
Abstract
Background:
Pulmonary vascular involvement represents one of the most severe manifestations of Behçet’s disease. Pulmonary artery aneurysm (PAA) and pulmonary artery thrombosis (PAT) are rare but potentially life-threatening complications. However, data regarding their frequency, coexistence, and clinical course remain limited, particularly from a pulmonology-based long-term follow-up perspective.
Objectives:
To evaluate the frequency and clinical characteristics of PAA and PAT in a large single-center Behçet’s disease cohort and to describe diagnostic and therapeutic challenges encountered during routine clinical practice.
Design:
Retrospective single-center observational cohort study.
Methods:
Adult patients diagnosed with Behçet’s disease and followed at a tertiary pulmonology center between January 2014 and January 2024 were retrospectively reviewed. Pulmonary vascular involvement was assessed using contrast-enhanced thoracic computed tomography and CT pulmonary angiography. The presence of deep vein thrombosis (DVT), treatment approaches, and clinical outcomes were recorded.
Results:
Among 279 patients, pulmonary vascular involvement was identified in 9 patients. Pulmonary artery aneurysm was detected in three patients (1.07%), and pulmonary artery thrombosis in six patients (2.1%). Concomitant DVT was observed in a minority of patients with pulmonary vascular involvement. Clinical follow-up revealed heterogeneous disease courses, including aneurysm development during anticoagulant therapy, hemoptysis-related treatment discontinuation, persistent pulmonary thrombosis, and rare interventional complications such as late coil migration. Mortality occurred in patients with severe pulmonary vascular disease.
Conclusion:
Pulmonary vascular complications in Behçet’s disease are rare but associated with significant morbidity and mortality. The coexistence of inflammatory and thrombotic processes creates substantial diagnostic and therapeutic challenges, particularly regarding anticoagulation strategies. Although the limited number of cases precludes definitive conclusions regarding pathogenetic mechanisms, our findings highlight the need for careful, individualized, and multidisciplinary management of pulmonary vascular involvement in Behçet’s disease.
Plain language summary
Behcet's disease is a chronic inflammatory condition that can affect blood vessels throughout the body. Although involvement of the lungs is uncommon, problems affecting the blood vessels in the lungs can be serious and sometimes life-threatening. These problems may include abnormal widening of the pulmonary arteries or the formation of blood clots within these vessels. In this study, we reviewed the medical records of patients with Behcet’s disease who were followed at our center over a 10-year period. Our aim was to better understand how often lung blood vessel problems occur, how they present clinically, and how they are managed in real-life practice. We also evaluated blood clots in the legs, which are common in Behcet’s disease and may coexist with lung involvement. We found that lung blood vessel complications were rare but associated with significant clinical challenges, including bleeding, treatment-related risks, and, in some cases, death. The clinical course varied considerably between patients, highlighting that there is no single approach suitable for all cases. Treatment decisions, particularly regarding the use of blood thinners, were often complex and had to be individualized. Our findings emphasize the importance of careful evaluation of lung symptoms in patients with Behcet’s disease and the need for close collaboration between different medical specialties. Early recognition and personalized management may help reduce serious complications and improve patient outcomes.
Keywords
Introduction
Pulmonary artery aneurysm (PAA) is defined as focal dilation in the main trunk or branches of the pulmonary artery, involving all three layers of the vessel wall and developing beyond normal diameter limits. 1 Pulmonary artery aneurysms (PAAs) are rare but potentially life-threatening vascular abnormalities. Although their incidence is low, they can pose significant diagnostic and therapeutic challenges. Pulmonary artery aneurysm is defined as a localized dilatation of the pulmonary artery beyond its normal diameter. The development of PAAs has been associated with various pathogenetic mechanisms. The most common etiologic factors include congenital heart diseases, infectious agents (bacterial or fungal), iatrogenic or traumatic arterial injury, and vasculitic inflammation. 2 Among the types of vasculitis, Behçet’s disease has been reported as the most frequent cause of pulmonary artery aneurysms. 3
Vascular involvement in Behçet’s disease is not limited to PAA; DVT, the most common form of venous involvement, can lead to significant morbidity, while PAT, although less frequent, remains an important life-threatening complication. 4 Pulmonary artery thrombosis (PAT) may be associated with clinical outcomes such as infarction, atelectasis, and hemoptysis, and in some cases, it occurs concurrently with aneurysms. Therefore, when PAA, PAT, and DVT are evaluated together in Behçet’s disease, the full scope and clinical impact of vascular involvement can be more clearly appreciated.5–7
Behçet’s disease is a chronic systemic form of recurrent and relapsing vasculitis. The vascular inflammation can involve multiple organs, including the skin, joints, eyes, mucosa, vessels, arteries, nervous system, and gastrointestinal tract 8 Behçet’s disease is typically diagnosed during the third and fourth decades of life, is slightly more common in men than in women, and tends to present with more severe features in young adult males. 7 Although Behçet’s disease is most prevalent in countries along the ancient Silk Road the highest prevalence of approximately 420 cases per 100,000 population has been reported in Turkey. 9
Behçet’s disease can involve the vascular system in approximately 25%–30% of cases. Pulmonary involvement is uncommon, with an overall reported incidence of less than 5%, among which pulmonary artery involvement is the most frequent. Pulmonary artery aneurysm tends to be the most life-threatening complication of Behçet’s disease. 10 These cases are often characterized by massive hemoptysis, bilateral hilar opacities on imaging, and high mortality rates. Moreover, PAA is not the only form of arterial involvement; “in situ” PAT is also observed in approximately one-third of patients. With advances in imaging techniques, the recognition of PAT appears to be increasing. 11
Although Turkey is one of the countries with the highest prevalence of Behçet’s disease, data on pulmonary artery involvement are limited to a small number of case series.10,12 Therefore, increasing awareness of the diagnosis and management of pulmonary vascular complications such as PAA and PAT is important. In particular, early evaluation from a pulmonology perspective of patients whose initial presentation is hemoptysis or, in some cases, who do not yet meet the diagnostic criteria for Behçet’s disease except for isolated pulmonary artery involvement is critical for both diagnosis and subsequent treatment and follow-up.
In this context, our study aims to retrospectively examine the frequency and clinical characteristics of pulmonary artery aneurysm, pulmonary artery thrombosis, and deep vein thrombosis in Behçet’s patients followed at our center from a pulmonology perspective, with the goal of contributing to improved diagnostic and follow-up processes.
Materials and methods
This study was designed as a retrospective cohort analysis. Medical records of patients followed with a diagnosis code of Behçet’s disease at our center between January 2014 and January 2024 were retrospectively reviewed. Patients included were those with a confirmed diagnosis according to the International Criteria for Behçet’s Disease (ICBD) 8 and aged ⩾18 years.
All patients registered under the diagnosis code “Behçet’s disease” during the study period were screened. Patients aged < 18 years, those with incomplete clinical records, and those with concomitant systemic autoimmune diseases were excluded. Cases whose medical history, physical examination findings, and laboratory data fulfilled the International Criteria for Behçet’s Disease (ICBD) were included in the study cohort.
Thoracic contrast-enhanced CT and/or CT pulmonary angiography were not routinely performed in all Behçet’s disease patients. Imaging evaluation for pulmonary vascular involvement was limited to patients who underwent thoracic imaging because of pulmonary symptoms or clinical suspicion of thoracic involvement, including hemoptysis, dyspnea, chest pain, or suspected pulmonary embolism. The presence of pulmonary artery aneurysm (PAA), pulmonary artery thrombosis (PAT), and additional vascular involvement was evaluated retrospectively in this imaging-defined subgroup. Lower extremity deep vein thrombosis (DVT) data were assessed only in patients with available vascular imaging or documented radiological evaluation during follow-up.
Demographic characteristics (age, sex), clinical findings, and laboratory data were recorded. Vascular involvement was specifically assessed, and the presence of DVT, PAA, and pulmonary embolism (PE) was investigated. The diagnosis of PAA and PAT was based on contrast-enhanced thoracic computed tomography (CT)/CT pulmonary angiography and/or magnetic resonance imaging (MRI), while DVT was assessed using Doppler ultrasonography. Aneurysmal vascular dilatation was defined as a focal increase in vessel diameter of at least 1.5–2 times compared with the adjacent proximal arterial segment and/or the accompanying segmental bronchial diameter. In segmental or peripheral pulmonary arterial branches, aneurysm evaluation was performed according to both the proximal vascular caliber and the adjacent bronchial diameter on thoracic imaging. In addition to pulmonary vascular involvement, other vascular aneurysms detected during follow-up were also recorded.
Treatment approaches including corticosteroids, immunosuppressive agents (azathioprine, cyclophosphamide), biologic therapies (anti-TNF agents), and anticoagulants were recorded. Treatment evaluations were performed only for patients with identified vascular complications (e.g., those diagnosed with DVT, PAA, or PAT). Additionally, relapses, complications, and mortality data occurring during follow-up were also reviewed.
The primary endpoint of the study was to determine the frequency of PAA, DVT, and PAT in patients with Behçet’s disease. Secondary endpoints included the treatment strategies applied and clinical events that occurred during the follow-up period.
Statistical analysis
Data obtained were analyzed using SPSS version 25.0 (IBM Corp., Armonk, NY, USA). Analyses were conducted using descriptive statistics, and prevalences were calculated using nominal data.
This study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement guidelines for observational cohort studies. 13
Results
In this study, a total of 279 patients diagnosed with Behçet’s disease over the past 10 years were retrospectively evaluated. Of these, 138 were female and 141 were male, with a mean age of 46.38 ± 12.96 years (range: 21–79) (Table 1). The group with vascular involvement consisted of 41 patients, 30 of whom were male (73.2%) and 11 female (26.8%); the average age was 48 years. In this group, mortality was observed in seven patients during the follow-up period (17.1%). The group without vascular involvement consisted of 238 patients, 110 of whom were male (46.2%) and 128 female (53.8%); the average age was 46 years. In this group, mortality was also observed in seven patients during the follow-up period (2.9%).
Demographic and baseline clinical characteristics of the study population.
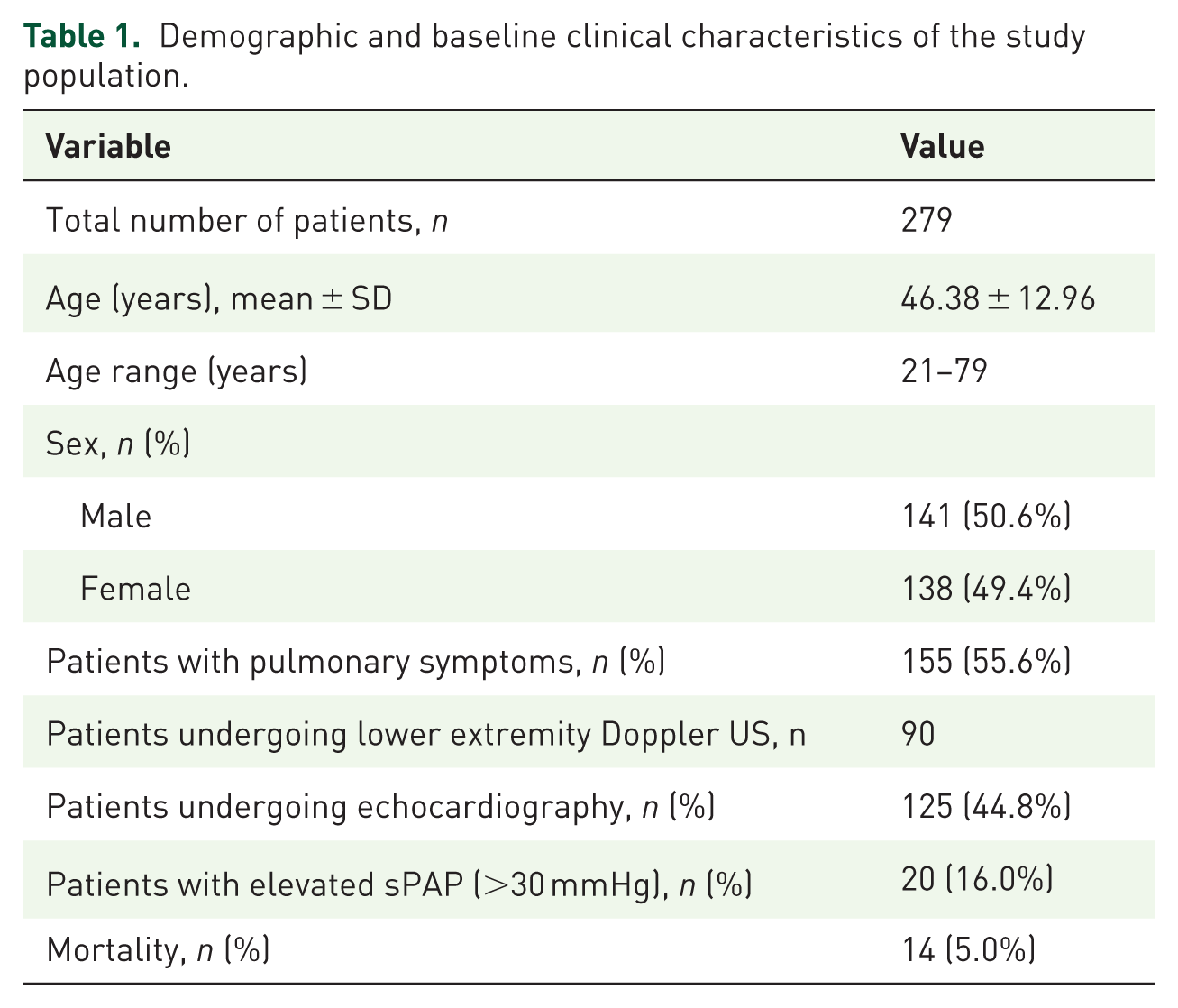
Among 155 patients presenting with pulmonary symptoms (dyspnea, chest pain, hemoptysis, etc.), thoracic CT as part of an embolism panel identified PAT in 6 patients and PAA in 3 patients (Table 2). Among 90 patients with lower extremity symptoms, venous Doppler ultrasonography detected DVT in 29 patients (21 males, 8 females). One patient had a non-complicated ascending thoracic aortic aneurysm and one patient had a non-complicated abdominal aortic aneurysm, neither requiring surgical intervention. Additionally, one patient was found to have a right jugular venous aneurysm, which was incidentally detected on cervical Doppler ultrasonography.
Distribution of vascular involvement in Behçet’s disease.
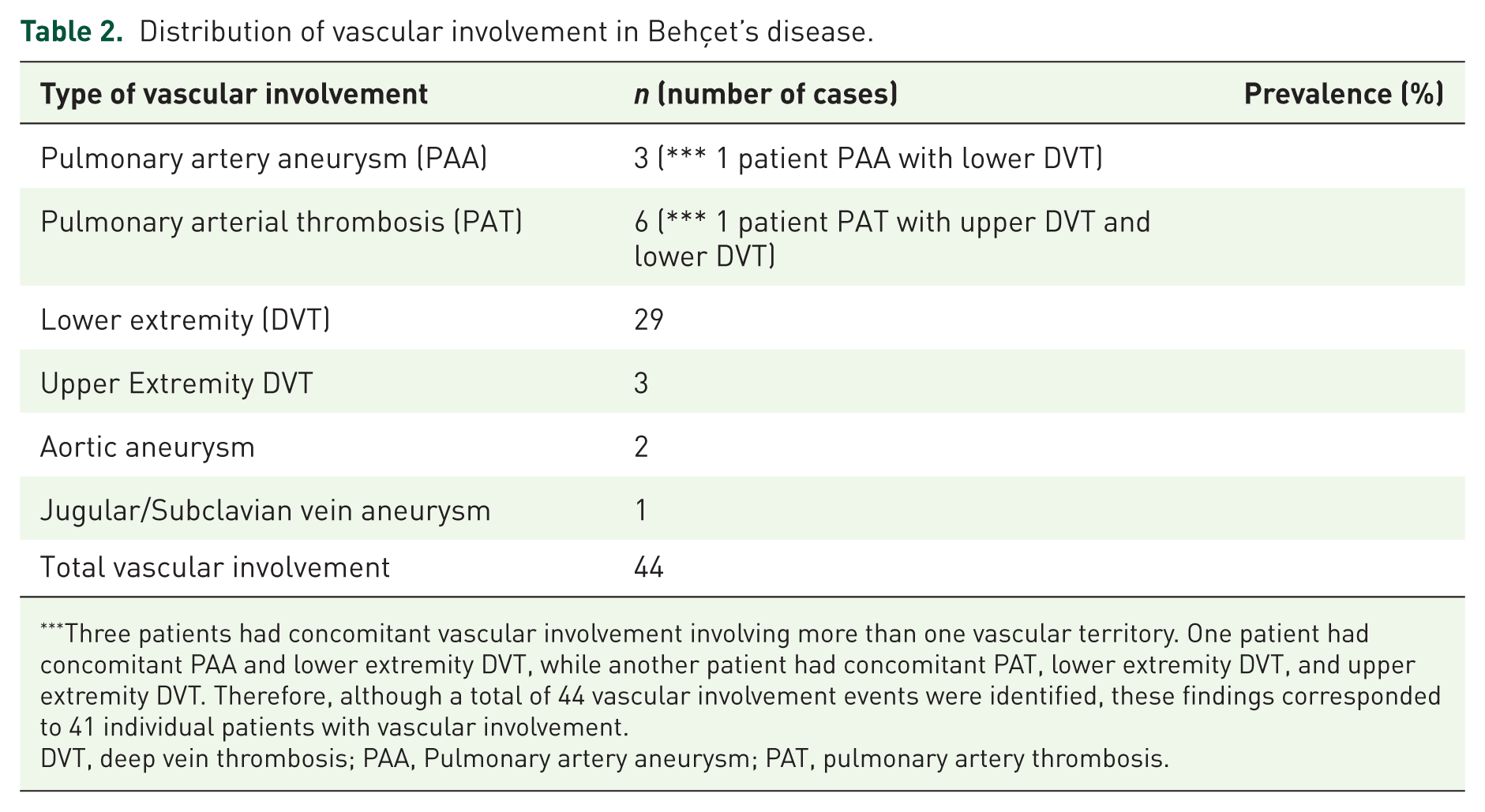
Three patients had concomitant vascular involvement involving more than one vascular territory. One patient had concomitant PAA and lower extremity DVT, while another patient had concomitant PAT, lower extremity DVT, and upper extremity DVT. Therefore, although a total of 44 vascular involvement events were identified, these findings corresponded to 41 individual patients with vascular involvement.
DVT, deep vein thrombosis; PAA, Pulmonary artery aneurysm; PAT, pulmonary artery thrombosis.
Among the three patients with PAA, concomitant DVT was present in only one patient. Similarly, among the six patients with PAT/PE, only one patient had accompanying DVT and additional upper extremity venous thrombosis. Interestingly, these two patients with combined venous and pulmonary vascular involvement were also the cases demonstrating markedly elevated systolic pulmonary artery pressure (sPAP) on echocardiographic evaluation, whereas most patients without concomitant DVT had normal or only mildly increased sPAP values.
Treatment approaches for patients with vascular complications (DVT, PAA, or PAT) were also evaluated. Of these patients, 22 (66.7%) received anticoagulant therapy in addition to anti-inflammatory treatment (corticosteroids and/or immunosuppressive therapy). Five patients (15.1%) received only anti-inflammatory therapy, one of whom showed DVT regression with adjunctive antibiotic therapy. In one patient with an aneurysm of the right external carotid artery, anticoagulant therapy was withheld due to bleeding risk, and only anti-inflammatory treatment was administered. Three patients (9.1%) who started anti-inflammatory therapy were lost to follow-up, and their treatment response could not be assessed. Additionally, one patient had upper extremity venous thrombosis in addition to lower extremity DVT. This patient also had a history of PAT and elevated systolic pulmonary artery pressure (sPAP) and was treated with combined anti-inflammatory and anticoagulant therapy.
Echocardiography (ECHO) was performed in 125 patients, with 20 patients (12 males, 8 females) showing sPAP above the cut-off of 30 mmHg. Among the 20 patients with elevated sPAP, 5 had documented vascular involvement related to Behçet’s disease. Of these, two patients had pulmonary vascular involvement (PAT/PAA), while the remaining patients had other vascular manifestations without documented pulmonary thromboembolic disease. Importantly, all patients with vascular involvement had preserved left ventricular ejection fraction (LVEF approximately 55%–60%), making significant left-sided systolic heart failure unlikely as the primary explanation for PAP elevation. Regarding pulmonary comorbidities, only one patient in the vascular involvement group had a known diagnosis of COPD, while another patient had desquamative interstitial pneumonia with only mild obstructive impairment on pulmonary function testing (FEV1/FVC: 65%). Several patients had no available pulmonary function test data; however, most of these individuals had either no smoking history or only minimal tobacco exposure.
Similarly, among patients without vascular involvement but with elevated sPAP, no clinically significant left heart dysfunction was identified. One patient had a history of mitral valve replacement, and another had mild chronic parenchymal lung disease, while the remaining patients lacked clear alternative causes that would fully explain pulmonary hypertension.
Among the 22 patients who received anticoagulant therapy for vascular involvement, 14 were treated with warfarin, 5 with low-molecular-weight heparin (LMWH), and 3 with rivaroxaban. In five patients, sequential use of more than one anticoagulant was required during the clinical course due to malignancy, need for surgical intervention, or regression of vascular lesions (e.g., transition from warfarin to LMWH in three patients, warfarin to rivaroxaban in one patient, and rivaroxaban to LMWH in one patient). Anticoagulant-related complications were limited. Hemoptysis occurred in one patient with pulmonary artery aneurysm receiving rivaroxaban, leading to a switch to LMWH. One patient on long-term LMWH developed significant menorrhagia, resulting in discontinuation of anticoagulation. In another patient with pulmonary artery aneurysm, warfarin was discontinued due to bleeding risk. No additional major bleeding complications were observed.
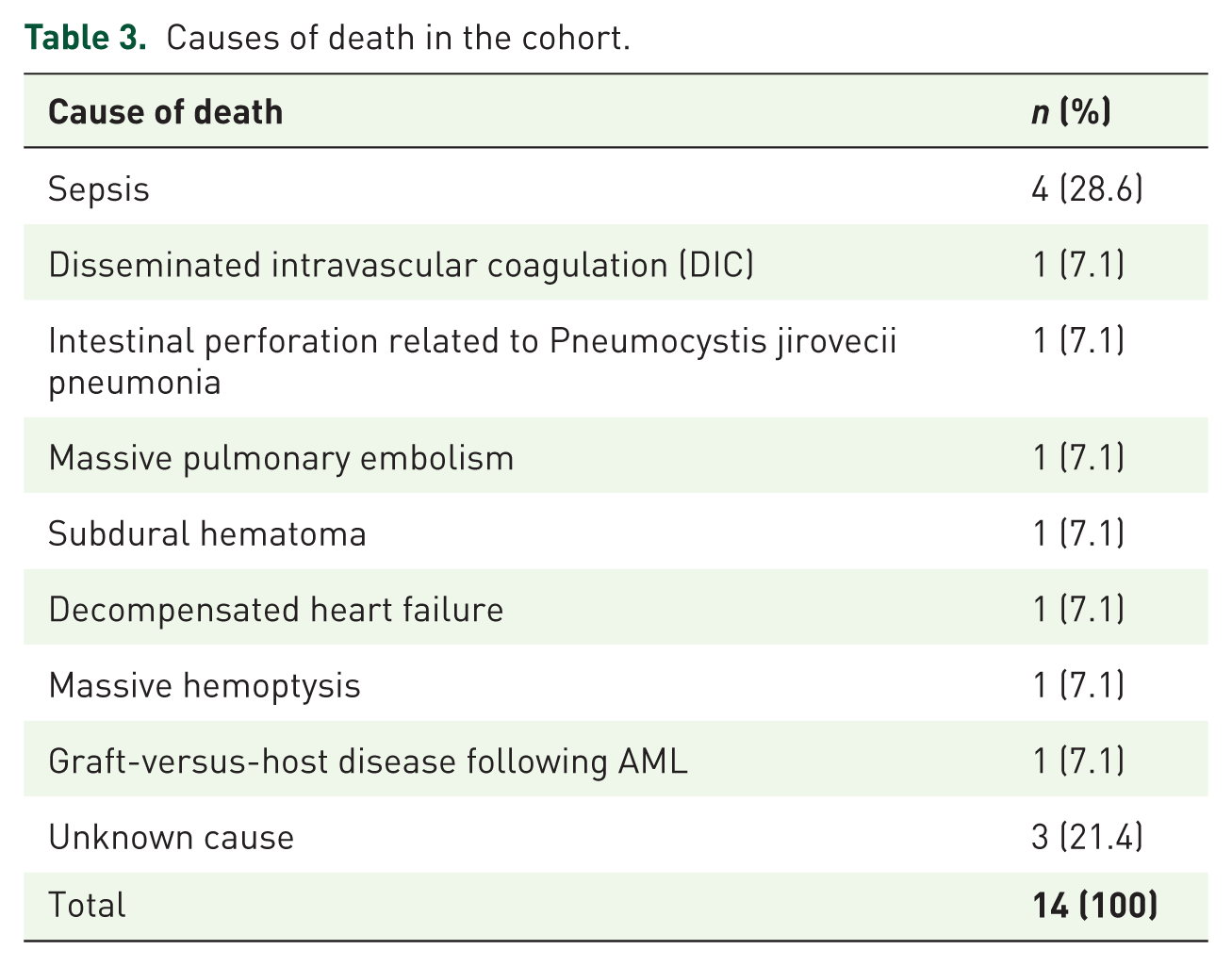
During follow-up, 14 patients (5.0%) were reported deceased. Causes of death included sepsis (n = 4), disseminated intravascular coagulation (DIC) (n = 1), intestinal perforation related to Pneumocystis jirovecii pneumonia (n = 1), PAT (n = 1), subdural hematoma (n = 1), decompensated heart failure (n = 1), massive hemoptysis (n = 1), and graft-versus-host disease (GVHD) following acute myeloid leukemia (AML) (n = 1; Table 3). Cause of death was unknown for three patients.
Causes of death in the cohort.
The clinical characteristics of the three patients with PAA, selected for their representative features, were as follows:
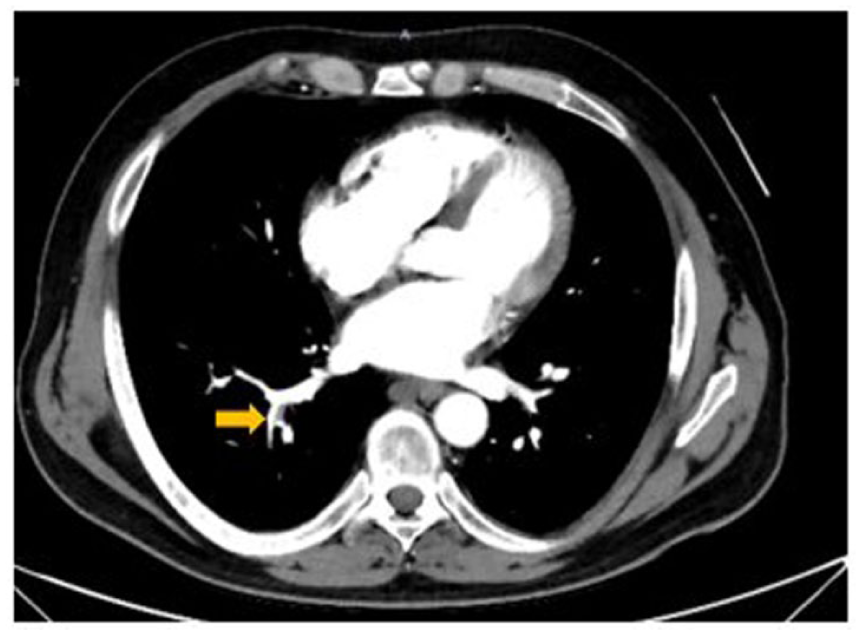
A focal aneurysmal dilation containing partial thrombosis (yellow arrow) is observed in the medial-basal segmental pulmonary artery of the right lower lobe.
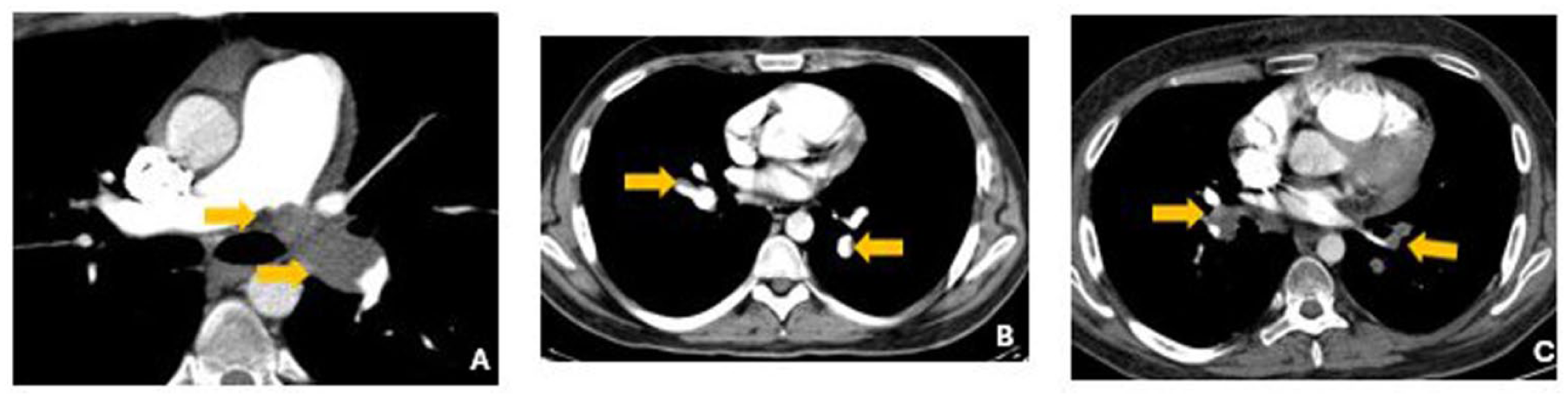
(a) Filling defects consistent with emboli were observed in the left main pulmonary artery (yellow arrows). (b) Bilateral pulmonary artery lower lobar branches show filling defects consistent with emboli. (c) In the segmental pulmonary artery of the left lower lobe, there is a pulmonary artery aneurysm measuring approximately 1 cm in diameter, with thrombotic material nearly completely occupying the aneurysmal lumen (yellow arrows).
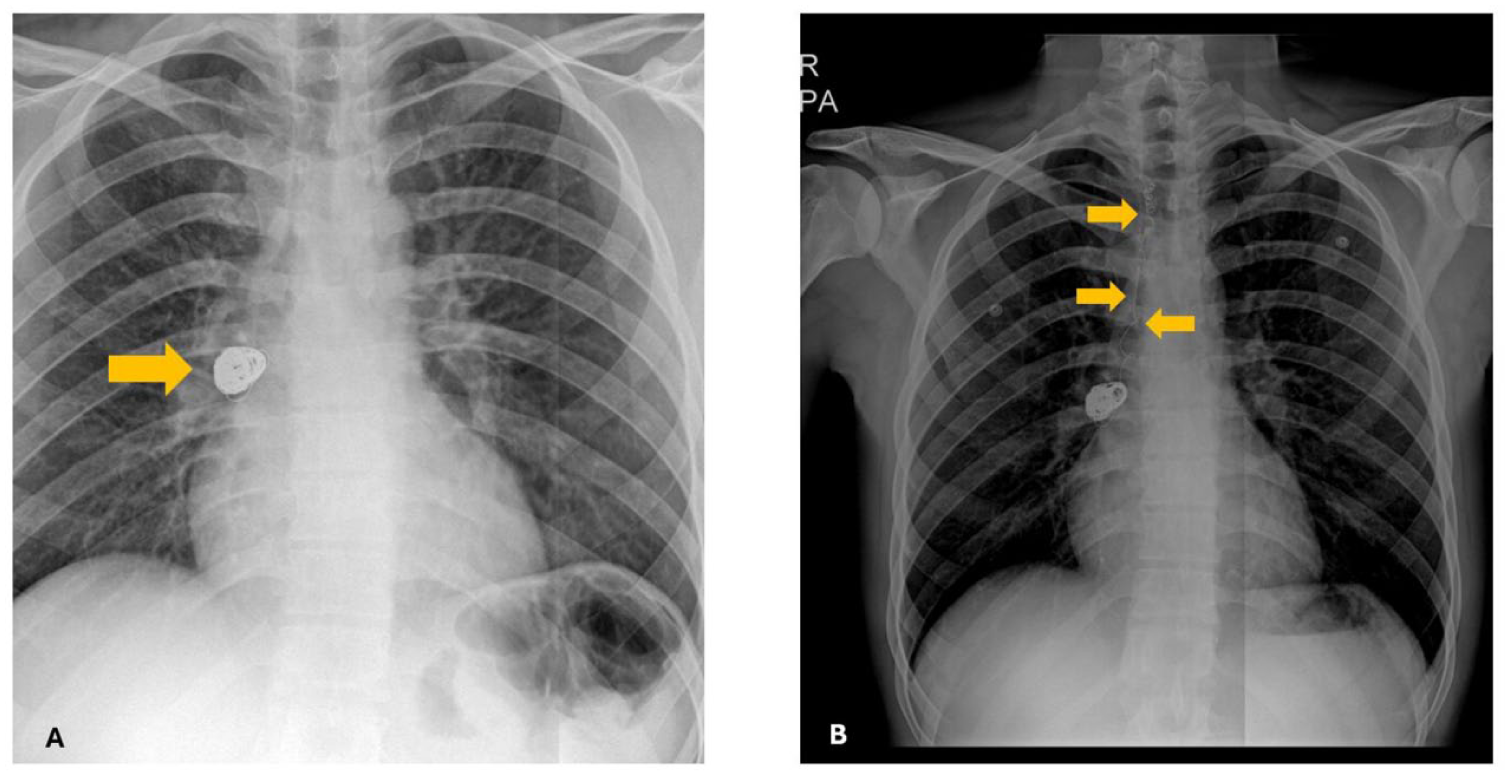
(a) Post-procedural appearance of the coil material deployed within the pulmonary artery aneurysm (yellow arrows). (b) Coil migration observed on CTA performed during the patient’s emergency department presentation with hemoptysis. A few hours after this imaging, the patient expelled the coil orally during a coughing episode (yellow arrows).
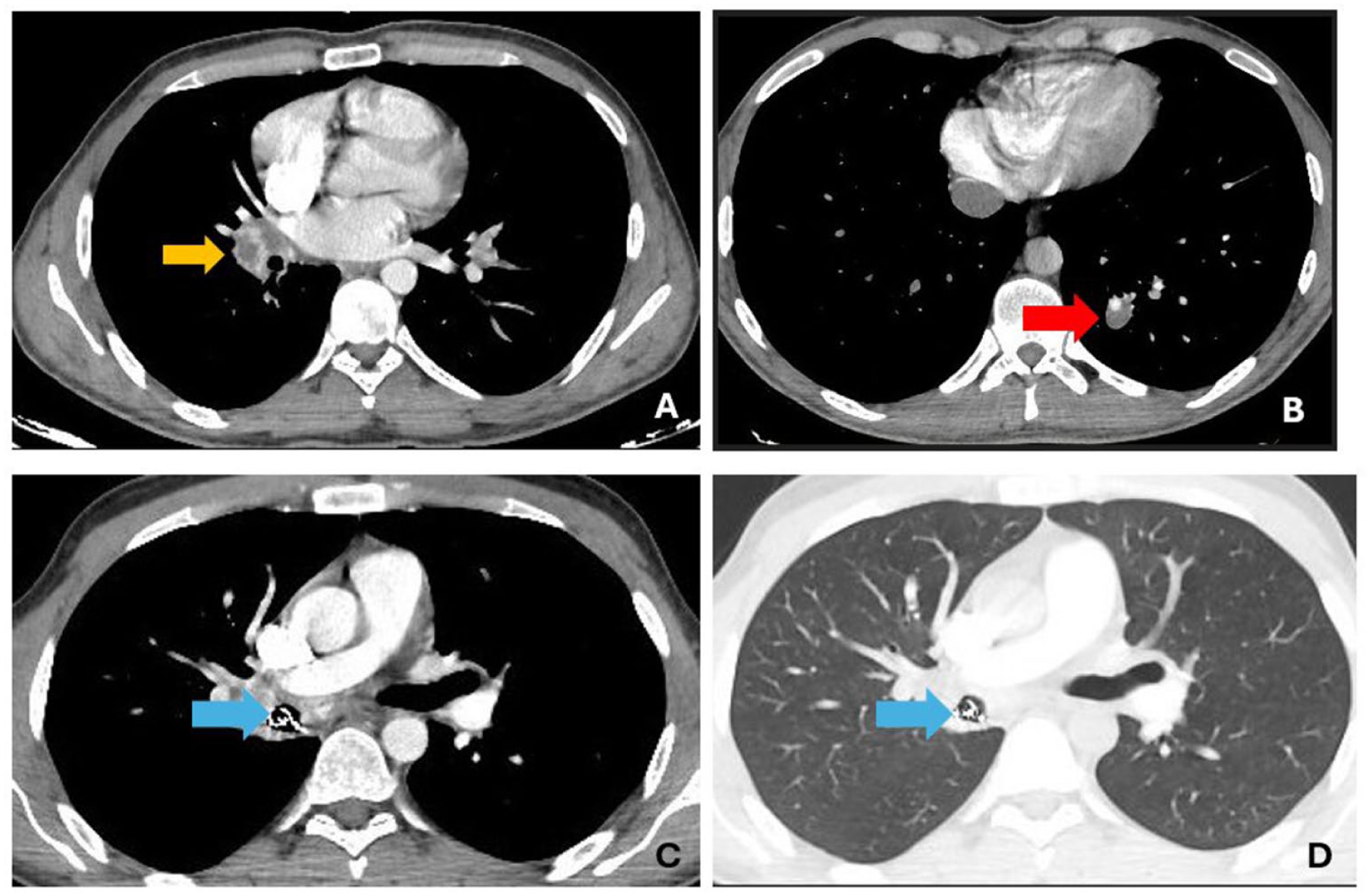
(a) A giant pulmonary artery thrombosis in the lower lobe branch of the right pulmonary artery (yellow arrow). (b) Pulmonary artery aneurysm in the lower lobe branch of the left pulmonary artery (red arrow). (c, d) Appearance consistent with coil migration in the right main bronchus lower lobe branch (blue arrows).
Discussion
The primary aim of this study was to determine the frequency of PAA and PAT in a large Behçet’s disease cohort and to explore the relationship between these two forms of pulmonary vascular involvement. This objective is clinically significant because current literature largely relies on isolated case reports or small series, providing limited insight into how often PAA and PAT truly coexist and whether they represent distinct or overlapping pathogenetic pathways. By systematically evaluating a decade-long cohort, our study addresses this knowledge gap and offers real-world data that clarify the spectrum of pulmonary vascular manifestations in Behçet’s disease. In addition, examining the prevalence of DVT and its association with PAT provides further understanding of whether pulmonary thrombotic lesions arise predominantly in situ or through embolic mechanisms.
Pulmonary vascular involvement in Behçet’s disease has long been recognized as a major determinant of morbidity and mortality. Previous reports have emphasized pulmonary artery aneurysms as the most distinctive and life-threatening pulmonary manifestation, frequently associated with hemoptysis and adverse outcomes. 14 These observations have shaped the current understanding of disease behavior and highlighted the clinical complexity of pulmonary involvement, particularly in the presence of concomitant thrombotic processes. However, the relationship between pulmonary arterial lesions and systemic venous thrombosis remains heterogeneous across reported series, suggesting that pulmonary vascular pathology in Behçet’s disease may not always follow a uniform thrombotic pattern. In line with these observations, subsequent studies further characterized the spectrum of pulmonary vascular involvement in Behçet’s disease. In a comprehensive analysis, pulmonary artery aneurysms and in situ pulmonary thrombosis were shown to represent overlapping but not invariably concomitant manifestations, reflecting the complex vasculitic nature of the disease. 15 Importantly, venous thrombotic involvement was reported with variable frequency, underscoring that pulmonary arterial pathology may evolve independently of overt deep venous thrombosis in certain patients. These findings support a more nuanced interpretation of pulmonary vascular lesions in Behçet’s disease, rather than a uniform thromboembolic model.
In the literature, the prevalence of PAA has been reported between 0.5% and 2.2%,16,17 with higher rates observed in young male patients.18,19 Our evaluation of a large cohort of 279 patients over a ten-year period demonstrated that the frequency of PAA in our center (1.07%) is consistent with the reported rates in the literature. Moreover, the ability to closely follow the clinical course of PAA cases in our study allowed detailed real-world insights into diagnostic and therapeutic processes. In this respect, our study represents one of the few national series documenting the prevalence and clinical characteristics of pulmonary vascular involvement in Behçet’s disease with long-term follow-up data. Moreover, in the present study, patients with vascular involvement demonstrated a marked male predominance compared with those without vascular involvement. Although the mean age was similar between the two groups, mortality was observed to be proportionally higher in the vascular involvement group. These findings suggest that vascular involvement in Behçet’s disease may be associated with a more severe clinical phenotype, particularly in male patients. However, given the retrospective design and limited ability to adjust for confounding factors, these observations should be interpreted as hypothesis-generating rather than causal. Further prospective studies are warranted to better define the prognostic implications of vascular involvement and its potential interaction with sex-related differences in disease expression.
In our series, in addition to PAA and pulmonary thrombosis, both arterial and venous involvement were observed at the levels of the aorta, carotid arteries, and extremities. This finding highlights the broad spectrum of vascular involvement in Behçet’s disease and its significant impact on the clinical course of the disease. Previous studies have reported that thrombosis develops in 14%–39% of Behçet’s patients, with approximately two-thirds of vascular involvement affecting the venous system. 16 In our cohort, vascular involvement was observed in 41 of 279 patients (%14.3), a rate compatible with the literature. These findings suggest that, despite temporal and geographic variations, the frequency of vascular involvement in Behçet’s disease remains relatively stable.
In the literature, variations in the reported rates of vascular involvement across studies can be attributed to changes in diagnostic criteria, differences in the frequency of imaging utilization, and variability in patient profiles among centers. In this context, the evaluation of a large cohort followed at a single center increases the homogeneity of our data and strengthens the clinical relevance of our findings. Turkey, being one of the countries with the highest prevalence of Behçet’s disease, 20 further enhances the sample size and observational power of our series, supporting the generalizability of the results.
From a pathogenetic perspective, weakness of the vessel wall due to obliterative endarteritis of the vasa vasorum provides a substrate for the development of aneurysms or pseudoaneurysms. However, in Behçet’s disease, where thrombotic and inflammatory processes coexist, this mechanism alone may not fully explain PAA formation. Therefore, it has been suggested that, in addition to immunological activity, the systemic pattern of vasculitis also plays a critical role in the development of PAAs. 16 PAAs most commonly involve the large and proximal branches of the pulmonary artery and are typically present clinically with massive hemoptysis.21,22 This situation increases the difficulty in treatment management.
The most significant debate regarding anticoagulant therapy in Behçet’s disease is related to the presence of PAAs. Anticoagulation should be administered under close clinical monitoring in patients with PAAs due to the risk of severe hemoptysis, with careful screening for potential new aneurysm formation. Furthermore, thrombosis in Behçet’s disease is not limited to the pulmonary vasculature and often manifests as DVT. DVT is the most common form of vascular involvement in Behçet’s disease, reported in up to approximately 50% of cases. 23 In our cohort, lower extremity venous Doppler ultrasonography was performed in 90 symptomatic patients, and DVT was detected in 29. This finding supports the notion that DVT represents the most frequent form of vascular involvement in Behçet’s disease and aligns with the distribution reported in the literature.
Although classic PE typically develops secondary to DVT, embolization in Behçet’s disease is relatively rare due to the thrombus being firmly adherent to the vessel wall.24–26 In our study, among the 29 patients with DVT, only one patient was found to have PAT. This finding supports the notion that PE in Behçet’s disease often does not result from the extension of systemic venous thrombosis but likely arises in situ due to arteritis or vasculitic processes within the pulmonary artery wall. However, our cohort lacks histopathological evidence to confirm this distinction. In the literature, the differentiation between arteritis and embolism has been clearly made in only a few studies, primarily using autopsy material. 22 Low autopsy rates in our country limit detailed histopathological investigation of pulmonary vascular involvement in Behçet’s disease, and histopathological confirmation was not possible in the current cohort.
Pulmonary involvement in Behçet’s disease has been reported in 1%–10% of cases. Among these lesions, PAAs are the most frequently described, although PAT is increasingly recognized as a relevant complication. 27 In our study, the prevalence of PAT was 2.1%, slightly higher than the PAA rate at our center. This observation suggests that thrombotic processes may play a more prominent role in the spectrum of pulmonary vascular involvement in Behçet’s disease than previously estimated. Among six patients diagnosed with PAT, four underwent lower extremity venous Doppler ultrasonography, and only one had DVT. However, the small number of PAT cases limits generalizability. Our findings underscore that pulmonary vascular involvement in Behçet’s disease should be evaluated not only for aneurysmal lesions but also for thrombotic processes.
The underlying mechanisms of thrombus formation in Behçet’s disease remain a topic of debate. Emmi et al. 26 proposed that the concurrent development of DVT and PAT may result from a widespread inflammatory process affecting both arterial and venous vessels. This perspective supports the view that vascular involvement in Behçet’s disease is not merely a thrombotic event but reflects a systemic vasculitic process. Nevertheless, the observation of recurrent DVT and PAT episodes despite immunosuppressive therapy, even in the absence of PAA formation, raises the possibility of hypercoagulability and embolization secondary to venous thrombosis. Additionally, an autopsy-based case report 28 demonstrated histopathologically both pulmonary artery thrombosis and embolism in Behçet’s disease, indicating that pulmonary thromboembolism may develop via distinct pathophysiological mechanisms. This finding suggests that the risk of embolization from DVT may be higher than previously assumed and supports the potential necessity of prophylactic anticoagulant therapy in selected cases.
An interesting finding of our cohort was that concomitant DVT was uncommon in patients with PAA or PAT/PE, being observed in only one patient in each subgroup. Notably, both of these patients also exhibited markedly elevated sPAP values. Although the small number of cases precludes definitive conclusions, this observation may suggest that combined pulmonary and systemic venous vascular involvement could reflect a more severe vasculitic phenotype associated with increased pulmonary vascular burden and secondary pulmonary hypertension. Therefore, concomitant DVT in patients with PAA or PAT may potentially serve as a marker of more advanced vascular disease severity. Further larger-scale studies are needed to clarify this relationship.
Elevated pulmonary artery pressure in Behçet’s disease is considered a multifactorial phenomenon and may develop secondary not only to overt pulmonary vascular involvement, but also to chronic inflammation, endothelial dysfunction, recurrent microvascular injury, and subclinical pulmonary vasculopathy. 22 Interestingly, elevated sPAP was observed not only in patients with overt pulmonary vascular involvement such as PAT/PAA, but also in several patients without a clearly identifiable alternative cardiopulmonary explanation. Left ventricular systolic dysfunction was absent in these patients, and advanced chronic pulmonary disease was uncommon. These findings are consistent with recent data suggesting that pulmonary hypertension in Behçet’s disease may develop even in the absence of overt thromboembolic disease or significant parenchymal lung involvement, potentially reflecting underlying pulmonary vascular inflammation or subclinical vasculopathy. In a recent multidisciplinary echocardiographic study, pulmonary hypertension was detected across different clinical phenotypes of Behçet’s disease, including patients without major secondary cardiopulmonary causes, emphasizing the complex and multifactorial nature of pulmonary vascular involvement in this disease. 29 Although our cohort lacked systematic right heart catheterization data, the coexistence of elevated sPAP and vascular involvement in several patients may support the hypothesis that Behçet-related pulmonary vascular inflammation contributes to increased pulmonary vascular resistance and pulmonary artery pressure.
In a retrospective study of 40 Behçet patients, Erol et al. 30 showed that the addition of anticoagulant therapy to immunosuppressive treatment significantly reduced thrombotic events. However, other studies in the literature have reported that adding anticoagulation to immunosuppressive therapy does not provide additional benefit in preventing recurrences.31–33 Anticoagulant therapy was frequently used in patients with vascular involvement, most commonly with warfarin, LMWH, or rivaroxaban, and in several cases, sequential switching between agents was required due to clinical conditions such as malignancy, surgical indications, or changes in vascular status. Overall, anticoagulant-related complications were uncommon in our cohort and were limited to isolated cases, including hemoptysis, menorrhagia, and treatment discontinuation due to bleeding risk in patients with pulmonary artery aneurysm. No major or life-threatening hemorrhagic complication was observed apart from these events. These findings suggest that, when carefully selected and closely monitored, anticoagulant therapy may be used with an acceptable safety profile in Behçet’s disease patients with vascular involvement, although the presence of pulmonary artery aneurysm remains a critical factor that necessitates individualized risk assessment. However, given the retrospective design and limited sample size, these observations should be interpreted cautiously.
In our study, among 155 symptomatic patients evaluated for pulmonary artery aneurysms, three male patients aged 55, 29, and 22 years (%1.07) were found to have PAAs. This prevalence aligns with the range reported in the literature. However, the rarity of these cases limits statistical comparisons and the ability to generalize treatment strategies. Notably, all three cases were male, highlighting potential gender-related differences in disease prognosis.
In our cohort, a 29-year-old male patient presented with recurrent hemoptysis due to an isolated PAA, raising differential diagnoses of Behçet’s disease versus Hughes-Stovin syndrome. Although immunosuppressive therapy was recommended, the patient refused treatment. During follow-up, late coil migration and oral expulsion of the coil were observed after coil embolization. This case underscores the challenges of disease control in patients with poor treatment adherence and the potential for rare mechanical complications. In the literature, Hansen reported a similar case of coil migration in a 29-year-old male patient with Behçet’s disease during follow-up, 34 while Law described migration shortly after coil placement in a 17-year-old patient. 35 These cases demonstrate that although coil embolization is an effective and life-saving treatment for PAA in Behçet’s disease, rare but serious complications may occur due to inflammatory-mediated vessel wall fragility. Continued documentation of such complications will enhance our understanding of the efficacy, safety, and management strategies for this therapeutic approach.
Pulmonary arterial abnormalities developing in the context of Behçet’s disease are rare but carry a significant risk of mortality, as highlighted by numerous case reports. For example, a 32-year-old male patient was found to have bilateral PAAs, which decreased in size after 24 months of treatment with colchicine and cyclophosphamide. 36 Alagha et al. 37 reported a 31-year-old female patient with multiple hospitalizations due to cerebral venous thrombosis, bilateral pulmonary thrombi, right ventricular thrombus, and right pulmonary artery aneurysm, who achieved clinical improvement with immunosuppressive therapy combined with prophylactic low-molecular-weight heparin (32). The importance of early diagnosis and a multidisciplinary approach for treating pulmonary artery aneurysms has been emphasized in multiple studies. Notably, the presence of arterial aneurysms has been reported to increase mortality risk by approximately threefold. 5
The strengths of our study include the evaluation of a large patient population and the use of a comprehensive cohort with a 10-year follow-up period. Additionally, the use of multiple imaging modalities during diagnosis and follow-up, together with systematically archived data, enhances the reliability of the results. Although the retrospective design and single-center nature of the cohort may limit the broader generalizability of the findings, data from the country with the highest prevalence still highlight areas that require further investigation.
The main limitation of our study is the insufficient number of rare vascular complications (PAA, PAT, and DVT), which precluded meaningful statistical inferences for these patients. This particularly restricts the generalizability of findings related to treatment efficacy and prognostic factors. One important limitation of this study is that thoracic imaging was primarily performed in patients presenting with pulmonary symptoms or clinical suspicion of thoracic involvement. Therefore, asymptomatic patients with pulmonary artery thrombosis (PAT) and/or pulmonary artery aneurysm (PAA) may have remained undetected, potentially leading to an underestimation of the true prevalence of pulmonary vascular involvement in this cohort.
Conclusion
Pulmonary vascular involvement in Behçet’s disease, although uncommon, represents one of the most severe and potentially life-threatening manifestations of the disease. In our cohort, pulmonary artery thrombosis and pulmonary artery aneurysm were identified at frequencies consistent with the literature, while deep vein thrombosis remained the most common form of vascular involvement. Our findings further support the concept that pulmonary thrombotic lesions in Behçet’s disease may frequently develop in situ rather than as classic thromboembolic events secondary to peripheral venous thrombosis. The coexistence of pulmonary and systemic vascular involvement, particularly in patients with elevated pulmonary artery pressures, may indicate a more severe vasculitic phenotype. Early recognition of pulmonary vascular complications through a multidisciplinary approach involving pulmonology, rheumatology, radiology, and cardiovascular specialties is critical for reducing morbidity and mortality. Increased awareness and close follow-up are essential for timely diagnosis and individualized management of these complex vascular manifestations
Supplemental Material
sj-doc-1-tar-10.1177_17534666261464447 – Supplemental material for Pulmonary artery involvement in Behçet’s disease patients: real-life data on aneurysm and thrombosis
Supplemental material, sj-doc-1-tar-10.1177_17534666261464447 for Pulmonary artery involvement in Behçet’s disease patients: real-life data on aneurysm and thrombosis by Nilufer Yigit, Hilal Arguner, Firdevs Ulutas, Vefa Cakmak, Veli Cobankara and Goksel Altınısık in Therapeutic Advances in Respiratory Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.