapholunate instability, and none had a positive Watson scaphoid shift test on either wrist. Group B included patients with a clinical diagnosis of symptomatic dynamic scapholunate instability on one wrist, which was defined as a positive Watson scaphoid shift test with painful clunk (Watson and Ballet, 1984). Other inclusion criteria for group B were patients who presented at the consultation with daily functional problems in their wrist consisting of dorsoradial wrist pain for at least 3 months, especially at the level of the scapholunate joint, exacerbated during activity or axial loading and a sensation of instability or clunking during wrist loading. Pain was assessed with a visual analogue scale (VAS) from 0 to 10, with 0 no pain and 10 the worst imaginable pain. Exclusion criteria for both groups included individuals under 18 years old, those with osteoarthritis, a history of previous wrist disorders or wrist surgery and patients with dynamic scapholunate instability defined as an SLD greater than 2.5 mm on a standard posteroanterior (PA) wrist radiograph (Dornberger et al., 2015, Oh et al., 2025).
Medical imaging modalities
The following radiographic views were obtained of both wrists to measure the SLD: a PA unloaded view with the forearm in pronation, a PA clenched fist view with the forearm in pronation, a PA clenched fist view plus ulnar deviation with the forearm in pronation, and an anteroposterior (AP) clenched fist view plus ulnar deviation with the forearm in supination (BUDS view) (Figures 1 and 2). The SLD on plain radiographs was measured as the distance between the adjacent articular surfaces of the scaphoid and lunate at the midpoint between Gilula’s lines. All measurements were done with the digital tools in the IMPAX 6 viewer (Agfa-Gevaert, Mortsel, Belgium). The radiographs and CT scans were anonymized by the first author to exclude observer bias. A fellowship-trained hand surgeon (CKG, observer 1) measured the distances twice with a 3 month interval to assess the intra-rater reliability. An orthopaedic trainee (AVR, observer 2) measured the distances once to assess the inter-rater reliability.
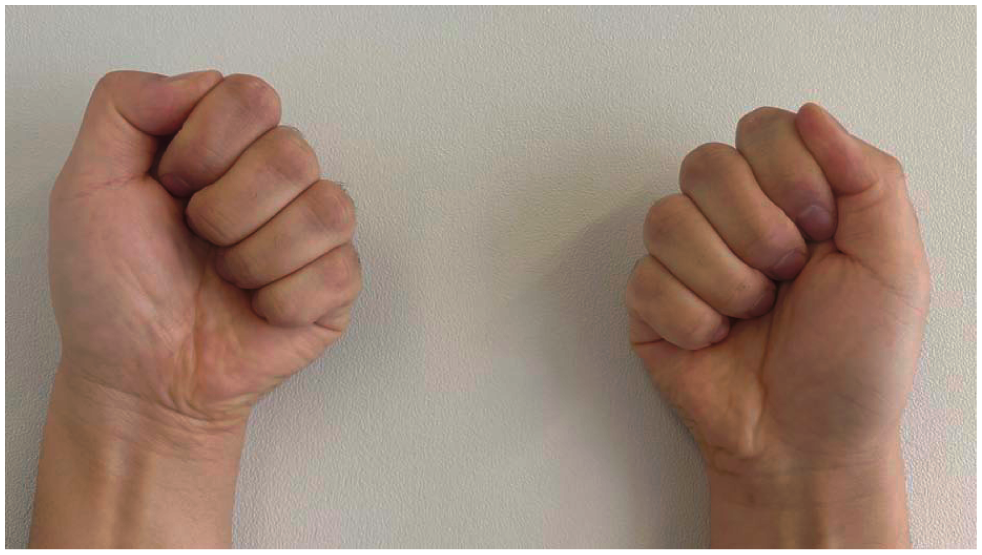
Wrists positioned in clenched fist, ulnar deviation and supination (bilateral ulnar deviation supination or BUDS position).
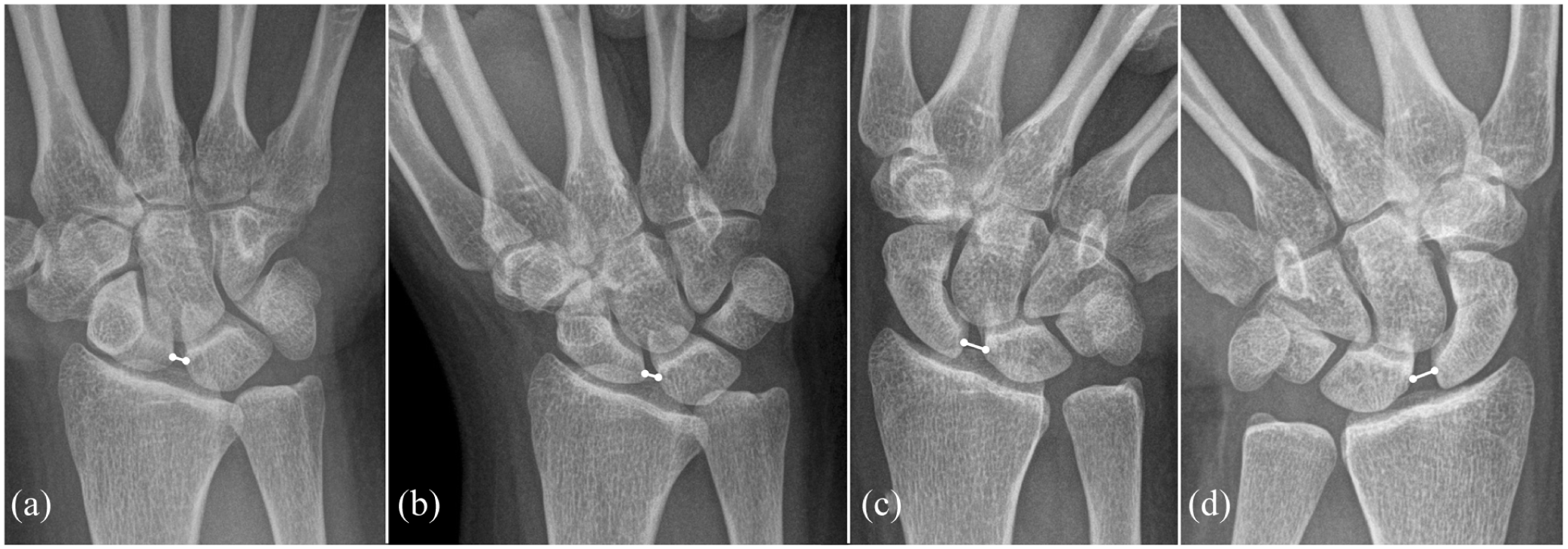
Measurement of the scapholunate distance (white line) on radiographs of a wrist with symptomatic scapholunate instability. (a) Posteroanterior (PA) view in pronation, (b) PA clenched fist view in pronation, (c) PA clenched fist view plus ulnar deviation plus pronation and (d) anteroposterior clenched fist view plus ulnar deviation plus supination.
First an unloaded CT scan of both wrists was taken with the forearms in full pronation, and then a stress CT was performed with the forearms in supination, the wrists in ulnar deviation and fists clenched (BUDS view). Semi-automated segmentation of the radius, lunate and scaphoid of the CT datasets was done. Details are presented in the supplementary document online (S1). The landmark of the scaphoid and lunate was the intersection of their longitudinal axis with their radiocarpal articular surface. The landmark of the radius was the intersection of the longitudinal axis of the radius with the distal articular surface of the radius (Figure 3). The CT-SLD was defined as the straight-line distance between the scaphoid and the lunate landmark and the CT-RSD was defined as the straight-line distance between the radius and the scaphoid landmark. This automated pipeline was defined for the first time by the first and second author and used to ensure consistency to identify identical landmarks for measurement across subjects and loading conditions. All measurements of the anonymized subjects were performed by an engineer experienced in musculoskeletal analysis (BK).
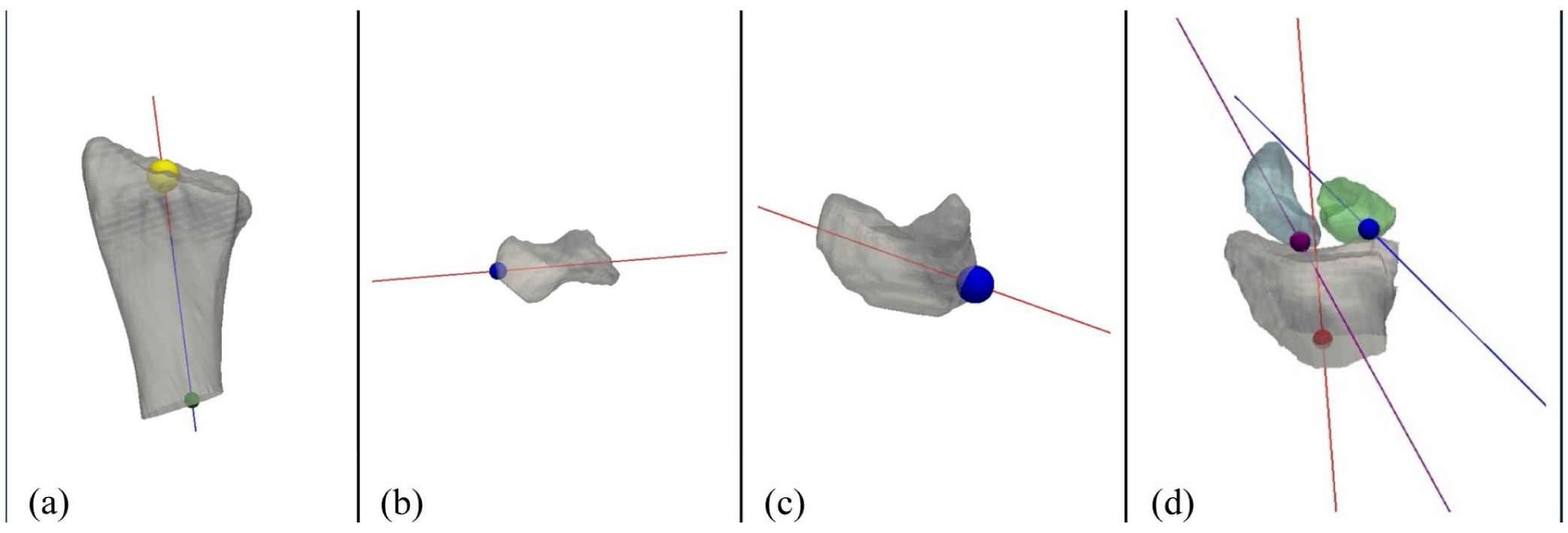
Three-dimensional reconstruction images with landmarks used for distance measurements. (a) The landmark of the radius (yellow dot): the intersection of the longitudinal axis of the radius with the radiocarpal articular surface of the radius. (b) The landmark of the scaphoid (blue dot): intersection of the longitudinal axis of the scaphoid with the radiocarpal articular surface of the scaphoid. (c) The landmark of the lunate: intersection of the longitudinal axis of the lunate with the radiocarpal articular surface of the lunate (blue dot). (d) The landmarks of the scaphoid (purple dot), lunate (blue dot) and radius (red dot) with their longitudinal axes.
Statistical analysis
For continuous variables, the Shapiro–Wilk test was used to assess normal distribution. Since variables did not follow a normal distribution, they were described as median and interquartile range (IQR) values. Outcomes of related samples were compared with a Wilcoxon signed-rank test: right vs. left wrist in group A and symptomatic unstable vs. contralateral wrists in group B. The Mann–Whitney U-test was used for non-related samples: age of group A vs. B and symptomatic wrists of group B with all stable wrists of group A. The Kruskal–Wallis test and the post-hoc Dunn’s test were used when more than two related groups were compared. This consisted of all types of loaded radiographs when compared with unloaded radiographs in the left and right wrists of group A and symptomatic unstable and contralateral wrists of group B. Male/female ratios in both groups were compared with a Pearson chi-squared-test. The significance level was set at p < 0.05 when the two groups were compared. Inter- and intra-rater consistency and absolute agreement were assessed by calculating the intraclass correlation coefficient (ICC) and their 95% confident interval (95% CI) based on a two-way mixed model (Koo and Li, 2016).
Results
Patient demographics
Group A consisted of 22 volunteers, with a median age of 38 years (IQR 31 to 54) and male/female ratio 8/14. Group B consisted of 21 patients with unilateral symptomatic instability (median VAS for pain 5 (IQR 6 to 8)), with a median age of 45 years (IQR 34 to 60) and a male/female ratio of 12/9. There were no statistically significant differences in age (p = 0.16) and male/female ratio (p = 0.16).
Radiographic analysis
Outcomes of SLD measurements are presented in Table 1. When comparing both wrists in the same participant, no statistically significant difference was present in median SLD on any of the radiographic incidences in group A or B. All wrists in both groups showed a statistically significant increase in median SLD when PA radiographs were taken with a clenched fist and even more when ulnar deviation and ulnar deviation with supination (BUDS view) were added (Figure 4). The post-hoc test revealed that median SLD increased in all types of loaded radiographs when compared with unloaded radiographs in the left and right wrists of group A (p < 0.001) and the symptomatic unstable and contralateral wrists of group B (p < 0.001). The SLD was significantly wider on the unloaded PA and the stress radiographs in the symptomatic unstable wrists of group B when compared with all wrists of group A.
Scapholunate distances measured on different radiographic wrist views of patients without (group A) and with dynamic scapholunate instability (group B).
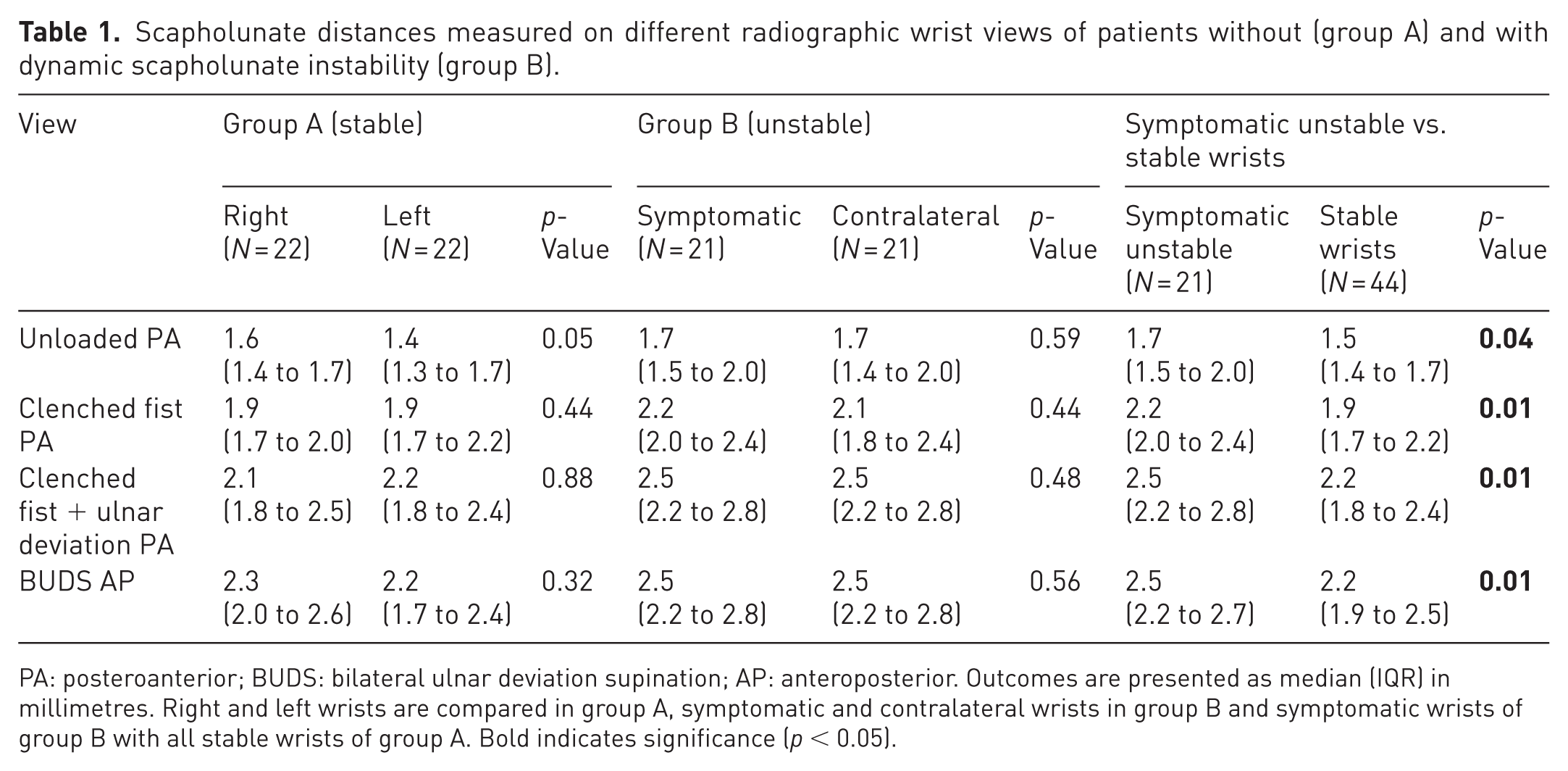
PA: posteroanterior; BUDS: bilateral ulnar deviation supination; AP: anteroposterior. Outcomes are presented as median (IQR) in millimetres. Right and left wrists are compared in group A, symptomatic and contralateral wrists in group B and symptomatic wrists of group B with all stable wrists of group A. Bold indicates significance (p< 0.05).
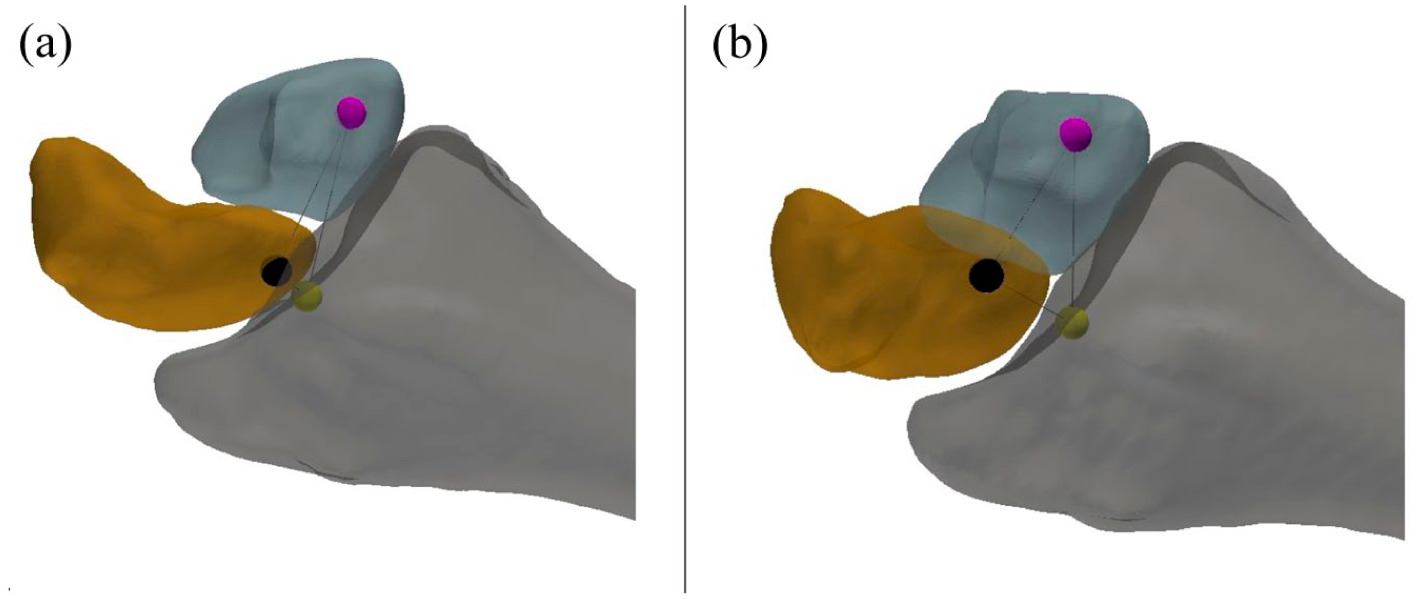
Three-dimensional reconstruction of radius, lunate and scaphoid in the coronal plane of a patient with scapholunate instability. (a) Unloaded CT and (b) stress CT. The black dot represents the scaphoid landmark, the purple dot the lunate landmark and the yellow dot the radius landmark. The scapholunate distance (CT-SLD) is the straight-line distance between the scaphoid and the lunate landmark. Minimal variation in CT-SLD is present between the unloaded and the stress CT.
The inter-rater reliability had an ICC of 0.75 (95% confidence interval 0.69 to 0.80) for the SLD measurements on the four PA and AP views. The intra-rater reliability had an ICC of 0.88 (95% CI 0.82 to 0.94) for the SLD measurements on the four PA and AP views.
Stress CT analysis
The outcomes of measurements with CT are presented in Table 2. When comparing both wrists, in group A as well as in group B, no significant differences were found in CT-SLD or CT-RSD on the unloaded or stress CT. When comparing the symptomatic unstable wrists of group B with all wrists of group A, the CT-SLD was significantly increased in group B on unloaded CT but not on stress CT. As illustrative example, Figure 3 demonstrates minimal variation in CT-SLD between the unloaded CT and the stress CT in a patient with scapholunate instability. In contrast, CT-RSD was not significantly different on unloaded CT, but it was significantly greater in the symptomatic unstable wrists than in stable wrists on stress CT. As illustrative example, Figure 5 demonstrates an increase in CT-RSD when comparing the stress CT with the unloaded CT in a patient with symptomatic scapholunate instability.
Scapholunate distance between scaphoid and lunate landmarks (CT-SLD) and radioscaphoid distance between radius and scaphoid landmarks (CT-RSD) on unloaded and stress CT of both wrists of patients without (group A) and with (group B) dynamic scapholunate instability.
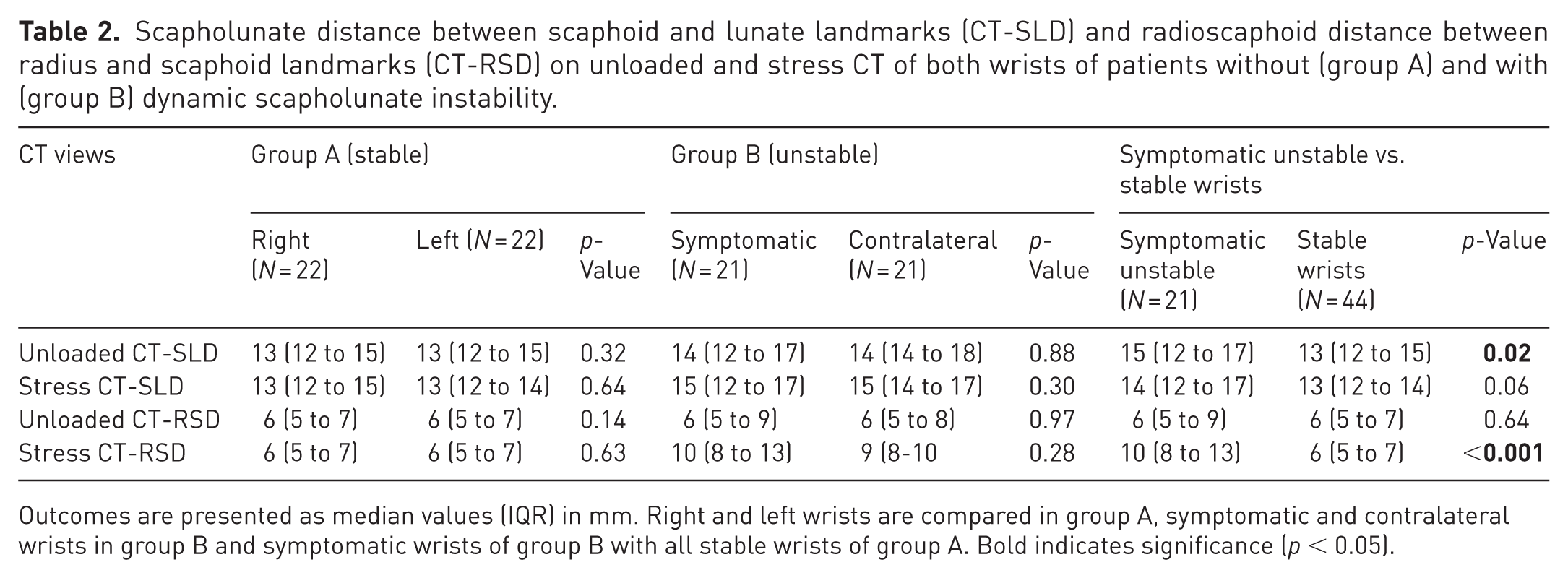
Outcomes are presented as median values (IQR) in mm. Right and left wrists are compared in group A, symptomatic and contralateral wrists in group B and symptomatic wrists of group B with all stable wrists of group A. Bold indicates significance (p < 0.05).
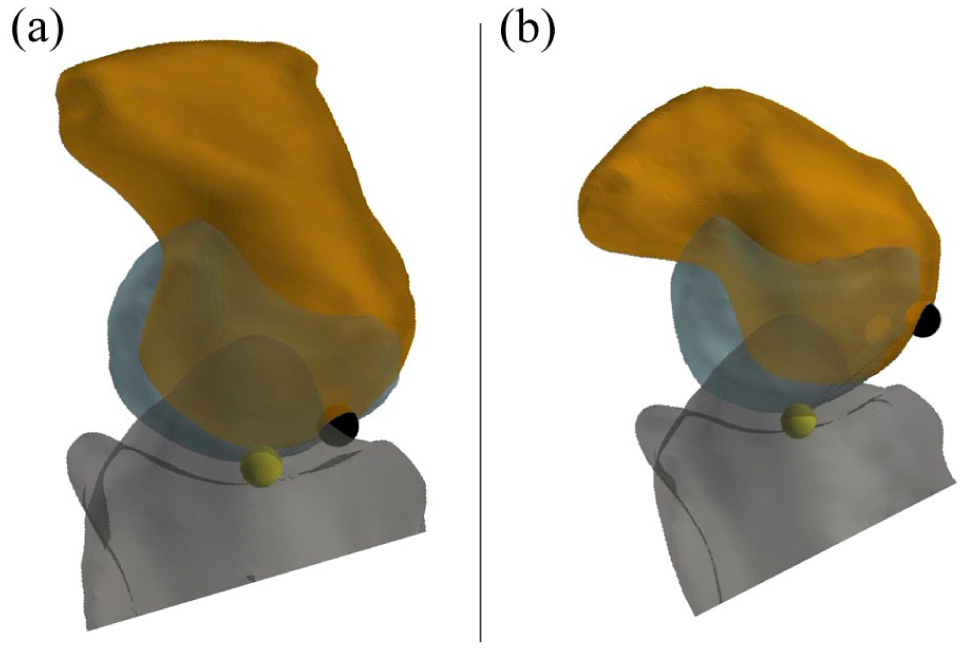
Three-dimensional reconstruction of the radius, lunate and scaphoid in the lateral plane of a patient with symptomatic scapholunate instability. (a) Unloaded CT and (b) stress CT. The black dot represents the scaphoid landmark, purple dot the lunate landmark and the yellow dot the radius landmark. The radioscaphoid distance (CT-RSD) is the straight-line distance between the scaphoid and the radius landmark. An increase in CT-RSD is present when comparing the stress with unloaded CT.
Discussion
This study revealed that median SLD was greater in radiographs with clenched fist plus ulnar deviation than in clenched fist radiographs without ulnar deviation in both symptomatic and asymptomatic volunteers. The median SLD was also greater in patients with dynamic instability compared with healthy individuals on all radiographic views. The CT-SLD on unloaded CT and CT-RSD on stress CT were greater in wrists with dynamic instability.
Conventional radiographs lack the ability to assess carpal bone motion during movements (Sulkers et al., 2014). Several stress radiographs have been described. (Kitay and Wolfe, 2012; Lawand and Foulkes, 2003; Puig de la Bellacasa et al., 2022). However, it has not been clear which stress views are best to diagnose carpal instability. Lee et al. (2011) compared different radiological views in a cadaveric model with nine wrists and found that the clenched fist in 30° ulnar deviation resulted in the greatest increase in SLD. The median SLD in 30° ulnar deviation was 4.7 mm, while the median SLD in 10° ulnar deviation was 3.6 mm and 2.1 mm in neutral position. This cadaveric finding was not completely confirmed in our clinical study since the differences were less than 1 mm although statistical significance was observed. Nevertheless, there is no consensus on how much widening between scaphoid and lunate is indicative of instability and whether the focus should be on absolute SLD measurement or on an increase in SLD between provocative and neutral radiographs. Our study focused on absolute SLD measurements. Authors have reported wide variation among normal individuals, and different thresholds have been published ranging from 2 to 4 mm (Dornberger et al., 2015; Kani et al., 2016). Moreover, wide scapholunate gaps can are present bilaterally in about 7% of individuals, and this can be asymptomatic. The evolution from stable wrist to carpal instability and cartilage degeneration does not necessarily happen simultaneously in both wrists (Hollevoet, 2019). As such, it is crucial to compare a clinically and radiologically symptomatic wrist with the contralateral side.
Biomechanical studies have demonstrated that the extensor carpi ulnaris muscle (ECU) increases pronation of the scaphoid, widens the scapholunate gap and plays a major role in destabilizing scapholunate-ligament-deficient wrists. In supination, the scaphoid pronation effect of the ECU tendon is maximal owing to resisted isometric contraction of the ECU muscle (Esplugas et al., 2016; Salva-Coll et al., 2011). Increased scaphoid pronation also maximizes the RSD or dorsal translation of the scaphoid in relation to the radius, which has been quantified by assessing the radioscaphoid angle or the RSD measured on lateral radiograph, CT or MRI (Gondim Teixeira et al., 2022; Meister et al., 2017; Vutescu et al., 2020). The BUDS position in supination was selected for our CT-based study, owing to its capacity to induce more RSD than in pronation. During provocative stress positions, alignment of the carpal bones is altered and an increase in RSD under stress is difficult to assess with conventional radiographs owing to superposition of the carpal bones on lateral radiographs. This can be solved by reconstructions of CT scan images in the lateral plane (Amarasooriya et al., 2025; Gondim Teixeira et al., 2022). Gondim Teixeira et al. (2022) demonstrated with 4-D CT that RSD increases proportionally with scapholunate instability but varied only 10% during radioulnar deviation. To avoid the use of 4-D CT technique, Gondim Teixeira et al. (2022) proposed measuring RSD solely in the neutral position. In this study, RSD was evaluated by the CT-RSD measurement in loaded and in unloaded CT scans. With the evaluation of these static CT images, motion-induced artefacts are prevented. These are commonly seen with 4-D CT and are difficult to avoid because the physiological movements of the wrist are fast compared with the speed of contemporary 4-D CT scanning devices (van der Heijden et al., 2025). In our CT-approach, only two CT scans are required with limited radiation exposure, and laborious segmentation of the multiple low-quality CT scans typically produced during 4-D CT is avoided. Therefore, this may potentially be a good alternative to 4-D CT scanning.
Although statistical significance was demonstrated, stress loading induced less than 1 mm of median SLD increase on plain radiographs. Our CT-based measurement method detected a median increase in RSD of 3 mm, perhaps making this method more relevant in the diagnostic decision making. Since no median increase in RSD was found in patients without instability, an increase in RSD of more than 1 mm, combined with clinical symptoms and a positive Watson test, could be suggestive of dynamic scapholunate instability.
Our study also indicated that a dynamic increase in RSD under loading may be present before a dynamic increase in SLD occurs in patients with dynamic instability. We hypothesize that the secondary stabilizers are still able to resist the dissociation between scaphoid and lunate. Both RSD and SLD will probably increase as the instability progresses. Finally, since no significant differences were measured between the symptomatic unstable wrist and the contralateral non-symptomatic wrist, CT findings should always be correlated with symptoms and a thorough clinical examination to distinguish pathological from asymptomatic instability.
This study has limitations. First, this was a feasibility study without a power analysis. Second, in the dynamic instability group, all had a positive painful scaphoid shift click test. However, less severe stages of predynamic or dynamic instability, with scaphoid shift pain but without a positive click test, were not evaluated. More research is necessary to determine if these earlier stages of instability are also detectable with loaded CT scans. Third, the SLD measurement was performed on pronated PA views, so no exact comparison is possible with studies that used standard wrist radiographs. Fourth, it is difficult to maintain an identical position during repeated examinations. To overcome this, the BUDS view was initially described in a bilateral forearm-holding device, which was also described in a previous 4-D CT study but was not included in this study (Puig de la Bellacasa et al., 2022; van der Heijden et al., 2025). Fifth, as the CT scan-based measurements were largely automated, interobserver reliability was not evaluated. Previous authors documented good intra-observer reliability (ICC > 0.95) and interobserver reliability (ICC of >0.77) when measuring SLD with 4-D CT (Goeminne et al., 2025). Sixth, a landmark technique was introduced that uses the intersection between the longitudinal axis and the articular surface of the scaphoid, lunate and radius. This measurement technique differs from other methods, such as the concentric circles, dorsal radial axis tangential line and posterior radioscaphoid angle, and still requires validation. Moreover, the distances between these landmarks that were described cannot be directly compared with those on plain radiographs, as different landmarks were used. However, we believe that this approach may possibly ensure greater consistency across subjects and loading conditions. Seventh, there may have been variability in the patients’ effort during wrist loading. Computed tomography scanning of both wrists simultaneously is performed with the patient in a prone position with outstretched arms. Maintaining this position in combination with BUDS loading of the wrist can be difficult, especially when patients are highly symptomatic. Finally, statistically significant differences observed in this study may not be clinically relevant as the mean difference was less than 1 mm for some variables.
Objective information on stress-induced SLD and RSD can guide surgeons and patients in their treatment decision and can determine if scapholunate stability is restored or has re-occurred (Athlani et al., 2021; Berkhout et al., 2025). More evidence is required to confirm our findings that this stress CT-based method may provide more relevant indicative information than plain radiographs.
Supplemental Material
sj-docx-1-jhs-10.1177_17531934261446778 – Supplemental material for Analysis of dynamic scapholunate instability with stress views on plain wrist radiographs and stress CT
Supplemental material, sj-docx-1-jhs-10.1177_17531934261446778 for Analysis of dynamic scapholunate instability with stress views on plain wrist radiographs and stress CT by Chul Ki Goorens, Benyameen Keelson, Joris Duerinckx, Kjell Van Royen, Antoine van Ravestyn and Thierry Scheerlinck in Journal of Hand Surgery (European Volume)
Footnotes
Acknowledgements
For this study, we would like to thank Mireia Esplugas, Kaplan Institute, for her valuable contribution in the initial phase of this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical approval
Informed consent
Informed consent was obtained from the participants of this study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.