
Abstract
Background:
Opportunistic pulmonary infections remain a significant threat in immunocompromised cases.
Objectives:
This study aims to evaluate the impact of early therapeutic modalities on 28-day mortality in non-AIDS and non-solid tumor immunocompromised patients hospitalized with opportunistic pulmonary infections, and to identify associated prognostic factors.
Design:
This multicenter retrospective study enrolled immunocompromised patients with opportunistic pulmonary infections from four respiratory centers between January 2022 and December 2024 to delineate their clinical characteristics and prognostic factors. The 28-day mortality was defined as the primary clinical outcome.
Methods:
Multivariate logistic analysis was utilized to identify the independent prognostic factors for 28-day mortality. Moreover, a predictive nomogram was constructed and validated.
Results:
A total of 127 patients were included. Differences in pathogen distribution, laboratory tests at admission, and treatment strategies were identified between survivors and non-survivors. A multivariate analysis suggested that longer time from onset to pathogen-targeted therapy (OR: 1.047, 95% CI: 1.004–1.091, p = 0.031), more cumulative glucocorticoid dose in the first week of hospitalization (OR: 1.005, 95% CI: 1.001–1.009, p = 0.035), escalation to endotracheal intubation with invasive mechanical ventilation (ETI-IMV, OR: 5.764, 95% CI: 1.137–29.213, p = 0.034), and septic shock development during hospitalization (OR: 9.888, 95% CI: 1.825–53.569, p = 0.008) may be independent risk factors for 28-day mortality, whereas pathogen-targeted therapy within 72 h after admission (OR: 0.200, 95% CI: 0.044–0.914, p = 0.038) was protective. By incorporating the five variables mentioned above, a nomogram demonstrated good discriminative ability and reliability.
Conclusion:
Early recognition, timely targeted antimicrobial therapy, and minimized glucocorticoid use are crucial to immunocompromised subjects suffering opportunistic pulmonary infections, which could prevent the escalation to ETI-IMV and septic shock, thereby reducing mortality.
Introduction
According to the Global Burden of Disease Study 2021, 1 lower respiratory infections (excluding COVID-19) were the seventh leading cause of age-standardized mortality globally, posing a significant threat to human health. There has been a rise in the number of immunocompromised patients attributed to the progression in immunosuppressive therapy for autoimmune diseases, as well as an increase in solid organ transplantation and hematologic malignancies. 2 Especially, pulmonary infections remain a significant contributor to higher morbidity and mortality rates in immunocompromised patients.3,4 Therefore, more attention should be paid to immunocompromised patients who suffer from pulmonary infections, who are more prone to acute hypoxemic respiratory failure, leading to worse outcomes. 5
Previously, clinical characteristics and risk factors of pulmonary infections in immunocompetent patients have been reported.6–9 However, few attempts have been made with respect to immunocompromised patients. Limited studies about immunocompromised patients only focus on specific pathogen-related pneumonia, such as Pneumocystis pneumonia (PCP), or influenza-related pneumonia,10,11 while others may be confined to specific subtypes of immunocompromised conditions.12–14 Moreover, few studies have conducted integrated analyses of post-hospitalization treatment modalities for immunocompromised patients with pulmonary infections. 15 Collectively, the real-world data of this vulnerable population were limited in existing clinical reports.
Therefore, to further describe the condition of opportunistic pulmonary infections in immunocompromised patients, we designed this multicenter retrospective study to investigate the clinical characteristics, risk factors, and predictors of outcome in these patients. Notably, both pre-hospital and post-hospital treatment for this vulnerable population were analyzed. Accordingly, the clinical-mortality nomogram model was established to determine the importance of each independent prognostic factor to 28-day mortality.
Methods and materials
Study design and population
This study retrospectively analyzed the clinical characteristics of immunocompromised patients with opportunistic pulmonary infections from four respiratory centers across China between January 2022 and December 2024. The reporting of this study conformed to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement 16 (Supplemental File 1). Patients were divided into survival and non-survival groups based on 28-day survival.
For inclusion in this study, patients were required to meet all of the following criteria: (1) Diagnosis of autoimmune disease, solid organ transplantation or hematologic malignancies; (2) Current immunosuppressive therapy with any of the following: (a) Corticosteroid therapy with a dose ⩾20 mg prednisone or equivalent daily for ⩾14 days or a cumulative dose >600 mg of prednisone17,18; (b) Treatment with biological immune modulators19,20; (c) Treatment with disease-modifying antirheumatic drugs or other immunosuppressive drugs (e.g., cyclosporin, cyclophosphamide, hydroxychloroquine, methotrexate) 21 ; (3) Pulmonary infection; (4) Patients received pathogen-targeted therapy. Exclusion criteria were as follows: (1) Patients who are HIV-Ab positive; (2) Patients after radiotherapy or chemotherapy for solid tumors. Primary outcomes were defined as all-cause mortality at 28 days from the date of admission.
Data collection
Patient data were extracted from the electronic medical record system. The baseline data collected included demographics, underlying diseases, and immunosuppressants. The microbiological data collected included pathogens isolated from the lower respiratory tract (LRT), bronchoalveolar lavage fluid (BALF) metagenomic next-generation sequencing (mNGS) results, BALF galactomannan (GM) test results, and peripheral blood cytomegalovirus (CMV) DNA test. The laboratory data included white blood cell (WBC), lymphocyte, monocyte, neutrophil, neutrophil-to-lymphocyte ratio (NLR), platelet, C-reactive protein (CRP), lactate dehydrogenase (LDH), D-dimer, and procalcitonin (PCT). The post-hospitalization treatments included pathogen-targeted therapy, glucocorticoid treatment, and respiratory support. Thus, the data on time from onset to pathogen-targeted therapy, pathogen-targeted therapy within 72 h after admission, total glucocorticoid dose in 7 days following hospital admission, oxygenation index (OI) at admission, escalation to endotracheal intubation with invasive mechanical ventilation (ETI-IMV), and septic shock during hospitalization were collected.
Disease definition
Pneumonia was confirmed by the presence of a new pulmonary infiltrate on chest X-ray, combined with at least two of the following: cough, sputum production, temperature exceeding 38°C or falling below 35°C, auscultatory signs indicative of pneumonia, CRP levels above 15 mg/L, leukocyte counts >10 × 109/L or <4 × 109/L, or >10% rods in leucocyte differentiation. 22 There is currently no clear definition of opportunistic pulmonary infections. In this study, opportunistic pulmonary infections were defined as pulmonary infections caused by conditionally pathogenic microorganisms that generally cause self-limiting diseases in healthy individuals but have serious consequences in immunocompromised hosts. There is currently no clear definition of opportunistic pulmonary infections. Therefore, we established our own operational criteria for this study based on clinical reasoning and published principles in immunocompromised populations. 23 The specific criteria are as follows: (1) Immunocompromised host status; (2) Detection of classic opportunistic pathogens by BALF mNGS or conventional microbiological testing (CMT); (3) Clinical determination of causation based on integrated assessment (clinical presentations, imaging changes, and response to targeted antimicrobial therapy) by two clinicians. Opportunistic pathogens in immunocompromised patients of this study included, but were not limited to: Pneumocystis jirovecii, CMV, Aspergillus spp., Cryptococcus spp., Nocardia spp. identified in LRT samples. In contrast, while gram-negative bacteria such as Acinetobacter baumannii, Pseudomonas aeruginosa, Klebsiella pneumoniae, and Legionella spp. can be detected in immunocompromised patients, they are not pathogens that occur relatively selectively in this population. In our cohort, gram-negative bacteria were consistently detected alongside opportunistic pathogens such as P. jirovecii and CMV, rather than as the sole pathogen identified.
Commonly used clinical scoring systems for sepsis include Systemic Inflammatory Response Syndrome (SIRS), Sequential Organ Failure Assessment (SOFA), and quick Sequential Organ Failure Assessment (qSOFA). SIRS, based on vital signs and WBC count, exhibits high sensitivity but limited specificity. SOFA, which assesses multiple organ functions to identify organ dysfunction, serves as a core tool in the Sepsis-3 definition. qSOFA is utilized for rapid screening of patients with suspected infection to assess the risk of poor outcomes, though it is not an independent diagnostic tool. In immunocompromised patients with concurrent pulmonary infections, these scores should be applied in conjunction with clinical and microbiological findings. 24 The diagnosis of septic shock is based on the presence of suspected infection, requiring vasopressors to maintain a mean arterial pressure ⩾65 mmHg and serum lactate >2 mmol/L without hypovolemia. 25
Pathogen detection
Common sampling methods included sputum cultures, bronchoalveolar lavage (BAL), endotracheal aspirates, and lung biopsies. Multidrug resistance (MDR) was characterized by resistance to ⩾1 antimicrobial agent in three or more drug classes, including aminoglycosides, antipseudomonal β-lactams (carbapenems, cephalosporins, and penicillin/β-lactamase inhibitors), monobactams, fluoroquinolones, and polymyxins. 26 Advanced molecular diagnostics included mNGS for comprehensive pathogen identification and quantitative PCR assays for CMV DNA detection. The BALF-GM test was primarily used to support the diagnosis of invasive pulmonary aspergillosis in immunocompromised individuals. A GM value of 1.0 or greater was considered positive in BALF.
Treatment modalities
Pathogen-targeted therapy was defined as antimicrobial treatment that matched the subsequently identified causative pathogens based on the results of mNGS or PCR, even if initially administered empirically. The cumulative glucocorticoid dose in the first week of hospitalization refers to the amount of systemic methylprednisolone or dexamethasone administered within 7 days from the start of hospital admission. Escalation to ETI-IMV means ETI-IMV was required during hospitalization due to deterioration of systemic conditions, which was not required at admission.
Statistical analysis
Measurement data were tested for normality using the Kolmogorov–Smirnov test and the Shapiro–Wilk test. Continuous variables were expressed as means and standard deviations or medians and interquartile ranges. Categorical variables were presented as frequencies and percentages. Differences between baseline characteristics, pathogens detected, laboratory examination, and treatments of the survival and non-survival group were tested for statistical significance using t tests for normally distributed continuous variables. Wilcoxon rank-sum test for non-normally distributed continuous variables and Pearson’s chi-square test for categorical variables. The binary logistic regression model was used to assess the effect of clinical characteristics on patients’ outcomes. Variables that were statistically significant in univariate analysis (p < 0.05) were included in the multivariate logistic model. Multivariable logistic regression was performed to identify independent prognostic factors for 28-day mortality. Two-tailed p < 0.05 was considered statistically significant. All statistical analyses were performed using IBM SPSS software, version 27.0 (IBM Corp., Armonk, NY, USA). For missing data, patients with >10% missing data were excluded from the analysis. Among the remaining patients, all included variables had a missing proportion of ⩽10%. Missing values for continuous variables were imputed using median imputation. 27
Nomogram construction and validation
A nomogram was developed based on the multivariate logistic regression results. The model’s discriminatory performance was evaluated by calculating the area under the curve (AUC) of the receiver operator characteristic (ROC).
To ensure internal validation, we performed 1000 bootstrap iterations and obtained a corrected AUC value of the model by setting the number of iterations to 1000. Additionally, calibration was assessed through a calibration plot to evaluate the goodness-of-fit of the nomogram. The nomogram was plotted and validated using the R programming language and environment (http://www.r-project.org/).
Results
Baseline characteristics
The study followed a specific flow chart to conduct every step (Figure 1). Baseline data are detailed in Table 1. A total of 127 immunocompromised patients were included in the final analysis, which predominantly comprised patients with connective tissue diseases (55.1%, n = 70), followed by hematologic malignancies (24.4%, n = 31), nephrotic syndrome (10.2%, n = 13), solid organ transplantation (4.7%, n = 6), and other qualifying conditions (5.5%, n = 7).
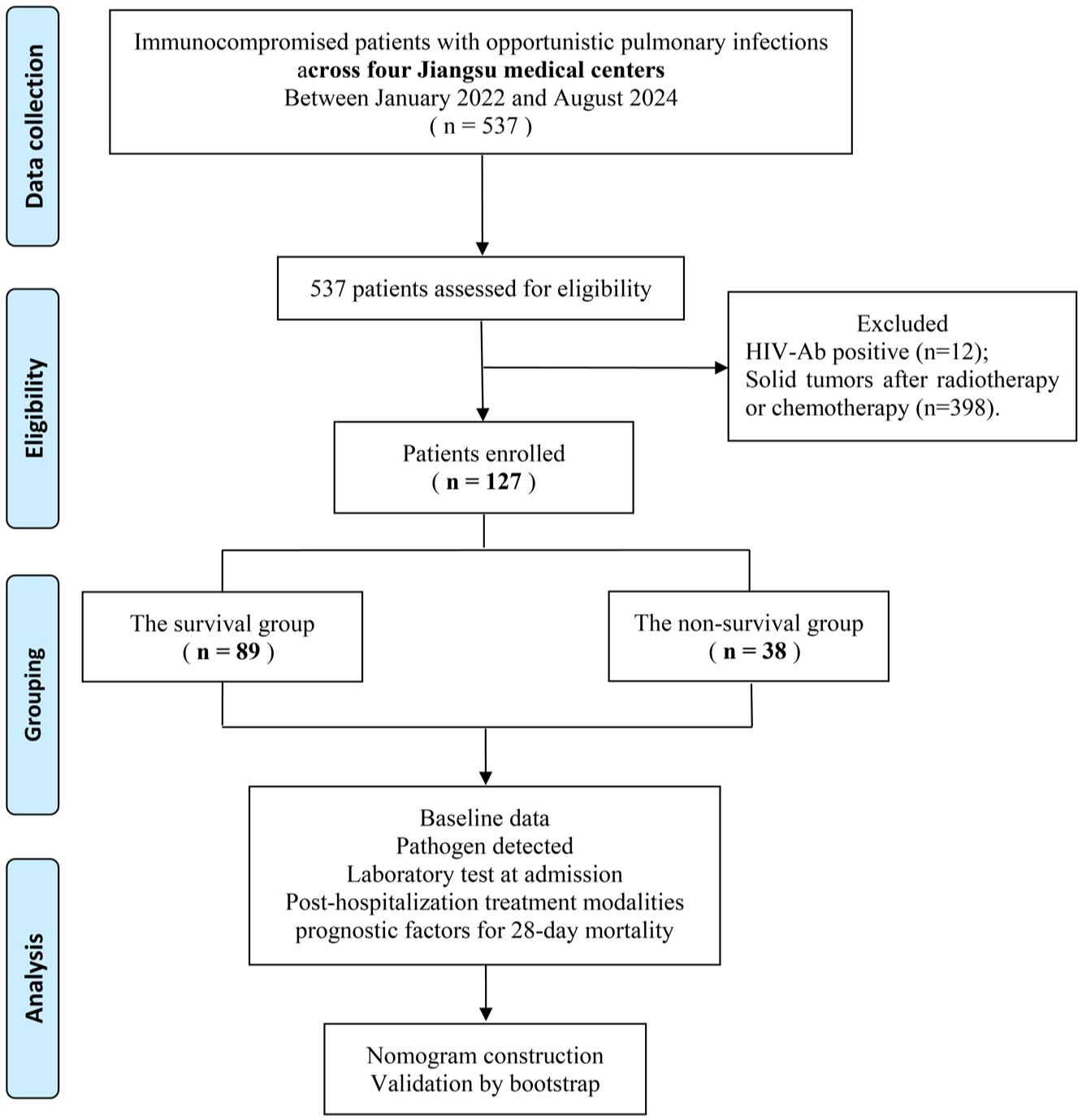
Flow chart of the study.
Baseline data of the patients.
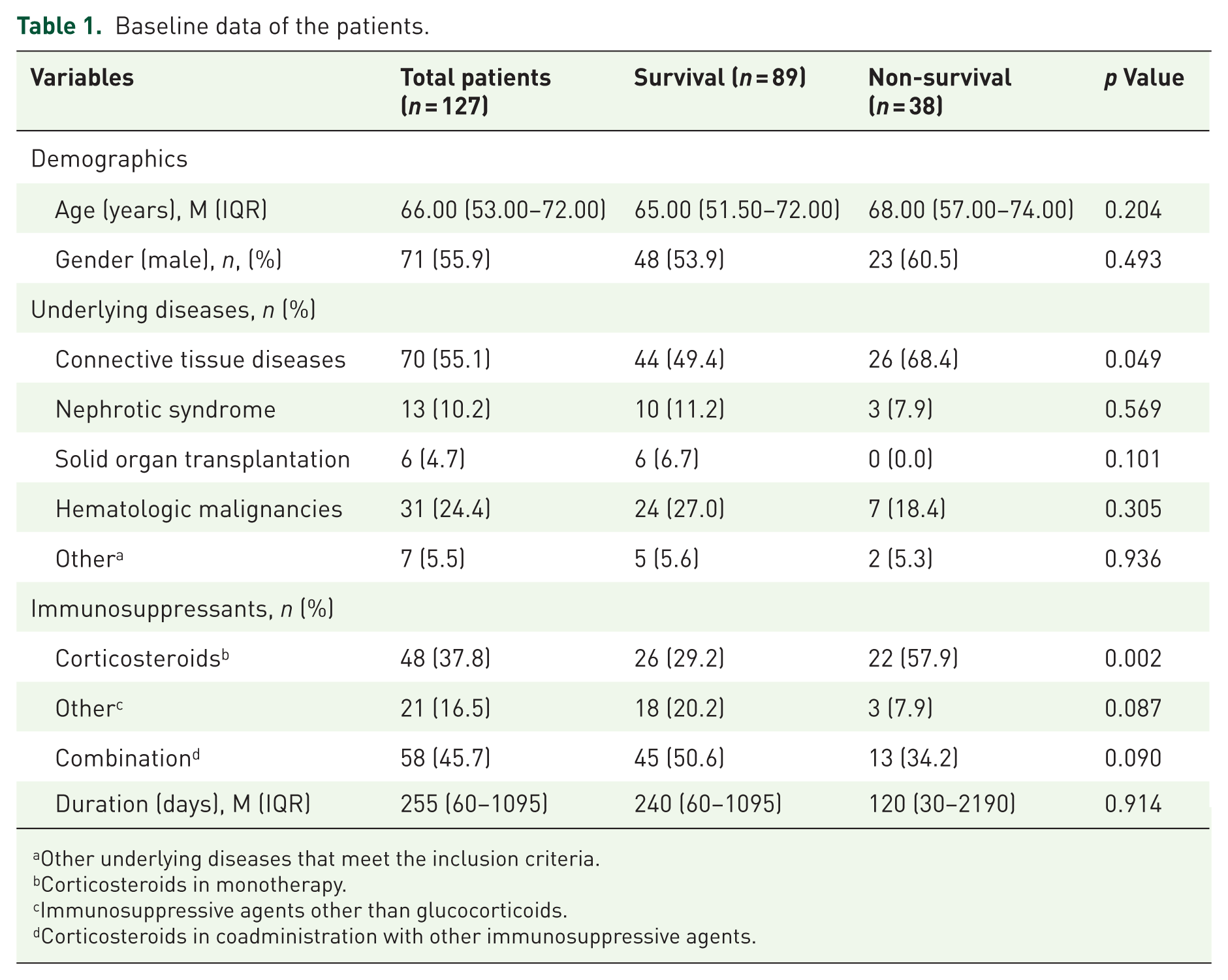
Other underlying diseases that meet the inclusion criteria.
Corticosteroids in monotherapy.
Immunosuppressive agents other than glucocorticoids.
Corticosteroids in coadministration with other immunosuppressive agents.
Demographic characteristics were compared between the survival group (n = 89) and the non-survival group (n = 38). The median age was 65 years in the survival group versus 68 years in the non-survival group (p > 0.05). The proportion of male patients did not differ significantly between groups (53.9% vs 60.5%, p > 0.05). In terms of underlying diseases, the prevalence of connective tissue diseases was higher in the non-survival group than in the survival group. (68.4% vs 49.4%, p = 0.049). Therapeutic histories of immunosuppressant therapy prior to hospitalization revealed that corticosteroid monotherapy was more frequent among non-survivors (57.9% vs 29.2%, p = 0.002), whereas immunosuppressant duration did not differ between groups (p > 0.05).
Comparison of microbial detection between the survival and non-survival groups
Opportunistic pathogens were further detected by BALF-mNGS in 110 enrolled patients (Figure 2), including P. jirovecii (35.5%, n = 39), CMV (31.8%, n = 35), Legionella (1.8%, n = 2), Nocardia (1.8%, n = 2), and Cryptococcus (2.7%, n = 3). Notably, none of these pathogens showed statistically significant differences in detection rates between survival and non-survival groups (all p > 0.05). Consistent with these findings, peripheral blood CMV-DNA assays also demonstrated comparable positivity rates between the two groups (p > 0.05). In contrast, BALF-GM testing revealed a significantly higher positivity rate in non-survivors compared to survivors (35.5% vs 13.0%, p = 0.009), which suggested that Aspergillus infection may represent a life-threatening opportunistic pathogen in immunocompromised individuals (Table 2).
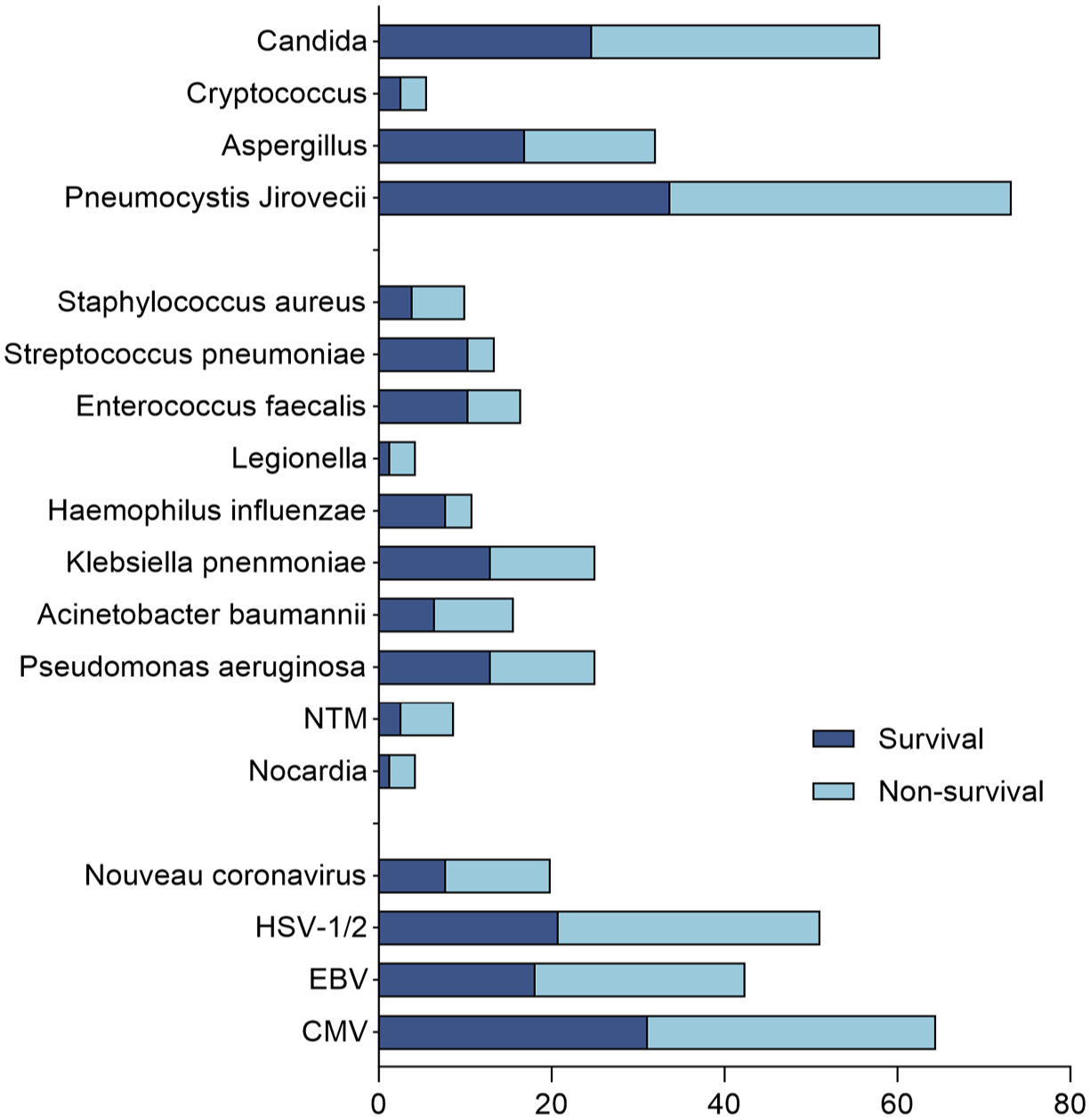
Pathogen distribution detected by mNGS in the two groups.
Characteristics of pathogenic infections.
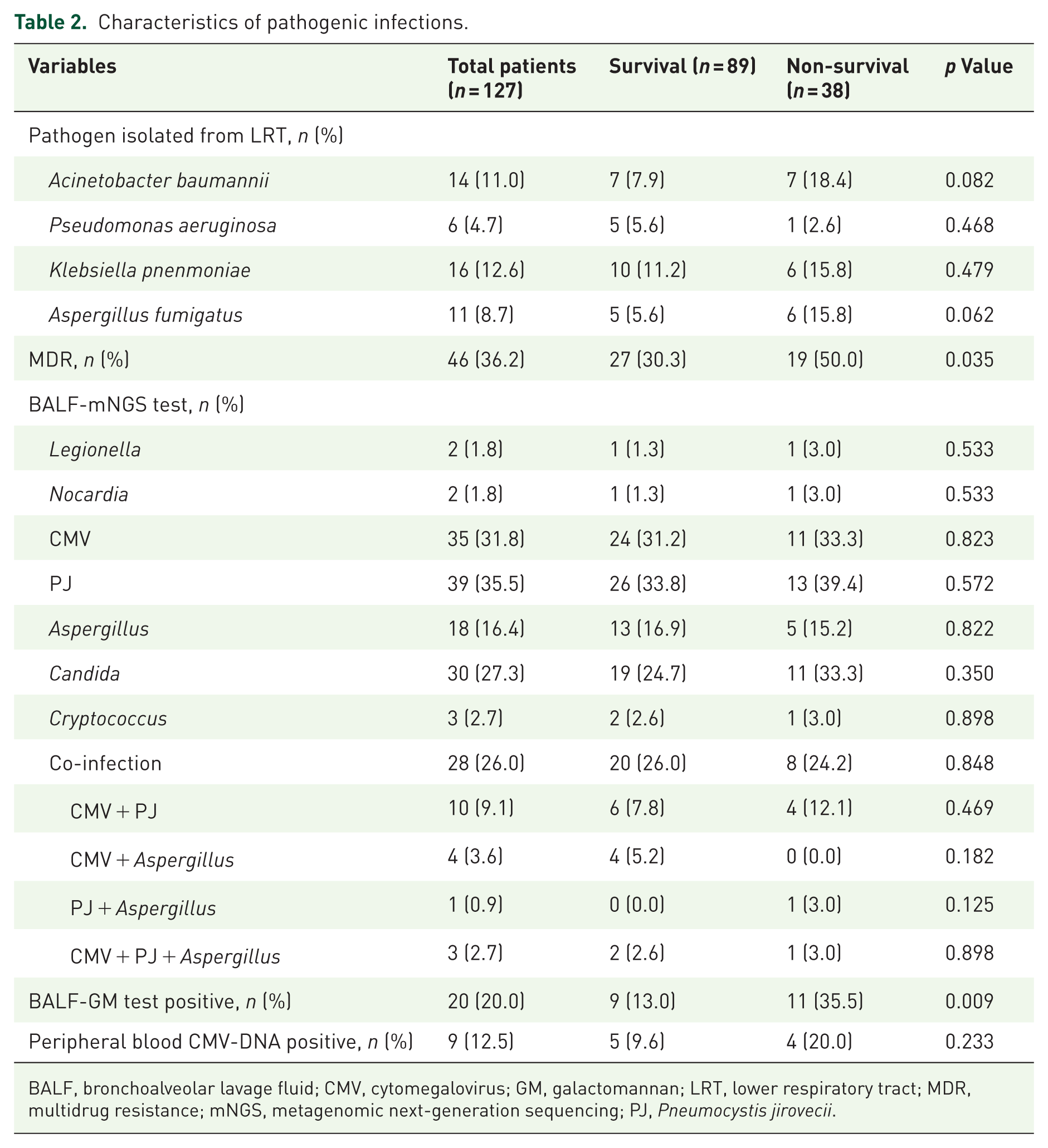
BALF, bronchoalveolar lavage fluid; CMV, cytomegalovirus; GM, galactomannan; LRT, lower respiratory tract; MDR, multidrug resistance; mNGS, metagenomic next-generation sequencing; PJ, Pneumocystis jirovecii.
LRT secretions were also analyzed as potential sources for pathogen detection during the course of treatment (Table 2). Among 127 LRT samples, the most prevalent isolates were K. pneumoniae (n = 16, 12.6%), followed by A. baumannii (n = 14, 11.0%), Aspergillus fumigatus (n = 11, 8.7%), and P. aeruginosa (n = 6, 4.7%). The above detected bacteria were distributed similarly between the survival and non-survival groups. However, the cultured MDR bacteria in the non-survival group were more frequent than those in the survival group (50.0% vs 30.3%, p = 0.035).
Laboratory findings in the survival versus non-survival cohort
Table 3 presents the comparison of admission laboratory parameters between survival and non-survival groups based on 28-day mortality outcomes. The non-survival group demonstrated significantly elevated levels of inflammatory and tissue damage markers, including NLR (14.09 vs 8.02; p = 0.006), CRP (77.53 vs 50.30 mg/L, p = 0.017), LDH (443.10 vs 295.30 U/L; p < 0.001), and PCT (0.29 vs 0.12 ng/mL; p = 0.002). Conversely, lymphocyte counts were significantly reduced in non-survivors (0.53 vs 0.78 × 109/L; p = 0.045). No significant intergroup differences were observed in other hematological parameters, including WBC count, monocyte and neutrophil counts, platelet levels, and D-dimer levels (all p > 0.05; Table 3).
Laboratory test of the patients at admission.
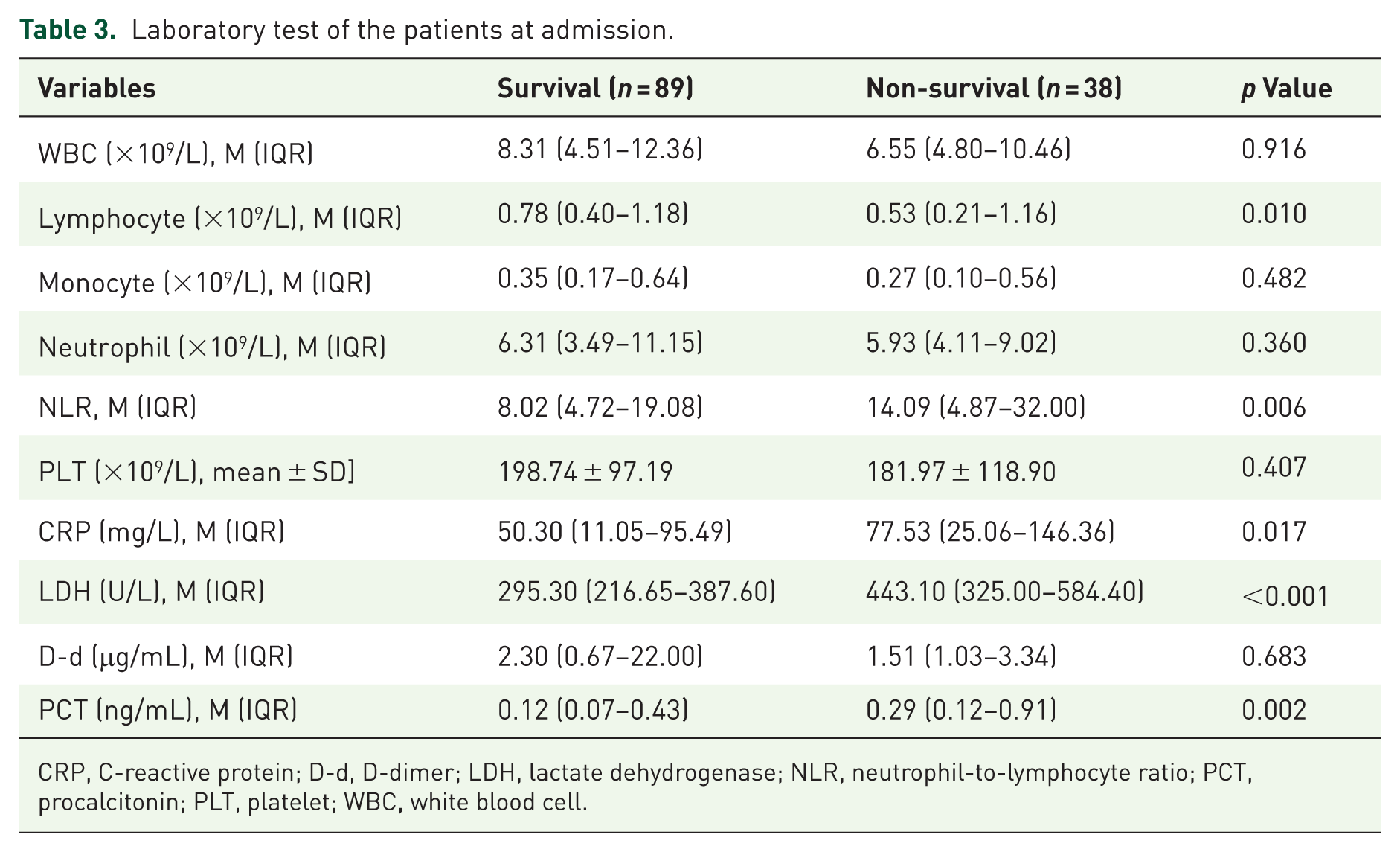
CRP, C-reactive protein; D-d, D-dimer; LDH, lactate dehydrogenase; NLR, neutrophil-to-lymphocyte ratio; PCT, procalcitonin; PLT, platelet; WBC, white blood cell.
Post-hospitalization treatment and clinical outcomes
Although all enrolled patients received a comprehensive post-hospitalization treatment protocol comprising anti-microbial therapy, systemic use of glucocorticoids, and respiratory support, significant differences emerged between survival and non-survival groups regarding treatment timing, intensity, and clinical adjustment (Table 4).
Post-hospitalization treatment modalities.
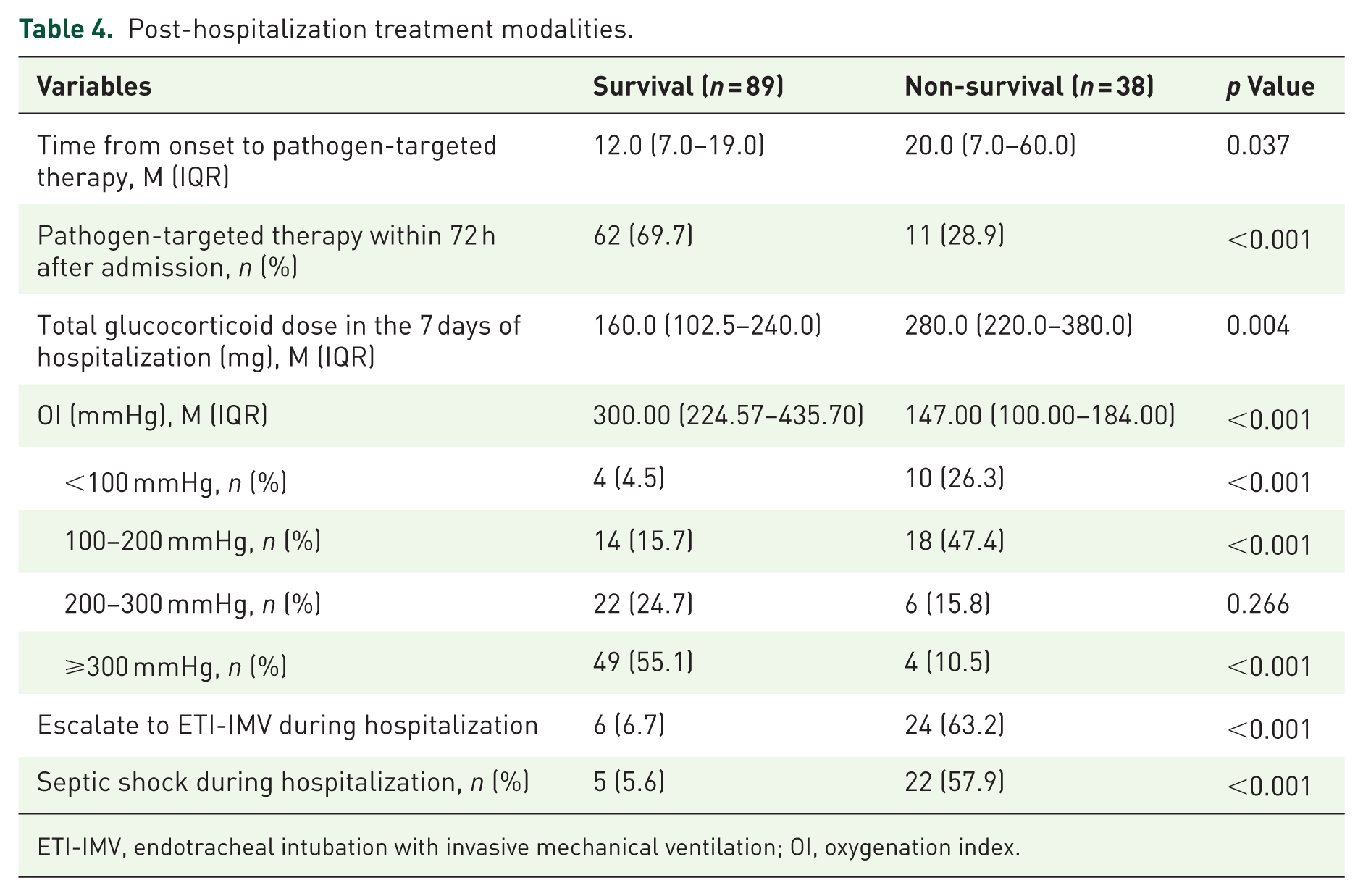
ETI-IMV, endotracheal intubation with invasive mechanical ventilation; OI, oxygenation index.
However, the non-survival group had a longer time from onset to pathogen-targeted therapy than the survival group (20.0 vs 12.0 days; p = 0.037). Pathogen-targeted therapy was initiated within 72 h of admission in only 28.9% of non-survivors, compared with 69.7% of survivors (p < 0.001). These findings underlined the critical importance of early recognition of opportunistic pulmonary infections and initiation of accurate antimicrobial therapy in immunocompromised patients. Moreover, non-survivors received significantly higher cumulative glucocorticoid doses during the first week of hospitalization (280.0 vs 160.0 mg; p = 0.004), which highlighted that more attention needs to be paid to the overuse of glucocorticoids in immunocompromised patients with concurrent infections.
Considering OI serving as a key indicator of disease severity, arterial blood gas analysis was routinely performed at admission. Notably, non-survivors exhibited more impaired oxygenation compared to survivors at admission (147.00 vs 300.00 mmHg; p < 0.001). Escalation to ETI-IMV (63.2% vs 6.7%; p < 0.001) and septic shock development (57.9% vs 5.6%; p < 0.001) during hospitalization were more prevalent among the non-survival group, indicating a worse prognosis (Table 4).
Factors associated with 28-day mortality
To identify prognostic factors in immunocompromised patients with opportunistic pulmonary infections, univariate logistic regression analysis was applied to integrate all the above-mentioned statistically significant variables. Factors with p < 0.05 in the univariate analysis were then analyzed in the multivariable logistic regression model. Multivariable logistic regression demonstrated that longer time from onset to pathogen-targeted therapy (OR: 1.047, 95% CI: 1.004–1.091, p = 0.031), more cumulative glucocorticoid dose in the first week of hospitalization (OR: 1.005, 95% CI: 1.001–1.009, p = 0.035), escalation to ETI-IMV (OR: 5.764, 95% CI: 1.137–29.213, p = 0.034), and septic shock during hospitalization (OR: 9.888, 95% CI: 1.825–53.569, p = 0.008) may be independent risk factors for 28-day mortality. Conversely, pathogen-targeted therapy within 72 h of admission (OR: 0.200, 95% CI: 0.044–0.914, p = 0.038) demonstrated protective effects (Table 5 and Figure 3).
Univariate and multivariate analysis of prognostic factors associated with 28-day mortality.
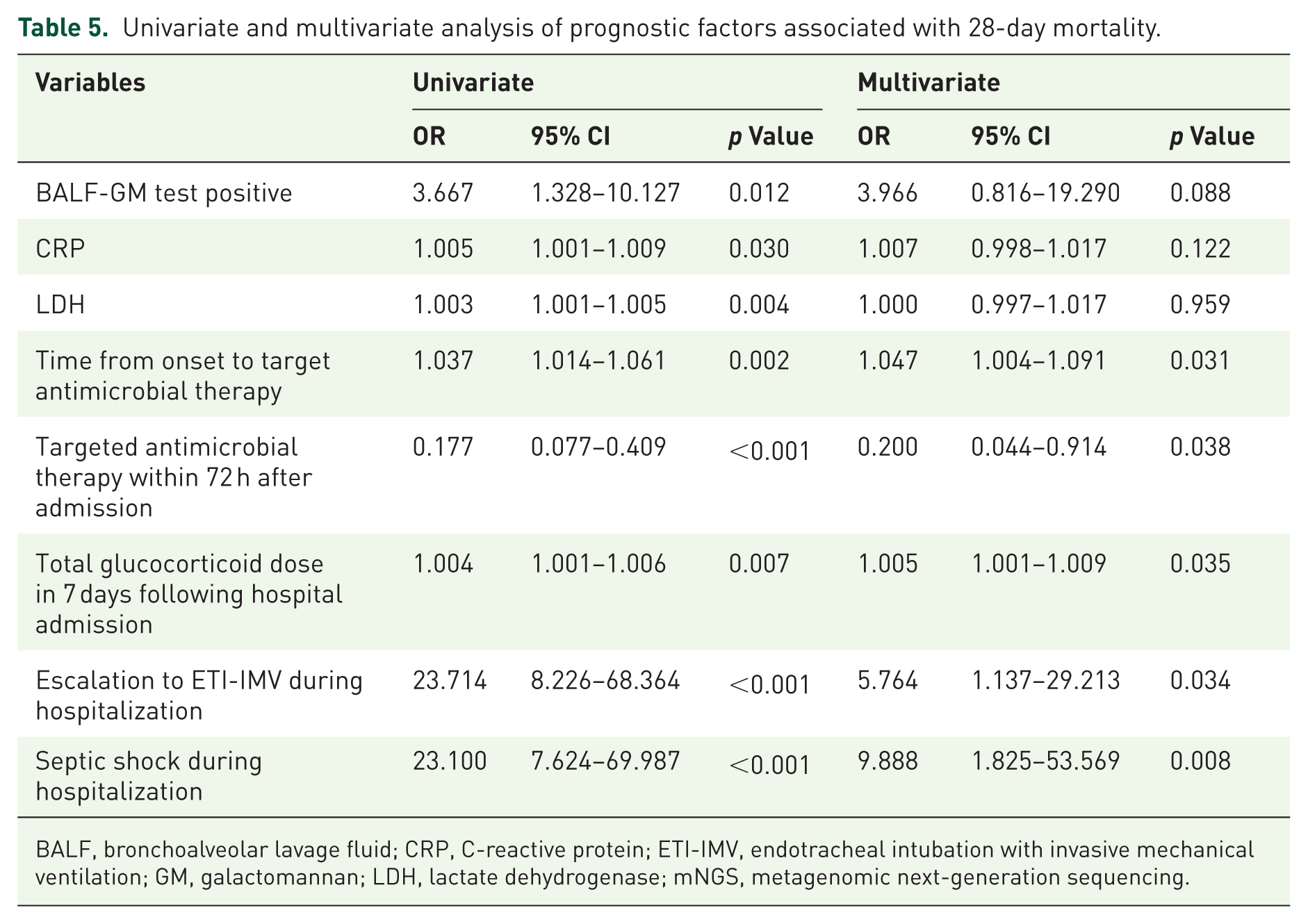
BALF, bronchoalveolar lavage fluid; CRP, C-reactive protein; ETI-IMV, endotracheal intubation with invasive mechanical ventilation; GM, galactomannan; LDH, lactate dehydrogenase; mNGS, metagenomic next-generation sequencing.
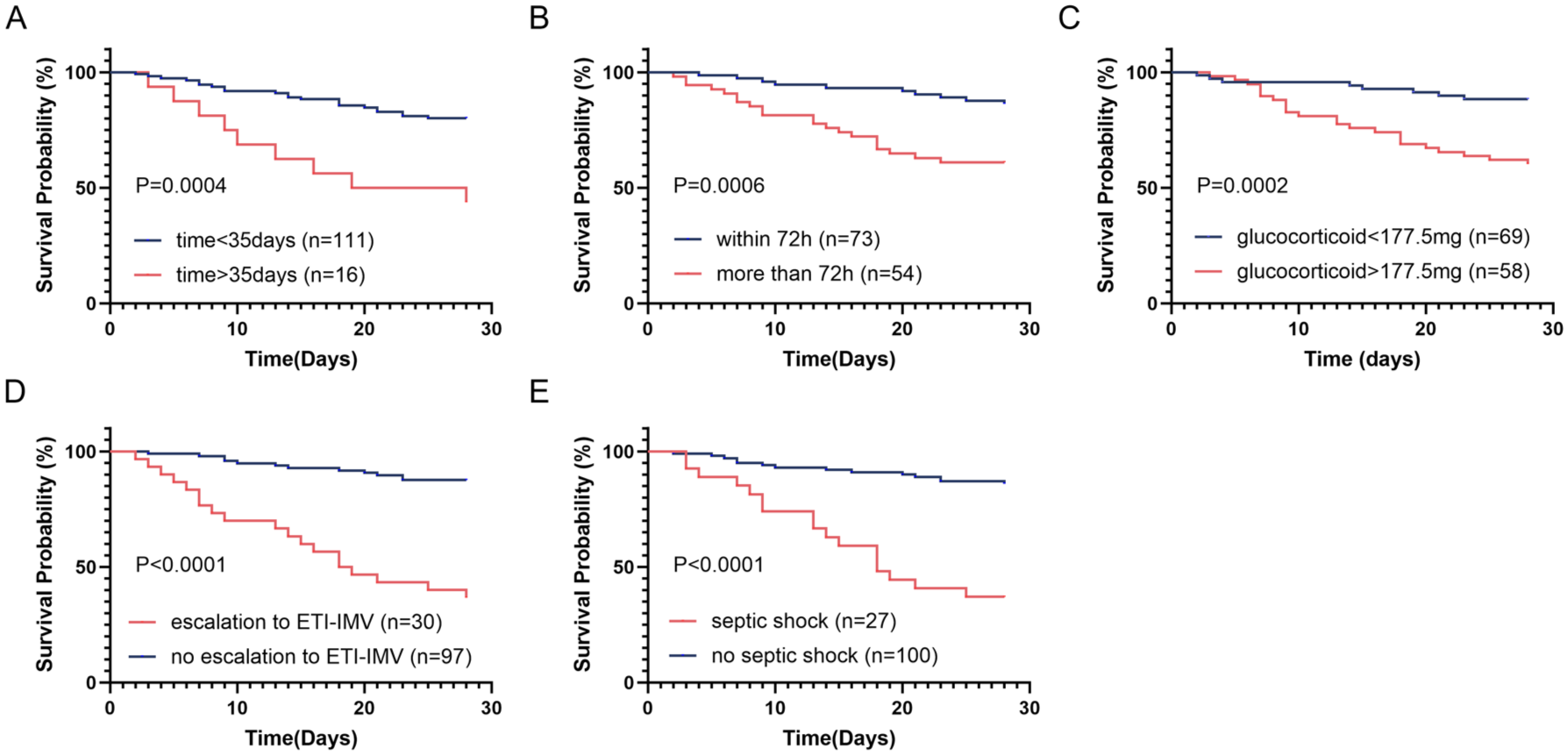
The 28-day survival curve of immunocompromised patients with opportunistic pulmonary infections. (a) Early (⩽35 days from symptom onset) versus delayed (>35 days) pathogen-targeted therapy; (b) pathogen-targeted therapy within 72 h after admission versus pathogen-targeted therapy more than 72 h after admission; (c) low-dose (⩽177.5 mg) versus high-dose (>177.5 mg) glucocorticoid in the first week of hospitalization; (d) escalation to ETI-IMV versus no escalation to ETI-IMV during hospitalization; (e) septic shock development versus non-progression during hospitalization (all p < 0.01).
A nomogram for 28-day mortality
Based on the five independent predictors identified by multivariate analysis, we developed a nomogram to predict 28-day mortality in immunocompromised patients with pulmonary infections (Figure 4(a)). The model revealed that septic shock during hospitalization was the strongest predictor of mortality (highest point contribution), followed by escalation to ETI-IMV, the cumulative glucocorticoid dose within the first week of admission, pathogen-targeted therapy within 72 h of admission, and time from onset to pathogen-targeted therapy. The nomogram demonstrated excellent discriminative ability, with a C-index of 0.893 (95% CI: 0.825–0.962; Figure 4(b)). Internal validation via bootstrapping yielded an optimism-corrected AUC of 0.884 (95% CI: 0.862–0.901), further confirming model robustness. To assess the reliability of the model’s predicted probabilities, we plotted calibration curves, which indicated close agreement between predicted probabilities and observed outcomes across the entire risk spectrum. In summary, through internal validation, we confirmed the stability and reliability of the nomogram. Furthermore, we analyzed the timing of the above two critical deterioration events. Among all enrolled patients, the mean time from hospital admission to septic shock diagnosis was 7.3 days. Similarly, the mean time from admission to escalation to ETI-IMV was 5.2 days. Accordingly, the nomogram could be better applicable by day 7 after admission.
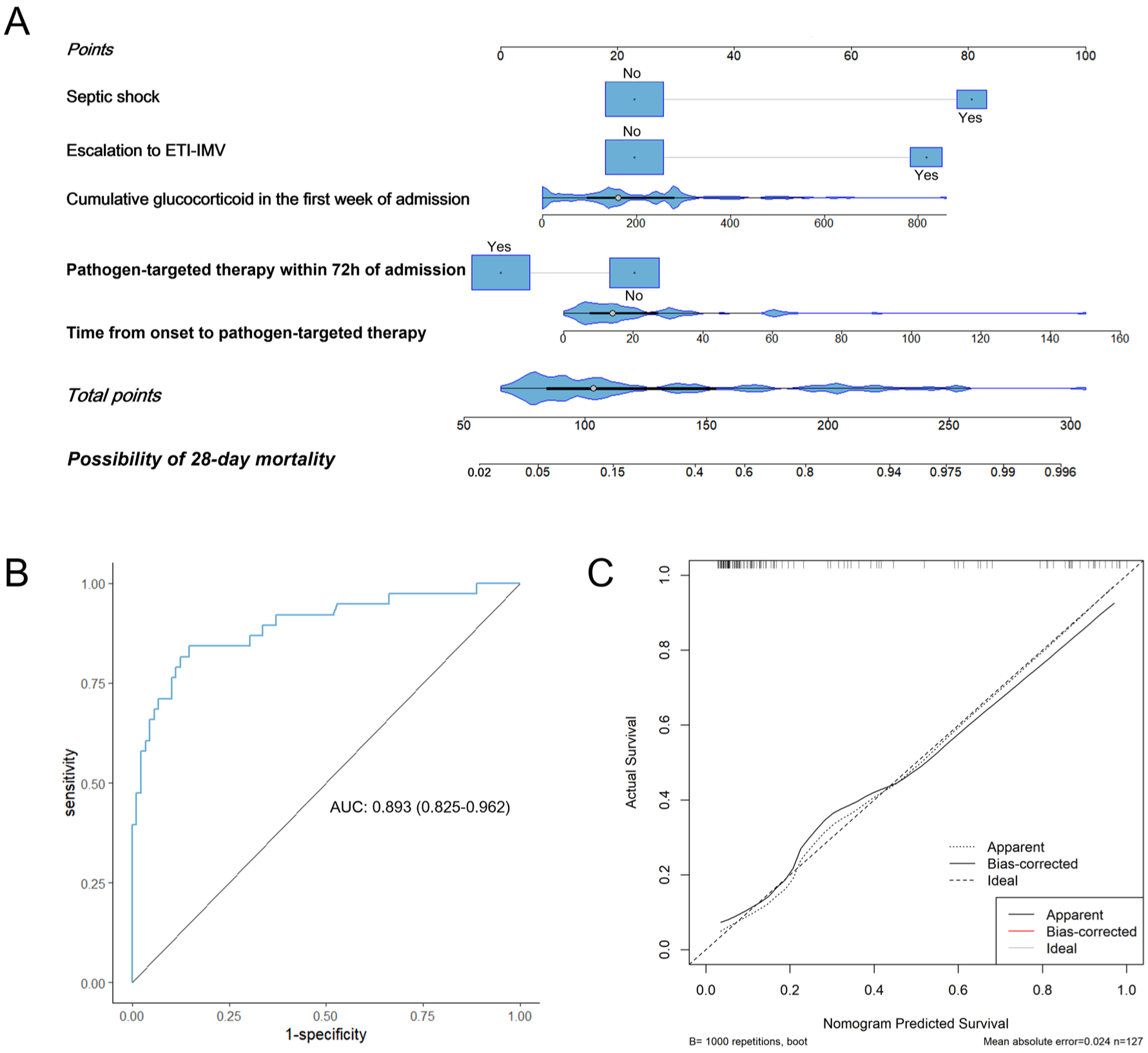
The construction and validation of a nomogram for independent prognostic factors. (a) The construction of a nomogram for 28-day mortality prediction based on the significant variables from the multivariate logistic regression analysis. (b) A ROC curve for the discriminative validation of the nomogram with a C-index of 0.893 (95% CI: 0.825–0.962). (c) A calibration curve for the estimation of agreement between the predicted 28-day mortality of the nomogram and the actual 28-day mortality.
Discussion
This multicenter, real-world study focused on immunocompromised patients of non-AIDS and non-solid tumor receiving corticosteroids and/or other immunosuppressants for underlying conditions. The clinical data of these patients were systematically characterized, revealing significant differences in admission laboratory tests and treatment strategies between survivors and non-survivors. Furthermore, we identified key independent predictors of 28-day mortality that may facilitate early risk stratification and inform therapeutic decision-making in this vulnerable population.
Previous studies have suggested that immunocompromised status is an independent risk factor for mortality in patients with opportunistic pulmonary infections. 28 However, Studies on risk factors for mortality of opportunistic pulmonary infections in immunocompromised patients are scarce and inconsistent in their findings. For instance, some retrospective studies29,30 concluded that neutrophil count was an independent risk factor associated with death in immunocompromised patients with severe pneumonia, which was not replicated in the present study. There have been studies10,31,32 showing that a high level of LDH can be one of the factors contributing to a poor survival outcome in immunocompromised patients of non-AIDS, which also differed from the findings of our study. Li et al. 33 concluded that IMV was significantly associated with increased 30-day mortality, which was congruent with the result of this study. Moreover, this present study extends current knowledge by demonstrating that time from onset to pathogen-targeted therapy, pathogen-targeted therapy within 72 h after admission, the cumulative glucocorticoid doses during the first week of hospitalization, escalation to ETI-IMV, and septic shock development during hospitalization were also independent prognostic factors for 28-day mortality in non-AIDS and non-solid tumor immunocompromised patients with pulmonary infections.
Notably, most patients have a history of long-term corticosteroid use prior to admission to the hospital. Corticosteroids have been proven to increase the risk of various infections, especially in immunocompromised individuals.34,35 Previous studies have demonstrated a significant association between corticosteroid use and increased mortality in this population, 36 which was consistent with our results. Specifically, our study also revealed that a higher cumulative glucocorticoid dose in the first week of hospitalization increased mortality in immunocompromised patients with opportunistic pulmonary infections, which was probably because corticosteroids have adverse effects on hemodynamic stability and increased risk of hyperglycemia. 35 Consequently, when considering corticosteroid therapy in immunocompromised patients, the immune status of the patient and the underlying immunocompromising disease should be properly assessed. Furthermore, in the treatment of the underlying disease, corticosteroid dose reduction should be considered when combined with immunosuppressive agents to minimize cumulative immunosuppressive effects.
Immunocompromised individuals demonstrate heightened susceptibility to fungal and viral pathogens. 37 BALF mNGS identified P. jirovecii and CMV as the predominant pathogens in non-AIDS and non-solid tumors immunocompromised patients of the present study, which caused life-threatening pneumonia in immunocompromised patients.38,39 Meanwhile, this study encompassed diverse pathogen-associated pneumonias rather than focusing on a single etiology. These features may account for the observed discrepancies with previous studies and enhance the clinical generalizability of our findings. Another study has reported significantly higher 30-day mortality rates in patients with CMV co-infection compared to those with P. jirovecii alone, 40 which was not shown in our findings. In addition, Aspergillus was frequently identified by BALF-mNGS in immunocompromised patients. Despite the lack of independent prognostic value, Aspergillus may still serve as a clinical marker for poor prognosis. 41 The mNGS serves as an exceptionally sensitive diagnostic tool for detecting inpatients with P. jirovecii who are non-HIV immunocompromised, 18 while quantitative PCR provides reliable CMV-DNA quantification. These advanced molecular techniques offer significant diagnostic advantages over traditional microbiological testing, enabling precise pathogen identification and being a cornerstone of effective antimicrobial stewardship. 22 This is particularly crucial for immunocompromised patients, who face elevated risks of severe infections and increased mortality with delayed pathogen-targeted therapy. 42
Our findings demonstrated that although LDH and PCT levels differed significantly between the two groups, these biomarkers did not serve as reliable predictors of mortality in immunocompromised patients with opportunistic pulmonary infections. It was reported that the increase of the tissue damage marker LDH was the most typical characteristic of patients with Pneumocystis jirovecii pneumonia (PJP), and evaluation of PCT can help in the diagnosis and prediction of the severity of Aspergillus infection in immunocompromised patients. 43 This may be attributed to the heterogeneous composition of our study population, which included patients with various pathogens rather than being restricted to P. jirovecii or Aspergillus infections alone.
Respiratory support strategies were tailored based on patients’ OI. In cases of critical respiratory failure, IMV serves as a vital life-sustaining intervention, particularly when acute circulatory failure accompanies refractory hypoxemia. 44 However, IMV may trigger structural and physiological changes in both tissue and microbiota of the lung and may ultimately lead to poor prognosis. 45 Current retrospective studies have demonstrated that the IMV requirement correlates with adverse outcomes in immunocompromised hosts. Dumas et al. 46 found that the need for IMV on the day of admission was a factor associated with in-hospital mortality in immunocompromised patients, while Azoulay et al. 47 pointed out that initial oxygenation did not affect mortality, but escalation to IMV was associated with in-hospital mortality. Consistent with these findings, our analysis revealed that escalation to ETI-IMV during hospitalization can be an independent risk factor for 28-day mortality in immunocompromised patients with pulmonary infections. Its association with adverse outcomes stressed the clinical importance of respiratory monitoring in critically ill immunocompromised patients. Therefore, early recognition and treatments to alleviate symptoms are critical in immunocompromised patients with opportunistic pulmonary infections to reduce the risk of ETI-IMV.
Septic shock occurs when sepsis is related to severe hypotension. Septic shock is the leading cause of death in hospitalized patients. 48 Immunocompromised patients are prone to developing severe infections and are at a heightened risk of septic shock. 34 Paiva et al. 49 suggested that septic shock was an independent risk factor for death in the immunocompromised population with opportunistic infections, which was also shown in our findings. This may be attributed to basic immunodeficiency, which amplifies organ damage.
To reduce the incidence of patients escalating to invasive ventilation and septic shock during hospitalization, it is critical to perform early pathogen-targeted therapy. Pathogen-targeted therapy precisely eliminates the causative pathogen while preserving commensal microbiota, reducing secondary infections, and minimizing the prevalence of MDR. Cillóniz et al. 22 supported that appropriate diagnosis and early initiation of adequate antimicrobial treatment for severe pneumonia are crucial in improving survival among critically ill patients. The present study confirmed this standpoint in immunocompromised patients.
The limitations of the current study are as follows. Firstly, despite efforts to standardize treatments, variations across participating centers may have introduced heterogeneity. Additionally, this observational study precludes definitive causal inferences, and residual confounding may persist despite our comprehensive adjustment for known prognostic factors. Given its retrospective design, although we have employed multivariable logistic regression to control for known confounding factors to the best of our ability, the completeness of medical records limited our capacity to capture and quantify all complex clinical details that might influence patient outcomes. Moreover, due to the current practical constraints, we were unable to enroll patients from other ethnic groups or countries. Future international prospective studies are needed to identify earlier, modifiable risk factors capable of predicting such clinical deterioration at an earlier time point.
Conclusion
In conclusion, this multicenter study comprehensively investigated a wide spectrum of pathogen detection, laboratory tests at admission, and post-hospitalization treatment in immunocompromised patients with opportunistic pulmonary infections. Our findings contribute to a better understanding of the clinical characteristics and independent prognostic factors in this high-risk cohort. Additionally, we developed and validated a clinical-mortality nomogram for predicting 28-day mortality in this population. However, despite the multicenter design, the study’s limited sample size requires further validation through larger prospective studies to strengthen generalizability.
Supplemental Material
sj-docx-1-tar-10.1177_17534666261459938 – Supplemental material for Impact of early therapeutic modality on 28-day mortality in immunocompromised patients with opportunistic pulmonary infections: a multicenter retrospective study
Supplemental material, sj-docx-1-tar-10.1177_17534666261459938 for Impact of early therapeutic modality on 28-day mortality in immunocompromised patients with opportunistic pulmonary infections: a multicenter retrospective study by Shiying Guo, Linlin Wang, Jinfang Shi, Xiaoyan Sai, Suping Tang, Jiajia Wang, Anqi Wang, Dong Qiu, Shuguang Han, Yan Wu and Cheng Chen in Therapeutic Advances in Respiratory Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.