
Abstract
Background:
National quality standards for bronchiectasis in Italy were last defined in 2016. The publication of the 2025 European Respiratory Society (ERS) guidelines offers the opportunity to evaluate current clinical practice against updated evidence-based recommendations.
Objectives:
To assess the extent to which Italian bronchiectasis centers align with key statements from the 2025 ERS guidelines.
Design:
National, multicenter, cross-sectional observational study based on a structured survey of Italian bronchiectasis centers, aligned with the 2025 ERS recommendations.
Methods:
A national survey was conducted across Italian bronchiectasis centers affiliated with the Italian Bronchiectasis Patient Association (AIB). The structured questionnaire assessed center organization, diagnostic resources, multidisciplinary care, and alignment with ten predefined core management domains derived from the 2025 ERS recommendations.
Results:
Most centers reported universal access to minimum bundle etiological tests, with improved capacity compared with 2016. However, specialized diagnostics for rare causes, structured physiotherapy programs, and written self-management plans remain inconsistently available. Long-term inhaled antibiotics and macrolides were widely prescribed, though access barriers persist. Monitoring practices were heterogeneous.
Conclusion:
Despite clear progress, substantial variability persists in physiotherapy access, rare disease diagnostics, self-management tools, and routine monitoring. Updated Italian quality standards aligned with ERS 2025 principles are warranted.
Plain language summary
Bronchiectasis is a chronic lung disease that causes coughing, infections, and mucus build-up. In Italy, national standards for treating this condition had not been reviewed since 2016. This study describes how bronchiectasis is currently managed across Italian hospitals, using data from a recent national survey. Most centers now perform the key tests needed to understand the cause of bronchiectasis and provide the essential treatments recommended by experts. However, more advanced diagnostic tests—such as those for rare genetic conditions—are not available everywhere. Access to specialist physiotherapy and written self-management plans is also uneven. The way hospitals monitor patients over time varies widely across the country. Overall, care for bronchiectasis in Italy has improved compared with past years, but important differences remain. Updating national standards in line with new European guidelines could help ensure more consistent, high-quality care for all patients.
Introduction
Although historically considered a neglected condition, bronchiectasis is now recognized as a chronic respiratory disease associated with substantial morbidity, increasing prevalence, and rising healthcare burden.1 –3 Despite expanding clinical and research interest, the implementation of evidence-based care remains poorly characterized across Europe, with few countries having developed national guidelines.4,5
In Italy, the only available national quality standards (e.g., measurable indicators designed to assess adherence to clinical guidelines and the quality-of-care delivery) date back to 2016 and were based on the 2010 British Thoracic Society (BTS) guidelines.6,7 Since then, the landscape has evolved considerably, with the establishment of the European Bronchiectasis Registry (EMBARC) and the establishment of multiple dedicated outpatient clinics for bronchiectasis care across the country. 8
At the dawn of the new European Respiratory Society (ERS) guidelines, it is crucial to assess how current national clinical practice aligns with these updated principles. 9 Italy still lacks country-specific guidelines, and clinical management predominantly follows European guidance from 2017.
The aim of this study was therefore to provide an updated 2025 overview of bronchiectasis care in Italy, assess consistency with the new ERS recommendations, define current clinical practices, identify persistent gaps, and highlight priorities for the development of future national guidelines.
Methods
Study design and center selection
This study represents a secondary analysis of the 2025 Italian National Survey on Bronchiectasis Clinics and was conducted and reported in accordance with the CROSS guidelines for survey-based research (Supplemental File). 10 The survey was conducted between March and September 2025, prior to the publication of the updated ERS 2025 guidelines (October 2025). 9 Consequently, participating clinicians based their responses on existing local practice and on available international guidelines. 11 The present analysis retrospectively applies the 2025 recommendations as an external benchmark for current practice. The questionnaire—developed through a Delphi process by a multidisciplinary panel (including pulmonologists, respiratory physiotherapists, and cystic fibrosis (CF) specialists) in collaboration with the Italian Bronchiectasis Patient Association (Associazione Italiana Bronchiettasie, AIB)—explored organizational structures, access to diagnostic and therapeutic facilities, and standards of care. 12
Potential participating centers were identified through the AIB network and the list of Italian centers enrolled in EMBARC. Additional centers were included through direct contacts at national scientific meetings and spontaneous reporting by clinicians or AIB members, reflecting the progressive expansion of the national bronchiectasis network. Each center was contacted by e-mail and invited to complete the web-based survey.
For the purpose of this analysis, all centers actively managing adult patients with bronchiectasis were eligible, regardless of the presence of a dedicated bronchiectasis outpatient clinic. Centers that exclusively manage pediatric patients or are not directly involved in bronchiectasis care were not included.
Identification of the 2025 ERS guidelines recommendations
To operationalize the 2025 ERS guidelines for comparative assessment, ten recommendations were selected by the study steering committee based on their clinical relevance and feasibility of measurement within the survey structure (Table 1). These recommendations encompass the essential domains of bronchiectasis management, including etiological investigations, physiotherapy and mucoactive therapy, Pseudomonas aeruginosa eradication, long-term antibiotic strategies, exacerbation management, and patient education/self-management. Survey responses were summarized using descriptive statistics and interpreted in relation to these guideline recommendations.
List of recommendations derived from the 2025 ERS guidelines and percentage of Italian bronchiectasis centers adherent to each recommendation.
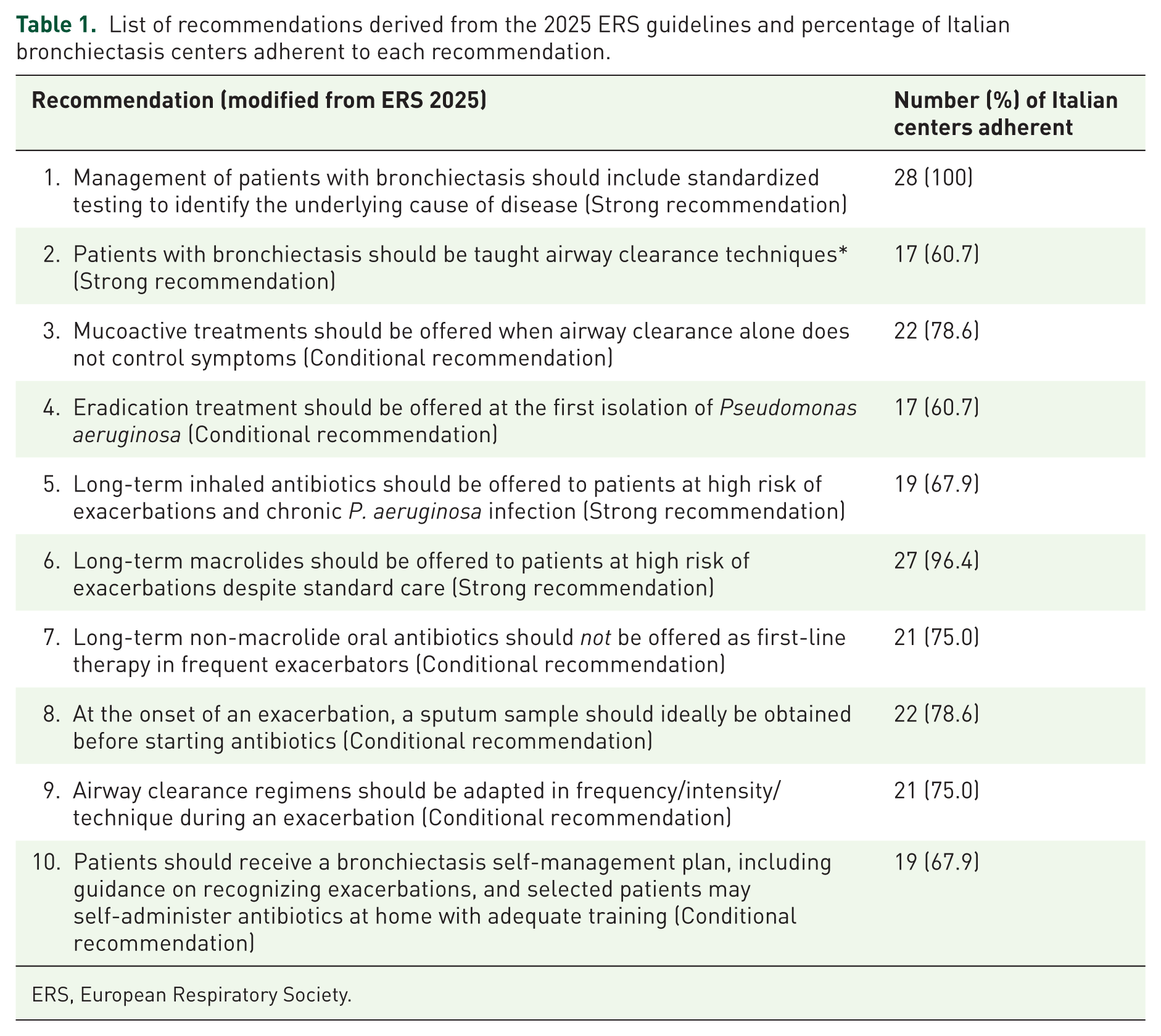
ERS, European Respiratory Society.
Results
The survey was distributed to 31 centers between May and September 2025. A total of 28 centers completed the questionnaire (response rate 90.3%). At each site, the questionnaire was completed by the lead physician or clinician responsible for the bronchiectasis clinic/service, who responded on behalf of the center. The geographical distribution was well represented across the country: 39.3% of centers were located in the North (n = 11), 32.1% in the South (n = 9), and 28.6% in Central Italy (n = 8). The regions with the highest number of participating centers were Lombardia (six centers), Lazio (four centers), and Toscana (three centers; Figure 1).
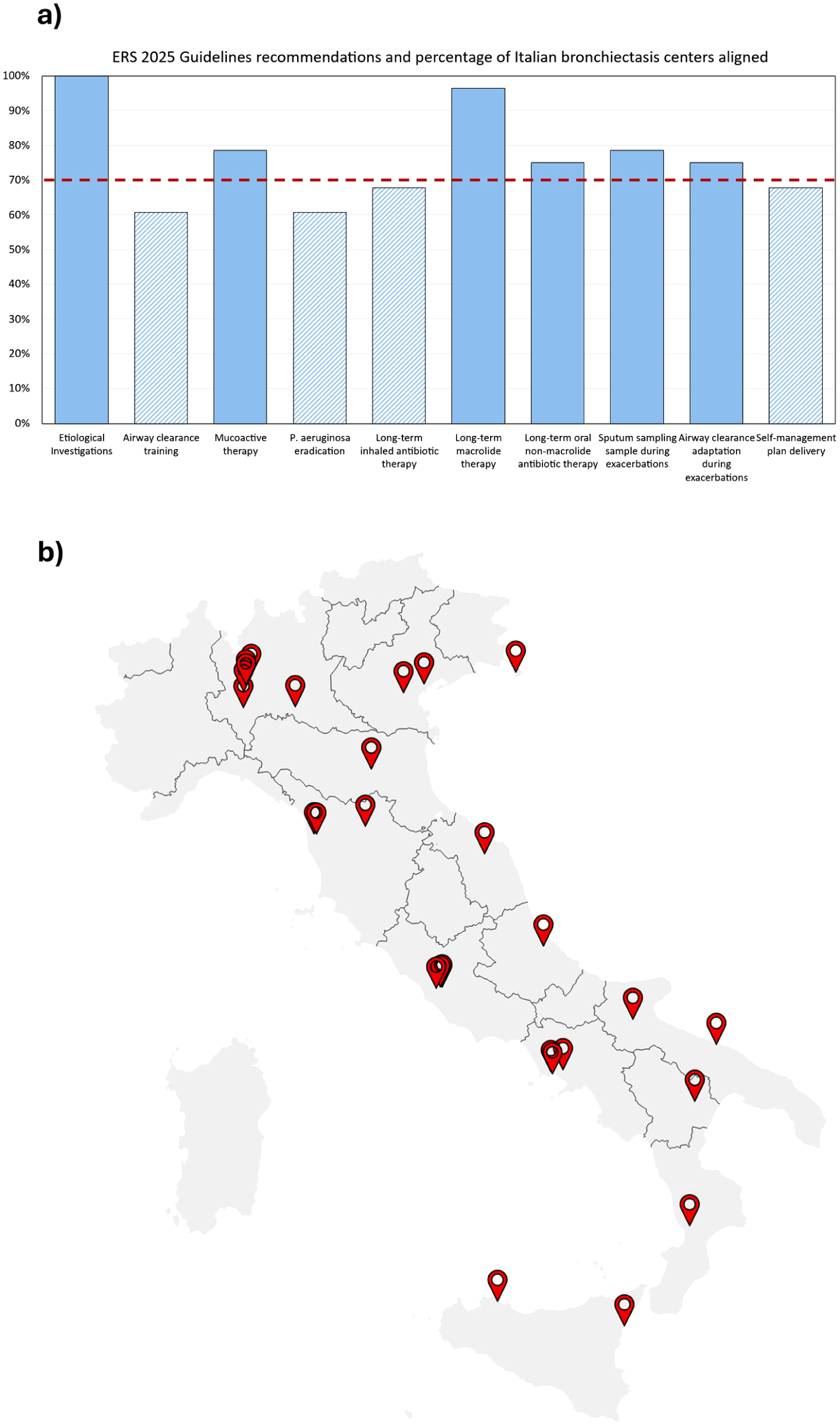
Geographic distribution of participating centers and alignment with ERS 2025 recommendations. (a) Percentage of Italian bronchiectasis centers aligned with the ten key ERS 2025 guideline recommendations. Solid bars indicate areas with higher alignment (⩾70%), while hatched bars indicate domains with lower alignment (<70%). The horizontal dashed line represents the 70% threshold. (b) Geographic location of the 28 Italian bronchiectasis centers that completed the national survey (response rate 90.3%).
Etiological and baseline investigations
All participating centers reported performing most core etiological assessments recommended by the 2025 ERS guidelines. A complete baseline evaluation, including serum immunoglobulins (IgG, IgA, IgM), serum α1-antitrypsin levels, selected autoimmunity screening, full pulmonary function testing, and routine sputum cultures for bacteria and fungi, was reported as routinely accessible across all centers. IgG subclass measurement was also universally available, while assessment of vaccine antibody response (pneumococcus/tetanus) was performed in 17 centers (60.7%). Testing for Aspergillus-related disease was widely accessible but with variable depth. Total IgE was available in all centers (100%). Specific IgE against A. fumigatus and other Aspergillus spp. was measured in 23 centers (82.1%), whereas specific IgG against A. fumigatus was measured in 16 centers (57.1%). Regarding infection screening, sputum culture for mycobacteria was available in 25 centers (89.3%). Genetic and rare disease investigations were less uniformly accessible. First-level CFTR genetic testing was available in 18 centers (64.3%), second-level CFTR testing and genetic testing for α1-antitrypsin deficiency in 12 centers each (42.9%), and sweat testing in 14 centers (50.0%). PCD-related investigations were limited: genetic testing was available in 12 centers (42.9%), while high-speed video microscopy and ciliary ultrastructural assessment by TEM were available in 3 centers each (10.7%).
Most centers reported managing key bronchiectasis-related conditions internally. A total of 25 centers (89.3%) actively followed patients with nontuberculous mycobacterial pulmonary disease (NTM-PD): 8 centers (28.6%) within a dedicated NTM outpatient clinic and 17 (60.7%) as part of the bronchiectasis service, whereas only 3 centers (10.7%) did not manage NTM infections directly. Allergic bronchopulmonary aspergillosis (ABPA) was diagnosed and treated within the same institution in 20 centers (71.4%), while chronic pulmonary aspergillosis (CPA) was managed in 16 centers (57.1%).
The frequency of routine monitoring showed marked variability across the country. Spirometry was repeated every 4–6 months in 10 centers (35.7%) and annually in 11 centers (39.3%). Microbiological monitoring for bacteria and fungi was performed at least once per year in 19 centers (67.8%), whereas mycobacterial sputum cultures were repeated annually in 16 centers (57.1%). Radiological follow-up was similarly heterogeneous: chest CT was repeated at least once every 2 years in 17 centers (60.7%).
Respiratory physiotherapy
In our cohort, 17 centers (60.7%) reported that all patients routinely received instruction in airway clearance techniques by respiratory physiotherapists, in line with guideline recommendations. In 11 centers (39.3%), airway clearance instruction was therefore delivered by physicians or nurses, or patients were referred externally for specialized training.
Mucoactive therapy
According to the ERS 2025 recommendations, mucoactive treatments should be offered to patients whose symptoms remain uncontrolled despite optimized airway clearance. In our cohort, 22 centers (78.6%) reported routinely prescribing mucoactive therapy. The most commonly used agents included hypertonic saline and N-acetylcysteine, either as monotherapy or in combination. In addition, five centers (17.9%) reported access to home humidified or high-flow nasal therapy to support secretion management, reflecting an emerging adjunct to conventional airway clearance strategies.
Pseudomonas aeruginosa eradication
Eradication of Pseudomonas aeruginosa was offered by all centers. In 17 centers (60.7%), this was reported only at the first isolation, according to current recommendations. An additional seven centers (25.0%) reported initiating eradication, also when P. aeruginosa was isolated for the second time, while four centers (14.3%) considered eradication even after subsequent isolations.
Regarding treatment modality, 14 centers (50.0%) reported using combination therapy with systemic plus inhaled antibiotics, whereas the remaining half relied on systemic antibiotic therapy alone.
Long-term inhaled antibiotic therapy
According to ERS 2025 recommendations, long-term inhaled antibiotics should be offered to patients at high risk of exacerbations—defined as those with ⩾2 exacerbations in the previous year, or ⩾1 severe exacerbation, or ⩾1 exacerbation combined with severe daily symptoms—when chronic Pseudomonas aeruginosa infection is present. In our cohort, 19 centers (67.9%) reported prescribing long-term inhaled antibiotics for patients with ⩾2 exacerbations and chronic P. aeruginosa infection, consistent with guideline recommendations. An additional six centers (21.4%) used inhaled antibiotics in patients with frequent exacerbations and chronic infection by pathogens other than P. aeruginosa. Regarding agent selection, colistin was the most frequently used agent (15 centers, 53.6%), followed by tobramycin (5 centers, 17.9%) and amikacin (3 centers, 10.7%). Treatment schedules varied across centers: continuous daily administration was reported by nine centers (32.1%), whereas 30-day on/off cycles and 14-day on/off cycles were used by eight centers (28.6%) and five centers (17.9%), respectively. Despite guideline endorsement, 11 centers (39.3%) reported barriers to the use of inhaled antibiotics, predominantly related to restricted access or prescribing limitations.
Long-term macrolide therapy
According to ERS 2025 recommendations, long-term macrolides should be offered to patients at high risk of exacerbations despite standard care. In our cohort, macrolides were prescribed by 27 of 28 centers (96.4%), primarily for patients considered at high risk of exacerbations according to 2017 international recommendations (i.e., ⩾3 exacerbations despite standard care). 11 Azithromycin was the only macrolide used, most commonly administered as 500 mg three times per week (50%) or 250 mg three times per week (39.3%).
Long-term oral non-macrolide antibiotic therapy
In keeping with the principles outlined in the ERS 2025 guidelines—which discourage the use of long-term non-macrolide oral antibiotics as first-line therapy for patients with bronchiectasis at high risk of exacerbations—most centers reported not prescribing these agents routinely. Specifically, 21 centers (75.0%) did not employ long-term non-macrolide oral antibiotics in this context, while seven centers (25.0%) reported using doxycycline as a suppressive option in selected circumstances, typically in patients who were intolerant of, or unsuitable for, macrolide therapy. This selected use was therefore interpreted as consistent with guideline principles rather than as routine first-line prescribing.
Exacerbation management
In accordance with ERS 2025 recommendations—which state that patients should obtain a sputum sample at the onset of an exacerbation before starting antibiotic therapy—22 centers (78.6%) reported advising patients to provide a sputum sample for microbiology in this context. ERS 2025 also recommends that airway clearance regimens be adapted during exacerbations by increasing frequency, intensity, or modifying technique. Consistently, 21 centers (75.0%) reported advising patients to adjust their airway clearance routine during exacerbations. Regarding patient guidance, the ERS 2025 guidelines highlight that an adult bronchiectasis self-management plan should include instructions on recognizing exacerbations and, in selected cases, support self-administration of antibiotics at home. In our cohort, 19 centers (67.9%) reported providing a written self-management plan: 15 centers (53.6%) issued personalized plans, while four centers (14.3%) used non-personalized templates. Another seven centers (25.0%) relied exclusively on verbal instructions, and two centers (7.1%) provided no self-management plan.
Discussion
This national analysis provides an updated overview of how Italian bronchiectasis centers align with the management domains outlined in the 2025 ERS guidelines. A substantial improvement emerged in the implementation of minimum bundle etiological investigations. Nearly all centers now report routine availability of serum immunoglobulins, α1-antitrypsin levels, autoimmune screening, and mycobacterial cultures—representing a marked progression from the 2016 national audit, where 59% of patients had undergone no etiological work-up and only 32% had been investigated for at least one cause. 6 Access to CFTR and PCD genetic testing has also expanded, although specialized ciliary studies remain available only in a small minority of centers, highlighting a persistent gap in the diagnostic pathway for rare causes. The high proportion of centers managing ABPA, CPA, and NTM internally reflects growing expertise and consolidation of bronchiectasis-focused services; however, formal referral pathways are still not established and should be strengthened within a coordinated national network.
Access to physiotherapy remains a major gap. In 2016, only 44% of patients had been taught airway clearance techniques by a respiratory physiotherapist, and despite a mild improvement, almost 40% of the centers still lack permanent physiotherapy support. Given the strong ERS 2025 recommendation that all patients—regardless of sputum production—should receive structured airway clearance instruction, expanding respiratory physiotherapy programs remains a national priority. Written self-management plans, another essential component of guideline-based care, are provided by only two-thirds of the centers, highlighting further room for improvement.13,14 The use of mucoactive agents remains widespread, reflecting clinical pragmatism rather than strict adherence to current evidence, which shows limited benefit. 15
Conversely, P. aeruginosa eradication strategies appear aligned with evidence-based practice. Most centers consider eradication at first isolation, and 50% use combination systemic plus inhaled therapy, consistent with meta-analytic data showing higher eradication rates with combination regimens compared with systemic therapy alone (48% vs 27%). 16 Clinicians’ experience with long-term inhaled antibiotics and macrolides appears to have expanded compared with 2016, reflecting growing confidence with these evidence-based strategies. However, prescribing restrictions and reimbursement barriers—reported by nearly 40% of centers—remain significant obstacles to their systematic use. Exacerbation management was generally comprehensive: routine microbiological sampling at the onset of an exacerbation was reported by 78.6% of centers, representing a substantial improvement from the 2016 audit, where this practice was recorded in only about 50% of patients. Most centers also reported intensifying airway clearance during exacerbations, in line with current recommendations.
Furthermore, this survey showed marked variability in follow-up practices and routine monitoring. The absence of standardized intervals for functional and microbiological reassessment underscores the need for national and international consensus on surveillance strategies. The 2025 ERS guidelines introduce the concept of the “deteriorating patient,” emphasizing periodic radiological, functional, and microbiological evaluation; however, the routine repetition of chest CT every 1–2 years in many centers may lead to unnecessary cumulative radiation exposure, calling for more individualized imaging strategies. 9
Several limitations must be acknowledged. First, the survey was conducted before publication of updated guidelines; therefore, clinicians responded based on prior knowledge and local standard operating procedures. Our analysis retrospectively applied the 2025 recommendations, which may not fully reflect contemporaneous expectations at the time of data collection. Second, the study relies on self-reported center-level data without external validation, introducing potential reporting bias. Third, the survey does not include patient-level outcomes, preventing assessment of how adherence to recommendations translates into clinical impact. Finally, although historical comparisons with the 2016 Italian audit offer contextual insight, differences in methodology and survey structure mean that direct quantitative comparisons between the two surveys should be interpreted with caution. Despite these limitations, this study provides the first national, center-level evaluation of alignment with the 2025 ERS Guideline domains. The high response rate (90%) and wide geographic coverage enhance representativeness (Figure 1), and the Delphi-based instrument co-developed with specialists and the national patient association ensures relevance and content validity.
Despite the meaningful progress observed across several domains, relevant heterogeneity persists in key areas, including access to respiratory physiotherapy, availability of rare disease diagnostics, structured longitudinal monitoring, and implementation of patient-centered tools such as written action plans. These findings suggest that, although core components of bronchiectasis care are increasingly established, their integration into a uniformly structured model remains incomplete at the national level.
Systematic center-level evaluations, particularly when integrated with national registry data, may represent a pragmatic strategy to identify gaps, define measurable quality indicators, and support the development of updated, country-specific clinical pathways. Such an approach could facilitate harmonization of care delivery and reduce regional variability in access to specialized services.
Conclusion
This study provides the first national, center-level benchmark of bronchiectasis care in Italy in relation to the 2025 ERS management domains. While substantial progress has been achieved in diagnostic work-up and evidence-based treatment strategies, significant variability persists in physiotherapy access, rare disease diagnostics, structured monitoring, and patient-centered care tools.
Bridging these gaps will require coordinated national efforts, measurable quality indicators, and harmonized care pathways to ensure equitable and consistently high standards of bronchiectasis management across the country.
Supplemental Material
sj-docx-1-tar-10.1177_17534666261459923 – Supplemental material for Evaluating current bronchiectasis care in Italy according to the 2025 European respiratory society recommendations
Supplemental material, sj-docx-1-tar-10.1177_17534666261459923 for Evaluating current bronchiectasis care in Italy according to the 2025 European respiratory society recommendations by Alessandro De Angelis, Vittoria Comellini, Andrea Gramegna, Salvatore Battaglia, Giuliano Montemurro, Angela Bellofiore, Francesco Pagnini, Emilia Privitera, Margherita Ori, Edoardo Simonetta, Mattia Nigro, James D. Chalmers, Donatella Nobile, Francesco Blasi and Stefano Aliberti in Therapeutic Advances in Respiratory Disease
Footnotes
Acknowledgements
The authors wish to express their sincere gratitude to the Associazione Italiana Bronchiectasie (AIB) and to the members of its Scientific Committee for their invaluable collaboration in the design, dissemination, and interpretation of this national survey.
Declarations
Supplemental material
Supplemental material for this article is available online.
Artificial intelligence policy
The authors did not use any Generative Artificial Intelligence (AI) in creating the text, references, figures, or other content of this manuscript. All authors are fully responsible for ensuring the accuracy, originality, and integrity of the submitted material.
Image declaration
The authors declare that all images included in this manuscript were prepared by the authors and have not been previously published elsewhere.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.