
Abstract
Persistent trigger finger distally to the A2 pulley after A1 pulley release is uncommon. We report five fingers in four patients successfully treated using a stepwise approach including A1 pulley release, ulnar flexor digitorum superficialis slip excision and flexor tenoplasty.
Trigger finger is a common condition in hand surgery caused by a mismatch between the size of the flexor tendons and the finger pulley system. Patients who are refractory to non-surgical treatments require A1 pulley release. However, in rare cases, persistent or recurrent triggering distally to the A2 pulley may occur despite adequate release, thereby necessitating additional procedures. This report presents our stepwise surgical strategy for persistent or recurrent triggering and the outcomes.
Our approach consists of three steps: (1) A1 pulley release or confirmation in recurrent cases; (2) ulnar superficialis slip excision (USSE) of the flexor digitorum superficialis; and (3) reduction flexor tenoplasty (RFT) of the flexor digitorum profundus (FDP) tendon (Figure 1). After each step, intraoperative active finger motion is assessed, and the next step is performed if triggering persists. All procedures are performed under local anaesthesia with a tourniquet on the upper arm. When active motion is hindered by tourniquet-induced ischaemia, the tourniquet is released. In step 1, we create an oblique skin incision over the A1 pulley and release the pulley up to the proximal third of the A2 pulley. This extended release is the standard surgical treatment of our institution for all trigger fingers. For recurrent cases, we release the reconstituted A1 pulley. If triggering is still apparent, we extend the incision and dissect distally to A2 pulley. In step 2, we open the C1 pulley to examine the flexor tendons. The tendons are usually found to be enlarged distally to the A2 pulley. Once triggering at this level is confirmed, we perform USSE by resection from the bifurcation proximally to phalangeal insertion. In step 3, if triggering still occurs, we perform RFT. We resect a central, enlarged portion of the FDP tendon longitudinally until triggering resolves. The gap in the FDP tendon is not sutured.
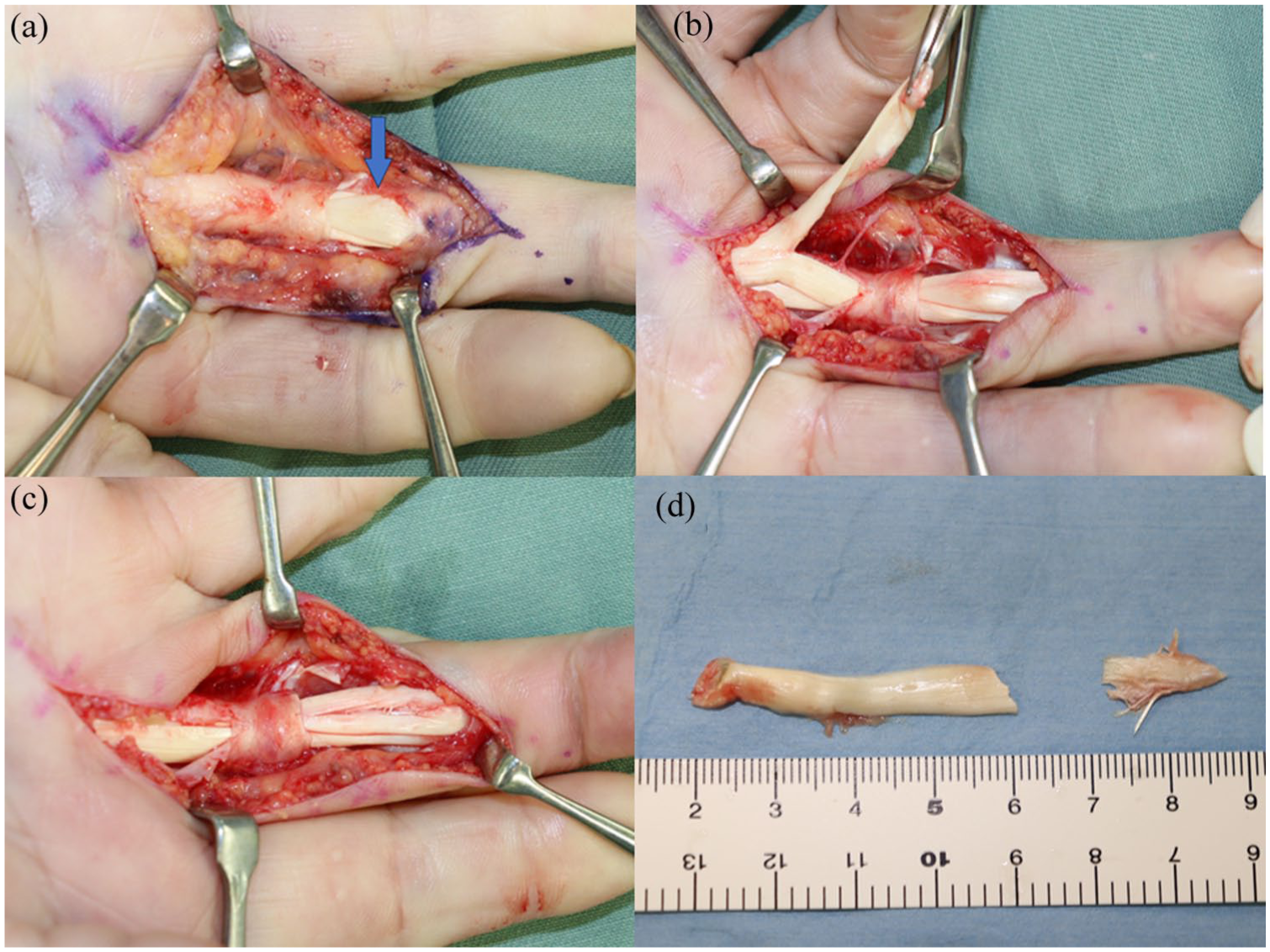
(a) Intraoperative photograph showing fusiform enlargement of the flexor digitorum profundus (FDP) tendon (arrow) distally to the A2 pulley. (b) Resection of the ulnar slip of the flexor digitorum superficialis (FDS). (c) Resection of the central portion of the FDP. (d) Resected FDS slip and FDP segment.
We assessed outcomes of patients who needed a procedure for recurrent trigger finger. All patients provided written informed consent, and the study was approved by the institutional review board. Among 431 fingers in 309 patients who underwent A1 pulley release between 2018 and 2025, five fingers in four patients required additional surgery (1.2%). The cohort included two women and two men, with a median age of 69 years (IQR, 64–69) at the time of definitive surgery. The affected fingers comprised four middle fingers and one ring finger, with four on the right side. Two patients had diabetes mellitus. The median duration of symptoms from onset to final surgery was 45 months (IQR, 7–108). All patients had a history of multiple trigger fingers: ten fingers in one patient, nine fingers in two patients, and eight fingers in one patient. The median follow-up period was 8 months (IQR, 6–10). One finger showed reduced but persistent triggering after A1 pulley release and subsequently underwent USSE. The other four fingers initially showed resolution of triggering after A1 pulley release but it recurred at 2 months; one of them resolved by USSE, and the other three additionally required RFT. All cases had tenderness at the midpoint of the proximal phalanx before revision surgery, except the primary case, for which this was not assessed. Intraoperative findings revealed no evidence of tendon wear, but hypertrophy of the FDP distally to the A2 pulley and thickening of the distal portion of the A2 pulley were observed. All patients ultimately had relief of pain and triggering at final follow-up. The median active range of motion of the proximal interphalangeal joint was 0° (IQR, 0–0) in extension and 90° (IQR, 55–95) in flexion preoperatively, and 0° (IQR, 0–0) and 95° (IQR, 90–95), respectively, at final follow-up.
Persistent triggering after surgical release, in the absence of incomplete release, fraying or partial tearing of the flexor tendon, is uncommon, with reported incidence ranging from 1.2 to 5.8% (Baidya et al., 2025; Fisher et al., 2025; Kwan et al., 2025). Various techniques address persistent triggering, with USSE becoming increasingly popular. USSE is beneficial not only for tendon debulking but also for proximal interphalangeal joint contracture (Le Viet et al., 2004). However, when USSE alone is insufficient, adding RFT can be effective. Risk factors for persistent triggering include involvement of multiple fingers or the middle finger and prolonged symptoms (Kwan et al., 2025). Our findings also suggest that tenderness distally to the A2 pulley is a useful clinical indicator. Ultrasonography and MRI are not routinely performed for trigger finger; however, in patients with these risk factors, they may be useful for detecting thickening of the flexor tendons and pulleys. Many patients who have persistent triggering have experienced surgery in other fingers and often expect simple release to suffice. Therefore, when persistent triggering is suspected, patients should be advised preoperatively about additional procedures. Limitations of this study include a small sample size, short follow-up and no control group.
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical approval declaration
This study was approved by the Ethics Committee of Ogori Daiichi General Hospital (Institutional Review Board 25-07).
Informed consent declaration
Written informed consent was obtained from all subjects before the study.