
Abstract
Introduction:
Osteoid osteoma and osteoblastoma can be difficult to differentiate without biopsy, and clinical management can differ. Therefore, we asked: (1) what are the differences in clinical symptoms and imaging characteristics between carpal osteoid osteoma and osteoblastoma; and (2) which radiological measurements can differentiate carpal osteoid osteoma from osteoblastoma, and what are their optimal cut-off values?
Methods:
This retrospective single-centre study included 20 surgically treated patients with carpal osteoid osteoma (16 patients) or osteoblastoma (four patients) from January 2012 to December 2025. Demographic, clinical and imaging data were collected. Clinical assessment included night pain worsening score, rest pain, activity-related pain, pain after non-steroidal anti-inflammatory drug treatment, local tenderness and swelling. Preoperative computed tomography images were used for three-dimensional segmentation analysis to measure lesion volume, mineralized volume, lesion diameter, lesion-to-carpal volume ratio and mineralization-to-lesion ratio. Bone marrow and soft tissue oedema were evaluated on magnetic resonance imaging when available. Diagnostic performance and measurement reliability were also assessed.
Results:
Baseline demographic characteristics were similar between groups. Compared with osteoblastoma, osteoid osteoma showed greater night pain worsening scores (2.0 (IQR: 1.0 to 2.0) vs. 0.5 (IQR: 0 to 1.0)) and lower pain visual analogue scale scores after non-steroidal anti-inflammatory drug treatment (3.5 (IQR: 3.0 to 4.0) vs. 6.0 (IQR: 5.8 to 6.0)). Rest pain, activity-related pain, local tenderness and swelling were similar between groups. Osteoblastoma had a larger lesion diameter (18 mm (IQR: 17 to 20) vs. 5.8 mm (IQR: 5.5 to 6.7)), lesion volume (1300 mm3 (IQR: 920 to 1700) vs. 72 mm3 (IQR: 48 to 120)), and lesion-to-carpal volume ratio (40% (IQR: 36 to 48) vs. 2.7% (IQR: 2.5 to 2.9)), whereas osteoid osteoma had a higher mineralization-to-lesion ratio (46% (IQR: 40 to 56) vs. 3.9% (IQR: 2.8 to 4.3)). The cut-off values were 460 mm3 for lesion volume, 16% for lesion-to-carpal volume ratio, and 9.4% for mineralization-to-lesion ratio. Magnetic resonance imaging oedema scores were similar between the two groups.
Conclusion:
Worsening nocturnal pain, relief following non-steroidal anti-inflammatory drug administration, a smaller lesion size and a higher mineralization-to-lesion ratio are suggestive of osteoid osteoma, while a larger lesion-to-carpal volume ratio and lower internal mineralization support a diagnosis of osteoblastoma.
Level of evidence:
IV
Introduction
Osteoid osteoma and osteoblastoma are benign osteogenic tumours (Bahouq et al., 2011; Choi and Ro, 2021; Marcuzzi et al., 2002; Tepelenis et al., 2021). Osteoid osteoma accounts for approximately 24% of primary carpal tumours, whereas osteoblastoma represents only about 2.3% (Chughtai et al., 2024; Murray et al., 1999). Owing to the small size and complex anatomy of the wrist, both lesions often present with non-specific clinical and imaging features, such as wrist pain and swelling, thereby complicating accurate preoperative differentiation between osteoid osteoma and osteoblastoma (Afshar, 2012). Moreover, histopathological distinction may occasionally be difficult, and diagnosis requires correlation with clinical and imaging findings (Jackson et al., 1977).
Traditionally, a 2.0 cm diameter cut-off has been used to distinguish osteoid osteoma from osteoblastoma (Gitelis and Schajowicz, 1989; Healey and Ghelman, 1986; Jackson et al., 1977). However, this size criterion was initially defined based on tumours arising in long bones. In the carpus, osteoblastomas may not reach 2.0 cm because of the small size of the involved bones, which may increase the risk of misdiagnosing as osteoid osteoma (Afshar, 2012). Accurate differentiation is clinically important because the treatment strategies differ between these tumours: osteoid osteoma is typically managed with intralesional curettage, bone grafting or radiofrequency ablation, whereas osteoblastoma may require en bloc resection of the involved carpal bone in selected cases (Afshar, 2012; Atesok et al., 2011; Meyer et al., 2023). Moreover, the literature on carpal osteoid osteoma and osteoblastoma remains limited, consisting of some case reports or small case series. To date, there is no diagnostic index to differentiate carpal osteoid osteoma from osteoblastoma.
Therefore, we asked: (1) what are the differences in clinical symptoms between carpal osteoid osteoma and osteoblastoma; and (2) which radiological measurements can differentiate carpal osteoid osteoma from osteoblastoma and what are their optimal cut-off values?
Methods
Study design and patient selection
This retrospective single-centre study included carpal osteoid osteoma or osteoblastoma patients who were surgically treated in our hospital between January 2012 to December 2025. The study was approved by the institutional review board of our institution and written informed consent was obtained from all patients. Included patients met the following criteria: (1) a primary lesion in the carpal bones; (2) histopathological diagnosis of osteoid osteoma or osteoblastoma; and (3) availability of preoperative CT images. Final diagnosis was based on histopathological findings as well as their clinical and imaging features.
Data collection
Baseline demographic characteristics, including age, sex and body mass index (BMI), were collected from medical records. Clinical assessment included night pain worsening, rest pain, activity-related pain, pain after non-steroidal anti-inflammatory drug (NSAID) treatment, local tenderness and swelling. Rest pain, activity-related pain and pain after NSAID treatment were assessed using a visual analogue scale (VAS) from 0 to 10. Local tenderness and swelling were recorded as present or absent. Night-time pain worsening was graded on a 0 to 2 scale: 0 = absent; 1 = worse at night without awakening; and 2 = awakening at night, sleep disturbance or the need for NSAIDs during the night. Diagnostic delay was defined as the time from symptom onset to diagnosis. Plain radiographs and CT were reviewed in all patients and MRI was available in 11 patients. Surgical procedures, symptom resolution and tumor recurrence were recorded.
Imaging analysis
CT analysis
CT images were analysed for lesion and mineralization characteristics. Lesion diameter, lesion volume, mineralized volume and involved carpal bone volume were measured using three-dimensional segmentation in 3D Slicer. Mineralized areas were defined as high-attenuation regions within the lesion on bone window images. All segmentations were performed using the Draw tool in the Segment Editor module. The lesion, mineralized component and involved carpal bone were outlined on axial, coronal and sagittal CT images to reduce partial volume effects (Figure 1). The lesion-to-carpal volume ratio was defined as lesion volume divided by the involved carpal bone volume, and the mineralization-to-lesion ratio was defined as mineralized volume divided by the lesion volume. All segmentations were performed manually by the observers using the Draw tool in 3D Slicer. In our experience, segmentation and measurement require approximately 10 min per case.
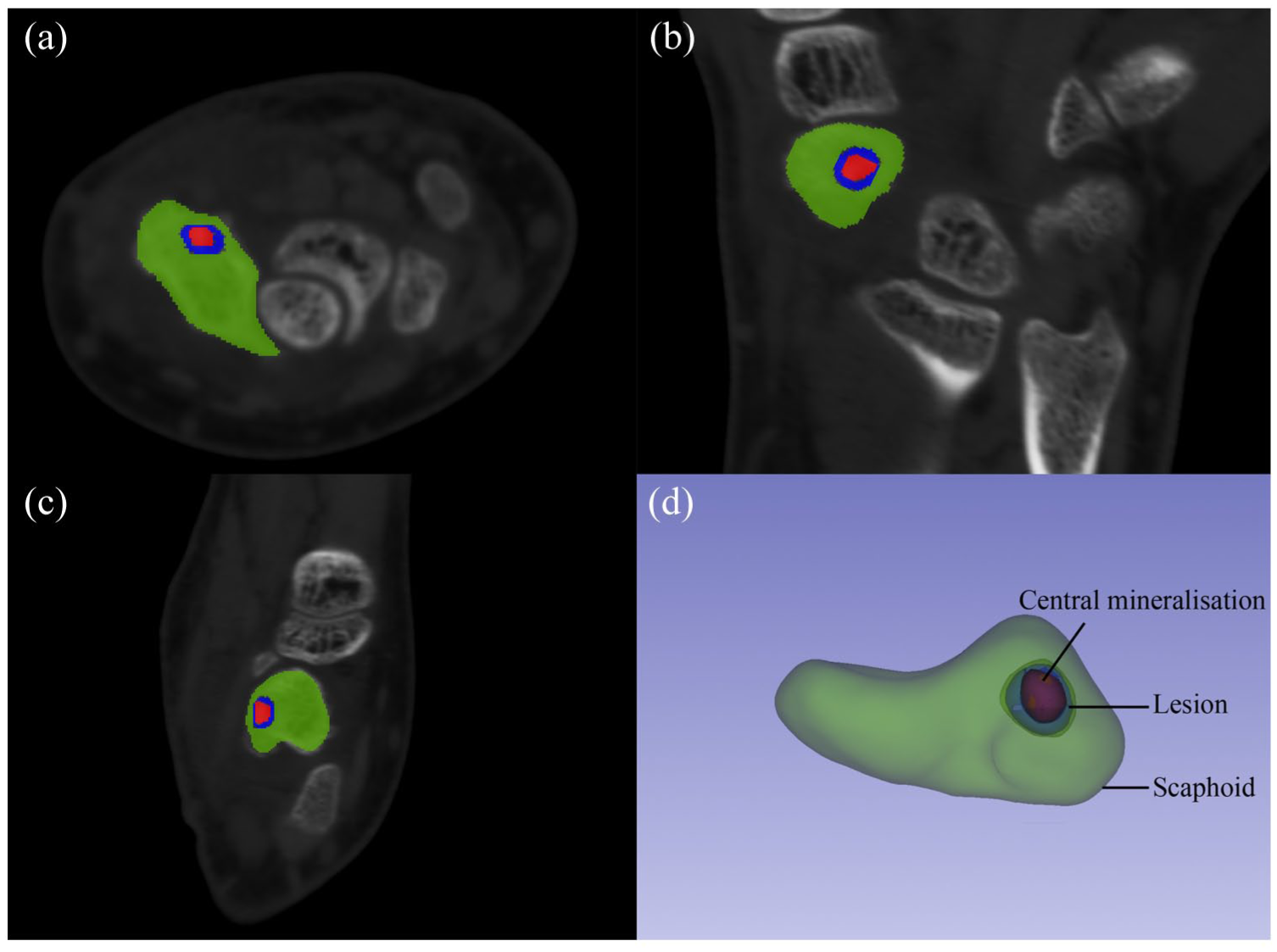
CT-based segmentation and volumetric measurement of a carpal osteoid osteoma in the scaphoid. Axial (a), coronal (b) and sagittal (c) CT images demonstrated segmentation of the scaphoid bone (green), the osteoid osteoma lesion (blue) and the central mineralization within the lesion (red). (d) Three-dimensional reconstruction illustrating the spatial relationship among the scaphoid bone, the lesion and the central mineralization. These segmentations were used to calculate carpal bone volume, lesion volume, mineralized volume, lesion-to-carpal volume ratio and mineralization-to-lesion ratio.
MRI analysis
In patients who underwent MRI, bone marrow oedema and surrounding soft tissue oedema were evaluated. The MRI sequences included T1-weighted, T2-weighted and fat-suppressed fluid-sensitive images. Bone marrow oedema was graded using the bone marrow oedema component of the Rheumatoid Arthritis Magnetic Resonance Imaging Score (Ostergaard et al., 2005). Bone marrow oedema was graded from 0 to 3 for each involved carpal bone according to the percentage of marrow involvement (0 = none; 1 = 1–33; 2 = 34–66; 3 = 67–100). When multiple bones were involved, the scores were summed. Soft tissue oedema was graded on a study-specific semiquantitative scale: 0 = none; 1 = focal edema; 2 = extensive oedema involving either the palmer or dorsal aspect; and 3 = extensive oedema involving both volar and dorsal aspects. The total MRI oedema score was the sum of the bone marrow oedema and soft tissue oedema scores.
Observer assessment and reproducibility
All CT- and MRI-based measurements were independently performed by two orthopedic surgeons who were blinded to the diagnosis. Each observer repeated the measurements after 2 weeks to evaluate intraobserver reliability. Interobserver and intraobserver reliability were evaluated using the intraclass correlation coefficient (ICC). The ICC values were interpreted as follows: <0.40 = poor; 0.40–0.59 = fair; 0.60–0.74 = good; and 0.75–1.00 = excellent. All CT- and MRI-based measurements showed good to excellent reliability. Interobserver ICCs ranged from 0.74 to 0.91, and intraobserver ICCs ranged from 0.77 to 0.93 (Table 1).
Interobserver and intraobserver reliability.
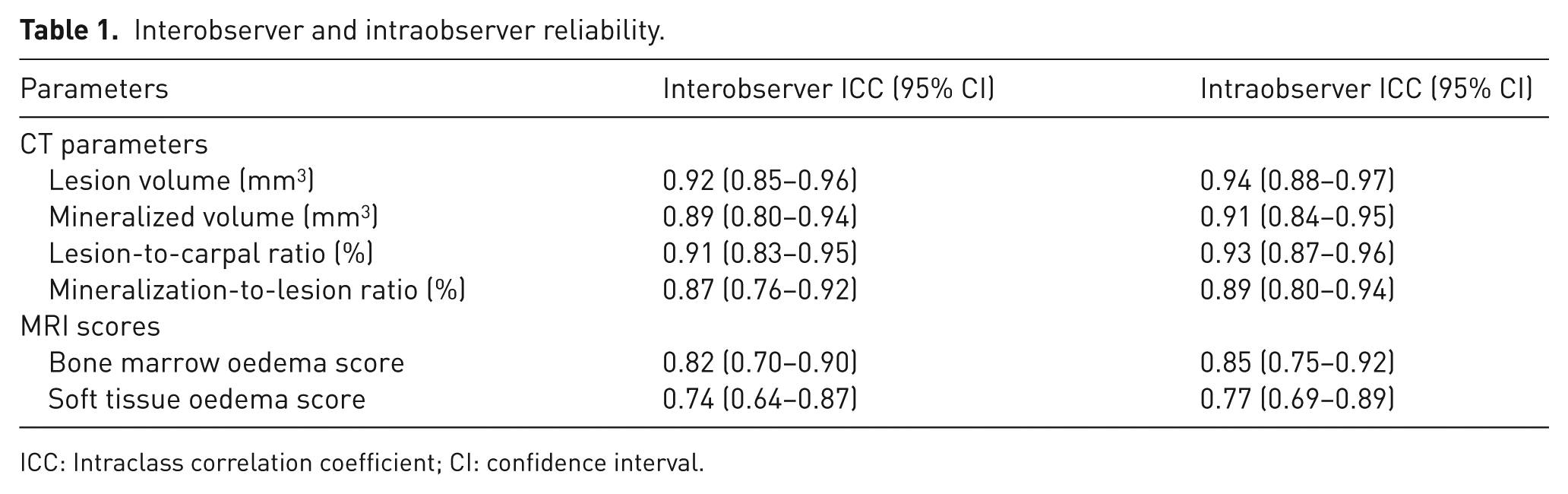
ICC: Intraclass correlation coefficient; CI: confidence interval.
Statistical analysis
The normality of continuous variables was assessed using the Shapiro–Wilk test. As all continuous variables were non-normally distributed, they are presented as medians with interquartile ranges (IQRs) and were compared using the Mann–Whitney U-test. Categorical variables are presented as counts and percentages. Categorical variables were compared using the chi-squared test when all expected cell counts were ⩾5; otherwise, the Fisher exact test was used. Receiver operating characteristic curve analysis was performed to evaluate the diagnostic performance of parameters in differentiating carpal osteoid osteoma from osteoblastoma. The area under the curve (AUC) was calculated, and cut-off values were determined using the Youden index. When complete separation occurred (AUC = 1.00), the cut-off was defined as the midpoint of the separation range. All tests were two-sided, and p < 0.05 was considered statistically significant. Statistical analyses were performed using SPSS software (version 27.0; IBM Corp.).
Results
Patient characteristics
The study cohort included 20 patients: 16 with osteoid osteoma and four with osteoblastoma. Age, sex and BMI were comparable between the two groups (Table 2). In the osteoid osteoma group, four cases involved the capitate, four the hamate, three the trapezoid and two the scaphoid. The lunate, triquetrum and trapezium had one case each. In the osteoblastoma group, the hamate was involved in two cases, the triquetrum in one and the trapezoid in one. The median follow-up duration was 12 months (range 6–108 months). All patients with osteoid osteoma underwent intralesional curettage and autologous cancellous iliac crest bone grafting. Among patients with osteoblastoma, two underwent curettage with iliac crest bone grafting, one underwent primary en-bloc resection, and one underwent secondary en-bloc resection after recurrence following initial curettage. Among patients who underwent bone grafting, radiographic bony consolidation was achieved in all cases at a median of 10 weeks (range 8–12 weeks). Magnetic resonance imaging was performed in eight patients with osteoid osteoma and three patients with osteoblastoma.
Baseline clinical characteristics of patients with carpal osteoid osteoma and osteoblastoma.
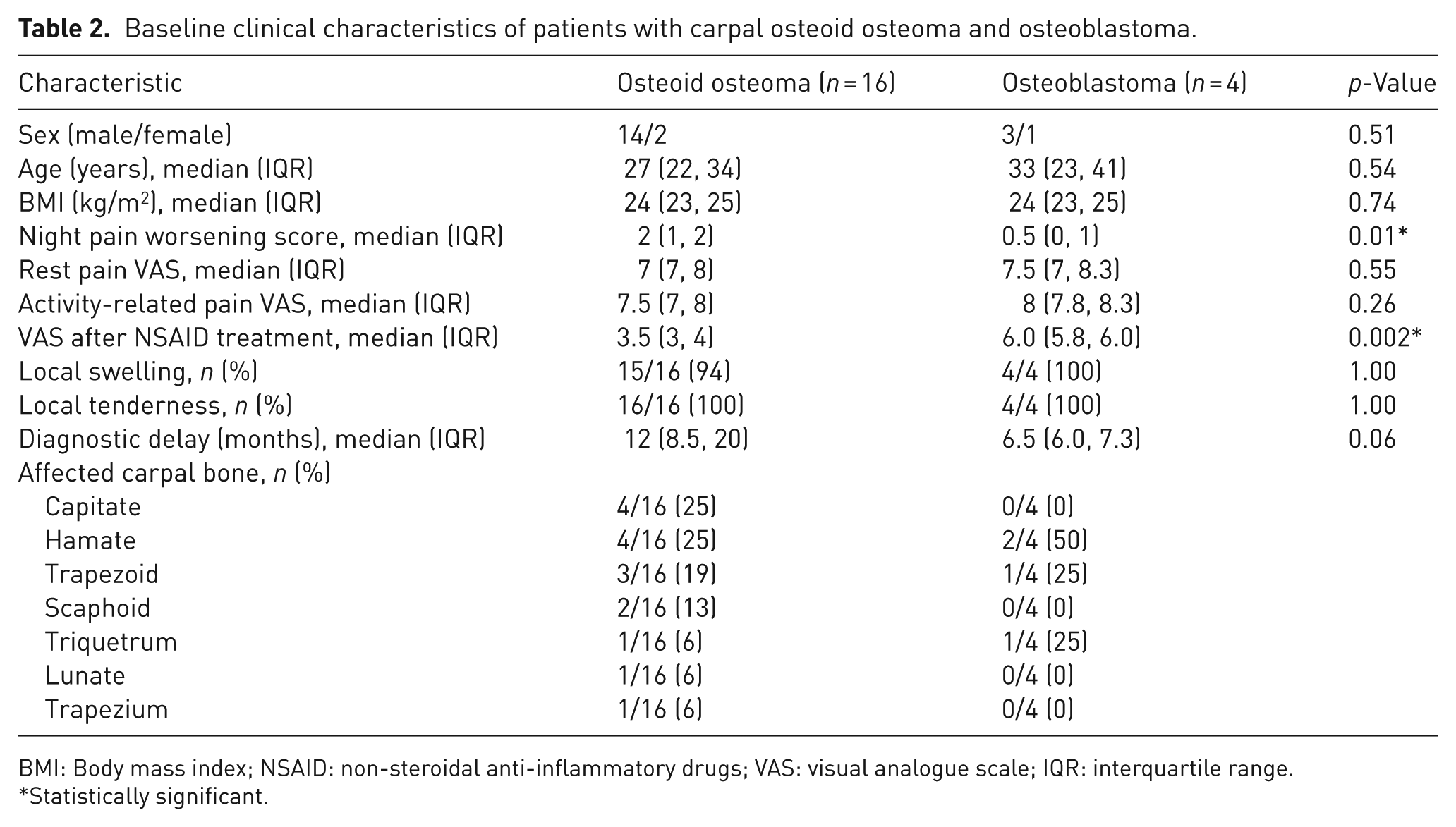
BMI: Body mass index; NSAID: non-steroidal anti-inflammatory drugs; VAS: visual analogue scale; IQR: interquartile range.
Statistically significant.
Difference in clinical findings
People with osteoid osteoma experienced greater night pain worsening than people with osteoblastoma (Table 2). Similarly pain intensity was lower after NSAIDs in people with osteoid osteoma. Discomfort at rest and pain during activity were similar. Local tenderness was present in all patients. Local swelling was present in 94% of patients with osteoid osteoma and in all patients with osteoblastoma.
Difference in imaging findings and diagnostic cut-offs
Lesion volume was larger in osteoblastoma than in osteoid osteoma (Table 3). Similarly, the lesion-to-carpal volume ratio and diameter were larger in osteoblastoma, while the mineralization-to-lesion ratio was greater in osteoid osteoma. Mineralization volume was comparable between osteoid osteoma and osteoblastoma (Figures 2 and 3). There was no difference in MRI bone marrow or soft tissue oedema with the numbers available (Table 4).
Comparison of CT characteristics between carpal osteoid osteoma and osteoblastoma.
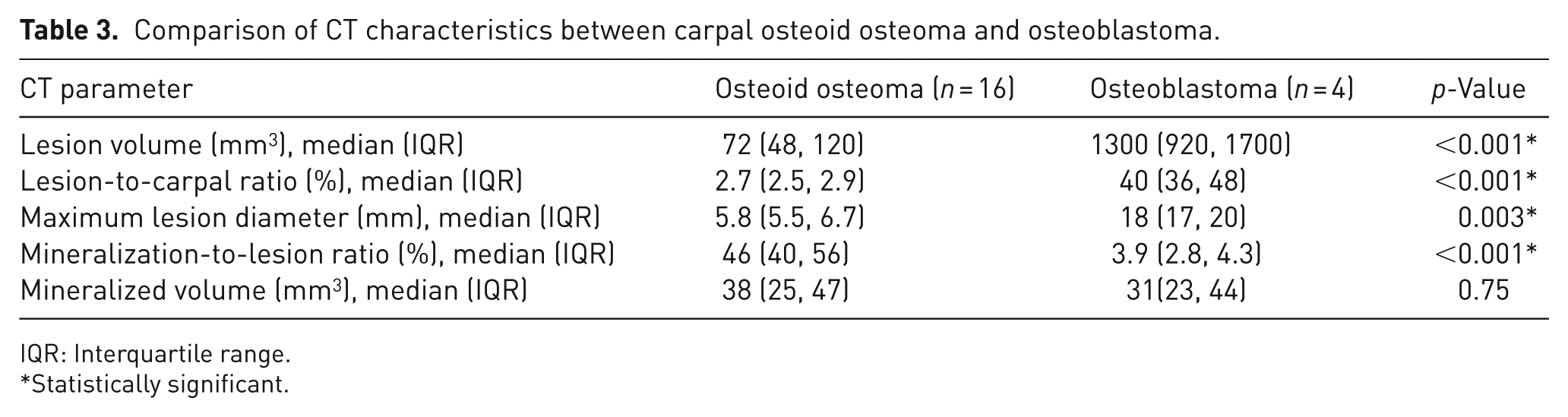
IQR: Interquartile range.
Statistically significant.
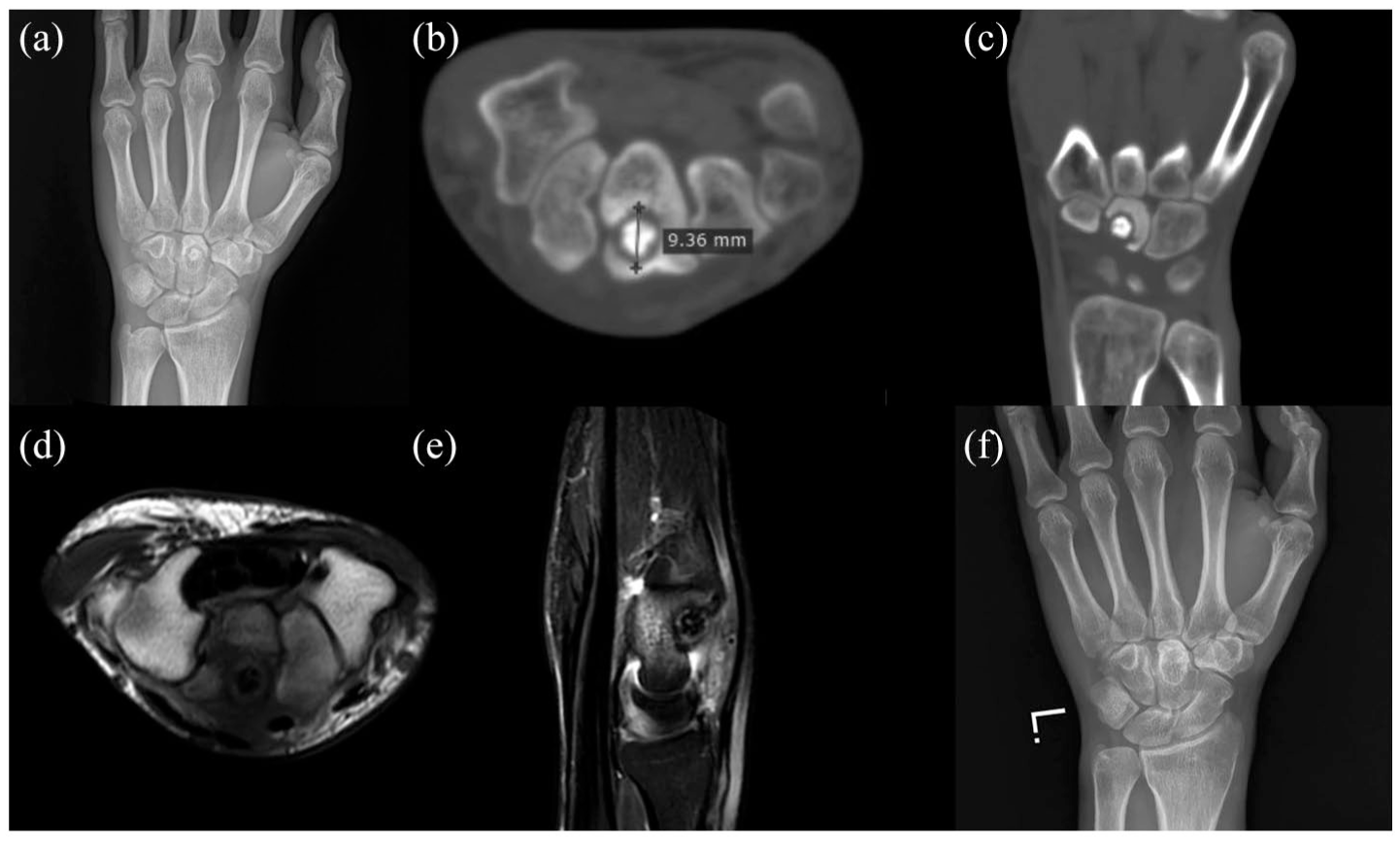
Imaging findings of osteoid osteoma in a 20-year-old male, involving the left capitate. Preoperative posteroanterior wrist radiograph (a) and axial (b) and coronal (c) CT images showed a clearly visible nidus with central mineralization and surrounding reactive sclerosis within the capitate, with a maximum nidus diameter of 9.4 mm. Magnetic resonance image showing a low-signal lesion in the capitate on axial T1-weighted imaging (d) and bone marrow oedema with dorsal soft-tissue oedema on sagittal T2-weighted imaging (e). Wrist radiograph (f) at the 20 month postoperative follow-up.
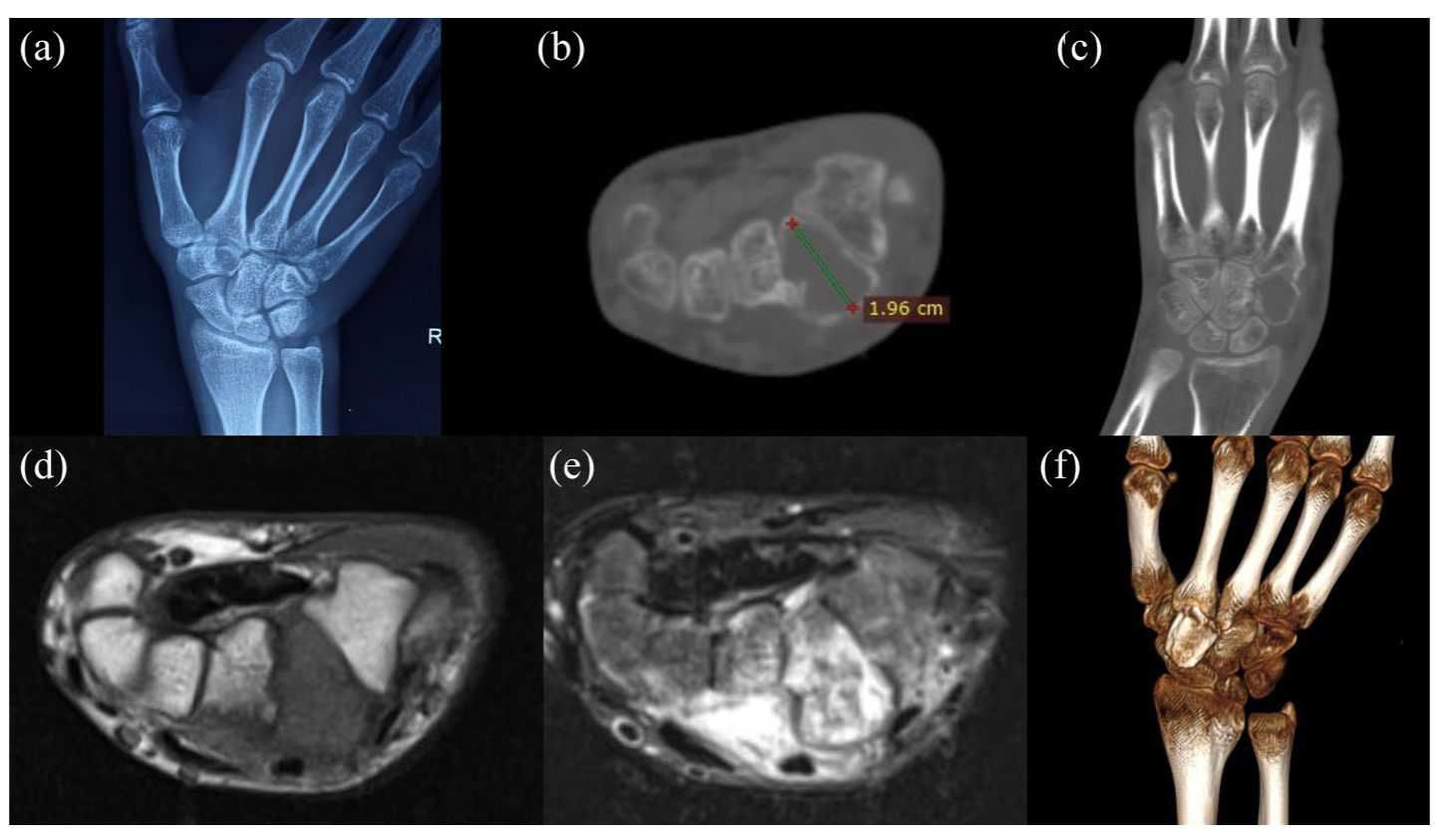
Imaging findings of an osteoblastoma in a 16-year-old male, involving the right trapezoid. Preoperative posteroanterior wrist radiograph (a) and axial (b) and coronal (c) CT images revealed a trapezoid lesion with a heterogeneous internal matrix and limited reactive sclerosis, with a maximum lesion diameter of 1.96 cm. Axial MRI showed a low-signal lesion in the trapezoid on T1-weighted imaging (d) and extensive bone marrow oedema with dorsal soft-tissue oedema on T2-weighted imaging (e). Follow-up three-dimensional CT reconstruction (f) after en bloc trapezoid resection and autologous bone grafting.
Comparison of MRI characteristics between carpal osteoid osteoma and osteoblastoma.
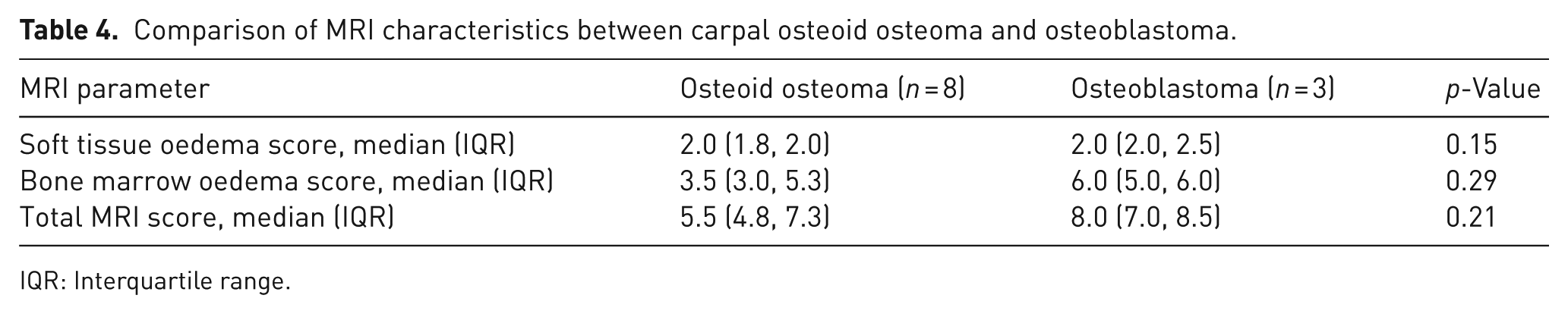
IQR: Interquartile range.
Lesion volume, lesion-to-carpal volume ratio and mineralization-to-lesion ratio all showed excellent diagnostic performance for differentiating carpal osteoid osteoma from osteoblastoma independently (AUC = 1.00; 95% CI: 1.00 to 1.00; p < 0.001). The cut-off values were 460 mm3 for lesion volume, 16% for the lesion-to-carpal volume ratio and 9.4% for the mineralization-to-lesion ratio, with 100% sensitivity and 100% specificity for all three parameters.
Discussion
Accurate preoperative differentiation between carpal osteoid osteoma and osteoblastoma is important because treatment strategies differ between the two tumours. Differentiation in the wrist is particularly difficult because the traditional size-based thresholds may be less reliable in the small carpal bones. Therefore we compared clinical and imaging characteristics. We found that worsening nocturnal pain, relief following NSAID administration, a smaller lesion size and a higher mineralization-to-lesion ratio are suggestive of osteoid osteoma, while a larger lesion-to-carpal volume ratio and lower internal mineralization support a diagnosis of osteoblastoma. These features can help hand surgeons distinguish carpal osteoid osteoma from osteoblastoma before surgery.
Osteoid osteoma was more often associated with worsening night pain and greater pain relief after NSAID treatment, whereas these features were less common in osteoblastoma. These findings are consistent with previous reports showing that osteoid osteoma typically presents with night pain and responds well to NSAID treatment (Carneiro et al., 2021; Cerase and Priolo, 1998; Noordin et al., 2018; Shu and Ke, 2022; Tepelenis et al., 2021), whereas osteoblastoma more often causes persistent or gradually progressive pain (Arkader and Dormans, 2008; Berry et al., 2008). In osteoid osteoma, this symptom pattern may be related to abundant nerve fibres within the lesion, often located near arterioles (Schulman and Dorfman, 1970). Increased prostaglandin production within the nidus may also contribute to pain by affecting local sensory nerve fibres and vascular tone (Atesok et al., 2011; Bedoya et al., 2024; Dookie and Joseph, 2026; Mungo et al., 2002). Recent molecular evidence suggests that FOS gene rearrangements in osteoid osteoma may enhance prostaglandin and NF-κB signalling (Lam et al., 2026). In contrast, osteoblastoma-related pain may be more related to progressive tumor growth and mechanical effects on adjacent structures (Atesok et al., 2011). Therefore, the pain pattern may provide an early clinical clue, but CT assessment remains necessary for accurate preoperative differentiation.
In our cohort, CT-based volumetric parameters provided stronger discrimination between carpal osteoid osteoma and osteoblastoma than lesion diameter alone. Osteoblastoma had a larger lesion diameter, a larger lesion volume and a higher lesion-to-carpal volume ratio, whereas osteoid osteoma had a higher mineralization-to-lesion ratio. During preoperative assessment, osteoblastoma becomes more likely when a carpal lesion occupies a large proportion of the involved bone and shows little internal mineralization. In contrast, a small lesion with prominent internal mineralization is more suggestive of osteoid osteoma. The traditional 2.0 cm diameter threshold for distinguishing osteoid osteoma from osteoblastoma was derived mainly from long bone tumours (Gitelis and Schajowicz, 1989; Healey and Ghelman, 1986; Jackson et al., 1977). However, this threshold may be less applicable in the carpus because osteoblastomas in small bones may not reach 2.0 cm, increasing the risk of misdiagnosis (Afshar, 2012). Others further suggested that lesion size alone cannot reliably distinguish these two tumours because small lesions may represent early-stage osteoblastoma (Chotel et al., 2012). To our knowledge, no previous study has used 3D images to quantify these parameters in carpal osteoid osteoma and osteoblastoma. Because carpal bones are small and vary in size, volumetric and ratio-based parameters may provide more information than lesion diameter alone. Although these parameters showed clear separation in our cohort, larger multicentre studies are needed to confirm their reproducibility and generalizability.
The MRI oedema patterns were less helpful than CT for differentiating carpal osteoid osteoma from osteoblastoma in our cohort. This is important because MRI is often used to evaluate patients with persistent wrist pain. However, marrow oedema and surrounding inflammatory change may obscure the nidus and overestimate lesion extent. These changes may complicate diagnosis and may even raise concern for malignancy (Bhure et al., 2019; Cerase and Priolo, 1998; Chakrapani et al., 2008; Villalobos et al., 2010). Our findings are consistent with previous studies showing that some osteoid osteoma lesions are not clearly visualized on MRI (Davies et al., 2002) and that MRI is less accurate than CT for diagnosing osteoid osteoma (Hosalkar et al., 2005). More recently, Gao et al. reported that marrow and soft tissue oedema were common in both osteoblastoma and osteoid osteoma. They also found that nearly half of the patients who underwent preoperative MRI were initially misdiagnosed as having malignant tumours (Gao et al., 2019). In clinical practice, wrist radiographs are usually performed first, followed by CT when a carpal bone lesion is suspected or when radiographic findings are unclear. Magnetic resonance imaging may be used in selected patients to assess bone marrow and soft tissue oedema. In our cohort, neither bone marrow oedema nor soft tissue oedema scores differed between the two groups, suggesting that MRI oedema patterns alone are insufficient for preoperative differentiation. However, MRI was available in only eight patients with osteoid osteoma and three with osteoblastoma, which limits the accuracy of this comparison. Future studies with larger MRI cohorts are needed to determine whether other MRI features can help distinguish these two tumours when combined with CT and clinical findings.
This study has several limitations. First, this was a retrospective single-centre study with a small and imbalanced sample, especially in the osteoblastoma group, which might limit the statistical power. Therefore, our findings need validation in the larger sample studies. However, both tumours are rare in the carpus. Second, only surgically treated and histologically confirmed cases were included. This design ensured diagnostic certainty, but it may also have introduced selection bias. However, without the reference standard of histopathology, we would be unable to perform this study. Third, MRI was available in only eight patients with osteoid osteoma and three patients with osteoblastoma. Therefore, the MRI findings should be considered exploratory. Fourth, CT-based measurements relied on manual image segmentation, which may introduce variability. However, interobserver reliability suggests this effect to be limited.
Worsening nocturnal pain, relief following NSAID administration, a smaller lesion size and a higher mineralization-to-lesion ratio are suggestive of osteoid osteoma, while a larger lesion-to-carpal volume ratio and lower internal mineralization support a diagnosis of osteoblastoma. These findings can help surgeons determine the origin of these bone lesions and help select appropriate treatment.
Footnotes
Acknowledgements
We appreciate all co-authors for their contributions to this study and the writing of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by Natural Science Foundation of Beijing Municipality (grant number: 7222087).
Ethics approval
All procedures performed instudies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.