
Abstract

Dear Editor,
The progress of orthopaedic surgery has depended not only on innovation but on the systematic understanding of failure. Sir John Charnley exemplified this principle through his rigorous use of implant retrieval and analysis, which underpinned the success of low-friction hip arthroplasty (Wroblewski and Siney, 1993). As trapeziometacarpal joint (TMJ) arthroplasty evolves, there is a compelling need to revisit these principles.
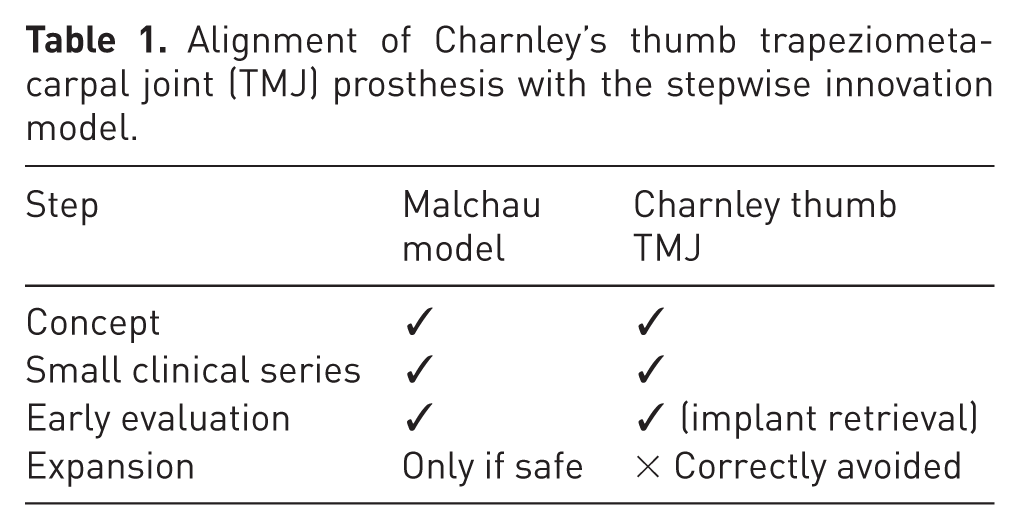
An often-overlooked aspect of Charnley’s work was his attempt to perform TMJ arthroplasty of the thumb. Although ultimately unsuccessful, his approach remains highly instructive. He introduced the implant cautiously, critically evaluated outcomes and discontinued its use once failure mechanisms became evident. This represents an early example of responsible, stepwise innovation, closely aligned with the later framework described by Malchau et al. (2011), in which progression depends on structured evaluation and, importantly, the willingness to stop (Table 1).
Alignment of Charnley’s thumb trapeziometacarpal joint (TMJ) prosthesis with the stepwise innovation model.
The history of large joint arthroplasty highlights the consequences of failing to adhere to such principles. Recurrent patterns of widespread adoption followed by unanticipated failure, seen in both early implant designs and more recent systems such as the Articular Surface Replacement (ASR; DePuy) hip, have demonstrated the limitations of relying solely on clinical observation or on the time lag inherent in registry data (Massoud et al., 1997; Morscher, 2003; Reed et al., 2024). While national registries have improved surveillance, they are constrained not only by time lag but may also ‘camouflage’ implant-specific failures within aggregated datasets. In contrast, retrieval analysis provides immediate, mechanism-based insight into implant performance (Phillips and Tucker, 2021).
In hand surgery, however, implant retrieval remains underutilized. Trapeziometacarpal joint arthroplasty reports generally favourable patient-reported outcomes, yet survivorship and functional gains remain variable. Structural implant failure, particularly in silicone devices, is common and without clear clinical correlation (Boe et al., 2018; McGovern et al., 2001). High patient satisfaction may paradoxically mask early warning signals, encouraging continued adoption despite incomplete understanding of failure mechanisms.
This trajectory reflects what has been described as ‘Scott’s phenomenon’: the expansion of surgical technologies in advance of robust long-term evidence. In the absence of structured retrieval programmes, there is a risk that small joint arthroplasty will repeat the historical patterns observed in larger joints.
The rationale for routine implant retrieval in hand surgery is clear. Failure mechanisms such as wear, loosening and biological response are not scale-dependent. Retrieval analysis provides direct insight into real-world performance, informs implant design and strengthens the evidence base for clinical practice. Moreover, there is an increasing ethical and medico-legal expectation that failed implants are accounted for and, where possible, analysed.
Charnley’s abandoned TMJ prosthesis should not be viewed as failure, but as a model of disciplined and ethical innovation. His willingness to stop, informed by early retrieval and analysis, remains as relevant today as it was then.
Many surgical specialities societies and associations have now advocated implant retrieval and analysis as essential practice, to enhance patient safety, support responsible innovation and ensure that the lessons of the past are not overlooked. We therefore advocate that routine retrieval and analysis of failed TMJ implants be considered essential practice within hand surgery. The lesson has already been written. The responsibility now lies in mandating its application.