
Abstract
Introduction:
The treatment of complex intra-articular fractures of the distal radius may require the use of ‘fragment specific’ plates potentially irritating the flexor tendons. Our hypothesis is that there may be different rates of tendon irritation depending on the level of projection (radial and/or ulnar) of the plate at the watershed line. We report our experience with a cohort of 113 patients comparing four different plates.
Methods:
We conducted a single-centre study with prospective inclusion of patients with distal radial fractures from May 2022 to March 2025. The primary objective was to evaluate the rate of tendon irritation according to the type of specific fixation used for intra-articular fractures. At the 6 month visit, an ultrasound was performed to assess the presence or absence of tendon irritation, along with a computed tomography scan to evaluate proper application of the plate to the bone.
Results:
Forty-two ulnar hook plates (Medartis and Newclip Technics), 31 extradistal plates (Newclip Technics), 21 adjustable anterior rim plates (Medartis) and 19 curved ‘babyfoot’ plates (Medartis) placed distal to the watershed line were used for the fixations. At 6 months, ultrasound revealed tendon irritation in nine cases involving hook plates, 15 involving extradistal plates, 10 involving babyfoot plates and none involving adjustable anterior rim plates. There was a significant difference in the frequency of tendon irritation between plate types (p < 0.001).
Conclusion:
Our results suggest that specific, ulnar side fixation, ideally with an adjustable plate, may significantly reduce the risk of tendon irritation after complex distal radial articular fractures.
Level of evidence:
III
Keywords
Introduction
The management of articular fractures of the distal radius remains a frequent therapeutic challenge for surgeons (Medoff, 2005; Rhee et al., 2017). In complex and/or comminuted cases, the use of so-called ‘fragment specific’ fixations makes it possible to stabilize fracture fragments that are difficult to reach with standard wrist plates (Biondi et al., 2022; Geissler and Clark, 2016; Hozack and Tosti, 2019a). These plates are prefabricated according to average dimensions of the different articular fragments of the distal radius described by Medoff (Medoff, 2005; Rhee et al., 2017). With their help, several configurations can be employed, such as hook plates on the ulnar side, adjustable plates and ‘buttress’ plates (for example, the extra-distal plate from Newclip Technics, Nantes, France). The position of these fixations may vary on the palmar surface of the distal radius, but they share one feature: they extend beyond the watershed line (WL) (Bergsma et al., 2020a; Tay et al., 2021).
On sagittal sections, plates considered ‘specific fixations’ extend distally past the WL, lying in close proximity to the digital flexor tendons. Because the definition of the WL is somewhat vague and imprecise, we will instead refer to the most palmar point of the distal radius (Bergsma et al., 2020b). Such plates are all considered high risk for tendon irritation (Soong type 2) (Hayakawa et al., 2021; Soong et al., 2011b; Yoğun et al., 2025). On axial and coronal sections, however, the position of these fixations relative to the WL may vary: some extend beyond it only on the ulnar side, others only on the radial side, and still others on both. Agnew et al. (2015) studied the position of the flexor pollicis longus (FPL) relative to the distal end of the radius and described the danger zone as being located at the radial edge, with a lower risk at the ulnar edge for plates not extending beyond the WL (Agnew et al., 2015). Yet this study was limited to plates considered standard, not specific fixations. The authors’ hypothesis therefore does not account for fixations extending distally beyond the WL.
This study aimed to compare different fragment specific fixations of the distal radius in relation to tendon irritation rates assessed using ultrasound. Our hypothesis is that these rates may vary depending on which fixation is positioned distal to the WL. We report our experience with 113 fixations positioned beyond the WL and analyse how their radial or ulnar projection influences this risk. The primary objective of this study was to evaluate the rate of tendon irritation according to the type of fragment-specific fixation used. As a secondary objective, we assessed whether tendon irritation was associated with improper plate application against the bone.
Methods
We conducted a single-centre study with prospective inclusion of patients with distal radial fractures from May 2022 to March 2025. All patients provided written informed consent and the study was approved by the local ethics committee (IRB no. 2022-015724-1).
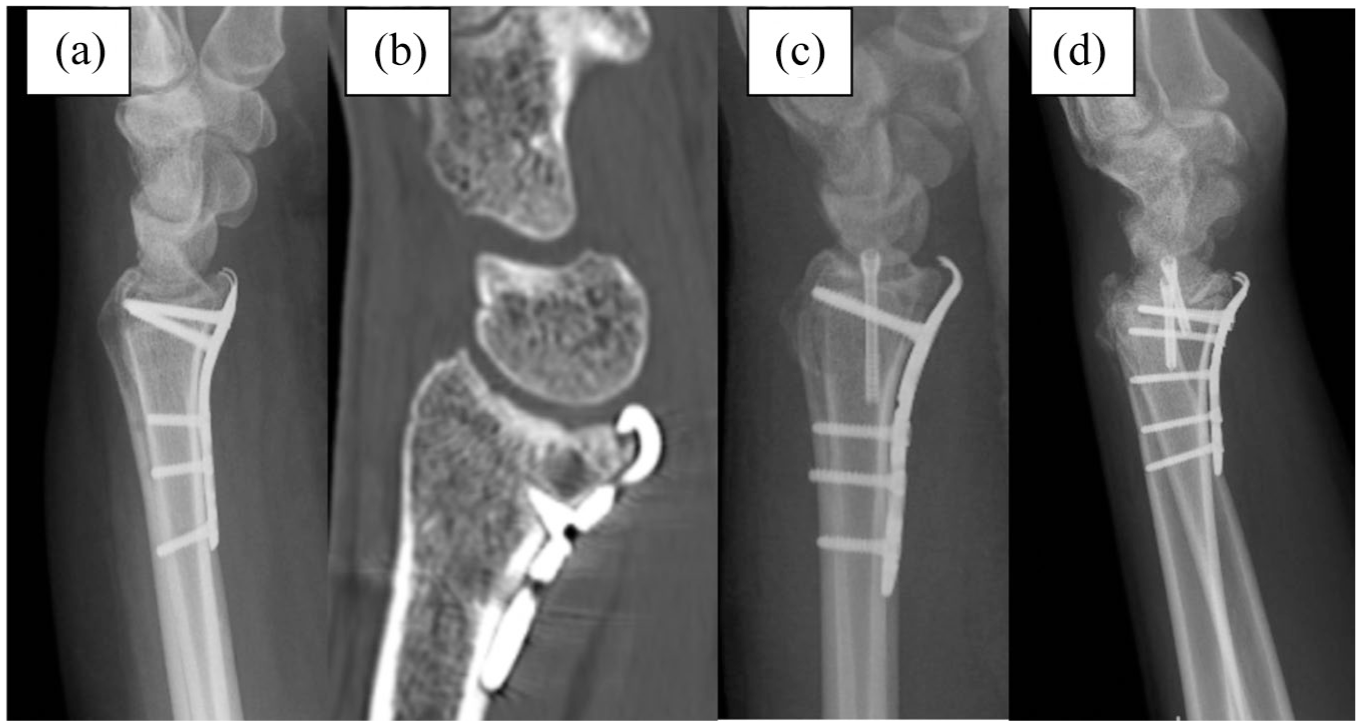
All operations were performed by a single trained wrist surgeon (level 4 expertise, Tang and Giddins, 2016), who also determined the choice of fixation. The four fragment-specific plates used were supplied by Newclip Technics (Nantes, France) and Medartis (Basel, Switzerland) (Figures 1 and S1). It should be noted that cases using TriLock palmar plates (volar/anterior rim adjustable plate or the adjustable ‘babyfoot’ plate (Medartis)) were only included if the plate had been bent to fit the most palmar point (MPP) (extending beyond the WL). Plate selection was based exclusively on the fracture pattern and intraoperative anatomical requirements, in accordance with routine clinical practice. No randomization was performed, as the objective of the study was to observe tendon-related complications associated with different fragment-specific fixations rather than to compare or define their indications.
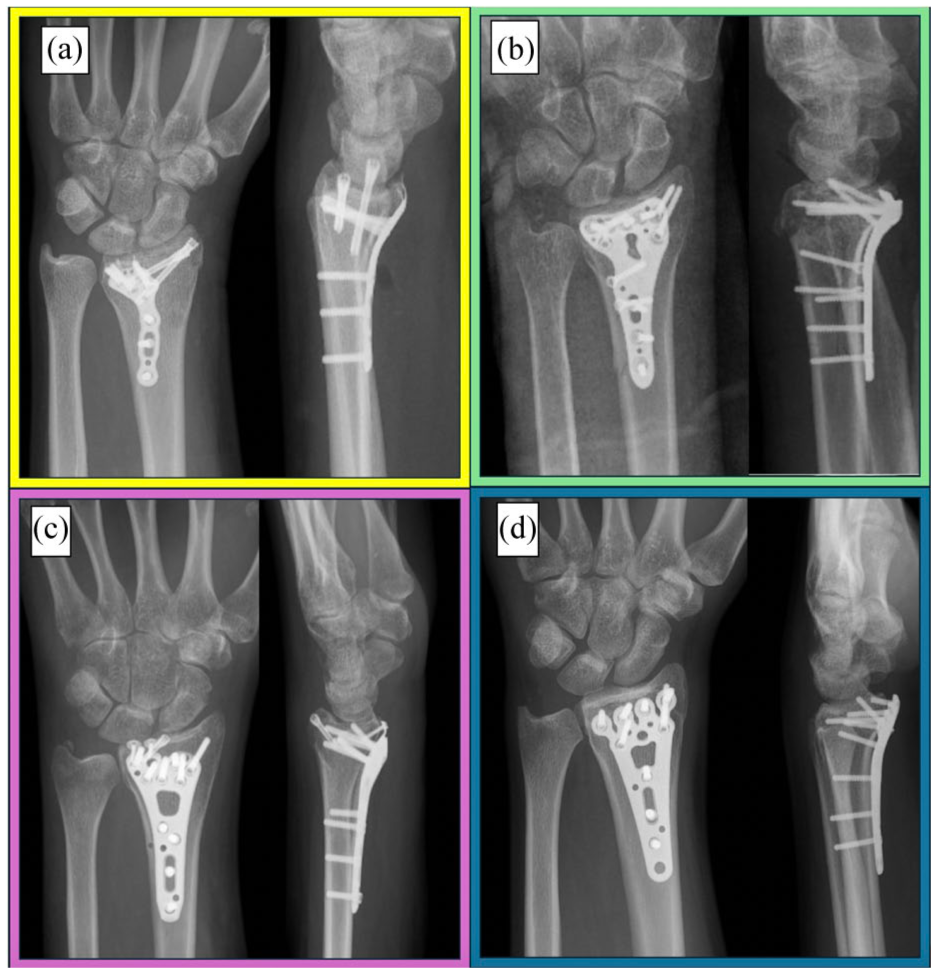
Frontal and lateral X-rays of the different plates analysed in our cohort. All plates have in common that they are positioned at least at the level of the watershed line (WL) (or beyond) on the lateral X-rays. (a) Example of fixation with an ulnar hook plate. Note that in the presence of a radial styloid fracture, headless screws will be used and buried in the styloid. The ulnar hook plates were from Newclip Technics (Nantes, France) (anterior hook plate) or from Medartis (Basel, Switzerland) (lunate facet plate). (b) ‘Extradistal’ (volar rim) plate from Newclip Technics (Nantes, France). (c) ‘Volar/anterior rim’ adjustable plate from Medartis (Basel, Switzerland). (d) Adjustable ‘babyfoot’ plate from Medartis (Basel, Switzerland). Note that only plates curved to fit the WL and applied distally to it were included in our study.
The inclusion criteria were an age >18 years, a distal radial fracture requiring specific fixation extending at least to the WL distally and operation within 14 days of injury. Because the anatomical definition of the watershed line is imprecise and subject to variability between individuals (Bergsma et al., 2020b), we deliberately chose to use the most palmar point of the distal radius as a reproducible and objective reference (Figure 2). This landmark was considered the most reliable surrogate for assessing plate prominence relative to the anterior rim in the context of this study.
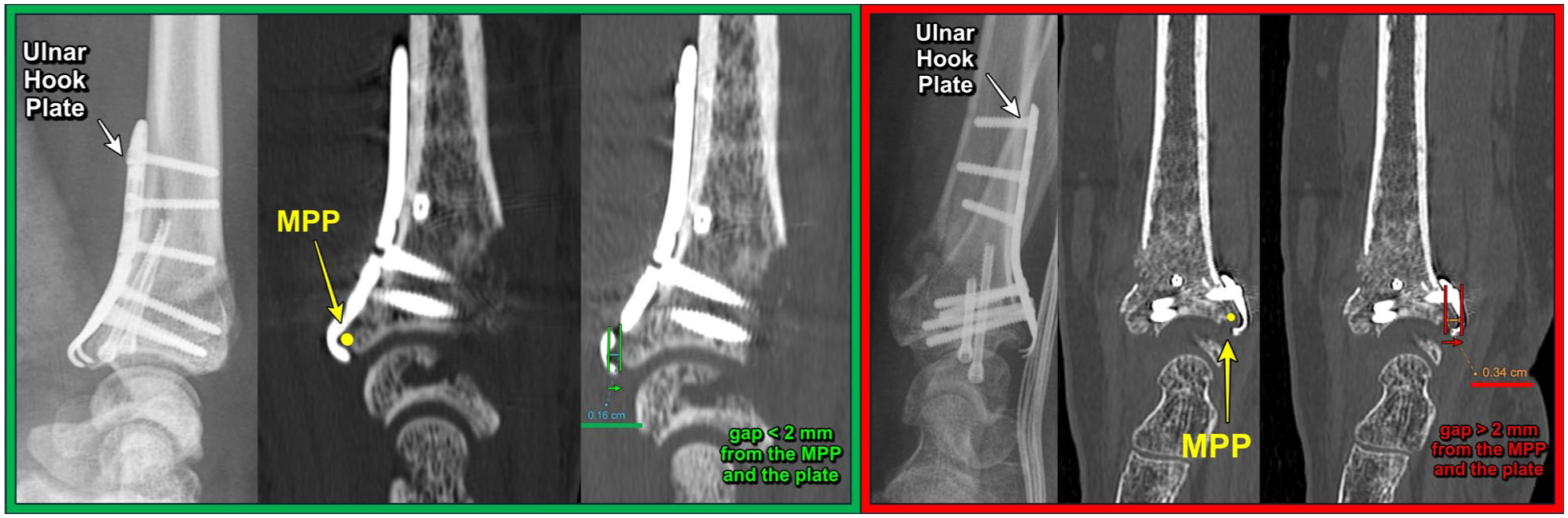
Sagittal CT-based measurement of plate prominence at the most palmar point (MPP). The MPP (yellow dot) was identified by musculoskeletal radiologists as the most anterior cortical point of the distal radius on sagittal reconstructions. Left (green frame): example of appropriate plate seating with a plate-to-bone distance <2 mm at the MPP. Right (red frame): example of imperfect plate seating, demonstrating a separation > 2 mm between the plate and the anterior cortex at the MPP.
The exclusion criteria were associated carpal lesions visible on initial radiographs (scapholunate diastasis >3 mm or perilunate lesions), open fracture, distal radioulnar or radiocarpal dislocation, an associated ulnar fracture at any location or a diaphyseal radius fracture. Because a fixation device placed outside its intended anatomical zone does not represent true fragment-specific fixation, such cases were excluded prior to analysis. The final cohort numbers for each type of plate therefore already exclude these mispositioned constructs (Figure 3).
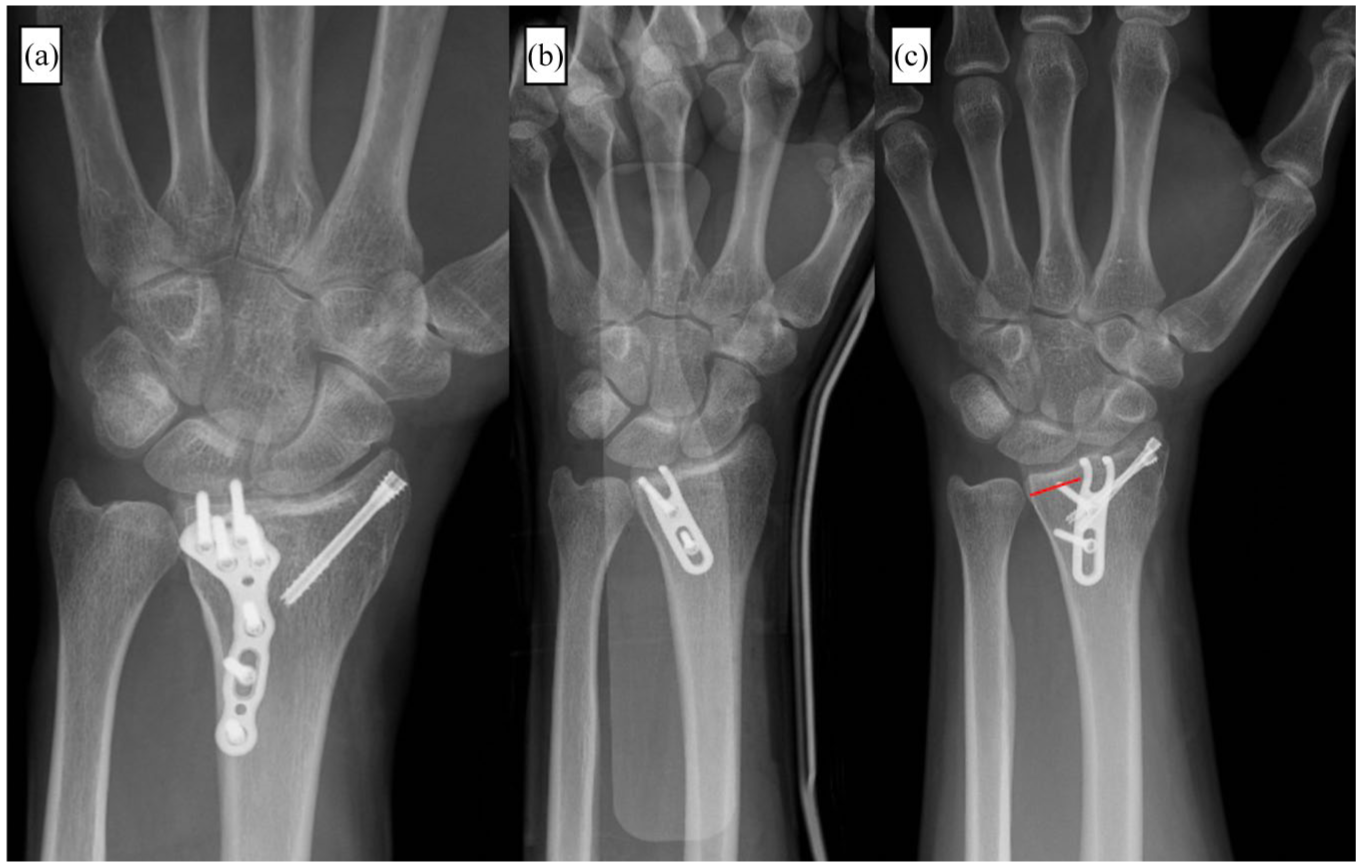
Examples of criteria for a well-positioned plate, according to the recommendations of different manufacturers (a and b), and an example of a poorly positioned plate (c). Ulnar column hook plates for distal radius fixation, hook type, (a) Medartis (Basel, Switzerland) and (b) Newclip Technics (Nantes, France). Both plates are correctly positioned on the ulnar column. (c) Hook plate from Newclip Technics, positioned away from the ulnar edge of the radius (red line), therefore not corresponding to the location specified by the company. Such cases were excluded from our cohort.
Further exclusion criteria were the absence of any data at the 6 month follow-up, non-adherence to physiotherapy or postoperative treatment and the presence of extra-articular malunion (defined radiographically as one or more of the following parameters at final follow-up: dorsal tilt >10°, volar tilt >20°, radial inclination <15°, radial shortening >3 mm compared with the contralateral side). No formal fracture classification was used for comparative analysis, as the objective of the study was not to evaluate plate indications according to fracture patterns. To limit selection bias related to fracture complexity, all cases underwent routine postoperative CT assessment to confirm appropriate plate application.
After surgery, all patients followed the same postoperative protocol with immobilization for 2 weeks in a wrist-stabilizing splint. Physiotherapy was initiated immediately to promote lymphatic drainage and digital mobility, while wrist mobility exercises began after 2 weeks.
Patients were reviewed at 1, 3 and 6 months. At the 6 month visit, an ultrasound examination was performed to assess the presence or absence of tendon irritation (to allow for timely plate removal if necessary), along with a computed tomography (CT) scan to evaluate proper fixation of the plate to the bone. It is our routine practice to perform a postoperative CT scan for articular fractures to assess reduction and plate positioning. Because the WL follows an oblique course, more distal on the radial side and more proximal on the ulnar side, radiographs may not reliably reflect the true prominence of the plate. For this reason, proper or improper plate application was confirmed on sagittal CT scans, which provide the most accurate postoperative assessment of plate position relative to the WL. Both CT scans and ultrasounds were carried out by a team of radiologists specializing in musculoskeletal imaging. All ultrasound examinations were performed by an evaluator who was blinded to the type of anterior plate used. On sagittal CT images, plate application was assessed by musculoskeletal radiologists by measuring the maximum distance between the plate and the anterior cortex of the distal radius at the most palmar point (Figure 2).
Two distinct situations must be differentiated: (1) plates implanted outside their intended anatomical location (e.g. a ulnar-specific plate positioned too radially) were excluded prior to group allocation, as they no longer represented true fragment-specific fixation; and (2) plates that were correctly indicated but imperfectly applied against the bone (i.e. with >2 mm separation from the MPP) were retained and analysed within their respective fixation group, since proper application to bone was one of the variables of interest.
We compared the rates of tendon irritation (rupture or irritation) diagnosed on ultrasound between the different plates used for fixation. Tendon irritation was defined as the presence of any of the following ultrasound findings: localized tendon thickening, intratendinous hypoechogenicity, Doppler signal hyperaemia, tendon fissuring, disorganization of the fibrillar pattern, direct or near-direct tendon–plate contact or evidence of tendon rupture (Figure 4).
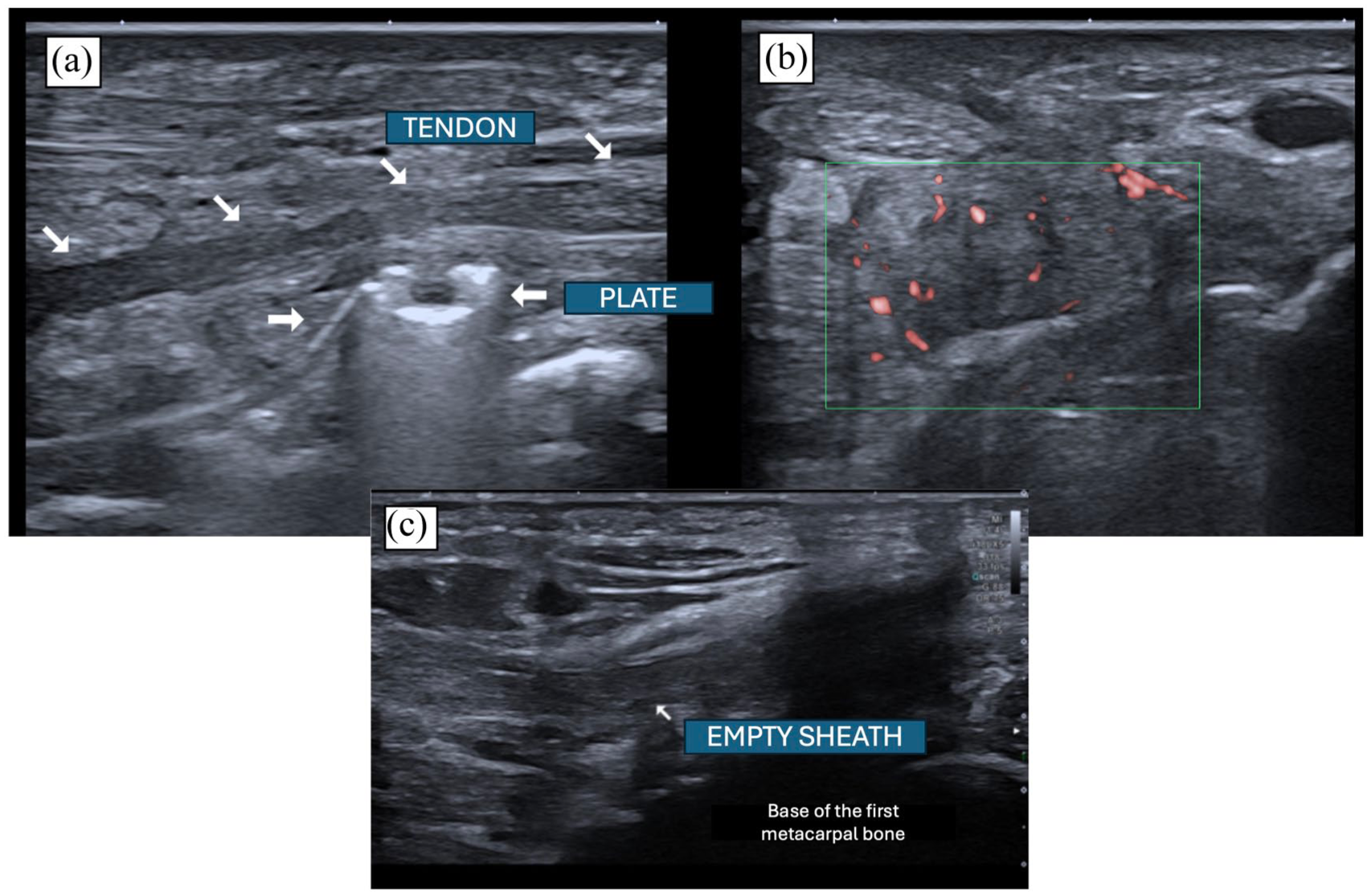
Examples of ultrasound images of tendon irritation resulting from contact with distal radial fixation plates. (a) Visualization of a tendon elevated because of contact with a plate. The tendon appears unstructured, hypoechogenic and non-fibrillar on a longitudinal section. (b) Clear hyperaemia in Doppler mode at the contact point with the plate. (c) Image of an empty sheath of the flexor pollicis longus tendon, representing an indirect sign of tendon rupture.
As a secondary analysis, we evaluated results according to the quality of plate application against the bone surface. A plate with more than 2 mm of separation from the bone at the MPP was considered ‘improperly applied’ (Figure 5).
Examples of well and poorly applied plates. (a) Images of correct application of the plate distal to the watershed line (WL) on a lateral radiograph. (b) The criterion for correct application (or otherwise) is confirmed on a sagittal CT scan. (c, d) The radiographs show incorrect application of the plates, resulting in a gap of more than 2 mm between the plate and the WL.
Statistical analysis
The data were analysed by an experienced statistician. A p-value of <0.05 was considered significant. P-values, 95% confidence intervals and standard deviations are reported. To compare the incidence of tendon irritation across the four fixation groups, a global chi-square test was first performed on a 4 × 2 contingency table. When the overall result was significant, pairwise comparisons were performed using Fisher’s exact test. Odds ratios with 95% confidence intervals were calculated for each pairwise comparison using the Haldane–Anscombe continuity correction because of zero-event cells in the adjustable anterior rim group. To account for multiple pairwise testing, p-values were adjusted using the Bonferroni method. Pairwise comparisons were presented in a consistent direction to facilitate interpretation of the odds ratios.
Results
In total, 131 patients presented with a distal radial fracture requiring fixation beyond the watershed line and were initially included in the study. Eighteen patients were excluded (eight lost to follow-up, five extra-articular malunion, four non-compliant with physical therapy and one plate implanted outside its intended anatomical location), leaving 113 patients for statistical analysis. The mean age was 47 years (range 18–84; SD 18).
Among the fixations, 42 were ulnar hook plates (Medartis and Newclip Technics), 31 were extradistal plates (Newclip Technics), 21 were volar (anterior) rim adjustable plates (Medartis) and 19 fractures required a curved ‘babyfoot’ plate placed distal to the WL (Medartis) (Figure 4) (Table 1).
Plate application quality and tendon irritation (n = 113).
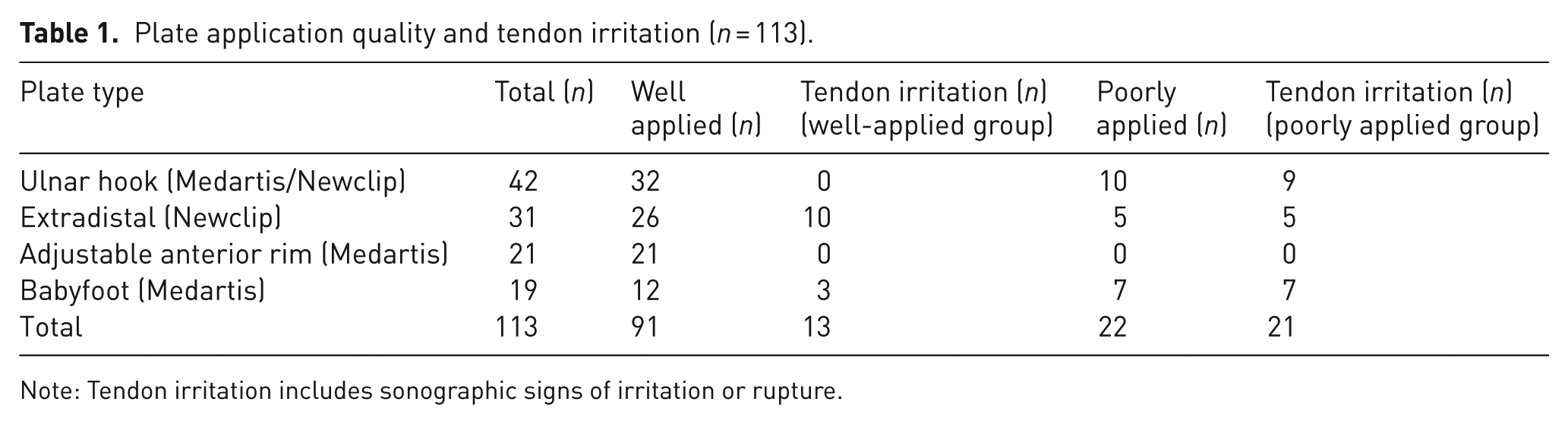
Note: Tendon irritation includes sonographic signs of irritation or rupture.
In our cohort, 10 hook plates, five extradistal plates, seven ‘babyfoot’ plates and no anterior rim plates were considered poorly applied on the basis of the postoperative CT scan. However, the total number of poorly positioned plates (22 across four groups) was too small to allow for a reliable statistical test.
At 6 months, ultrasound revealed tendon irritation in nine of 42 cases with hook plates, 15 of 31 with extradistal plates, 10 of 19 with babyfoot plates and none with adjustable anterior rim plates. Notably, only two true ruptures of the FPL were observed during follow-up, both associated with extradistal plates.
When considering all cases of incorrect application (22 of 113 plates; 20%), tendon irritation occurred in nine of 10 hook plates and in all five of the extradistal and seven babyfoot plates. Both FPL ruptures occurred in incorrectly applied extradistal plates.
In contrast, among correctly positioned plates (91 of 113; 82%), tendon irritation was observed in 10 of 26 extradistal plates and three of 12 babyfoot plates, while no irritation was recorded for correctly positioned hook plates or adjustable volar rim plates.
The overall chi-square test yielded χ2 = 20.06 (p < 0.001), indicating a statistically significant difference in the frequency of tendon irritation between plate types. Pairwise comparisons were then performed using Fisher’s exact test with odds ratios. After adjustment for multiple comparisons, only the comparisons between anterior rim and babyfoot plates and between anterior rim and extradistal plates remained statistically significant (Table S1, Figure 6).
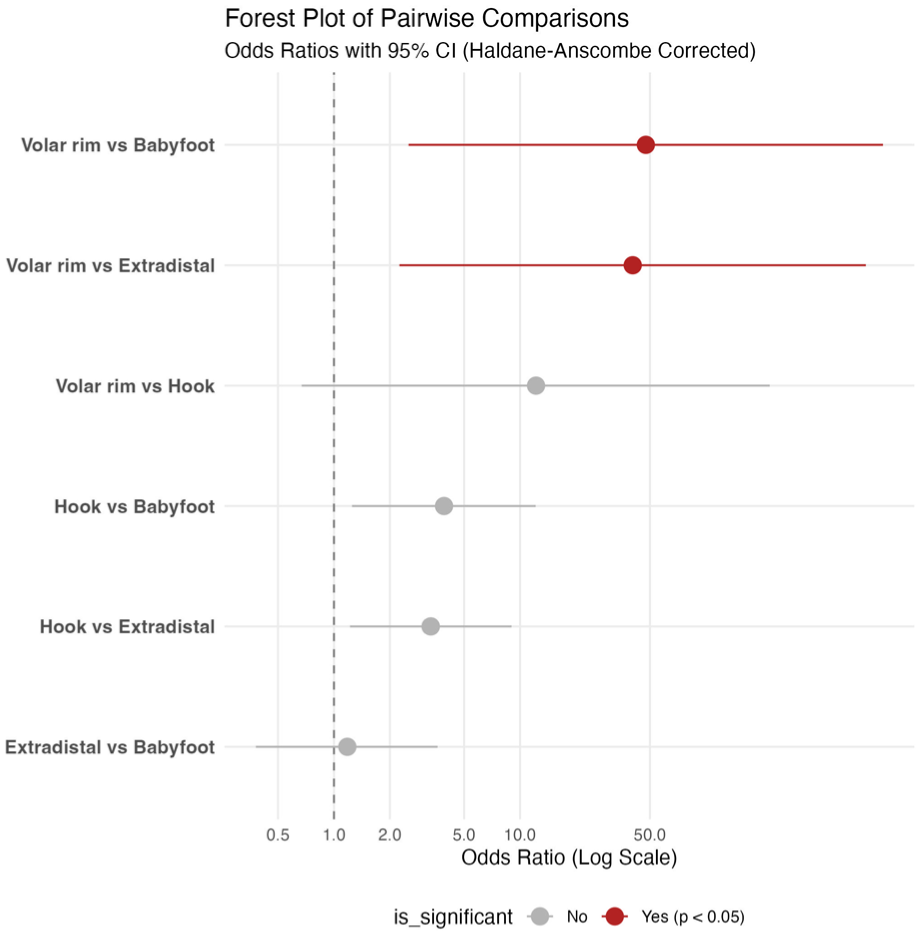
Forest plot of pairwise comparisons of tendon irritation according to plate fixation method. Odds ratios with 95% confidence intervals are displayed on a logarithmic scale. Odds ratios were calculated using the Haldane–Anscombe continuity correction because of zero-event cells in the anterior (volar) rim group. An odds ratio >1 indicates a higher likelihood of tendon irritation in the second plate of the comparison. Red markers indicate comparisons that remained statistically significant after Bonferroni adjustment.
Discussion
Our results suggest that plates extending beyond the watershed line do not necessarily cause tendon irritation when prominence is limited to the ulnar side. When correctly applied, adjustable ulnar plates may further reduce this risk.
Achieving and maintaining articular reduction often depends on the fixation method used, as some fractures cannot be stabilized with a standard palmar plate (Bowers et al., 2023; De Villeneuve Bargemon et al., 2023, 2026; Rhee et al., 2017). An inappropriate choice of fixation can lead to complications with significant consequences (Beck et al., 2014; Orbay and Bain, 2022; Orbay et al., 2016). Fragment-specific fixation is valuable in very distal articular fractures, but tendon irritation may still limit recovery. Rupture of flexor tendons represents a severe complication often requiring complex secondary procedures (Azzi et al., 2017; Soong et al., 2011a).
Fragments specific plates may cause tendon irritation, particularly those with a ‘buttress’ effect (Bowers et al., 2023; Hozack and Tosti, 2019b; Limthongthang et al., 2014). All fragment-specific palmar fixations extend beyond the WL and are therefore considered high risk for tendon rupture under Soong’s classification (type 2) (Soong et al., 2011a, 2011b; Yoğun et al., 2025). Because these plates carry a risk of tendon irritation, early removal is often recommended. In our series, plates with radial projection beyond the anterior rim, particularly extradistal and babyfoot designs, showed the highest irritation rates, whereas ulnar-specific plates appeared safer.
Limthongthang et al. (2014) analysed the vulnerability of the FPL in relation to the design of five standard palmar plates and found that the tendon lies at approximately 54% of the width from the anterior ulnar corner. This anatomical configuration is consistent with our finding of lower tendon irritation when plates extend beyond the watershed line only on the ulnar side.
Our study compared different specific fixation plates in relation to tendon irritation, particularly with respect to radial and/or ulnar protrusion. Agnew et al. (2015) reported that a plate thickness greater than 2 mm carries a high risk of tendon irritation, which guided our threshold for defining a plate as poorly applied. Surgical precision is essential, as plates not seated properly on the anterior rim were associated with tendon irritation in 90–100% of cases in our series.
Interestingly, plates that are adjustable only on the ulnar side (adjustable anterior rim plates) did not result in either misapplication or tendon irritation. A recent study highlights significant variability in the anatomy of the anterior rim (Valerio et al., 2025), suggesting that prefabricated plates may not always adapt perfectly in this area, whereas adjustable plates may better accommodate anatomical variability. In our series, babyfoot and extradistal plates, both extending radially beyond the watershed line, were associated with higher tendon irritation rates, whereas hook plates showed a lower risk profile. Nevertheless, even with correct plate positioning, close radiological and clinical monitoring remains essential, as inadequate articular reduction may still expose patients to tendon rupture (Park et al., 2025).
Our study has certain limitations. With 113 patients, the sample size remains modest and limits definitive confirmation of our hypothesis. However, published cohorts on fragment-specific distal radius fixation rarely exceed 60 patients, making this one of the largest series addressing tendon irritation with these devices (Biondi et al., 2022; Bowers et al., 2023; Chua et al., 2022; Gundecha et al., 2024). Despite the limited sample size, our analyses detected significant differences between fixation methods. However, the small number of poorly applied plates precluded reliable subgroup comparison.
The lack of randomization reflects the observational design of the study, as plate selection was based on fracture anatomy rather than comparative intent. Nevertheless, our findings may help guide implant choice when more than one fragment-specific option is feasible.
A potential limitation is the use of ultrasound at 6 months, as tendon ruptures may occur later. However, this time point was chosen to allow early detection of tendon irritation, and two FPL ruptures were still observed. Intraoperative tendon assessment at plate removal could provide additional information but was not available in this study. Ultrasonography has inherent diagnostic limitations, as tendon irritation may be asymptomatic or clinically silent, and early examinations may be falsely reassuring. This limitation is supported by recent findings from Estermann et al. (2025), who reported that ultrasound findings were not predictive of intraoperative tenosynovitis or tendon fibre discontinuity following anterior plate fixation.
Moreover, identification of the watershed line may be subject to anatomical variability; the use of the most palmar point on sagittal CT provides a reproducible and observer-independent landmark for assessing plate prominence relative to the anterior distal radius cortex. Finally, the Soong index has been questioned in other studies. Zhuang et al. (2026) reported that sagittal or coronal plate positioning does not appear to significantly influence the risk of tendon complications or hardware removal.
In conclusion, strictly ulnar-side fragment-specific fixation, when rigorously applied, may reduce tendon irritation and the need for secondary hardware removal after complex distal radius fractures.
Supplemental Material
sj-docx-1-jhs-10.1177_17531934261461998 – Supplemental material for Tendon safety profiles of fragment-specific fixations of the distal radius extending beyond the watershed line
Supplemental material, sj-docx-1-jhs-10.1177_17531934261461998 for Tendon safety profiles of fragment-specific fixations of the distal radius extending beyond the watershed line by Jean-Baptiste de Villeneuve Bargemon, Camille Brenac, Lucas Audiffret, Najib Kachouh, Remy Dubian and Emma Abecidan in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-jpg-1-jhs-10.1177_17531934261461998 – Supplemental material for Tendon safety profiles of fragment-specific fixations of the distal radius extending beyond the watershed line
Supplemental material, sj-jpg-1-jhs-10.1177_17531934261461998 for Tendon safety profiles of fragment-specific fixations of the distal radius extending beyond the watershed line by Jean-Baptiste de Villeneuve Bargemon, Camille Brenac, Lucas Audiffret, Najib Kachouh, Remy Dubian and Emma Abecidan in Journal of Hand Surgery (European Volume)
Footnotes
Acknowledgements
The authors would like to thank Dr Nicolas Fauvet for his valuable intellectual input and critical comments during the revision of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethicial approval
The study was approved by the local ethics committee (IRB no. 2022-A00912891).
Informed consent
All patients provided written informed consent.
AI declaration
No artificial intelligence was used in this study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.