
Abstract
Introduction:
Radial polydactyly is often underestimated in its complexity. While many cases can be managed by excision and reconstruction of a dominant thumb, suboptimal outcomes persist when soft-tissue imbalance or bony deviation is not fully addressed. Expectations for aesthetic symmetry have also increased, placing greater demands on surgical precision and judgement.
Limitations of current approaches and classifications:
In cases where both duplicates are small (typically <70% of the contralateral thumb), achieving adequate thumb girth and a satisfactory nail complex frequently requires augmentation or combined procedures. Traditional techniques such as the Bilhaut–Cloquet procedure, although conceptually elegant, may result in split nail deformity, joint stiffness, and excessive bulk. Likewise, the Wassel–Flatt classification, despite its widespread use, does not adequately capture soft-tissue anomalies, axial deviation, or triphalangeal components, limiting its value for operative planning.
A proposed classification and surgical philosophy:
We present a simplified, two-group classification derived from decades of cumulative clinical experience. This framework integrates key anatomical and morphological factors, including size discrepancy, axis deviation, soft-tissue quality and nail deformity, to guide surgical strategy. It incorporates both transverse (modified Bilhaut–Cloquet) and longitudinal (on-top plasty) reconstructive concepts, as well as combinations of these techniques where required. This approach also recogizes the need for a comprehensive surgical skillset, including paediatric orthoplastic and microsurgical expertise for optimal refinement.
Conclusion:
This pragmatic classification aims to address at least 95% of cases with radial polydactyly configurations, while remaining intuitive for clinical use. It provides a structured approach to surgical planning, communication, and outcome assessment, and should be applicable. By aligning anatomical complexity with tailored reconstruction, it supports more consistent functional and aesthetic outcomes.
Level of evidence:
V
Keywords
Introduction
Radial polydactyly (RP) remains one of the most common types of congenital hand differences (Chung et al., 2013; Khabyeh-Hasbani et al., 2022; Manske et al., 2017). In Asia, RP has probably surpassed syndactyly as the most common condition encountered by surgeons (Yeh et al., 2025). Globally, the Wassel–Flatt classification remains the predominant system for categorizing RP; nevertheless, as clinical experience increased, there has been a corresponding rise in reports highlighting perceived limitations in Wassel’s original description. This is unsurprising, as a system based solely on radiological levels of duplication lacks information about the extent of soft-tissue and tendinous variability and the degree of skeletal deformities, such as hypoplasia or deviation. Consequently, the classification provides little or no guidance for surgical decision-making.
Many modifications have been made to the original Wassel–Flatt system to address increasingly diverse or atypical presentations and to provide more clinically relevant guidance for surgical management (Dijkman et al., 2014; Kim et al., 2021; Wood, 1978; Zuidam et al., 2008). Although these modifications have led to more comprehensive classifications, the literature has not yet established a common language. Moreover, these modified classifications are becoming increasingly complex, making them harder for surgeons to remember and apply. The question remains whether we can consolidate our experiences and develop a unifying yet simplified framework to classify and manage RP.
This article draws on cumulative experience from different institutions to develop a unified approach. It raises key philosophical questions to encourage discussion and challenge dogma. A simplified algorithm, based on our experience and the literature, is presented for systematically managing the different types of deformities. For each subtype, we present pearls and pitfalls to achieve optimal results. It is hoped that this new, streamlined classification will help us progress toward a unified approach to surgically managing all RP of the duplicate configuration.
Relevance of the Wassel–Flatt classification system
The discussion inevitably needs to start with the Wassel–Flatt system. Initially described in 1969 (Wassel, 1969), the system has stood the test of time and been cited in almost every article on RP, probably because of its simplicity. Herein lies the problem. A radiological system based on the level of duplication, without regard for soft-tissue abnormalities, the size of duplicates or the degree of hypoplasia, may mislead one into thinking that RP is deceptively simple to manage, but it is most definitely not (Tian and Chen, 2020). The surgery should not be undertaken by the occasional hand surgeon or even by most hand surgeons who do not regularly perform paediatric hand surgery. Surgical management of RP requires not only addressing the skeletal duplication but also managing the complex soft-tissue and tendon abnormalities and performing realignment osteotomies in small skeletons. Furthermore, achieving a higher level of aesthetic refinement requires microsurgical skills to raise small island flaps and reconstruct nail beds in complex cases.
Without insight into the complex anatomy and biomechanics of the deformities, complications are prone to occur and can be very challenging to correct (Hovius and Kruit, 2024). This is especially true for RP cases with preoperative deviations at either the metacarpophalangeal or interphalangeal joints. However, even a seemingly innocent configuration, such as a ‘simple’ pedunculated hypoplastic duplicate, may present with future deviations if aberrant tendons are not addressed (Saito and Morimoto, 2021). In other words, there is a need to discuss whether the Wassel–Flatt system, based solely on a numerical grading system dependent on the level of duplication, can be reliably improved or should instead be replaced.
What is needed among surgeons is a system that systematically assesses all aspects of the deformity, uses descriptive terms that surgeons can immediately understand and provides a practical, reliable guide for surgery: excision, combination procedures (both transverse and longitudinal on-top plasty) or their combination, if necessary. Having this information allows one to work backwards to provide a holistic, pragmatic classification system applicable to all ‘duplicate’ RP cases. Such an approach has probably been attempted and hinted at in various publications (Kim et al., 2021; Tian and Chen, 2020; Wang et al., 2021), but to date, there has not been universal agreement on a single system (Tonkin, 2021).
Are we focusing on the wrong outcome measures?
Another area we must address is the definition of a good surgical outcome for RP. Various studies use the Tada scoring system (Al-Qattan et al., 2017; Maillet et al., 2007; Monjardino et al., 2023; Stutz et al., 2014). Widely considered one of the most structured and condition-specific scoring systems available, it evaluates alignment, stability and mobility using predefined parameters to produce a comprehensive overall score. The way the results are reported highlights a common problem in hand surgery research: dichotomization (Harvey et al., 2023). While a certain level of dichotomization is necessary in research and useful for producing a score, the final number of ‘Tada points’ may be meaningless to the parent or child, whose priorities may be completely different. Additionally, the Tada score misses one very important component: appearance. The importance of patient-reported outcome measures should be emphasized, although challenges remain in the paediatric literature. Patient-Reported Outcomes Measure Information System (PROMIS) and the Pediatric Outcomes Data Collection Instrument (PODCI) are well validated, but they may not be sufficiently condition specific for RP.
The importance of appearance
Outcomes in hand surgery have long focused on functional improvement such as strength, mobility or range of motion. This has heavily influenced how we measure outcomes in congenital hand surgery. Based on our experience and recent literature (Nietosvaara et al., 2021; Werner et al., 2022), there is a growing focus on appearance among parents. This is also true for other congenital hand conditions, such as hypoplastic thumb reconstruction. In the author’s own experience, parents would often choose to reconstruct a severely hypoplastic thumb rather than agree to a pollicization, because the appearance of a five-fingered hand, even with a stiffer, smaller reconstructed thumb, is considered more important than a ‘functionally superior’ pollicized thumb and a resultant four-digit hand (Liu et al., 2021).
What are the important aesthetic elements in RP? Following an excision procedure, the importance of achieving proper thumb alignment, i.e. a straight thumb, is recognized as the most important thing for parents (Hovius and Kruit, 2024). This reinforces the priority of producing a visually pleasing result, since a deviated thumb is easily noticed by both parent and child. The established techniques to ensure correct alignment during the initial surgery are well known, e.g. osteotomy, tendon balancing, etc., and should always be adopted during the primary surgery.
Besides alignment, there is growing recognition of the importance of thumb girth and nail appearance. Achieving a reconstructed thumb with a girth, in terms of nail or interphalangeal joint width, that is comparable to that of the contralateral thumb or, at a minimum, matching the index finger has become an increasingly crucial objective in RP surgery. Most cases of thumb polydactyly present with at least one underdeveloped thumb. Unlike thumb hypoplasia, in which augmentation is extremely challenging or nearly impossible, the vast majority of RP cases may be reconstructed using combination techniques to achieve an appearance close to that of a normal thumb.
Given these inherent anatomical advantages in RP, pursuing an optimal cosmetic appearance is a feasible and ideal surgical strategy and therefore should be pursued. However, combination procedures have traditionally earned a bad reputation, as methods that use components from the excised duplicate, such as the Bilhaut–Cloquet (BC) procedure, are often associated with pronounced scarring, joint stiffness and nail deformities (Tonkin and Bulstrode, 2007). Nonetheless, recent efforts by colleagues to achieve optimal outcomes using modified combination techniques have been promising (Liu et al., 2026; Sriswadpong et al., 2026). It remains debated whether every paediatric hand surgeon can replicate these results.
A simplified classification – overview
Drawing from these two main discussion areas – meaningful elaboration of the simplicity of the Wassel–Flatt system and a focus on postoperative aesthetics – we aimed to create a more streamlined system. A general overview of our proposed system is shown in Figure 1. A systematic approach can be employed when implementing this system to guide surgical management of RP as follows:
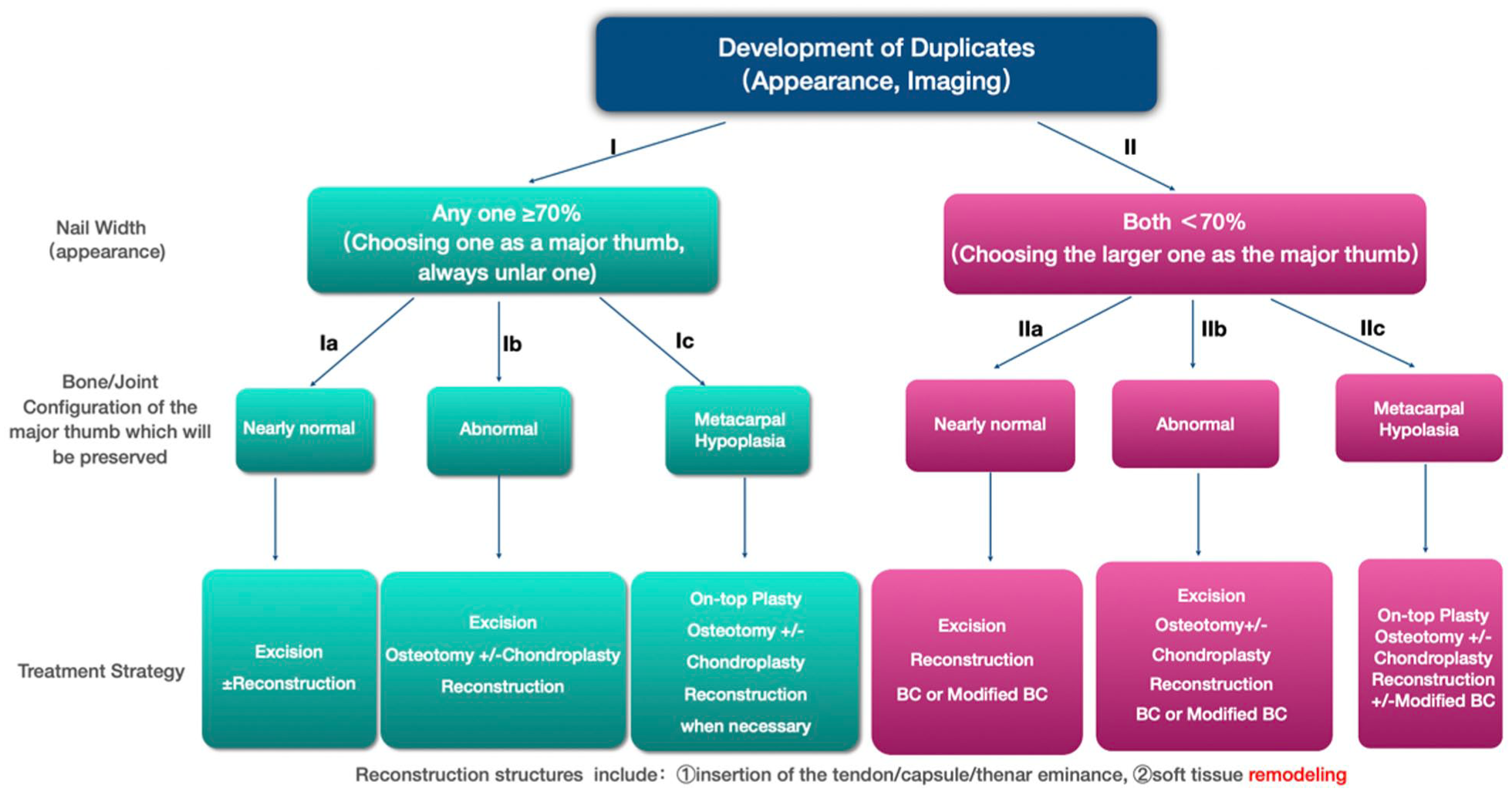
A proposed algorithm for management of radial polydactyly (RP).
Step 1: Assess whether the width of the nail and interphalangeal joint of at least one duplicate thumb in this RP is > or < 70% of the contralateral thumb, thereby dividing the RP into one of two major groups. The division into these two groups is deliberate: in Group I, an excision method (with reconstruction) is usually sufficient but in Group II, a combination method may be needed to achieve optimal results.
Step 2: Assess the configuration of the dominant duplicate in terms of the bone/joint and overall alignment. This would further divide the RP into either a ‘near normal’ or an ‘abnormal’ subgroup. Then, assess the proximal skeletal morphology of the duplicates. If there is a degree of metacarpal hypoplasia in one of the thumbs that is more developed distally, then an on-top-plasty may be needed.
Step 3: Final matching and recommendation of a surgical procedure for the RP within its particular subgroup.
A few other comments should be made: (1) we have moved away from the Wassel–Flatt system to de-emphasize the importance of the level of duplication; (2) a degree of dichotomization is necessary to simplify the algorithm but small nuances remain which will be discussed; and (3) this system assumes one is willing to perform a combination method (and possesses the necessary skillsets) to obtain better symmetry when neither thumb seems sufficient for reconstruction on its own.
This algorithm should allow surgeons to manage at least 95% of duplicate RP cases, even the more uncommon configurations, as the focus is on basic principles rather than a prescribed technique for each subtype.
Group I: at least one of the duplicates is >70% (nail width or interphalangeal joint) of the contralateral thumb
This constitutes the majority of RP cases encountered in clinical practice where an excise and reconstruct technique is typically employed (Dijkman et al., 2016; Wall and Goldfarb, 2015) as the remnant thumb is >70% of the contralateral thumb. If the child has bilateral RP, the index finger can serve as a guide.
Group Ia: a ‘nearly normal’ bone/joint configuration in the dominant thumb
In these cases, one duplicate has a bone/joint morphology that is nearly normal in overall size, alignment and nail appearance, allowing it to be clearly selected for preservation (Figures 2 and 3). Slight deviation may be present, but this is usually less than 20°, and osteotomy is usually not needed (Lee et al., 2013). The emphasis here should be on the morphology of the dominant thumb that is to be preserved. We do not see the need to further subdivide this group based on the condition of the removed duplicate, even if it is hypoplastic (Figure 2), as has been suggested by others (Kim et al., 2021).
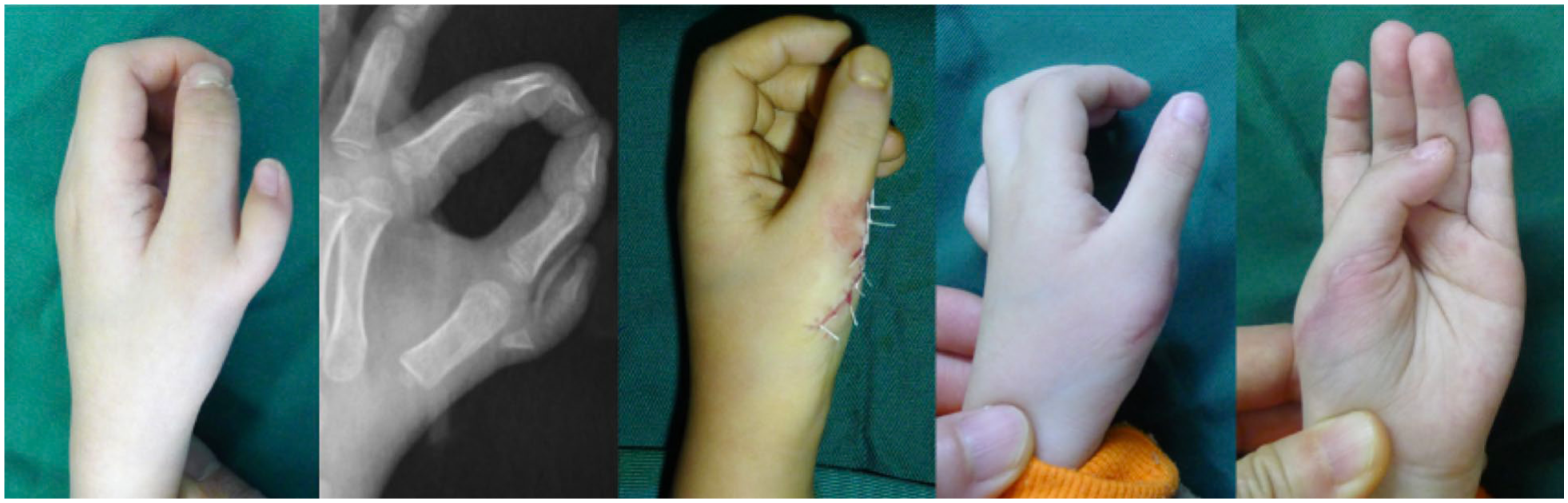
In this Group Ia patient (age at surgery 3 years, postoperative 4 months), the ulnar duplicate was >70% of the contralateral thumb and the severely hypoplastic radial duplicate was excised. It was essential to check for aberrant tendons, especially in broader attachments, as failure to excise these could lead to future deviations.

In this Group Ia patient (age at surgery 9 months, postoperative 4 years), both duplicates were >70%, and the ulnar one was preserved. It is important to note that this is not simply a soft tissue procedure to improve the appearance but also involves reconstruction of the joint capsule and collateral ligaments. Vertical mattress sutures were used to produce an inverted lateral fold.
Group Ib: an ‘abnormal’ bone/joint configuration in the dominant thumb
In these cases, one or both duplicates are still >70% of the contralateral thumb, but the thumb to be preserved has an abnormal morphology, mainly in alignment. One duplicate can be safely removed via a traditional ‘excise and reconstruct’ approach, rather than a combination method. However, more attention is needed to restore the alignment of the remnant duplicate (Figures 4 and 5). In general, a deviation of more than 20–30° is an indication for osteotomy (Lee et al., 2013).
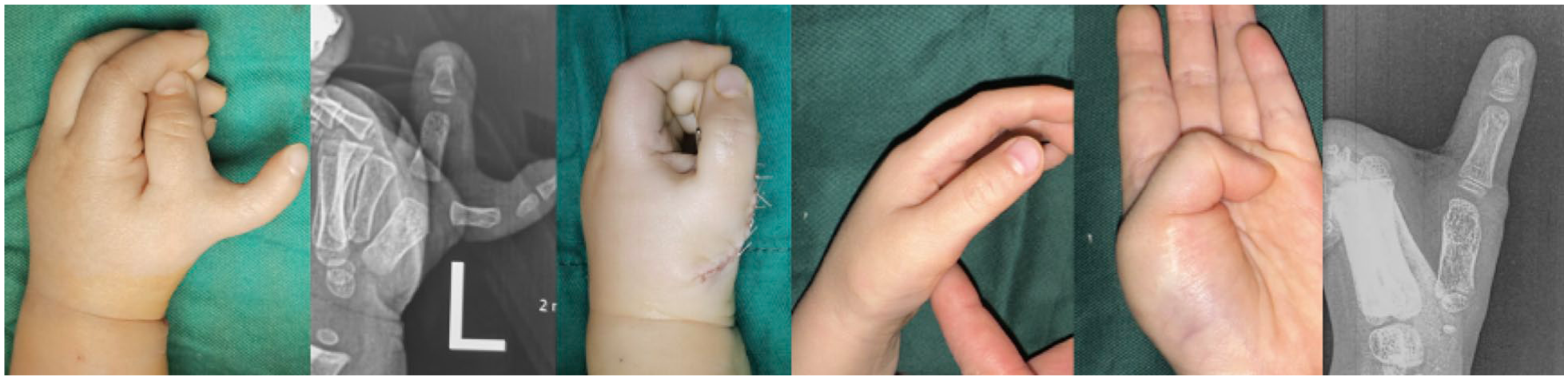
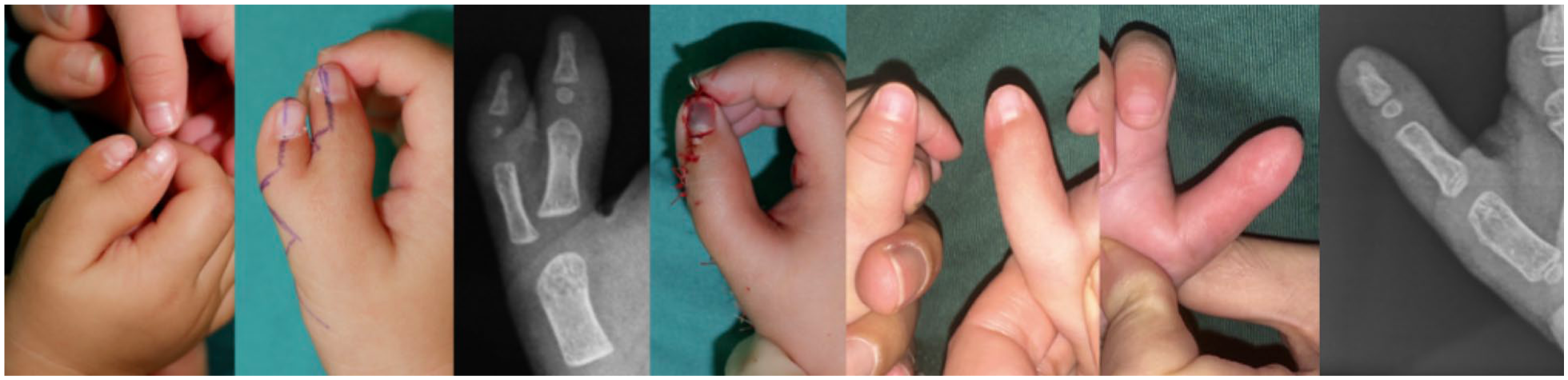
In this Group Ib patient (age at surgery 1 year, postoperative 3 years 2 months), there was significant ulnar deviation of the ulnar duplicate. Excision of the radial duplicate necessitated a formal closing wedge osteotomy, tendon realignment and reconstruction of the APB/RCL complex. The first web space also required assessment and, if necessary, widening. APB/RCL: abductor pollicis brevis/radial collateral ligament.

In this Group Ib patient (age at surgery 1 year, postoperative 3 years), the ulnar duplicate was the main thumb, and the nail was >70% of the contralateral side, but the bone and joint were significantly deviated, with a divergent–convergent pattern. The key to the surgery lay in chondroplasty performed at the distal end of the metacarpal bone and reconstruction of the APB/RCL complex. At the distal end of the proximal phalanx, open bone grafting was carried out on the radial side, and the collateral ligament of the joint capsule was tightened on the ulnar side. Finally, Kirschner wires were used to fix the interphalangeal joint to over-correct the radial deviation. APB/RCL: abductor pollicis brevis/radial collateral ligament.
Group Ic: metacarpal hypoplasia in the thumb that is more developed distally
These cases are very rare in our experience. Although one duplicate has a distal width of >70% when compared with the contralateral thumb, radiographs reveal that its proximal metacarpal is severely hypoplastic and floating, whereas the other has a severely hypoplastic distal element but a better-formed proximal element. In these instances, a standard on-top plasty is necessary to achieve optimal results (Figure 6).

In this Group Ic patient (age at surgery 3 years, postoperative 5 months), an on-top plasty was performed, where the ulnar duplicate was transferred to the radial duplicate. At the level of the proximal phalanx, the distal phalanx fracture end was trimmed and then inserted into the proximal phalanx fracture end, with a K-wire used for fixation. No nail reconstruction was needed as the distal ulnar duplicate was >70% of the contralateral thumb.
Surgical technique of on-top plasty
The on-top plasty is technically demanding and should be performed by paediatric hand surgeons experienced in pollicization procedures. Preoperatively, the level of the proposed osteosynthesis between the duplicates is marked. As far as possible, this should be at the proximal phalangeal level, as preserving the native metacarpophalangeal joint is advantageous because it leaves the collateral ligaments intact. Circumferential incisions are made on both thumbs for the transfer. On the more dominant distal duplicate, both the venous supply and neurovascular bundles are isolated and preserved for mobilization, similar to a pollicization. We advocate dividing and repairing the distal and proximal flexor/extensor tendons to reduce bulk. Although gliding in the repaired flexor tendons may be limited by scar adhesions and might not effectively flex the interphalangeal joint, they can still be adequately tensioned to preserve the normal balance of flexion and extension strength of the thumb. Osteosynthesis is usually performed with a K-wire. Following a transfer, it is important to ensure pulp-to pulp pinch with the rest of the digits (Figure 6).
Group II: both duplicates are <70% of the contralateral thumb
Achieving alignment is of the utmost priority; however, obtaining a thumb as symmetrical as possible to the contralateral thumb has become increasingly important to parents (Liu et al., 2026; Sriswadpong et al., 2026). In Group II cases, where both duplicates are <70% of the contralateral thumb (or index finger) in terms of the nail and interphalangeal width, we find it necessary to perform, or at least consider, some form of combination surgery to produce a more pleasing result. The challenges are to avoid nail deformities, preserve motion and avoid any growth disturbances.
Strategies to increase nail diameters
History
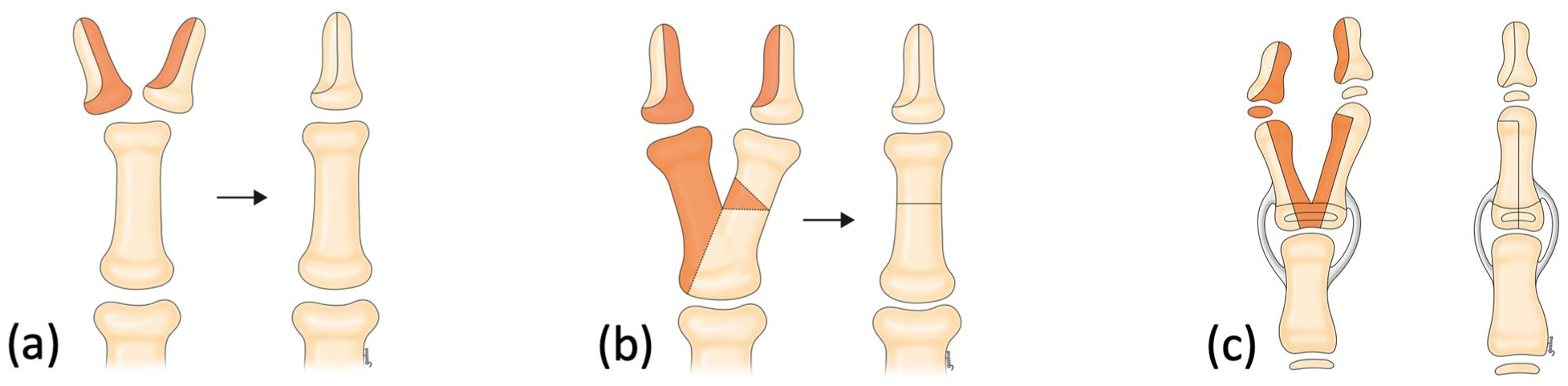
The BC procedure was first described in 1889 (Bilhaut, 1889) and is considered the precursor to all subsequent combination techniques for augmenting nail diameter. However, many now consider this a historical procedure because of the risks of nail deformity, growth disturbance and prominence of pulp scarring (Tonkin and Bulstrode, 2007). Joint stiffness is also considered unavoidable because the two hemi-joints are osteosynthesized together to form a single articulating joint (Figure 7).

The traditional Bilhaut–Cloquet procedure is shown, where complications such as (a) a nail ridge deformity, (b) a bulky thumb and (c) joint stiffness are almost inevitable.
Baek et al. (2007) described their modification of the BC procedure, which has since been widely adopted. In their description, one nail bed is preserved predominantly with its underlying distal phalanx, while most of the nail bed of the other duplicate is excised to minimize nail bed scarring. Also, only one joint is preserved and the other is removed, thus maintaining joint motion. Achieving this requires combining only non-articular bony elements (Figure 8). In addition, all elements of alignment surgery proximally are respected, including primary osteotomies and centralization of tendons, if necessary. Although the reconstruction principles for bony and nail bed reconstruction are robust, their description provides minimal detail about the skin incision. Similarly, Baek et al. (2007) did not mention employing an islanded neurovascular flap.
Baek’s modified Bilhaut–Cloquet procedure is illustrated. (a) In the distal phalanx, he described preserving only one joint, while the other was removed except for a small sliver of bone, thus maintaining joint motion. Osteotomy and combination of the proximal phalanges were performed as necessary (b, c).
To improve thumb girth, not every author chooses to combine the nail beds. Horii et al. (2009) and then Dautel and Perrin (2015) described the use of a proximally based ‘U’ flap from the excised duplicate to augment the radial side of the remnant thumb. No reconstruction of the distal phalanx or nail bed was made. These procedures result in two longitudinal scars that run along the side of the thumb, which may be unsightly. Also, the nail bed may be too narrow, as only one is preserved.
Mak et al. (2021) described the use of an islanded neurovascular island flap rather than a proximally based flap to augment the thumb tip. Although more detailed dissection is needed with an increased risk of avascularity in the transferred flap, the procedure yielded better aesthetics by placing a single scar along the radial aspect of the thumb. Part of the nail bed is also taken with the flap and combined with the remnant nail bed to provide a wider nail. Importantly, Mak et al. (2021) highlighted the importance of paying meticulous attention to nail bed reconstruction with 9–0 sutures to minimize the risk of nail deformities.
In our experience, if the nails are separate, almost every case can be treated using Baek’s modification of osteosynthesis with a neurovascular island flap. Reliable outcomes can be achieved with thumbs that maintain a reasonable range of motion, reduced scarring, and an optimal nail width. In addition, if the distal phalanx of the remaining thumb is well developed and the nail is only slightly smaller than 70% of the size of the contralateral side, a neurovascular island nail flap can be harvested with only a small sliver of bone or no bone at all without compromising function or causing nail deformities. This can effectively prevent the postoperative appearance of a bulky thumb.
A few technical points are important, such as repairing the nail bed with microsutures and approximating the germinal matrix carefully. The postoperative thumb girth should be made slightly smaller rather than larger, as it tends to stretch. Finally, any ‘J-shaped’ deformity of the paronychium needs to be excised so that a final pleasing proximal ‘U’ flap eponychia fold can be reliably achieved with a neurovascular island flap (Figure 9).

A Group IIa patient with a ‘J-shaped’ deformity of the paronychium was observed. The upward slope of the proximal nail fold in both duplicates was noted. These required excision and reconstruction with a neurovascular island flap to produce a proximal ‘U’-shaped eponychial fold.
When should we perform a traditional BC procedure?
Although the BC procedure is considered historical, there are still valid indications for its use. When the nails are jointed together, i.e. a ‘big nail’, it does not make sense to perform a neurovascular island flap from one thumb. In these situations, the only way to narrow the thumb may be to perform a central wedge excision of the skin and nail bed (Figure 9). Following soft-tissue excisions, a longitudinal split through the joint is needed to mobilize the two distal phalanges together, which are then fixed transversely with a K-wire. The traditional BC should be performed only by highly experienced congenital hand surgeons. A degree of joint stiffness should be expected, but hopefully nail deformities can be avoided with meticulous suturing. Some may choose not to operate on patients with a big nail, but if the parents insist, then the limitations of a traditional BC should be explained (Figure 10).

In this patient, two symmetrical duplicates were closely joined to form a ‘big nail’. A traditional Bilhaut–Cloquet procedure may have been the only option to reduce the width.
Group IIa: a ‘nearly normal’ duplicate (bone/joint configuration) although it is <70% of the contralateral thumb
These cases are also uncommon in our experience and are usually Wassel–Flatt II or III cases. Excision of one duplicate followed by Baek’s modification of the BC with a neurovascular island flap should be performed in most of these cases (Figure 11).

In this Group IIa patient with a Wassel–Flatt III patient (age at surgery 1 year 4 months, postoperative 10 months), both duplicates were <70%. The ulnar duplicate had a bone/joint configuration that was ‘nearly normal’, was chosen as the preserved duplicate and was augmented with Baek’s modification of the Bilhaut–Cloquet procedure using a neurovascular island flap. The proximal phalanges were also combined distally.
Group IIb: an ‘abnormal’ duplicate (bone/joint configuration) that is <70% of the contralateral thumb
In our experience, these cases are relatively common and often exhibit a divergent–convergent configuration. Most are Wassel–Flatt IV cases in which one duplicate would be excised, but significant alignment surgeries would be required to achieve a straight thumb. In addition, combination procedures with a neurovascular island flap is necessary, as the preserved duplicate on its own would be too small (Figures 12 and 13).
A Group IIb or Wassel–Flatt IV patient (age at surgery 1 year 8 months, postoperative 8 months) with a divergent convergent pattern, where excision of the radial duplicate with alignment of the ulnar duplicate alone would have been insufficient, as the preserved thumb would have been too small. Therefore, a modification of the Bilhaut–Cloquet procedure, with a neurovascular island flap and only a small sliver of bone, was added.

A Group IIb or Wassel–Flatt IV patient (age at surgery 10 months, postoperative 6 months). In this instance, the ulnar duplicate had a better morphology, but the nail was still insufficient on its own, so a neurovascular island nail flap without bone from the radial duplicate was transferred to the retained thumb to enlarge the nail and finger body (modified Bilhaut–Cloquet procedure).
Group IIc: metacarpal hypoplasia in the thumb that is more developed distally and <70% of the contralateral thumb
Although complex, these cases are actually not too uncommon. Similar to Group Ic cases, one duplicate has well-formed distal bone/joint components, but the proximal metacarpal is severely hypoplastic and floating, whereas the other has a severely hypoplastic distal element but a more well-formed proximal metacarpal. An on-top plasty is needed, but also a distal combination surgery to augment the girth. These cases are probably the most technically challenging, as both a longitudinal (on-top plasty) and a transverse (neurovascular island flap) reconstruction are needed to achieve optimal results. In addition, alignment surgery should also be performed, if needed, to produce a straight thumb (Figures 14 and 15).

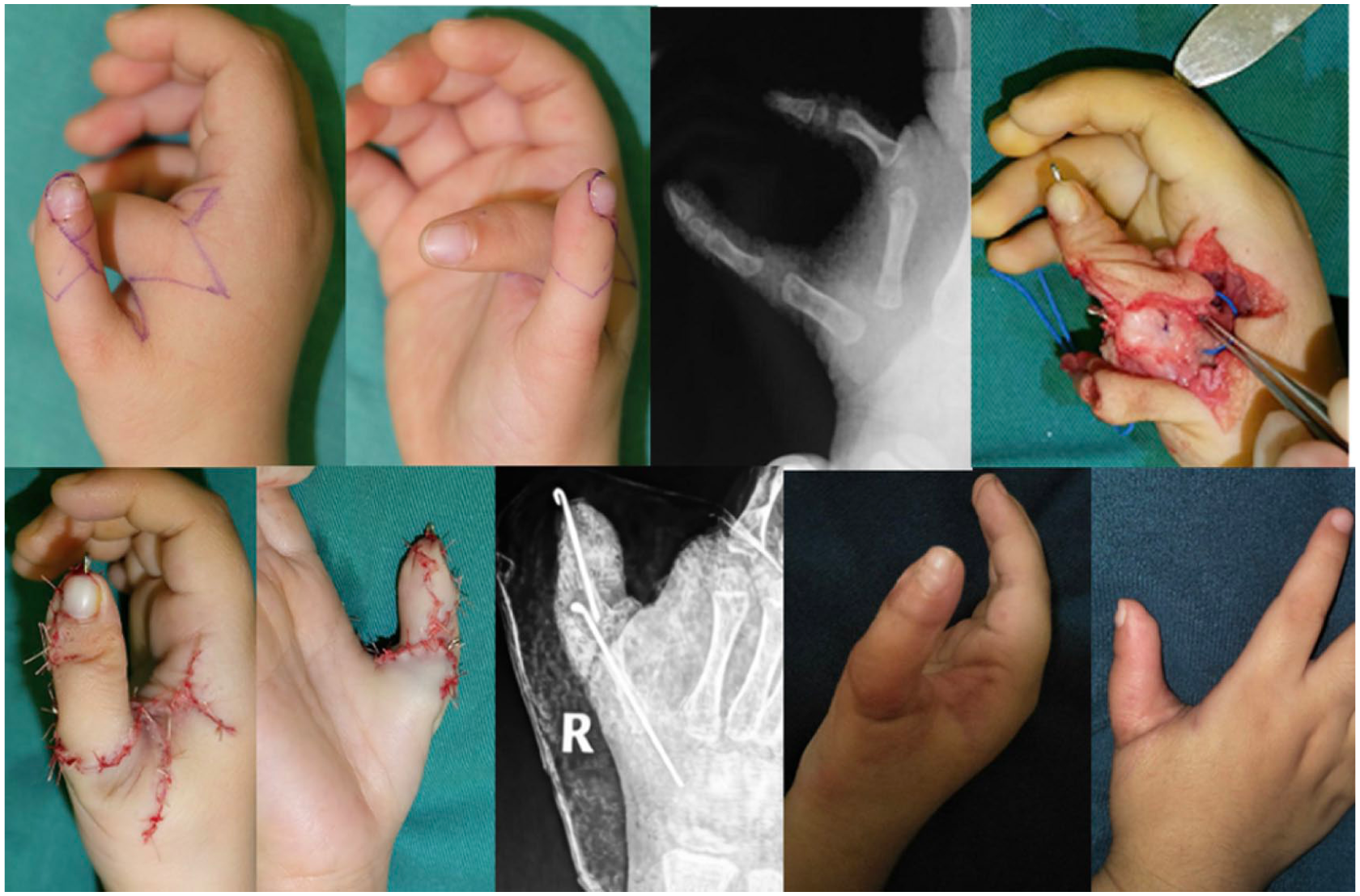
A Group IIc or Wassel–Flatt VI patient (age at surgery 1 year 7 months, postoperative 1 year 4 months). A combination of all the techniques described was necessary, including an on-top plasty, Baek’s modification of the Bilhaut–Cloquet procedure with a neurovascular island flap and an opening wedge osteotomy to correct the deviation.
A Group IIc or Wassel–Flatt VI patient (age at surgery 4 years 4 months, postoperative 2 years). Again, a combination of different techniques was necessary, including an on-top plasty. However, in this instance, only soft tissue augmentation of the transferred ulnar duplicate was performed, as the radial duplicate had a hook-shaped nail and was suboptimal to be raised as a nail complex.
Discussion
Tonkin et al. (2013) previously described the criteria for an ideal classification in congenital hand differences. It should give some indications as to the cause and the site where the aberration occurs in the molecular or anatomical pathway, utilize a reproducible and consistent terminology, use a universal language for discussion of complex clinical entities and finally, provide indications for treatment and a comparison of results for the collection of incidence and prevalence rates.
It can be argued that the Wassel–Flatt classification falls short of these criteria in many ways. While it may be useful for general communication in uncomplicated cases, the system is unable to account for configurations that are not simple or straightforward (Figure 16). For example, it does not comprehensively account for variations in soft-tissue abnormalities. In terms of skeletal duplication, the classification fails to adequately describe a triphalangeal component at any level, or account for an abnormal proximal phalanx or metacarpal where realignment bony or tendon surgery would be required. For severely hypoplastic duplicates such as a floating thumb, one can argue that the duplication level becomes entirely irrelevant, as the management would be to simply excise the duplicate.
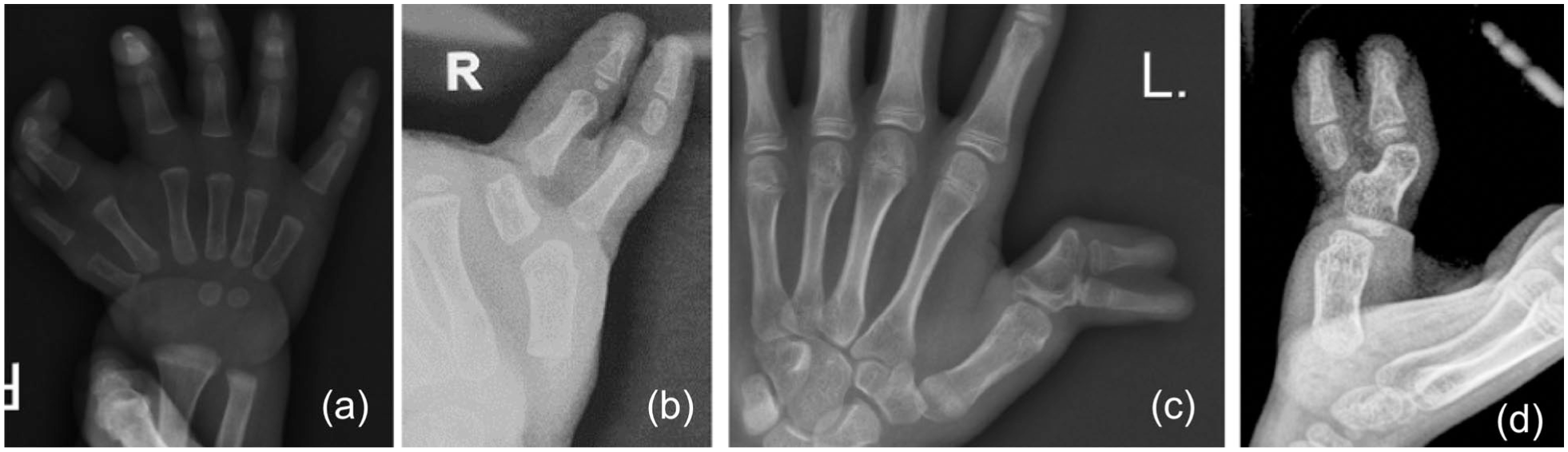
Different cases are presented to illustrate the limitations of the Wassel–Flatt classification including: (a, b) triphalangeal; (c, d) abnormal epiphyses; (d) hypoplastic and other asymmetrical morphology were not considered, despite each case being assigned a level of duplication.
With such limitations, one wonders whether classifying RP using the Wassel–Flatt classification is often more of an academic exercise, which has little practical application in real life. When approaching a new case, the surgeon is immediately drawn to the procedures required to achieve the final objective of a well-aligned, aesthetically pleasing thumb. One would first consider whether an ‘excise and reconstruct’ or a combination method should be employed, and also whether a realignment surgery via a primary osteotomy or tendon centralization is needed. It would soon become apparent that the level of duplication using the Wassel–Flatt classification may be clinically irrelevant in these thought processes.
Over the last few decades, the true prevalence of RP has become increasingly clear. It has overtaken syndactyly as the most common hand difference, especially on the Asian continent (Yeh et al., 2025). The demands of achieving better results are also increasingly recognized, as are its challenges. A unifying approach that accounts for the management of all the various manifestations of RP is much needed but remains lacking.
In this article, we present an approach that simplifies a highly complex condition, creating an algorithm that is accessible and practical for all surgeons. To achieve this, it was essential to have oversight of the broad range of presentations and a depth of understanding of the complexity of the problem. To design this algorithm, experience was collected from a few institutions over several years, encompassing at least 3000 cases. We also believe in the importance of transparency about the skills required to achieve optimal aesthetic results: a surgeon should be an experienced paediatric hand specialist, proficient in bony and soft-tissue procedures in the small hand, as well as in microsurgery. Possessing these skills enables the surgeon to adapt and apply different techniques, such as ‘excise and reconstruct’ or ‘combination’ (either transverse or longitudinal), or to integrate multiple methods when required. Surgeons should also understand what matters most to parents. Increasingly, our foremost priority is appearance. After appearance, the next thing parents care about is function, and finally, radiographic appearance. This order of priority may differ for surgeons, but perhaps a change in thinking is necessary if surgeons are to strive for the appearance as their first goal.
To achieve optimal aesthetic outcomes, alignment remains the most important objective, but increasingly, a good outcome must include a final thumb diameter that is at least comparable with that of the contralateral thumb. In our experience, surgeons often compromise on the final diameter appearance, as achieving symmetry in duplicates <70% often requires a combination procedure, which remains highly unpopular owing to the technical skills required. In a matched comparative study, Dijkman et al. (2016) recommended that conventional resection techniques should be the preferred procedure until proven otherwise, after reporting worse aesthetic results with the BC procedure. It is worth noting that the study lacked details of the surgical techniques, although the images suggest that incisions that produced prominent dorsal scarring were used, which may have influenced the results. Also, the authors admitted that, in the linear-mixed model analysis, the poorer results relate mainly to nail appearance rather than overall diameter. Nail appearances mainly relate to a post-operative split nail deformity. However, in our experience, meticulous reconstruction of the nail bed with microsutures tends to significantly reduce this complication or eliminate it completely.
In our experience, the use of a neurovascular island flap has revolutionized the reconstruction of thumbs that are <70% of the contralateral thumb. These flaps are versatile and can be customized to reconstruct the amount of soft tissue needed for augmentation. They can also be configured to correct any ‘J-shaped’ eponychial deformities. In addition, the use of a flap allows a length mismatch between two duplicates to be addressed as it can be easily mobilized to reach the tip of the remnant thumb and restore symmetry. Liu et al. (2026) recently described an algorithm for Wassel III thumb using Baek’s osteosynthesis and a neurovascular island flap. They also recommended an osteotomy of the duplicated proximal phalanges if their combined diameter exceeds the metacarpal width by a ratio of >1.3. Other modifications by the same team include the use of a larger ‘boot-shaped’ flap incision to improve the contours of the thumb tip (Shen et al., 2020). By paying attention to these small details, an aesthetically pleasing result should be achievable in most cases.
Tonkin (2021), in his final comments on the growing number of newly introduced classifications for RP noted that ‘perhaps it is an error to demand too much of our classifications, . . . and that surgical management dictated by classification type may never allow a full consideration of all anatomical variations found in thumb duplications’. This is probably true, but in this article, we have attempted to share a simplified classification that may bring us a step closer towards a unifying approach to managing at least 95% of all RP cases of the duplicate configuration. When developing this algorithm, references to the Wassel–Flatt classification have been deliberately minimized, as the emphasis is on adhering to core principles and addressing what is missing or abnormal, rather than the extent of duplication. Finally, it is important to emphasize the need for meticulous attention to postoperative care, including bandaging and scar management, in order to achieve better longer-term results.
As with any new system, this would require evaluation and acceptance by the broader surgical community before becoming standard practice (Lam, 2025). Our proposed algorithm welcomes feedback and suggestions, especially regarding clearer language for group descriptions. Ideally, future studies will adopt this pragmatic method, focusing on comparing techniques within these broader categories, rather than making less meaningful comparisons between highly varied thumbs within the same Wassel–Flatt groups.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval declaration
Ethical approval was not sought for this article as there was no review of patient data.
Informed consent declaration
All authors were involved in study development and drafting/writing of the final manuscript.