
Abstract
Nerve surgery for unmeasurable upper extremity neuropathophysiology – such as pronator syndrome, supinator syndrome/radial tunnel syndrome, lacertus syndrome, and neurogenic thoracic outlet syndrome – remains a subject of ongoing debate due to the lack of objective reference tests confirming the diagnoses. This round table discussion outlines the perspectives of five expert surgeons navigating the clinical and ethical uncertainties of offering surgery for theoretical neuropathies presenting as non-specific pain. The panel explores the balance between subjective patient reporting and objective diagnostic limitations, the ethical implications of surgical placebo effects, and how to determine treatment effectiveness. The discussion highlights the divergent strategies among specialists regarding risk tolerance, overtreatment, and the implementation of shared decision-making in the absence of measurable disease.
Keywords
Introduction
Historically physicians had to contend mostly with syndromes: groups of signs and symptoms that occur together and are expected to be caused by an underlying pathophysiology. Through technological advances many initial syndromes now have a known, measurable cause. However, several syndromes remain without detectable pathophysiology. Examples include unmeasurable neuropathies such as pronator syndrome, supinator syndrome/radial tunnel syndrome, lacertus syndrome and neurogenic thoracic outlet syndrome.
It is useful to consider what is needed to move from an unmeasurable to a measurable neuropathy using current understanding of idiopathic median and ulnar neuropathies and their signs and symptoms, such as carpal and cubital tunnel syndromes.
When moderate to severe, idiopathic median neuropathy at the carpal tunnel can be accurately and reliably measured using neurophysiology or ultrasound (Dahlin et al., 2024). Advanced median neuropathy results in measurable loss of sensation in the median nerve distribution. The same applies to cubital tunnel syndrome, the signs and symptoms of idiopathic ulnar neuropathy at the elbow (Nyman and Dahlin, 2024).
Regarding median neuropathy, prior studies have compared specific signs and symptoms with the objective reference test of neurophysiology (Graham, 2008, Teunis et al., 2024). These studies suggest that when neuropathy is moderate to severe, additional testing is not required, and clinical signs and symptoms alone can establish the diagnosis. This is less consistent for ulnar neuropathy, with almost a third of patients having no neuropathy, or having other neuropathology (e.g. cervical), when signs and symptoms were tested against an objective reference test (Kortlever et al., 2023). The natural history of untreated median and ulnar neuropathy may be gradual deterioration (Nathan et al., 1998). Since surgery measurably improves neuropathophysiology and its signs and symptoms, altering the natural history of the disease, we can have confidence in its effectiveness even without a randomized controlled trial.
This contrasts with the characteristics of suspected neuropathies such as pronator, supinator and lacertus syndrome. The accuracy of their signs and symptoms in establishing the diagnosis cannot be determined because there is no objective reference test. Symptoms generally include pain, tenderness and weakness. Weakness is at least partially related to effort and discomfort, and discomfort is strongly related to mental and social health (Nunez-Cortes et al., 2022), making such symptoms potentially less accurate. Because there is no measurable neuropathophysiology, neither natural history studies nor improvement after surgery can be used to determine the effectiveness of surgery. Instead, the only experiment that could establish effectiveness would be a randomized trial comparing surgery with sham surgery with effective blinding of patients and evaluators. Still, surgery to address theoretical mononeuropathies continues to be discussed as a treatment for non-specific pain at professional society meetings (Boyer et al., 2025) and journals (Chim et al., 2025).
This raises the question of how surgeons tend to navigate these uncertainties. In this round table discussion, five surgeons with level 5 expertise in nerve surgery discuss some of these issues.
Dr Teunis (Editor)
In my opinion, no, but there is no way to be certain without proper studies. The magnitude of every variable in that equation – theoretical neuropathy, regression to the mean, self-limiting course, and placebo effect – is unknown. Even if those variables were known, there could still be some benefit to surgery if, for example, the self-limiting course could be hastened. Furthermore, we can’t rule out the possibility that these conditions are due to an as yet unidentified pathophysiologic process that doesn’t register on currently available nerve tests. In a scientific field we should not use opinion to reject an idea any more than to accept it. Not when we have a tool (controlled trials) to answer the question definitively. However, until we have appropriately controlled trials supporting such surgeries, I tend to fall back on the principle that undergirds most of my decision-making: risk-to-benefit ratio. If the benefit is reasonably certain and potentially large, I can tolerate a commensurate amount of risk, but if, as with these surgeries, the benefit beyond a non-specific effect is unclear or unlikely, I am generally unwilling to accept the risk of surgery. I like low-risk, high-benefit surgeries; these surgeries might be fairly low risk, but they are not zero risk, so I would like to know that they are producing a real physiological benefit before recommending them.
We have not proved yet that these treatments are better than no treatment or sham surgery. However, this has not been studied well, and several experts recommend surgery for theoretical neuropathies. Since the reference values used for electrodiagnostic testing are based on population means, their inaccuracy lies at the edges of normal. A person might have early or mild neuropathy but have a normal objective study. I am concerned about irrecoverable nerve damage by waiting and am inclined to offer surgery in such instances as a shared decision, even though this might risk overtreatment and the risk of developing severe, irrecoverable neuropathy in a short time could be low. I also consider most surgeries to remove suspected compressive tissue around a nerve to be low-risk procedures. And I think that the low probability of adverse events is outweighed by the risk of severe, irrecoverable or even painful neuropathy.
In cases of severe pain without objective findings, I sometimes offer surgery under the philosophy of ‘compassionate use’. This is comparable with seriously ill patients, who get access to investigational treatments outside clinical trials when no other options exist. Additionally, when treatments through pain management specialists have failed to alleviate severe pain, I will consider offering such surgeries. However, I do this while explicitly stating that the surgery offered is experimental (not evidence based) and might not (fully) provide symptom improvement. I emphasize strong shared decision-making between the patient and myself, incorporating the risks of surgery.
I’m more concerned about the risks of surgery. Although surgical intervention may be regarded as a definitive treatment, it inevitably entails tissue injury and scar formation in the skin and surrounding structures, including those adjacent to the targeted tissue, such as peripheral nerves. Surgery also carries inherent risks related to anaesthesia and postoperative adverse events, including infection, which may increase the likelihood of ongoing discomfort and perhaps neuropathy-related pain. Because of the difficulty establishing the diagnosis, the risks of surgery and an unpredictable outcome, surgery for a suspected neuropathy should be offered with caution. Especially since the self-limiting nature of these disorders is well recognized, I therefore first offer non-surgical treatment (such as activity modifications, improved ergonomics and reduced repetitive gripping) (Adler and Wolf, 2020).
I agree with the concerns about the risks of surgery and I don’t think surgeries intended to address unmeasurable neuropathy causing discomfort have more than non-specific effects. I would rather offer treatments without the potential risks of surgery, such as watchful waiting or splints. Even if such treatment also only has non-specific effects, it doesn’t have the same risks as surgery.
I must admit that, specifically regarding suspected compressive neuropathy of the median nerve at the lacertus (lacertus syndrome), a video showing immediate improvement in strength of the deep flexor of the index finger after release is compelling, although it’s unclear if discomfort also improved. Regardless, it’s a surgery I have not performed, as I have not diagnosed the problem as of yet.
Yes, I believe specifically that transection of the lacertus for suspected median neuropathy at the elbow, as mentioned by Dr Xing, would outperform sham surgery. I believe this because, for example, a study reported less discomfort and greater strength after a steroid injection around the median nerve when this neuropathy was suspected (Greene et al., 2025). I realize this study did not compare against a placebo injection, and improvement might be related to non-specific effects. Regardless, I had my own lacertus transected and obtained instantaneous improvement in numbness and weakness. Clearly, I personally got a ‘specific effect’ resolution from a dynamic compression causing neuropraxia. I have seen the same result in many lacertus releases that I have performed.
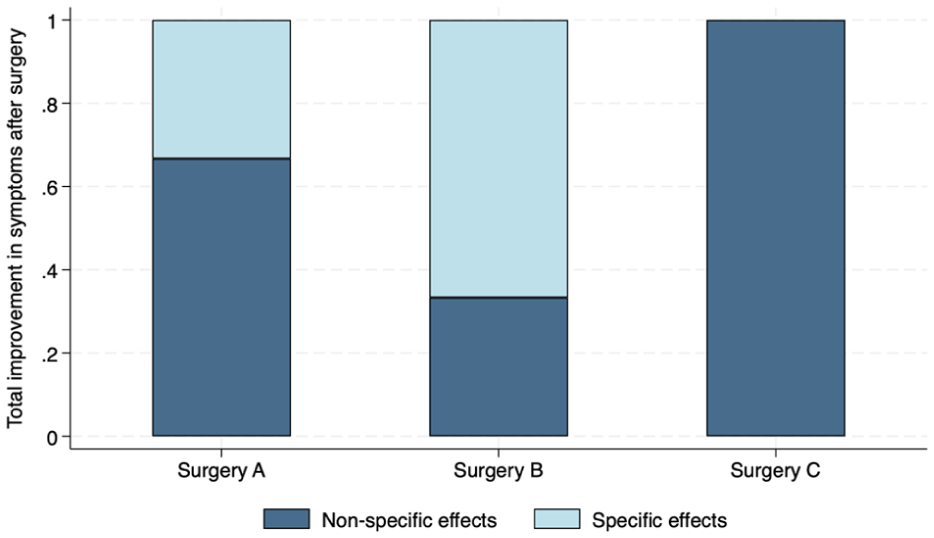
Conceptualization of the effects of surgery. Specific effects are the proportion of symptom alleviation directly related to changes in physiology/pathophysiology; non-specific effects are the proportions alleviated due to placebo effects, natural history of the disease and regression to the mean. Surgery A: the mean symptom improvement related to non-specific effects after surgery was 67% derived from 100 trials of various surgeries (95% CI, 61 to 73 per cent) (Karjalainen et al., 2022). Surgery B represents a very effective surgery, with a large specific effect owing to changes in pathophysiology. Surgery C is a surgery that is no better than sham surgery, such as release of the origin of the extensor carpi radialis brevis tendon for tennis elbow (Matache et al., 2016).
Dr Teunis
One of the basic tenets of medicine is ‘Above all, do no harm’. To stay with suspected median neuropathy at the lacertus, I’m convinced that the lacertus release is effective, so doing a sham surgery controlled trial will just expose participants in the sham surgery group to unnecessary surgery, with risks and recovery time. And then later, they have a second surgery to really divide the lacertus because the problem is still there. Which is more difficult and perhaps dangerous owing to the additional scar tissue. Since I know transection of the lacertus is effective, I’m not concerned about people having this surgery unnecessarily.
I agree that the concept of placebo surgery contains an inherent tension between the ethical imperatives of pursuing rigorous scientific evidence and protecting research participants from harm (Horng and Miller, 2002). The principle of non-maleficence – primum non nocere (roughly expressed as ‘first, do no harm’) is central to discussions surrounding placebo surgery (or ‘sham surgery’).
However, there are examples in which surgical procedures have been evaluated against placebo surgery, leading to the abandonment of costly and potentially harmful interventions, such as arthroscopy for knee osteoarthritis (Moseley et al., 2002). The use of placebo controls in randomized controlled trials of surgical procedures may therefore be ethically justified when supported by a strong scientific and ethical rationale (Hostiuc et al., 2016; Rogers et al., 2014). Particularly relevant are the Applying Surgical Placebo in Randomised Evaluations guidelines (Beard et al., 2020).
However, the mere presence of a placebo effect does not ethically justify surgical interventions that lack specific effects, because surgery entails real risks, might involve deception and diverts scarce healthcare resources from effective care even in ‘theoretical neuropathy’ disorders. In addition, anxiety and depression are recognized as strong drivers of symptom intensity in musculoskeletal disorders, including nerve entrapment disorders (Dahlin et al., 2022). A surgical placebo effect may also stem from the surgical incision, potentially triggering endogenous mechanisms involved in pain modulation, including processes related to anxiety reduction; these are similar mechanisms to those observed in self-inflicted injury undertaken to manage anxiety.
I agree with Dr Dahlin. One could argue that it may be beneficial to harness the placebo effect, if one accepts the ethics of ‘tricking’ a patient into feeling better. However, even a small surgery carries far more risk (pain, expense, complications) than a sugar pill. A confident surgeon might argue that the risk is negligible, but that is a viewpoint distorted by our health insurance system – if patients were forced to pay the entire cost of a surgery for which controlled trials show only a placebo effect, and were also on the hook for any adverse events, few would sign up. And even if the surgical risk were negligible for an individual patient, over thousands of iterations there will be some major complications.
In general, I don’t think we should offer surgery with potentially only non-specific effects. Placebo surgeries should be undertaken with caution.
I don’t think we should perform (likely) placebo surgeries outside of a properly designed trial.
Dr Teunis
As one of the people offering such surgeries, to me the evidence that transection of the lacertus is an effective treatment for suspected median neuropathy is that many, if not all, people get better after surgery, including myself. That is not absence of evidence. In fact, I think it would be unethical to offer sham surgery after having seen so many people improve. Moreover, perhaps a sham surgery controlled trial is too high a bar. Tell me which new operations were proved by sham surgery other than the rare exception?
I see this differently. There is an ethical obligation to properly prove the efficacy of any medical intervention, and indeed, most economic transactions. A plumbing manufacturer is ethically obligated to test their pipes before customers install them in their homes. Even casinos calculate and report the RTP (return to player) of a particular game – if the ethics of the medical profession cannot match up to the gambling industry, we have lost our aim.
I agree, it is essential that rigorously designed scientific and ethical clinical research studies are conducted to evaluate both novel and previously established surgical interventions, including those described in the introduction. This is particularly important in situations where the benefit to the individual patient may be uncertain, where there is a potential risk of harm, and/or where the procedure may incur substantial health care costs in a setting characterized by increasing competition for limited health care resources.
I recognize that designing and executing such clinical research studies is demanding for the principal investigator. The studies will probably need to be conducted as multicentre trials to ensure adequate sample sizes, as determined by appropriate power analyses.
We both agree that we shouldn’t offer surgery without evidence supporting its effectiveness, outside of well-designed trials. Physicians inclined to offer such surgeries have the ethical obligation to perform such a trial. We both recognize that the suspected conditions seem to be rare, complicating trial execution.
There is evidence that a limited number of specialists are comfortable making unverifiable diagnoses and offering surgery for them (Brinkman et al., 2024). What seems to vary is the specialist level of comfort with: (1) diagnosis based on symptoms and subjectively influenced signs (e.g. weakness) alone (no measurable pathophysiology); and (2) judging the effectiveness of surgery based on symptom alleviation after surgery without a proper control group that would account for any non-specific effects.
Dr Teunis
Not every intervention needs a sham-controlled trial. We don’t need to perform a sham trial of insulin for type 1 diabetes, because we can accurately and reliably measure the physiological effect of insulin, and we know the physiological result of non-treatment. But clearly the conditions and treatments we are discussing are in no way like type 1 diabetes and insulin, instead involving what appear to be purely subjective complaints and outcomes, like capability and discomfort. If we want to forgo sham-surgery controlled trials, we need better ways of measuring nerve pathophysiology. Electrodiagnostics, ultrasound, MR neurography – these all have disappointing levels of accuracy, precision, specificity and sensitivity. Sham surgery is disturbingly crude, too. I wouldn’t relish the act of cutting someone’s skin and immediately sewing it closed just for the sake of blinding. That particular someone is clearly not benefiting from that surgery, even if the greater medical community is. But unless we develop better diagnostic tools, sham surgery is the best we have.
There are few circumstances in which the conduct of scientifically and ethically sound clinical research may be considered unnecessary (e.g. if an intervention’s safety and efficacy have previously been conclusively established and applicable for the relevant population and similar indication). Nevertheless, the use of a placebo-controlled design may be neither appropriate nor ethically justified when a new surgical technique represents only a minor modification of an established procedure and is intended to be less invasive or more efficient. In such cases, comparison with an active control procedure may be sufficient to address the relevant research question, while minimizing ethical concerns and avoiding exposure of participants to sham surgery.
Currently, in order to establish the effectiveness of nerve surgery for non-specific arm pain, there is no other option than a sham-surgery controlled trial. Even a non-sham-surgery randomized controlled trial would only offer preliminary guidance at best. Only if we would be able to accurately measure neuropathy in instances of non-specific pain could we forgo sham-surgery controls.
I think that consistent improvement in patient-reported outcomes or strength measures are the best evidence that transection of suspected compression sites works. If we want to study this more thoroughly, perhaps we could perform intraoperative measurement of flexor pollicis longus and deep flexor of the index finger power with a pinch meter before and after division of the lacertus by an independent observer – I find this more ethical than sham surgery.
For me this also applies to suspected idiopathic ulnar neuropathy at the elbow. People with cubital tunnel syndrome without measurable ulnar neuropathy get better after surgery, which in my mind proves the effectiveness of surgery. I realize that these outcomes are subjective and that this approach doesn’t account for any non-specific effects, such as the placebo effect.
For me there are several conditions that need to be met in order to offer surgery for potentially speculative neuropathies. First, the surgery needs to have a known, low-adverse-event risk and the patient needs to be willing to accept those risks. Second, I use ultrasound-guided ‘triple’ nerve blocks, when possible, to determine if neuropathy is likely (Rijsdijk et al., 2024). These blocks consist of short- and long-acting anaesthetic and a placebo – in random order. The patient is not informed about the type of block to encourage blinding, but I acknowledge the blinding is limited owing to the numbing effect on the skin. Surprisingly, I have noticed that some patients have difficulties in quantifying the numbing effect in intensity and duration. When the patient reports pain resolution in accordance with the type of block provided, I regard this as indicative of neuropathy of the tested nerve, and I am willing to offer surgery. Third, the patient needs to have substantial discomfort that cannot be treated in any other way. Fourth, the patient needs to be aware that this is experimental surgery and may not improve their symptoms.
One of my concerns with using nerve blocks in this manner is the selection of placebo responders. We know from a prior sham-surgery trial that patients notice skin numbness, which probably reduces the effectiveness of blinding (Guyuron et al., 2009). Because of this, it seems unlikely that nerve blocks can be an accurate test of neuropathophysiology.
Dr Teunis
In situations like this, where there is potential for under-treatment and over-treatment, I would rather risk under-treatment. Non-operative treatments carry minimal risk and avoid potentially unnecessary harm. Over-treatment, however, poses more significant concerns, including potential adverse events (even if rare), increased patient morbidity and additional economic burden. Therefore, regarding people with non-specific arm pain, non-operative treatment should be the initial approach, rather than proceeding directly to surgery in the absence of sufficient evidence supporting its effectiveness.
I agree, if it turns out I undertreated this phenomenon, I’m comfortable knowing that I chose prudence.
Before I began my medical training, I had a general gestalt that I suspect is shared by most laypeople – that physicians have good evidence for everything they do. Having been in the field for a few decades, I now know that medicine is often a practice of educated guessing. I have guessed wrong many times in my career, doing a surgery when I shouldn’t have, or not doing a surgery when I should have. I think we must all – skeptics and advocates – embrace this epistemic humility, and deploy whatever tools we have to minimize the guesswork in our field.
If it turns out that transecting the lacertus does not outperform sham surgery, I would accept that result – but only if the study was well done and scientifically valid. But even then, for me the study really should be repeated by at least one second set of investigators for it to become real. For those who are skeptical about the effectiveness of ‘unproven surgery’ such as lacertus release, I strongly suggest you read the paper by George Phalen in 1981 when he discussed carpal tunnel origins in the 1950s (Phalen, 1981).
If it turns out, in adequately designed studies, that these surgeries are no better than sham surgery, I would stop offering them and I would urge my colleagues to do the same. Since I currently discuss with the patients that this possibility may occur in the future, we have accepted this risk together.
And with that I want to thank Drs Coert, Dahlin, Henry, Lalonde and Xing for discussing such a complex topic, and sharing how they navigate the uncertainties surrounding surgery for unmeasurable neuropathy in an attempt to alleviate non-specific arm pain.
Footnotes
Acknowledgements
We are grateful to David Ring for providing editorial assistance and for his critical evaluation of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical approval
Not applicable.
Informed consent
Not applicable.