
Abstract
Background:
Medical thoracoscopy (MT) is primarily employed to obtain histopathological evidence via parietal pleural biopsy. However, parietal pleural lesions are not uniformly accessible, and evidence on visceral pleural biopsy remains limited.
Objectives:
This study aimed to investigate the diagnostic sensitivity and safety of visceral pleural biopsy performed under semi-rigid MT in patients with undiagnosed exudative pleural effusions (EPEs).
Design:
Single-center retrospective observational study.
Methods:
A retrospective analysis was conducted on 459 patients with undiagnosed EPEs who underwent pleural biopsy via MT. Among the 324 patients who met the inclusion and exclusion criteria, 38 who underwent visceral pleural biopsy and 74 who underwent parietal pleural biopsy were included in the final analysis after propensity score matching. The diagnostic sensitivity and safety were determined for both groups.
Results:
The diagnostic sensitivity was 78.9% in the visceral pleural group (85.7% for malignancy and 55.6% for tuberculosis) and 91.9% in the parietal pleural group (92.6% for malignancy and 89.5% for tuberculosis). Subgroup analysis based on macroscopic patterns suggested that the difference in diagnostic sensitivity was mainly driven by cases of tuberculous pleural effusion presenting as diffuse pleural thickening under MT, whereas comparable sensitivities were observed between the two groups in malignant pleural effusion and nodular-type tuberculous pleural effusion. The median time to chest tube removal was 2 days in both the visceral pleural group and the parietal pleural group. No statistically significant differences were observed between groups.
Conclusion:
Medical thoracoscopic visceral pleural biopsy is safe and demonstrates comparable diagnostic sensitivity to parietal pleural biopsy for malignancies and tuberculosis presenting as nodular lesions under MT in patients with undiagnosed EPEs.
Plain language summary
In most cases, biopsies are taken from the outer lining of the chest wall (parietal pleura). However, in some patients, visible disease is found mainly on the lung surface itself (visceral pleura), making standard biopsies difficult. Until now, there has been limited evidence on whether taking biopsies from the visceral pleura is safe and reliable. In this study, we reviewed medical records of patients with unexplained exudative pleural effusions who underwent medical thoracoscopy. We compared patients who had biopsies taken from the visceral pleura with those who had biopsies from the parietal pleura. To make the comparison fair, patients were matched by age and sex. We found that biopsies taken from the lung surface were generally safe, with no increase in serious complications or longer recovery time compared with standard chest wall biopsies. The procedure showed a high ability to detect cancer, and was also effective in diagnosing tuberculosis presenting as nodular lesions when compared with parietal pleural biopsy. Overall, our results suggest that visceral pleural biopsy under medical thoracoscopy is a safe and useful option, especially when abnormal lesions are mainly located on the lung surface. This approach may help doctors reach a diagnosis in patients where standard biopsy sites are not accessible.
Introduction
The global burden of pleural diseases has been increasing, contributing to diminished quality of life and significant morbidity and mortality. 1 Accurate diagnostic approaches are required for subsequent optimal management. Among exudative pleural effusions (EPEs) that cannot be diagnosed by pleural fluid analysis alone, pleural neoplasms and tuberculosis are the two most common underlying causes. 2 Currently, pleural biopsy can be performed using several approaches, including image-guided percutaneous biopsy and medical thoracoscopy (MT). 3 In clinical practice, MT is often employed as a diagnostic modality when less invasive approaches fail to yield a definitive diagnosis. MT has been shown to improve the diagnostic yield in undiagnosed EPEs; it enables direct inspection of the pleural surfaces and permits biopsy under direct visualization. A meta-analysis reported a sensitivity of 91% for MT in the diagnosis of EPEs. 4
In current clinical practice, diagnoses achieved through MT are predominantly based on histopathological findings from parietal pleural tissue. 5 However, sampling may remain challenging when no visible lesions are identified on the parietal pleura, or when parietal pleural lesions are too firm to obtain adequate tissue samples. 6 Given that parietal pleural biopsy is not feasible in all clinical scenarios, and that evidence on visceral pleural biopsy remains limited, with existing studies largely confined to interstitial lung disease and peripheral parenchymal pulmonary lesions, further investigation is warranted.7,8 In this study, we conducted a retrospective analysis to compare the diagnostic sensitivity and safety of visceral versus parietal pleural biopsy performed during MT in patients with undiagnosed EPEs.
Methods
Study design
A previous study from our center evaluated the diagnostic performance of CT-guided percutaneous pleural biopsy in patients with undiagnosed EPEs. 9 In contrast, the present study focuses on patients undergoing medical thoracoscopic biopsy and aims to assess its diagnostic sensitivity and safety, with particular emphasis on the comparison between visceral and parietal pleural biopsy. This study retrospectively analyzed 459 patients with undiagnosed EPEs who underwent medical thoracoscopic biopsy at West China Hospital, Sichuan University, between November 2020 and August 2025. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 10 The completed STROBE checklist is provided as Supplemental Table 1.
Patients were included if they: (1) had pleural effusion fulfilling Light’s criteria for exudative effusion; (2) remained undiagnosed after initial diagnostic evaluation, including clinical assessment, imaging findings, and thoracentesis with routine pleural fluid analysis (biochemistry, cytology, and microbiology); (3) underwent MT with pleural biopsy; and (4) were aged ⩾18 years. Patients were excluded if they: (1) had a diagnosis of pneumothorax, bronchopleural fistula or empyema; (2) did not achieve a definitive diagnosis within 6 months of MT biopsy; or (3) had incomplete clinical or histopathological data.
Procedure
All MT biopsy procedures in our hospital were performed by two experienced operators, each with more than 5 years of experience in MT. Patients were positioned in the lateral decubitus (healthy side down). Intravenous dexmedetomidine and sufentanil were used for sedation and analgesia. 5–10 mL of 2% lidocaine was administered for local anesthesia. Under thoracic ultrasound guidance, a 1.0-cm skin incision was made following standard disinfection and draping. The subcutaneous and muscle layers were bluntly dissected with vascular forceps to access the pleural cavity, after which the trocar (MAJ-1058, OLYMPUS, Tokyo, Japan) was inserted. After drainage of the fluid, semi-rigid thoracoscopy (LTF 240, OLYMPUS, Tokyo, Japan) was introduced through the trocar into the pleural space. The parietal pleura and the visceral pleura were thoroughly examined for any abnormal lesions. Biopsy sites were determined according to macroscopic findings during thoracoscopy. For nodular lesions, specimens were preferentially obtained from larger and more prominent nodules, whereas for diffuse pleural thickening, biopsies were performed in areas with more pronounced thickening or visually abnormal features. Six to eight biopsy specimens from two to three lesions were obtained from the parietal or visceral pleura using biopsy forceps (MTN-BF-23/18-B-1, Nanjing Micro-Tech Co., Ltd., Nanjing, China). The biopsies were then sent for histopathological diagnosis. Finally, a chest tube was inserted, and a water-sealed drainage system was used. The chest tube was clamped for 12 h after cessation of the air leak and subsequently removed if chest CT confirmed resolution of pneumothorax. The time to chest tube removal was recorded for each patient. Postoperative complications were documented. We presented a case of tuberculosis in Figure 1 and a case of mesothelioma in Figure 2, both of which were from the visceral pleura group.
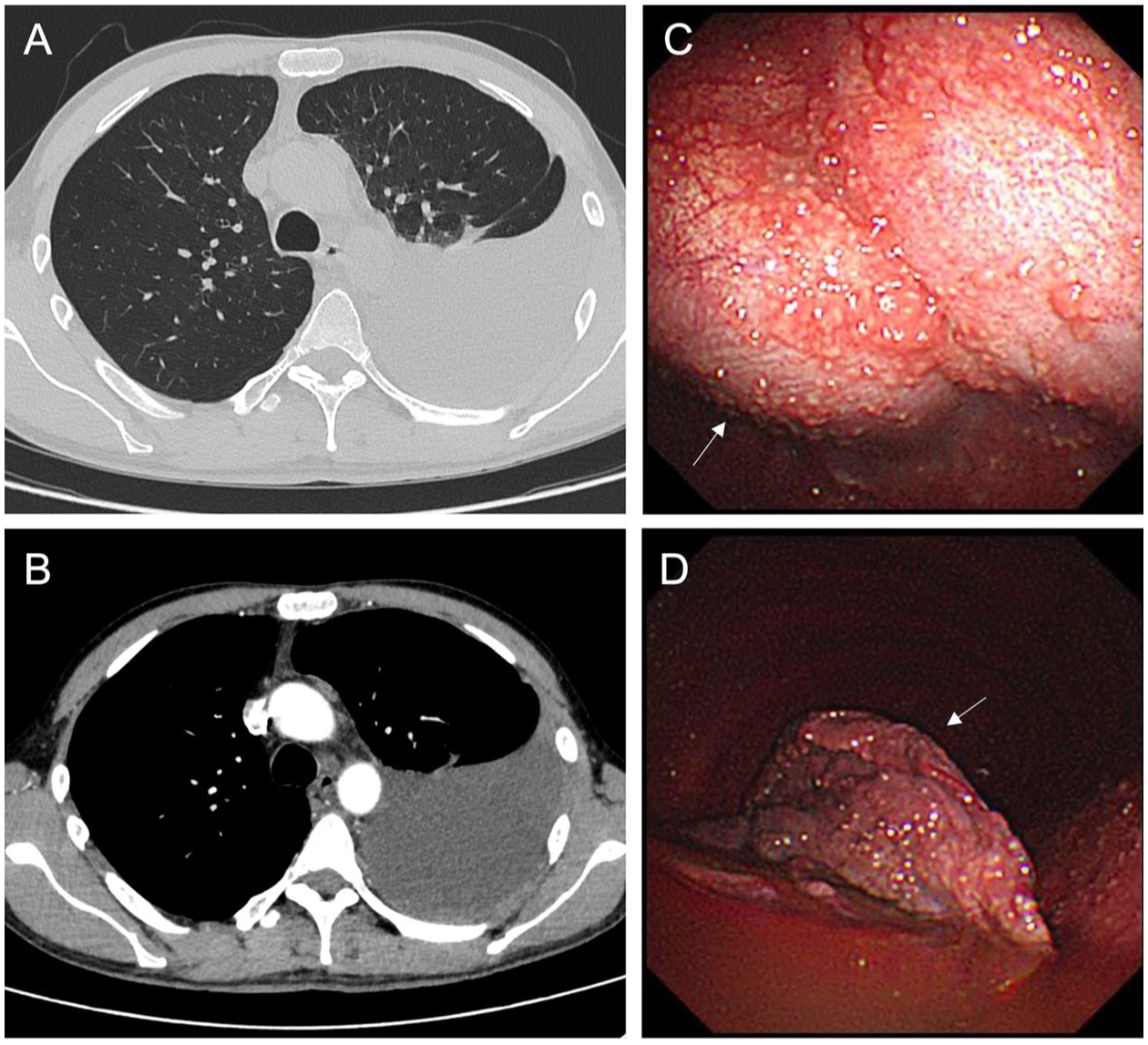
A representative case of tuberculosis in which visceral pleural tissue was sampled. (a, b) Lung window and mediastinal window of the patient’s computed tomography scan. (c, d) Medical thoracoscopic imaging of the biopsy procedure. The white arrows indicate the visceral pleura.
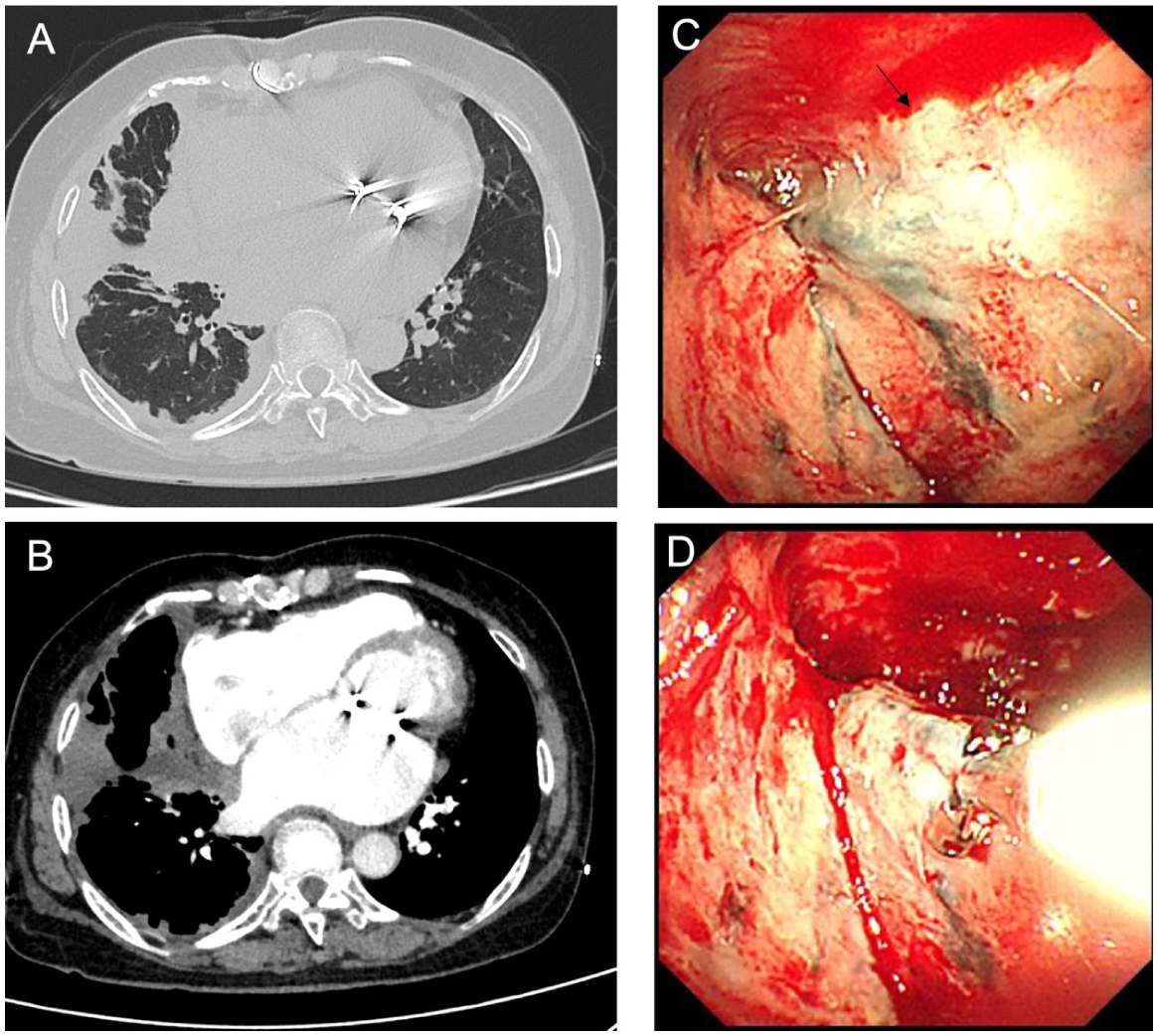
A representative case of mesothelioma in which visceral pleural tissue was sampled. (a, b) Lung window and mediastinal window of the patient’s computed tomography scan. (c, d) Medical thoracoscopic imaging of the biopsy procedure. The black arrow indicates the lesion on the visceral pleura.
Standardized diagnostic criteria for malignancies and tuberculosis
The standardized diagnostic criteria in this study are consistent with our previous study. 9 Malignancies were diagnosed based on: (1) a malignant tumor confirmed by the combination of cytology, biopsy, and imaging findings with a minimum follow-up of 6 months; or (2) pleural effusion cytology or pleural biopsy positive for malignant cells.
Tuberculosis was diagnosed based on: (1) growth of Mycobacterium tuberculosis on pleural effusion culture; (2) isolation of Mycobacterium tuberculosis from granulomatous tissue on pleural biopsy histology; or (3) granulomatous inflammation on pleural biopsy with a clinical response to antituberculosis therapy.
Statistical analysis
To minimize potential bias arising from differences in underlying etiologies between groups and to enable a more valid comparison of diagnostic sensitivity, propensity score matching was performed. Patients who underwent visceral pleural biopsy were matched in a 1:2 ratio with those who underwent parietal pleural biopsy alone, based on age and sex, with a caliper width of 0.05. Continuous variables are presented as mean ± standard deviation (SD) or as ranges when the data were not normally distributed. Categorical variables are expressed as counts and percentages. Comparisons of diagnostic sensitivity between groups were performed using the chi-square test with Yates’ correction or Fisher’s exact test, as appropriate. All statistical analyses were conducted using R software (version 4.2.2), and a two-sided p value <0.05 was considered statistically significant.
Results
Study population
In this study, a total of 324 patients met the inclusion and exclusion criteria, of whom 38 underwent visceral pleural biopsy. After matching, these 38 patients who underwent visceral pleural biopsy (of whom 9 also underwent parietal pleural biopsy) were matched to 74 patients who underwent parietal pleural biopsy alone (Figure 3 and Supplemental Figure 1). All baseline demographic and clinical parameters were comparable between the two groups (Table 1). The mean age of the overall cohort was 60.3 ± 12.6 years, and 59.8% were male. The final clinical diagnoses for the two groups are presented in Table 2. Among all patients, 73.2% and 25% were diagnosed with malignancies and tuberculosis, respectively. In addition, there was one case of sarcoidosis in the visceral pleural biopsy group (Group VP) and one case of endometriosis in the parietal pleural biopsy group (Group PP).
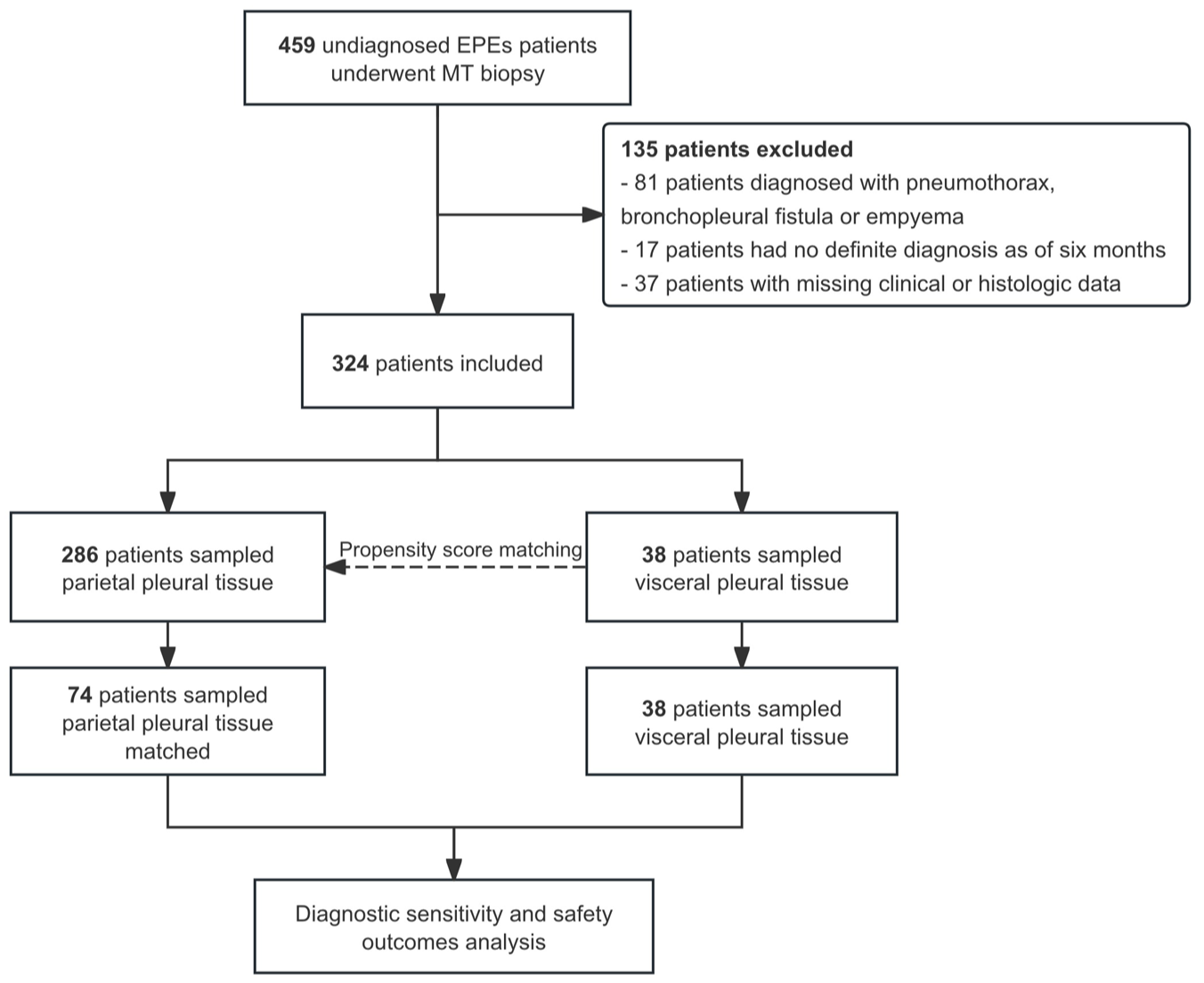
The flowchart of the study screening and propensity score matching procedure.
Clinical characteristics of the study population.
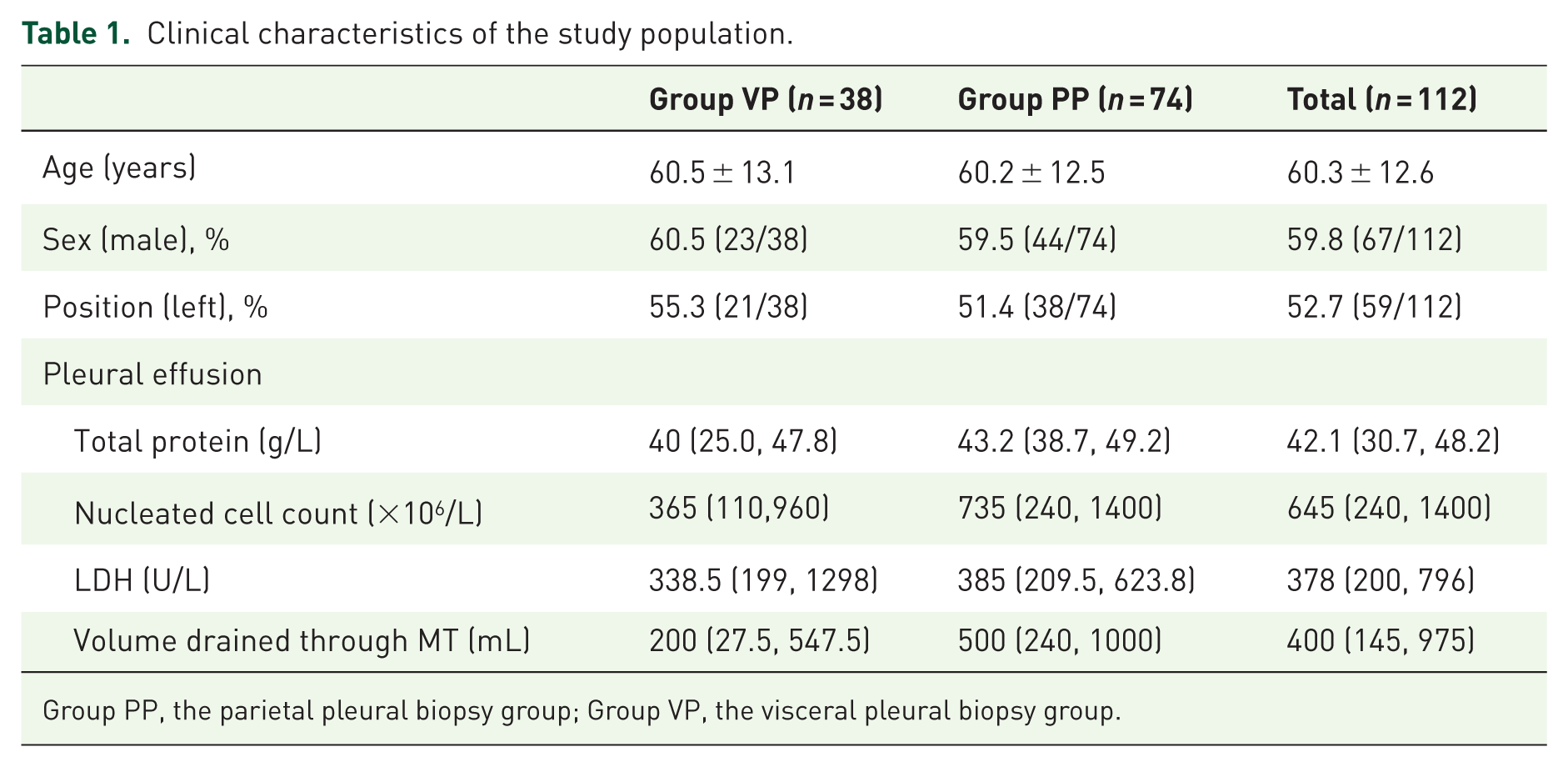
Group PP, the parietal pleural biopsy group; Group VP, the visceral pleural biopsy group.
Diagnosis distribution of the study population.
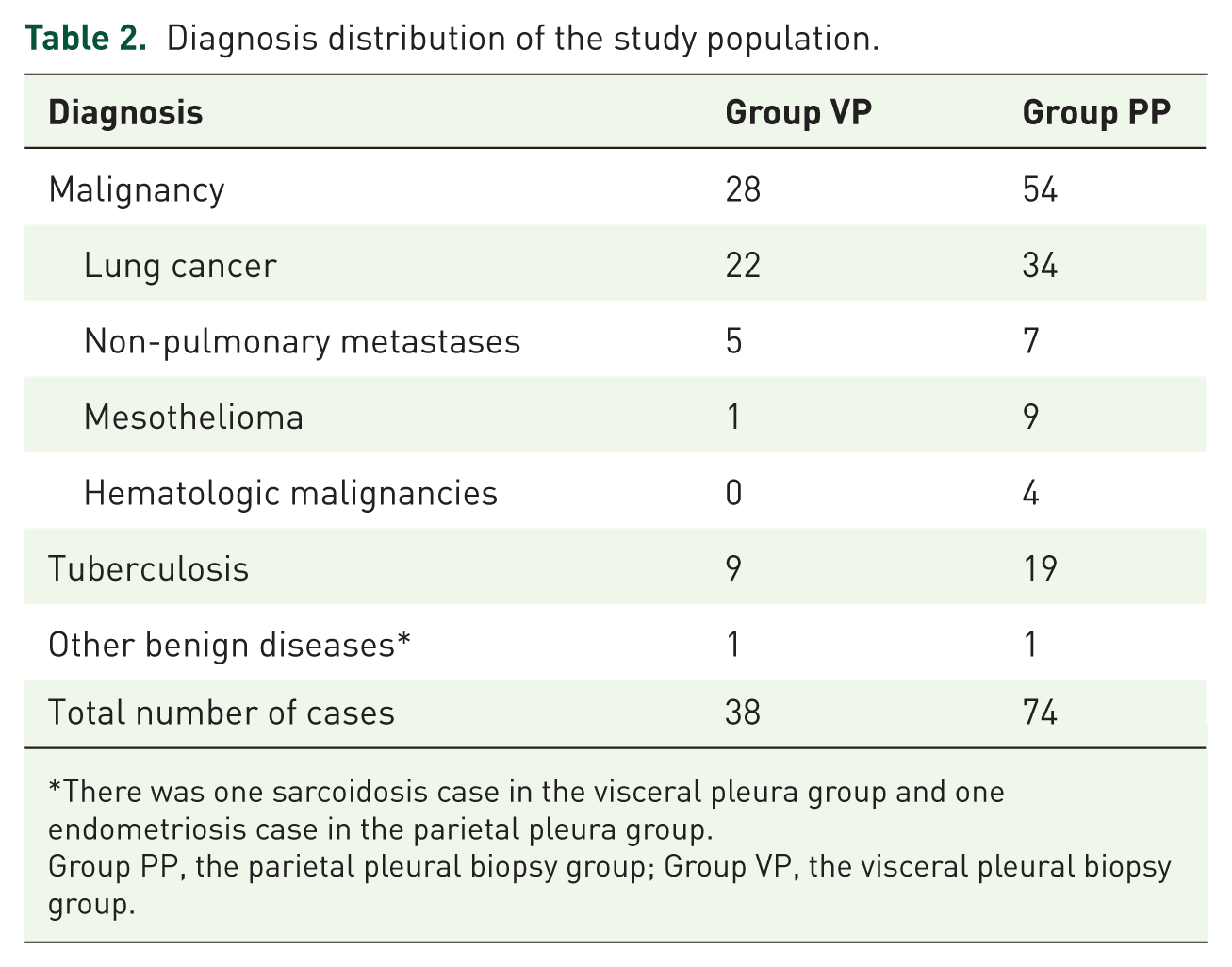
There was one sarcoidosis case in the visceral pleura group and one endometriosis case in the parietal pleura group.
Group PP, the parietal pleural biopsy group; Group VP, the visceral pleural biopsy group.
Macroscopic findings under MT
The macroscopic findings observed during MT can be classified into three patterns: nodular, diffuse thickening, and diffuse thickening with nodule. Among all patients diagnosed with malignancies, patterns with nodule (including the nodular pattern and the diffuse thickening with nodule pattern) were the most common, accounting for up to 73.2% (60/82) of cases; this finding was similar in the Group VP and Group PP (64.3% vs 77.8%). Compared with malignancies, the nodular pattern is less prominent in tuberculosis; 46.4% of tuberculous lesions exhibited the diffuse thickening pattern under MT. In Group VP, 66.7% of tuberculous lesions exhibited the diffuse thickening pattern, which was notably higher than the 36.8% observed in Group PP. The distribution of macroscopic findings in relation to the final diagnoses in both groups is presented in Figure 4.
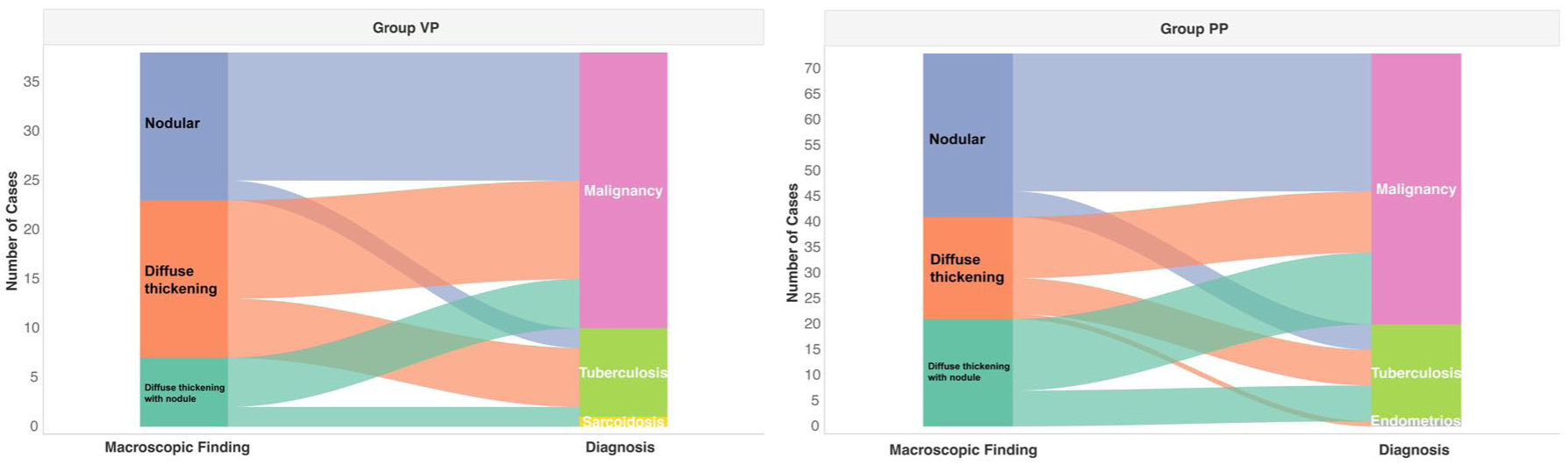
Distribution of macroscopic findings in relation to the final diagnoses in the visceral and parietal pleural biopsy group.
Diagnostic sensitivity and safety
The overall diagnostic sensitivities were 78.9% (30/38; 95% CI 62.7–90.4%) in the visceral pleura group and 91.9% (68/74; 95% CI 83.2–97.0%) in the parietal pleura group, with no statistical difference observed (p = 0.142). Diagnostic sensitivity was further analyzed separately for malignancy and tuberculosis in the visceral and parietal pleural groups. Regarding malignancies, the diagnostic sensitivity was 85.7% (24/28; 95% CI 67.3–96.0%) and 92.6% (50/54; 95% CI 82.1–97.9%) in the visceral pleura and parietal pleura groups, respectively. For tuberculosis, the sensitivity was 55.6% (5/9; 95% CI 21.2–86.3%) and 89.5% (17/19; 95% CI 66.9–98.7%) in the visceral pleura and parietal pleura groups, respectively. There were no significant differences in sensitivity between the two groups. For patients in whom MT did not yield a definitive diagnosis, the subsequent diagnostic approaches are summarized in Supplemental Table 2.
We performed a subgroup analysis of diagnostic sensitivity for the two diseases based on their macroscopic patterns. The results showed that when nodular lesions were observed under MT, the diagnostic sensitivity for both malignancy and tuberculosis exceeded 80% in both groups. For the nodular pattern, sensitivities for malignancy were 100% (13/13; 95% CI: 75.1–100%) in Group VP and 89.3% (25/28; 95% CI: 71.8–97.7%) in Group PP; for tuberculosis, they were 100% (2/2; 95% CI: 15.8–100%) and 80% (4/5; 95% CI: 28.4–99.5%), respectively. For the diffuse thickening with nodules pattern, sensitivities for malignancy were 80% (4/5; 95% CI: 28.4–99.5%) in Group VP and 100% (14/14; 95% CI: 76.8–100%) in Group PP; for tuberculosis, they were 100% (1/1; 95% CI: 2.5–100%) and 100% (7/7; 95% CI: 59.0–100%), respectively. In contrast, when diffuse pleural thickening was observed, the Group PP demonstrated a higher diagnostic sensitivity. Specifically, for malignancy with diffuse thickening, the sensitivity was 70% (7/10; 95% CI 34.8–93.3%) in the Group VP and 91.7% (11/12; 95% CI 61.5–99.8%) in the Group PP; for tuberculosis with diffuse thickening, it was 33.3% (2/6; 95% CI 4.3–77.7%) in the Group VP and 85.7% (6/7; 95% CI 29.0–96.3%) in the Group PP. However, these differences were not statistically significant. Detailed diagnostic sensitivities according to different thoracoscopic patterns are presented in Table 3.
Diagnostic sensitivity of Group VP and Group PP biopsies for malignancy and tuberculosis stratified by macroscopic findings.
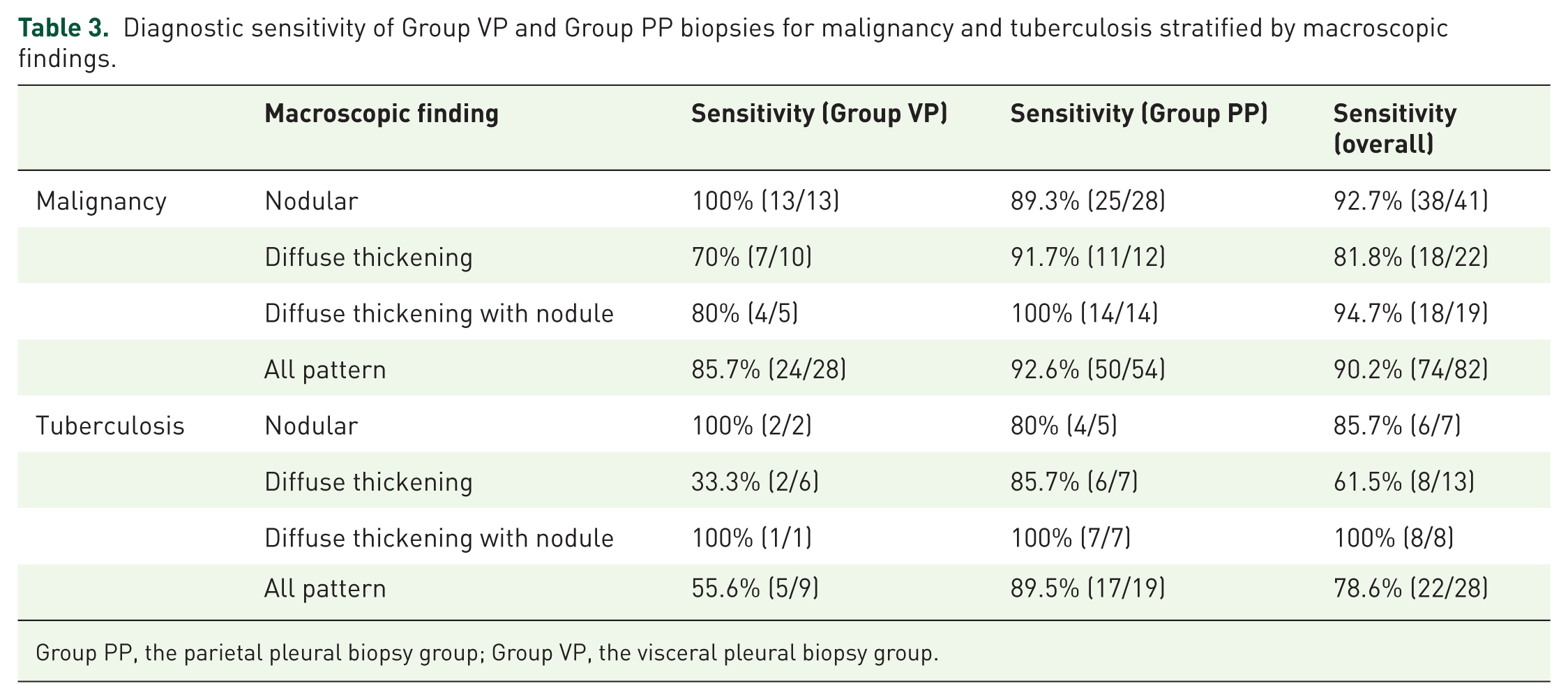
Group PP, the parietal pleural biopsy group; Group VP, the visceral pleural biopsy group.
Regarding safety, chest tube placement was not required in six patients in the visceral pleura group and in two patients in the parietal pleura group. The time to chest tube removal was 2 days in both the visceral pleura and the parietal pleura groups, with no statistically significant difference. There were six cases of chest pain in the visceral pleura group and five cases in the parietal pleura group; three cases of subcutaneous emphysema in the visceral pleura group, but none in the parietal pleura group. In addition, the parietal pleura group reported one case of fever and one case of vasovagal response. The safety outcomes of the visceral and parietal pleural biopsy groups are summarized in Table 4.
Comparison of safety outcomes between Group VP and Group PP.
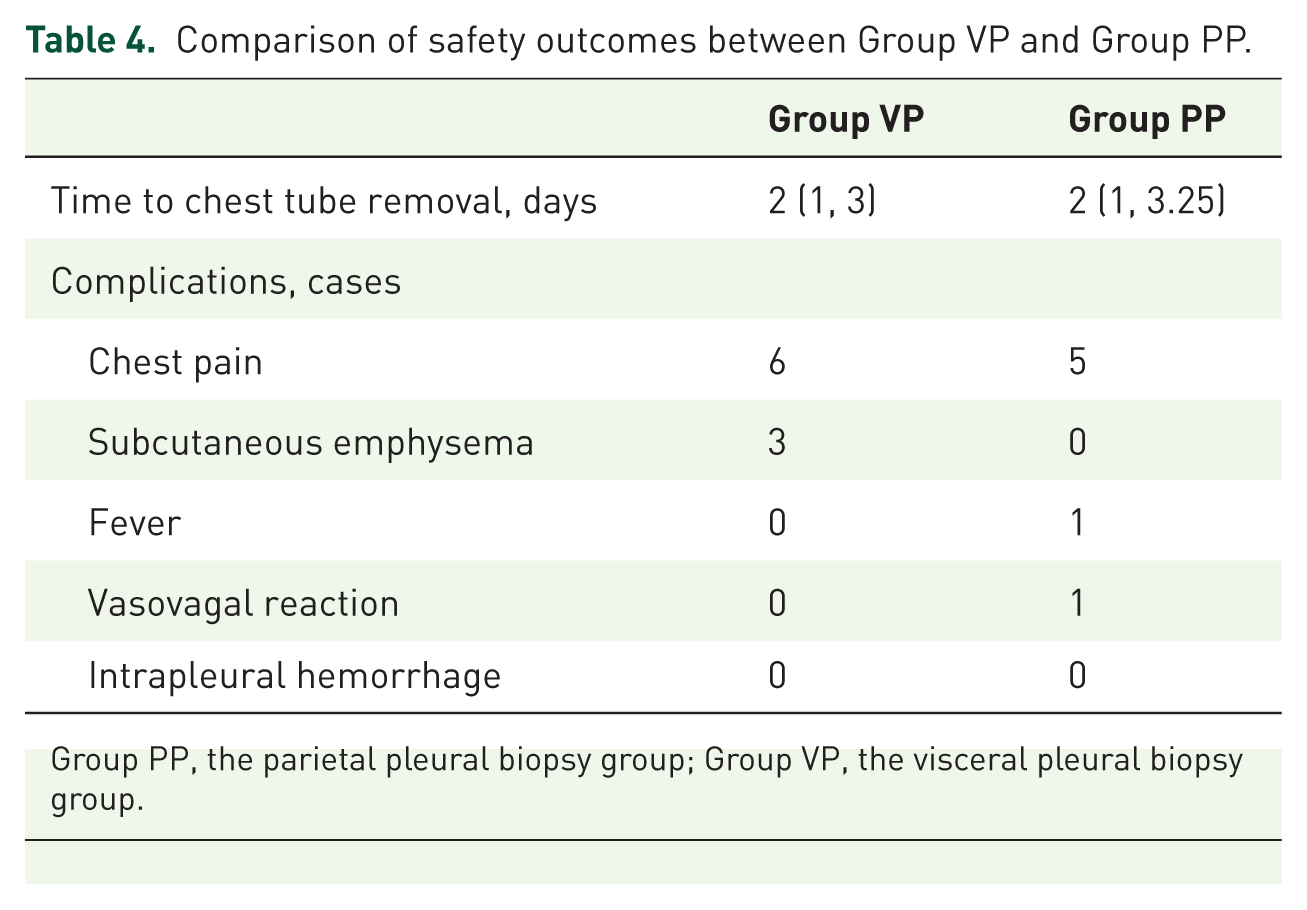
Group PP, the parietal pleural biopsy group; Group VP, the visceral pleural biopsy group.
Discussion
British Thoracic Society guidelines define parietal pleural biopsy as a Level I skill for general physicians, whereas visceral pleural biopsy is a Level II procedure requiring specialist expertise in dedicated pleural units. 11 In the present study, we investigated the diagnostic sensitivity and safety of visceral and parietal pleural biopsies performed under MT. Given that the underlying etiologies of pleural effusion may vary in age and sex distribution, propensity score matching based on these variables was performed to enhance comparability between groups and reduce potential confounding bias. Our results demonstrated that visceral pleural biopsy can be performed with an acceptable safety profile. Notably, when stratified by thoracoscopic morphology, its diagnostic sensitivity for nodular lesions was comparable to that of parietal pleural biopsy, whereas for diffuse pleural thickening, the diagnostic sensitivity of visceral biopsy was lower than that of parietal biopsy.
Visceral pleural biopsies are performed less frequently than parietal pleural biopsies, owing to concerns regarding the risk of prolonged air leak. 12 In our study, three cases of subcutaneous emphysema were observed in the visceral pleural biopsy group. This may be attributed to the fact that biopsy of the visceral pleura involves the lung surface and may increase the risk of air leakage, which has been reported as a potential cause of subcutaneous emphysema. However, the median time to chest tube removal in these patients was not prolonged compared with the parietal pleural biopsy group. For medical thoracoscopic biopsy in interstitial lung diseases, Schaberg et al. reported that the postoperative drainage times were on average between 4 and 5 days 13 ; Boutin et al. reported that a prolonged air leak (>5 days) was noted in 15% (3/20) patients with stiff lungs and fibrosis. 14 These findings suggest that visceral pleural biopsy via MT is safe in patients without interstitial lung disease.
The diagnostic yield of medical thoracoscopic parietal pleural biopsy for malignant and tuberculous pleural effusions has been reported to range from 91% to 94% and 93% to 100%, respectively. 11 In the present study, a pattern-specific difference in diagnostic performance between visceral and parietal pleural biopsy was observed. For nodular lesions, defined as nodular findings with or without associated pleural thickening, visceral pleural biopsy demonstrated diagnostic sensitivity comparable to that of parietal pleural biopsy in both malignancies and tuberculosis. Specifically, in malignancies, the sensitivity was 100% versus 89.3%, and in tuberculosis, it was 100% versus 80% in the visceral and parietal groups, respectively. In contrast, for lesions presenting as diffuse pleural thickening without nodules, visceral pleural biopsy showed lower diagnostic sensitivity compared with parietal pleural biopsy. This difference was observed in both malignancies (70% vs 91.7%) and tuberculosis (33.3% vs 85.7%), suggesting that the overall discrepancy in diagnostic performance between the two approaches is largely driven by this specific macroscopic pattern.
A review of the relevant literature was conducted to examine the characteristics of pleural thickening in these two conditions. A thoracoscopic study by Ellayeh et al. demonstrated that malignant pleural disease most commonly presents with nodular lesions, whereas benign conditions are more frequently associated with inflammatory changes. Notably, even in malignant cases without overt nodular features, inflammatory appearances (defined as erythema or pleural thickening) were more commonly detected on the parietal pleura than on the visceral pleura. 15 We hypothesize that diffuse thickening of the visceral pleura in malignant cases may more likely represent reactive changes rather than direct tumor involvement. Regarding tuberculosis, prior studies have reported that the granulomas of tuberculous pleurisy are characteristically located within the submesothelial connective tissue layer and the submesothelial adipose tissue compartment of the parietal pleura. 16 This is postulated to result from the distinctive blood supply and lymphatic drainage of the parietal pleura, which may favor the deposition of Mycobacterium tuberculosis and the subsequent development of pleural inflammation. These findings are therefore consistent with the established pathology of tuberculous pleurisy.
A key strength of the present study is that, to our knowledge, it is the first to compare the diagnostic sensitivity and safety of visceral versus parietal pleural biopsy performed under MT. Importantly, we further stratified lesions based on thoracoscopic appearance and demonstrated that, for nodular lesions, visceral pleural biopsy achieves a diagnostic sensitivity comparable to that of parietal pleural biopsy, while maintaining an acceptable safety profile. This study has several limitations. First, the retrospective design introduces inherent selection bias and the possibility of incomplete data collection. Second, although the overall cohort was relatively large, the number of patients undergoing visceral pleural biopsy was limited, particularly in subgroup analyses stratified by disease type and thoracoscopic morphological features. As a result, some subgroup comparisons were based on small sample sizes, which may have reduced statistical power. Nevertheless, our results provide preliminary evidence suggesting that, in selected clinical scenarios—particularly in patients with nodular pleural lesions—visceral pleural biopsy may achieve an acceptable diagnostic sensitivity and safety profile. Therefore, prospective studies with a larger sample size are needed to further validate these findings.
Conclusion
In patients with undiagnosed EPEs, medical thoracoscopic visceral pleural biopsy is safe and demonstrates comparable diagnostic sensitivity to parietal pleural biopsy in diagnosing malignancies and tuberculosis with nodular pleural lesions under MT.
Supplemental Material
sj-doc-1-tar-10.1177_17534666261455300 – Supplemental material for Diagnostic sensitivity and safety of visceral pleural biopsy under semi-rigid medical thoracoscopy in patients with undiagnosed exudative pleural effusions: a retrospective study
Supplemental material, sj-doc-1-tar-10.1177_17534666261455300 for Diagnostic sensitivity and safety of visceral pleural biopsy under semi-rigid medical thoracoscopy in patients with undiagnosed exudative pleural effusions: a retrospective study by Rui Xu, Lu Wen, Fen Tan, Jing Liu, Weimin Li, Dan Liu and Kaige Wang in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-docx-2-tar-10.1177_17534666261455300 – Supplemental material for Diagnostic sensitivity and safety of visceral pleural biopsy under semi-rigid medical thoracoscopy in patients with undiagnosed exudative pleural effusions: a retrospective study
Supplemental material, sj-docx-2-tar-10.1177_17534666261455300 for Diagnostic sensitivity and safety of visceral pleural biopsy under semi-rigid medical thoracoscopy in patients with undiagnosed exudative pleural effusions: a retrospective study by Rui Xu, Lu Wen, Fen Tan, Jing Liu, Weimin Li, Dan Liu and Kaige Wang in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-pdf-3-tar-10.1177_17534666261455300 – Supplemental material for Diagnostic sensitivity and safety of visceral pleural biopsy under semi-rigid medical thoracoscopy in patients with undiagnosed exudative pleural effusions: a retrospective study
Supplemental material, sj-pdf-3-tar-10.1177_17534666261455300 for Diagnostic sensitivity and safety of visceral pleural biopsy under semi-rigid medical thoracoscopy in patients with undiagnosed exudative pleural effusions: a retrospective study by Rui Xu, Lu Wen, Fen Tan, Jing Liu, Weimin Li, Dan Liu and Kaige Wang in Therapeutic Advances in Respiratory Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.