
Abstract
We report the outcomes of 25 open dorsal proximal interphalangeal joint dislocations treated without palmar plate reinsertion. Stiffness was frequent, but no residual dorsal instability was observed. These findings suggest that routine palmar plate reinsertion may not be necessary.
Open dorsal proximal interphalangeal joint (PIPJ) dislocations are uncommon injuries. In a series of 74 fingers, six were open (8%) (Bewsey and Giddins, 2026). The need for palmar plate reinsertion remains controversial. While some authors have recommended reinsertion (Stern and Lee, 1985), this is not routinely performed in our practice. These injuries are often associated with palmar soft-tissue damage, which may lead to scarring, soft-tissue retraction and extension loss. Such changes may inherently limit hyperextension and reduce the risk of residual instability, even in the absence of palmar plate reinsertion. The aim of this study was to evaluate the functional outcomes of open dorsal PIPJ dislocations treated without palmar plate reinsertion and to describe the presence of residual instability and stiffness at follow-up.
We retrospectively reviewed 25 open dorsal PIPJ dislocations in 22 patients treated between May 2017 and November 2023. Three patients sustained two dislocations each. Patients were included if they were managed within 15 days of injury and had a minimum follow-up of 6 months. Palmar and lateral dislocations were excluded. Fracture–dislocations were excluded when involving more than 30% of the articular surface, in accordance with the classification of Kiefhaber and Stern (1998). All cases were managed surgically with palmar wound debridement, joint irrigation, exploration of relevant structures and reduction. Palmar plate reinsertion was not performed in any case. Collateral ligament injuries were not systematically recorded. Joint stability was assessed intraoperatively by testing laxity in the frontal plane in both flexion and extension to evaluate the integrity of the proper and accessory collateral ligaments.
Postoperative management included protected mobilization using buddy taping, extension-block splinting or temporary pinning depending on joint stability. Extension-block pinning or splintage was performed only in cases of persistent instability after reduction and not for fracture management. Clinical assessment included measurement of PIPJ range of motion (ROM), total active motion and relative TAM, as well as pain, instability, and Quick Disability of the he Arm, Shoulder and Hand (QuickDASH) score.
The cohort comprised 22 patients (16 men, six women) with a median age of 48 years (IQR 38 to 63). The index finger was involved in five cases, the middle finger in four, the ring finger in five and the little finger in 11. In 10 fingers the dislocation was caused by a fall, in eight it was sport-related, in four the cause was an industrial accident and in three it was a traffic accident. Protected mobilization was achieved using buddy taping in 16 fingers, extension-block splinting in five and pinning in four. The duration of protection was 3 weeks in all cases. Hand therapy was prescribed in 11 cases.
Associated injuries were present in nine cases and included palmar skin defects, two of which required coverage with a palmar Hueston flap, as well as digital neurovascular injuries, flexor digitorum superficialis avulsion and non-displaced fractures. Functional outcomes are presented in Table 1. Range of motion was limited, with frequent flexion contracture. No cases of lateral instability, hyperextension laxity, or recurrent dislocation were observed. Pain was minimal and functional impairment was low. No postoperative infections were observed.
Outcomes after open dorsal proximal interphalangeal joint dislocations.
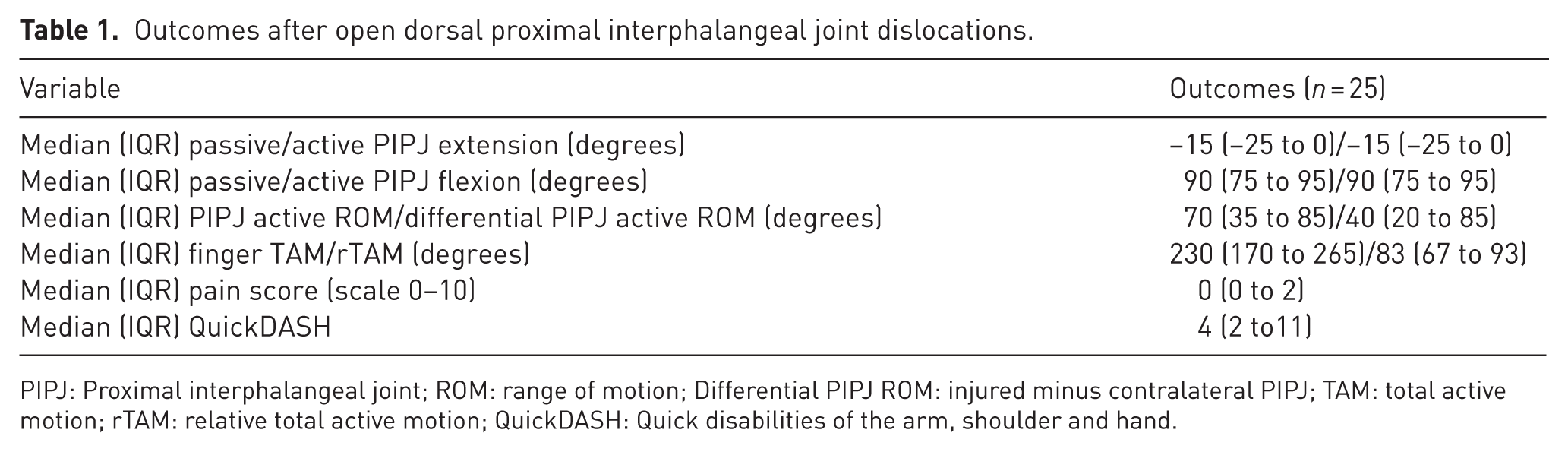
PIPJ: Proximal interphalangeal joint; ROM: range of motion; Differential PIPJ ROM: injured minus contralateral PIPJ; TAM: total active motion; rTAM: relative total active motion; QuickDASH: Quick disabilities of the arm, shoulder and hand.
The main finding of this study is that open dorsal PIPJ dislocations treated without palmar plate reinsertion are associated with substantial stiffness but no residual instability. Flexion was predominantly affected, with a mean flexion contracture of 18°, and no patient demonstrated hyperextension laxity or objective medial/lateral instability.
Evidence regarding treatment of open dorsal PIPJ dislocations remains limited. Stern and Lee (1985) reported 17 patients. In nine the palmar plate was reinserted. Direct comparison is limited, however, as treatment differed between the two groups in their study. Patients undergoing palmar plate reinsertion received operative management including debridement, antibiotic therapy, and K-wire fixation, whereas fingers without palmar plate reinsertion were splinted postoperatively. Our findings are comparable in terms of motion, with a mean ROM of 61°, similar to the 56° reported by Stern and Lee (1985), despite their recommendation for palmar plate reinsertion and postoperative K-wire fixation. The rationale for reinsertion could be to prevent hyperextension instability. However, no instability was observed in either series.
In this study, functional impairment was limited despite reduced PIPJ motion, with low QuickDASH scores and minimal pain. The observed ROM was close to the functional range required for daily activities, estimated at 60° (Hume et al., 1990). This study is limited by its retrospective design and modest sample size.
These findings suggest that routine palmar plate reinsertion may not be necessary in open dorsal PIPJ dislocations.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical approval
All patients gave oral and written informed consent before being included in this study. Ethical approval was given by our facility’s local Ethics Committee based on the retrospective nature of the study, as all the procedures being performed were part of the routine care and follow-up of patients.
Informed consent
Oral and written informed consent was obtained from all individual participants included in the study.