
Abstract
Background:
Hypercapnia is linked to a poor prognosis in acute exacerbation of chronic obstructive pulmonary disease (AECOPD) and severe community-acquired pneumonia (SCAP), and reduced early anti-inflammatory capacity in SCAP. However, its impact on AECOPD+SCAP patients remains unclear.
Objectives:
To assess hypercapnia’s effects on inflammatory responses and short-term outcomes in AECOPD+SCAP patients.
Design:
This retrospective, dual-center study included 185 hospitalized AECOPD+SCAP patients from January 2014 to June 2025.
Methods:
Patients were stratified by PaCO2 levels on the day of admission: hypercapnia (>45 mmHg), normocapnia (35–45 mmHg), and hypocapnia (<35 mmHg). Data were collected on clinical data, biomarkers (procalcitonin [PCT], C-reactive protein [CRP], lactate and red cell distribution width coefficient of variation [RDW-CV]) and 30-day survival.
Results:
The three groups had similar invasive mechanical ventilation needs and in-hospital and 30-day mortality. Hypercapnic patients (especially with acidosis) had a higher intensive care unit (ICU) admission risk than normocapnic patients. The hypercapnia group had lower PCT, CRP and lactate levels versus the hypocapnia group (p < 0.05), while RDW-CV showed no significant intergroup differences(p > 0.05). Such trends persisted in ICU-admitted patients, largely independent of acidosis and were unaffected by prior systemic corticosteroid therapy. Multivariate analysis indicated hypercapnia, PaO2/FiO2, lactate, and RDW-CV could independently predict ICU admission. The nomogram incorporating these predictors showed good discriminatory ability (area under the curve = 0.72), comparable to pneumonia severity scores (CURB-65, PSI, SMART-COP, and Quick SOFA), with clinical utility confirmed by calibration and decision curve analyses.
Conclusion:
Hypercapnia in AECOPD+SCAP patients could indicate higher ICU admission risk (especially in cases of acidosis) and impaired early anti-inflammatory responses, which are largely independent of acidosis. The combination of hypercapnia, RDW-CV, PaO2/FiO2 ratio, and lactate levels can help to identify patients requiring intensive care.
Introduction
Chronic obstructive pulmonary disease (COPD) is a progressive respiratory disorder characterized by persistent, incompletely reversible airflow obstruction and ranks among the leading causes of mortality in many developed and developing countries. Severe community-acquired pneumonia (SCAP) frequently co-occurs during acute exacerbations of COPD (AECOPD). Hypercapnia is commonly seen in diseases such as COPD and severe pneumonia.1 –4 Although hypercapnia may help alleviate lung inflammation and alveolar oxidative stress, it can also have adverse effects such as impaired alveolar tissue repair and reduced alveolar fluid clearance. 5 A growing body of evidence reveals that its harmful effects carry greater weight than the protective benefits. 4 It has been reported that hypercapnia is an independent predictor of mortality in patients with severe AECOPD requiring admission to the intensive care unit(ICU). 6 Additionally, higher PaCO2 levels in AECOPD are associated with a longer hospital stay 7 and an increased need for invasive ventilation in patients admitted to the ICU. 8 A recent study has further shown that hypercapnia upon admission is significantly associated with adverse outcomes in patients with severe pneumonia, including an increased requirement for invasive mechanical ventilation (IMV), elevated mortality, and diminished early inflammatory reactions indicated by reduced circulating concentrations of inflammatory biomarkers such as C-reactive protein (CRP), procalcitonin (PCT) and interleukin-6 (IL-6). 2 The red cell distribution width (RDW), a measure of erythrocyte volume heterogeneity, is a key tool for distinguishing types of microcytic anemia. A growing body of evidence suggests that an elevated RDW indicates a poor prognosis in various diseases, including pneumonia,9,10 AECOPD,11,12 COPD13,14 and septic shock.15,16 The mechanisms underlying elevated RDW levels remain unclear. Some speculate that it may be related to interference from the inflammatory process during erythropoiesis. 17 Bacterial infections are known to elevate lactate (Lac) production. In clinical settings, lactate levels serve as a critical biomarker for prognosticating patients with severe infections. Hyperlactatemia (>2 mmol/L) constitutes a key diagnostic criterion for septic shock. Lactate is a powerful predictor of in-hospital mortality in SCAP. 18 It is also associated with adverse clinical outcomes in AECOPD, often indicating the presence of serious complications. 19
However, to our knowledge, few studies have yet explored the impact of hypercapnia on the short-term prognosis and early inflammatory response patterns of patients with AECOPD and SCAP. Therefore, this study aims to: (1) compare the clinical characteristics and biomarker levels (PCT, CRP, Lac, red cell distribution width coefficient of variation [RDW-CV]) between the group with hypercapnia and the groups with normal or low PaCO2 levels in patients with AECOPD and SCAP; (2) evaluate the association between hypercapnia and short-term clinical outcomes in this population, including the need for IMV, intensive care unit (ICU) admission, and in-hospital and 30-day mortality.
Methods
Study design and population
This retrospective multicenter investigation utilized data from two tertiary hospitals in China. It was led by Shuangliu District First People’s Hospital, Chengdu, in collaboration with The Second Affiliated Hospital, Chongqing Medical University. A total of 185 patients with AECOPD and SCAP were enrolled from January 2014 to June 2025. This study complied with the Declaration of Helsinki and received approval from the hospitals’ ethics committees. Waiver of informed consent was granted for this retrospective analysis. The reporting of this study conformed to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement for cohort studies. 20 Eligible patients were ⩾40 years old, hospitalized for AECOPD with concurrent SCAP, and had pre-existing confirmed post-bronchodilator FEV1/FVC < 0.70. A SCAP diagnosis requires radiographic confirmation using a chest computed tomography (CT) scan or X-ray by two independent reviewers (excluding attending physicians and data analysts), with symptom onset occurring in the community. Additionally, the diagnosis of SCAP must meet the Infectious Diseases Society of America (IDSA)/American Thoracic Society (ATS) 2007 guideline criteria, which entails fulfilling one major criterion (septic shock requiring vasopressors; respiratory failure requiring IMV) or at least three minor criteria (respiratory rate ⩾30 breaths/min; PaO2/FiO2 ⩽250; multilobar infiltrates; confusion or disorientation; blood urea nitrogen level ⩾20 mg/dL; white blood cell count <4000 cells/μL; platelet count <100,000/μL; core temperature < 36°C; hypotension requiring aggressive fluid resuscitation). 21 According to the Global Initiative for Chronic Obstructive Lung Disease report, AECOPD is defined as worsening dyspnea and/or increased cough and sputum occurring in <14 days. 22 This study strictly adhered to this definition, including eligible cases with clear documentation in medical records that the above-mentioned respiratory symptoms worsened <14 days before admission.
The exclusion criteria were as follows: bronchiectasis; severe immunosuppression due to causes other than severe pneumonia (e.g. cytotoxic therapy, HIV, active malignancy, bone marrow or organ transplantation, or receipt of either ⩾20 mg/day of prednisolone or equivalent for ⩾2 weeks, or a cumulative dose > 600 mg); autoimmune diseases; recent (within 1 month) acute cardiovascular or cerebrovascular events; the main respiratory symptoms recorded in the medical record include increased shortness of breath and/or cough and sputum that occurred ⩾14 days prior to admission; cases with incomplete required data and a hospitalization within the 4 weeks prior to admission. For patients with multiple admissions, only data from the first eligible hospitalization were analyzed.
All patients received standardized care and treatment, with the treatment plan determined by the attending physician based on the widely recognized global guidelines for AECOPD and SCAP, which were updated over time to reflect evolving evidence and guideline recommendations. According to the medical management regulations of the two tertiary hospitals involved in this study, all non-invasive mechanical ventilation(NIMV) must be initiated in general wards, while all IMV must only be initiated in the ICU.
The study group was subsequently classified according to PaCO2 levels at admission: hypocapnic (PaCO2 <35 mmHg), normocapnic (35–45 mmHg) and hypercapnic (>45 mmHg) groups. All patients underwent routine automated tests for CRP, PCT, Lac and RDW-CV in blood on the day of admission. Data were collected from enrolled cases using standardized forms, including information on demographic variables, clinical status during hospitalization, laboratory results, and assessed Pneumonia Severity Index (PSI), CURB-65, Charlson Comorbidity Index (CCI), SMART-COP, and Quick SOFA (qSOFA) scores on admission, along with outcomes including the need for IMV, ICU admission, in-hospital mortality, and 30-day mortality obtained via telephone follow-up.
Data analysis
We used IBM SPSS Statistics 26.0 and R 4.5.1 (R Core Team, 2025) for statistical analysis. Post hoc power analysis was conducted with PASS 2023 (version 23.0.2). Normality was evaluated using the ratios of skewness and kurtosis to their standard errors. Data were deemed normally distributed if these ratios were within ±1.96. Data for normally distributed continuous variables are presented as mean ± SD, with an independent samples t-test used to assess intergroup differences between two groups. A comparison of the variables among multiple groups was performed. Where ANOVA revealed statistically significant differences, post hoc tests incorporating Bonferroni correction were conducted. Skewed data were summarized as the median and interquartile range, and group comparisons were made using the Kruskal–Wallis H test. Categorical data, presented as frequencies and percentages, were analyzed using the chi-squared or Fisher’s exact test. Spearman’s correlation was utilized for correlation analysis. MedCalc 15.6 software was utilized to evaluate diagnostic test accuracy and comparisons. Predictors with p < 0.10 in univariate analysis were included in a binary logistic regression model to forecast ICU admission risk in AECOPD-SCAP patients, with the model’s goodness of fit assessed by the Hosmer–Lemeshow test. A nomogram derived from this model underwent validation in R 4.5.1. A significance level of p < 0.05 was applied to most analyses. However, comparisons involving three or more categorical variables (analyzed by chi-square or Fisher’s exact test) adopted Bonferroni correction, using an adjusted significance threshold of α = 0.05/number of pairwise comparisons.
Results
Clinical characteristics and outcomes of 185 patients with AECOPD+SCAP
This retrospective analysis enrolled 185 eligible patients with AECOPD and SCAP, who were stratified into hypercapnia (n = 88), normocapnia (n = 56), and hypocapnia (n = 41) groups based on their admission-day arterial blood Paco2 levels (Supplemental Figure 1). The in-hospital mortality rate was 16.76% (31/185). Forty-nine patients (26.49%) died within 30 days after admission. Within the cohort, 69.7% (129/185) were aged 60 years or older and 43.2% (80/185) had at least one comorbidity included in the PSI score. The hypercapnia group exhibited lower baseline CCI than the hypocapnia group(p < 0.01). In comparison with normocapnic patients, hypercapnic patients were more likely to have elevated pneumonia severity scores (PSI, qSOFA, and CURB-65), higher ICU admission rates, prolonged ICU stays, decreased oxygenation indices, impaired consciousness, and greater pre-admission systemic corticosteroid (SCS) use(all p < 0.05). Furthermore, hypercapnic patients exhibited lower pH levels, higher HCO3¯ and PaCO2 levels, higher SMART-COP scores, and higher rates of non-invasive ventilation use than the other two groups(all p < 0.05). The three patient groups demonstrated similar rates of multi‑lobar involvement on chest X‑ray/CT, need for invasive mechanical ventilation, hospital length of stay, in‑hospital mortality, and 30‑day mortality. Other baseline characteristics and complications (e.g., sepsis/septic shock) were also comparable across groups (Table 1).
A comparative analysis of demographic characteristics, biomarker concentrations, and clinical outcomes in patients with AECOPD and SCAP, stratified by hypercapnia versus normocapnia or hypocapnia groups.
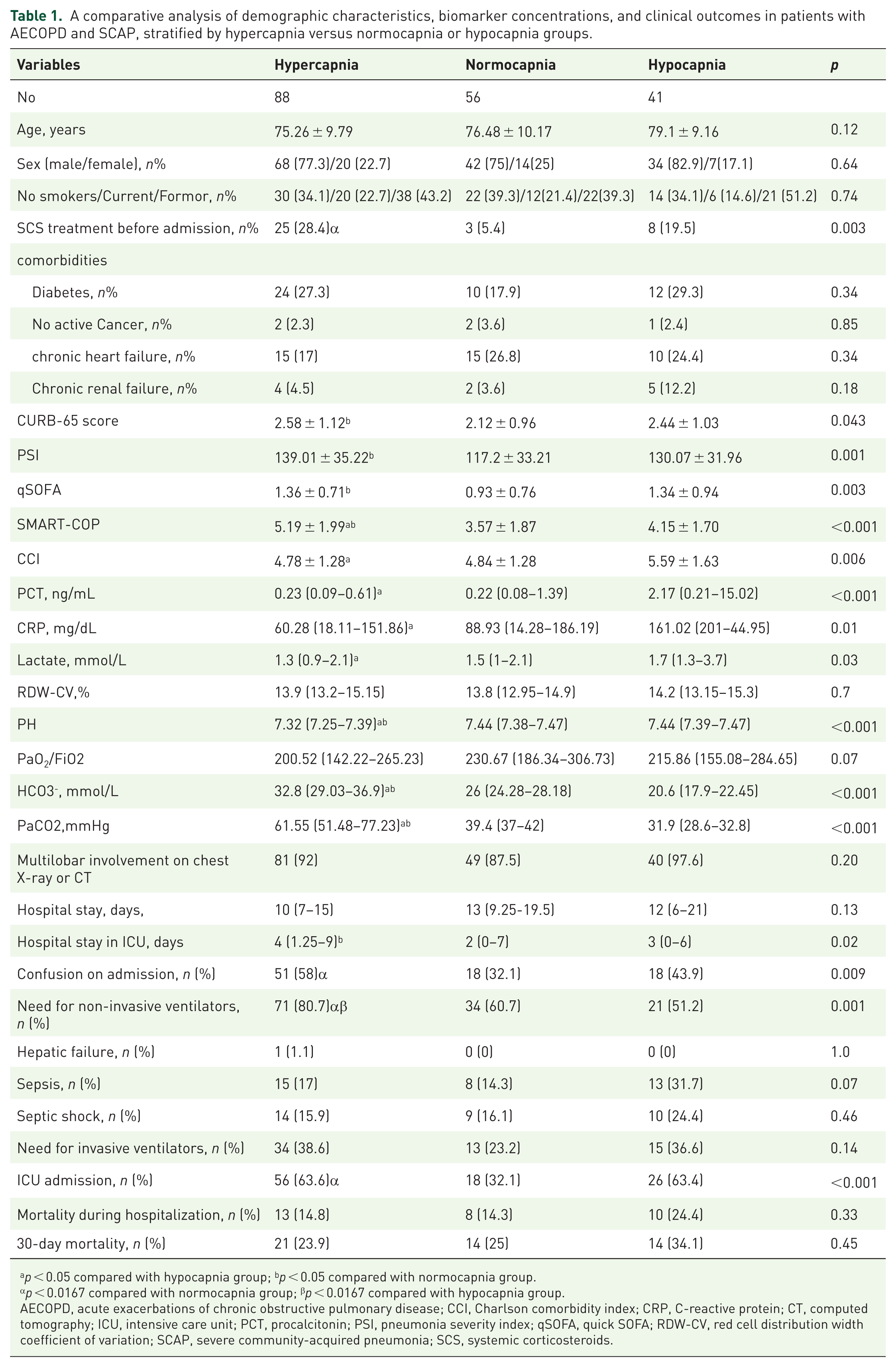
p < 0.05 compared with hypocapnia group; bp < 0.05 compared with normocapnia group.
p < 0.0167 compared with normocapnia group; βp < 0.0167 compared with hypocapnia group.
AECOPD, acute exacerbations of chronic obstructive pulmonary disease; CCI, Charlson comorbidity index; CRP, C-reactive protein; CT, computed tomography; ICU, intensive care unit; PCT, procalcitonin; PSI, pneumonia severity index; qSOFA, quick SOFA; RDW-CV, red cell distribution width coefficient of variation; SCAP, severe community-acquired pneumonia; SCS, systemic corticosteroids.
Differences in inflammatory response patterns and the impact of hypercapnia with acidosis on short-term outcomes
This study found that in patients with AECOPD+SCAP, the levels of CRP, PCT, and lactate on the day of admission were significantly lower in the hypercapnia group than in the hypocapnia group (p < 0.05), but showed no significant difference compared with the normocapnia group. RDW-CV levels were similar among the three groups (Table 1). Subsequent three subgroup analyses were performed. After excluding AECOPD+SCAP patients not admitted to the ICU, the first subgroup analysis still showed significantly lower CRP, lactate, and PCT levels in the hypercapnia group than in the hypocapnia group (p < 0.05), with no significant difference compared to the normocapnia group. RDW-CV did not differ across groups (Table 2). The second subgroup analysis indicated that there were no significant differences in PCT, CRP, RDW-CV, or lactate levels, regardless of prior systemic corticosteroid treatment (p > 0.05; Table 3). In the third subgroup analysis, the hypercapnia group was subdivided into those with and without acidosis, using normocapnic and hypocapnic groups as controls. The results showed that CRP, PCT, and lactate levels in the two hypercapnia subgroups were lower than those in the hypocapnia group. Specifically, CRP and lactate levels were lower still in the hypercapnia without acidosis subgroup (p < 0.05), while PCT was significantly lower in both hypercapnia subgroups(with or without acidosis) (p < 0.001). Moreover, the risk of ICU admission was significantly higher only in hypercapnic patients with acidosis compared to the normocapnic group, but not in those without acidosis. However, no significant differences were observed among the four groups with regard to the need for invasive mechanical ventilation, in-hospital/30-day mortality and RDW-CV levels (Table 4).
CRP, PCT, RDW-CV, and lactate levels in patients with AECOPD and SCAP admitted to the ICU.
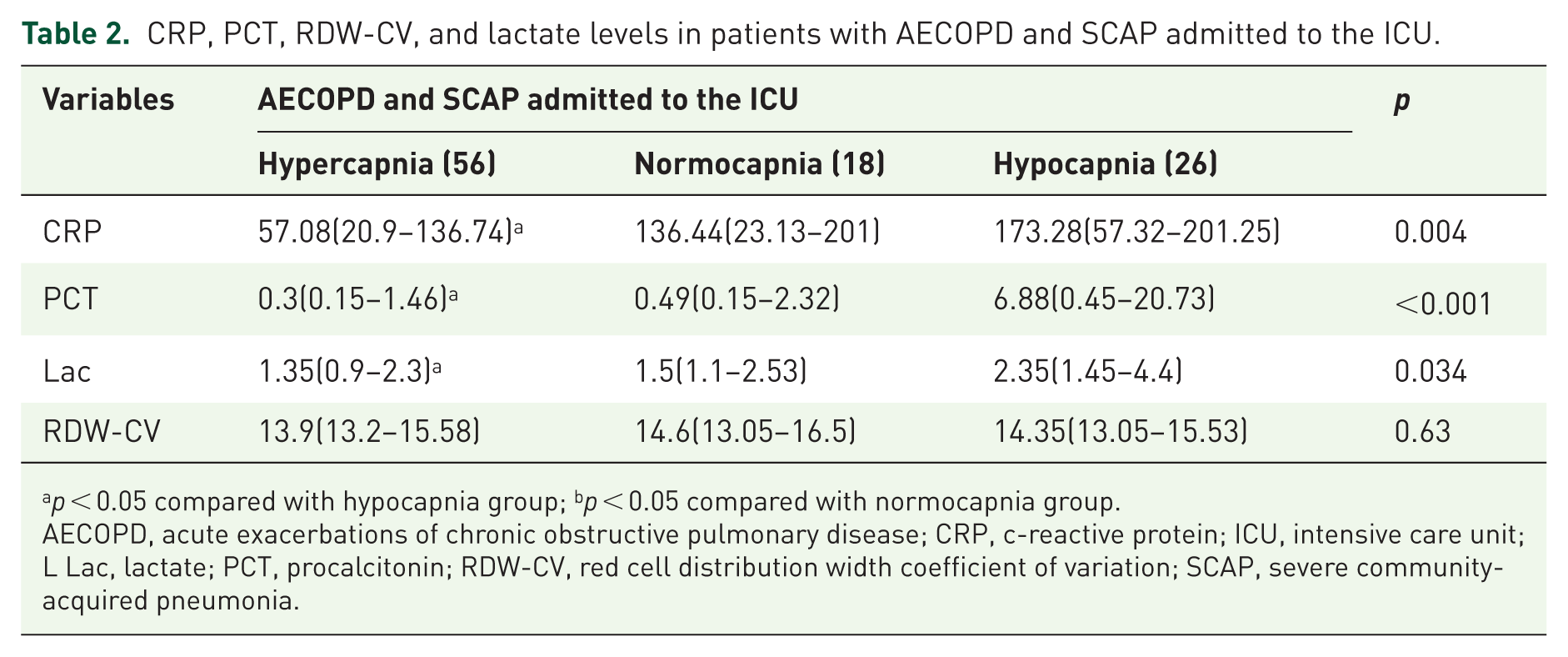
p < 0.05 compared with hypocapnia group; bp < 0.05 compared with normocapnia group.
AECOPD, acute exacerbations of chronic obstructive pulmonary disease; CRP, c-reactive protein; ICU, intensive care unit; L Lac, lactate; PCT, procalcitonin; RDW-CV, red cell distribution width coefficient of variation; SCAP, severe community-acquired pneumonia.
The levels of CRP, PCT, RDW-CV, and Lac in patients with AECOPD and SCAP according to SCS treatment before admission.
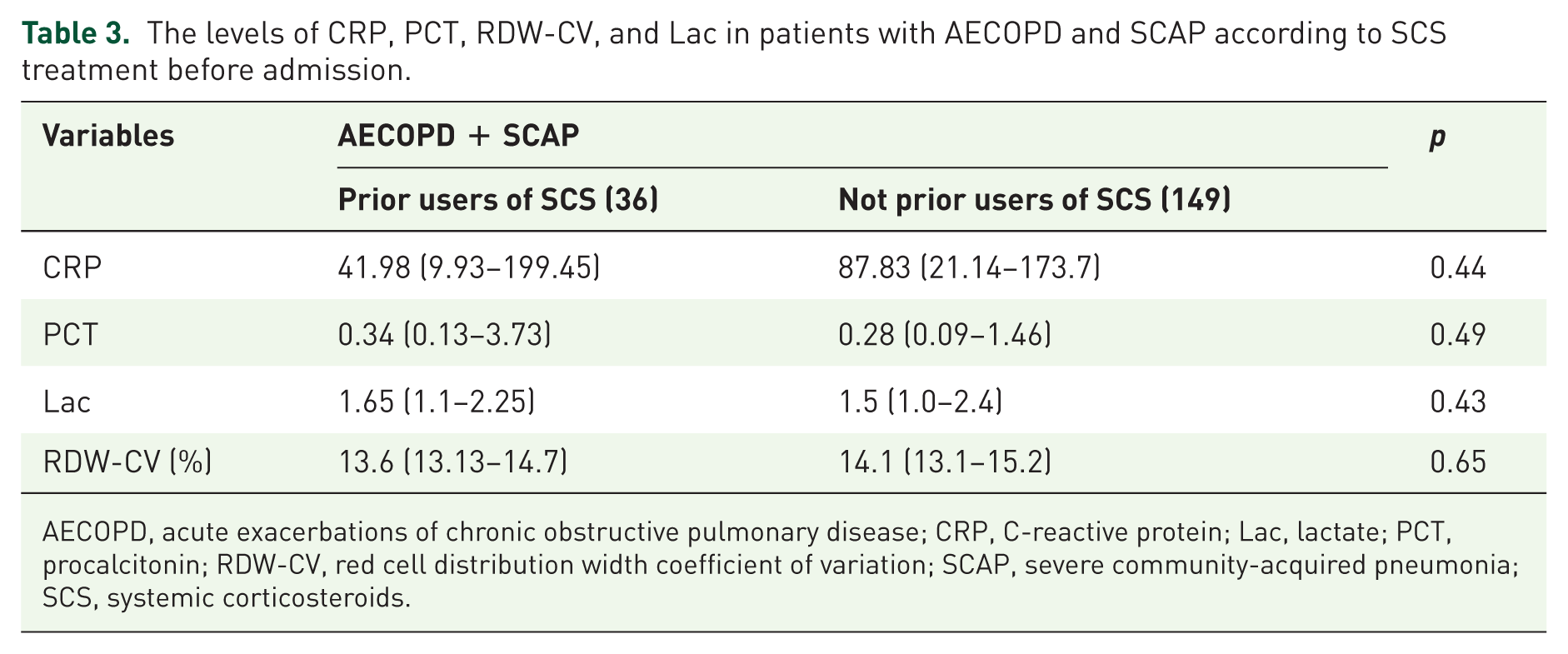
AECOPD, acute exacerbations of chronic obstructive pulmonary disease; CRP, C-reactive protein; Lac, lactate; PCT, procalcitonin; RDW-CV, red cell distribution width coefficient of variation; SCAP, severe community-acquired pneumonia; SCS, systemic corticosteroids.
The impact of acidosis on biochemical markers and short-term prognosis in patients with AECOPD complicated by SCAP and hypercapnia.

Hypercapnia without acidosis versus normocapnia group, p < 0.05.
Hypercapnia without acidosis versus hypocapnia group, p < 0.05.
Hypercapnia with acidosis versus normocapnia group, p < 0.05.
Hypercapnia with acidosis versus hypocapnia group, p < 0.05.
Hypercapnia without acidosis versus normocapnia group, p < 0.0083.
Hypercapnia without acidosis versus hypocapnia group, p < 0.0083.
Hypercapnia with acidosis versus normocapnia group, p < 0.0083.
Hypercapnia with acidosis versus hypocapnia group, p < 0.0083.
AECOPD, acute exacerbations of chronic obstructive pulmonary disease; CRP, C-reactive protein; ICU, intensive care unit; IMV, invasive mechanical ventilation; PCT, procalcitonin; Lac, lactate; RDW-CV, red cell distribution width coefficient of variation; SCAP, severe community-acquired pneumonia.
Associations of PaCO2 with length of ICU stay, length of stay (LOS), and systemic biomarkers
Spearman’s correlation analysis showed PaCO2 was positively correlated with ICU LOS (r = 0.19, p = 0.008) but not with total LOS or RDW-CV, while it was negatively correlated with PCT, CRP, and lactate (r = −0.26, p < 0.001; r = −0.2, p = 0.005; r = −0.18, p = 0.01; Figure 1).
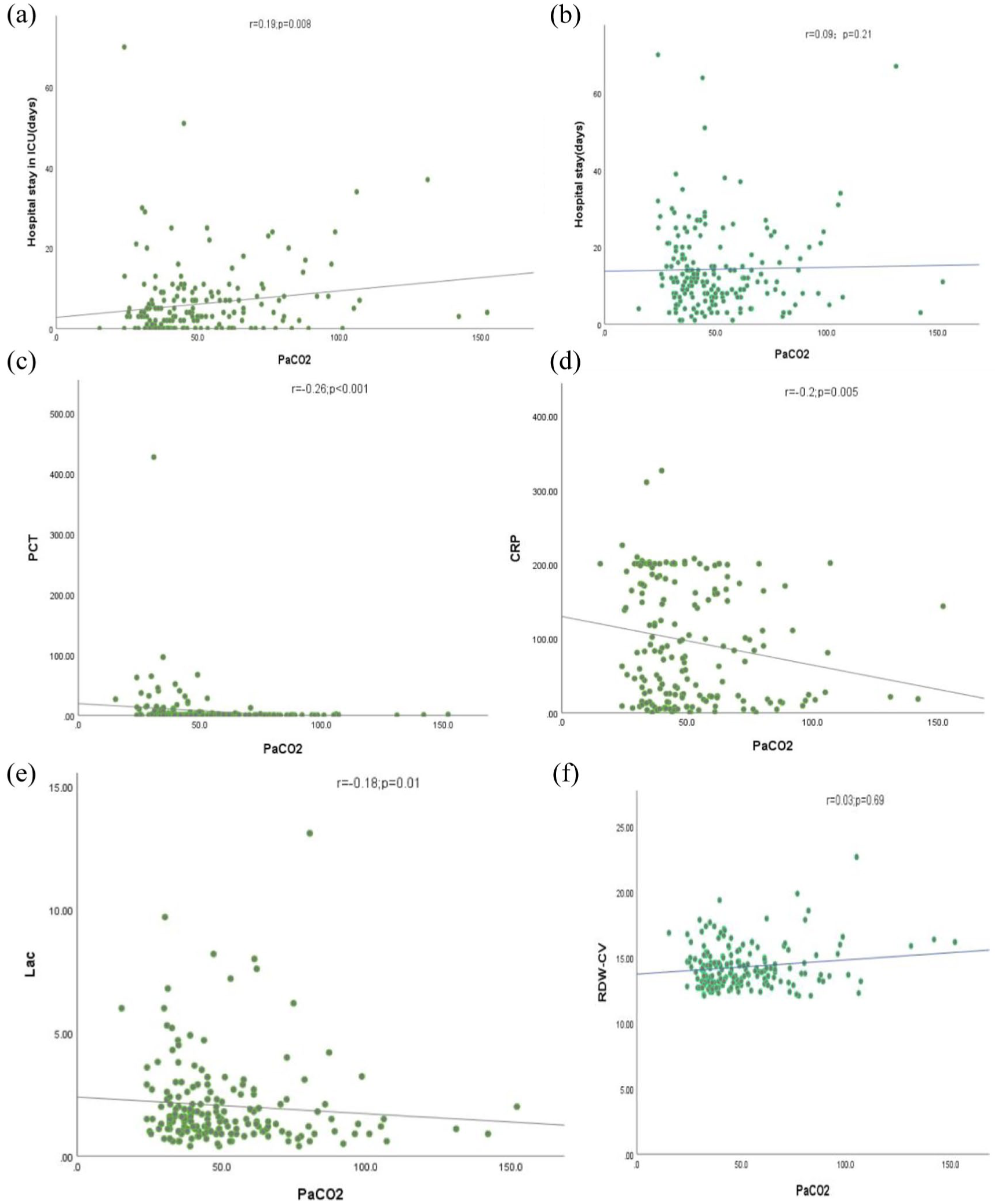
Correlations between hospital stay, hospital stay in the ICU, RDW-CV, lactate, PCT and CRP with PaCO2 in patients with AECOPD and SCAP. (a) Hospital stay in ICU; (b) hospital stay; (c) PCT; (d) CRP; (e) lactate; (f) RDW-CV.
Factors predicting ICU admission in patients with AECOPD and SCAP
Of the 185 patients with AECOPD+SCAP, 100 (54.05%) required ICU admission due to critical illness. Univariate analysis identified hypercapnia, elevated lactate and RDW-CV levels, as well as decreased PaO2/FiO2 ratio and pH levels as significant risk factors for ICU admission (p < 0.05). After including the above-mentioned five variables into a binary logistic regression model, hypercapnia (OR = 2.24, 95% CI: 1.18–4.20, p = 0.01),elevated lactate (OR = 1.31, 95% CI: 1.03–1.66, p = 0.03) and RDW-CV levels (OR = 1.25, 95% CI: 1.02–1.55, p = 0.03), and a decreased PaO2/FiO2 ratio (OR = 0.996, 95% CI: 0.992–0.999, p = 0.02) remained independent predictors of ICU admission (Table 5). A nomogram incorporating these predictors had a C-index of 0.72 (95% CI: 0.64–0.79) (Supplemental Figure 2, Table 6). Although its area under the curve (AUC) was the highest among the models compared, Delong’s test showed that its discriminative ability was not statistically superior to the pneumonia severity scores (PSI, CURB-65, SMART-COP, and qSOFA) (p > 0.05) (Table 6, Supplemental Figure 3). The nomogram showed good calibration (Hosmer–Lemeshow test, p = 0.909; the calibration curve aligned well; Supplemental Figure 4(a)), and decision curve analysis (DCA) confirmed its clinical net benefits from using the nomogram for clinical guidance across a wide range of threshold probabilities (Supplemental Figure 4(b)).
Logistic regression model of factors predicting admission to ICU in AECOPD+SCAP.

AECOPD, acute exacerbations of chronic obstructive pulmonary disease; CCI, Charlson comorbidity index; CRP, C-reactive protein; ICU, intensive care unit; Lac, lactate; PCT, procalcitonin; RDW-CV, red cell distribution width coefficient of variation; SCAP, severe community-acquired pneumonia.
AUC values for different models predicting ICU admission in patients with AECODP and SCAP.

AECOPD, acute exacerbations of chronic obstructive pulmonary disease; AUC, area under the curve; ICU, intensive care unit; Lac, lactate; PSI, pneumonia severity index; qSOFA, quick SOFA; RDW-CV, red cell distribution width coefficient of variation; SCAP, severe community-acquired pneumonia.
Discussion
The main findings of this study are as follows: (1) in patients with AECOPD complicated by SCAP, hypercapnia showed no statistically significant association with in-hospital mortality, or 30-day mortality, or the need for IMV, regardless of the presence or absence of acidosis; (2) the hypercapnia group, particularly those with concomitant acidosis, had a higher risk of ICU admission compared to the normocapnia group; (3) the hypercapnia group exhibited lower levels of PCT, CRP, and Lac compared to the hypocapnia group, but these differences were not significant compared to the normocapnia group. RDW-CV showed no significant differences across groups. This pattern was largely independent of acidosis, persisted in ICU-admitted patients, and was unaffected by prior systemic glucocorticoid therapy; (4) multivariate analysis identified hypercapnia, PaO2/FiO2 ratio, lactate, and RDW-CV as independent predictors of ICU admission. A nomogram constructed by combining these predictors demonstrated good discriminative ability, comparable to pneumonia severity scores (CURB-65, PSI, SMART-COP, and Quick SOFA), and indicated clinical utility as confirmed by DCA and calibration curve analysis.
Our analysis revealed no statistically significant association between hypercapnia and in-hospital mortality, 30-day mortality, or the need for IMV among patients with AECOPD and SCAP, regardless of the presence of concurrent acidosis. Hypercapnia was found to be associated with the need for NIMV in this patient cohort. These findings suggest that, although hypercapnia indicates impaired respiratory function, its impact on the short-term prognosis of patients is likely to be limited due to advancements in medical technology, such as the prompt implementation of non-invasive mechanical ventilation, standardized pharmacological treatment and systematic nursing interventions. Furthermore, an in vitro experiment confirmed that restoring mice exposed to 10% CO2 to normal air before or upon nasal infection with P. aeruginosa could reverse the host defense deficits and increased pneumonia mortality induced by hypercapnia. 1
Hypercapnia in pneumonia patients is associated with an increased risk of ICU admission. 23 However, few studies have investigated its impact on ICU admission for patients with AECOPD and SCAP. Our study demonstrated that hypercapnia was associated with an increased risk of ICU admission and a prolonged ICU stay in patients with AECOPD and SCAP. Subgroup analysis further revealed that this increased risk was primarily observed in hypercapnic patients with acidosis, but not in those without acidosis. Hypercapnia has been reported to be associated with a worsening of pneumonia (as assessed by PSI), irrespective of whether patients with COPD were excluded.2,23 Our study also confirmed that patients with hypercapnia in SCAP and AECOPD had significantly higher PSI, CURB-65, SMART-COP, and qSOFA scores than the normocapnic group, further suggesting that hypercapnia is closely linked to greater disease severity of SCAP in AECOPD patients, which may be one of the potential mechanisms underlying the increased risk of ICU admission in AECOPD+SCAP patients with hypercapnia. Additionally, poor baseline pulmonary function in AECOPD patients, combined with severe pneumonia, may have a synergistic effect, exacerbating the development or progression of hypercapnia, which could be another important reason why patients with AECOPD and SCAP with hypercapnia are more likely to be admitted to the ICU. Chronic hypercapnia in COPD patients is associated with poorer lung function,24 –26 potentially arising from structural alterations of the airways and alveoli, dysfunctional alveolar ventilation, and ventilation-perfusion (V/Q) mismatch. 24 During AECOPD, alterations in cardiac output, oxygen consumption, and minute ventilation can exacerbate the V/Q mismatch,27,28 thereby potentially contributing to arterial hypoxemia and the onset or exacerbation of hypercapnia. 22 In this population, the occurrence of SCAP further compromises the structure and function of lung tissue, leading to aggravated V/Q mismatch 29 and impaired optimal pulmonary gas exchange, which could potentially induce or even exacerbate hypercapnia. Severe hypercapnia, particularly with significant acidosis, can induce systemic complications including peripheral vasodilation with hypotension, cerebral edema, intracranial hypertension, hemodynamic instability, life-threatening arrhythmias, and even death.30,31
The most commonly used CAP severity assessment tools are CURB-65, PSI and SMART-COP. Although the CURB-65 score is simple and easy to use, its specificity may be limited due to atypical symptoms and non-specific laboratory markers in early-stage or elderly patients. 32 The PSI score, which includes 20 parameters, may underestimate disease severity in young and otherwise healthy patients due to its heavy weighting on age and comorbidities. 33 Therefore, both scores are considered suboptimal for determining ICU admission requirements in CAP.33,34 However, recent studies have shown that PSI and CURB-65 scores still have certain value in predicting ICU admission risk or assessing the severity of pneumonia, with AUC values ranging from 0.69 to 0.796.35 –37 These phenomena may be attributed to the high proportion of elderly patients included in these studies, as both CURB-65 and PSI emphasize age as a key factor. In the AECOPD+SCAP cohort of our study, 69.7% of patients were aged over 60% and 43.2% met the PSI comorbidity criteria. The SMART-COP score is used to predict the need for intensive respiratory or vasopressor support (IRVS) in CAP patients, thus indirectly assessing the requirement for ICU admission.35,38 Meanwhile, qSOFA, as a rapid sepsis screening tool, also demonstrates utility in assessing CAP severity and predicting the need for ICU admission.36,39 Our nomogram, which integrates four indicators (hypercapnia, the PaO2/FiO2 ratio, lactate and RDW-CV), demonstrated a higher AUC value of 0.72 for predicting ICU admission risk in AECOPD+SCAP patients than the aforementioned pneumonia severity scores, though the difference was not statistically significant. Given its simplicity, effective risk-stratification capability for ICU admission and verified predictive performance and clinical utility using calibration curves and DCA, the nomogram could potentially be implemented in emergency departments or outpatient clinics.
In preclinical models, hypercapnia alleviates pulmonary inflammation by the pH-independent inhibition of the NF-kappaB (NF-κB) pathway, 40 which plays a pivotal role in mediating inflammatory responses. 41 However, this process can potentially delay epithelial wound healing and impair bacterial clearance.1,40,42 In vitro study has demonstrated that hypercapnia inhibits macrophage expression of Tumor Necrosis Factor-alpha(TNF-α) and IL-6 via NF-κB. 42 Subsequently, an animal experiment further confirmed that hypercapnia reduces the levels of IL-6 and TNF-α in the lungs in the early stage of pneumonia. 1 Pro-inflammatory cytokines, such as IL-6 and TNF-α, regulate the synthesis of both CRP and PCT.43,44 In addition to the aforementioned regulation by cytokines, the transcription of the CRP and PCT genes can be directly activated by NF-κB during the acute inflammatory response.45,46 A retrospective clinical study found that SCAP patients with hypercapnia had lower blood levels of CRP and PCT within 24 h of admission than those with normocapnia or hypocapnia. 2 Previous studies have shown that CRP and PCT levels are significantly elevated in COPD patients with pneumonia compared to those with acute exacerbation of COPD without pneumonia.47 –49 Our research found that, on the day of admission, CRP, PCT and lactate levels were lower in AECOPD and SCAP patients with hypercapnia than in the hypocapnia group. Furthermore, a weak inverse correlation was identified between PaCO2 and CRP, PCT, and lactate levels. These results provide new evidence that hypercapnia can inhibit the early inflammatory response and lactate secretion in AECOPD patients with severe pneumonia. A subgroup analysis limited to ICU patients yielded similar findings, suggesting that hypercapnia influences innate immune responses in AECOPD with SCAP. Another subgroup analysis revealed that, compared to the hypocapnia group, both CRP and lactate levels were significantly lower in patients with hypercapnia without acidosis. Furthermore, PCT levels were significantly lower in hypercapnic patients, regardless of acidosis, compared to the hypocapnia group. These results suggest that hypercapnia’s suppression of the inflammatory response in these patients is likely to be mediated by non-acidotic mechanisms rather than being primarily dependent on acidosis itself. Moreover, the use of SCS prior to admission did not significantly affect the levels of these markers, thus making the results more reliable. Based on the above preclinical research results and our findings, we speculate that the reason why hypercapnia was found to inhibit the inflammatory response in patients with AECOPD and SCAP at an early stage might be as follows: hypercapnia may inhibit the NF-κB signaling pathway, which in turn downregulates IL-6 and TNF-α expression, thereby diminishing circulating CRP and PCT concentrations; on the other hand, hypercapnia may directly reduce gene transcription of CRP and PCT by inhibiting the NK-FB pathway, thereby decreasing their protein levels in the blood. Lac, a metabolic and signaling molecule, 50 sometimes increases in AECOPD due to the cumulative use of high-dose beta-2 receptor agonists 19 or potential complications such as sepsis shock and Cardiogenic shock. 51 Our study revealed significantly lower lactate levels in the hypercapnia group than in the hypocapnia group among patients with AECOPD and SCAP on the day of admission. The mechanisms behind this association remain unclear and require further investigation.
Strengths and limitations
Previous studies have rarely explored the relationship between hypercapnia and the clinical characteristics as well as early infection severity in patients with AECOPD complicated by severe pneumonia. To the best of our knowledge, our study filled a critical gap in this area of research.
This dual-center retrospective study has several limitations. Firstly, the sample size may restrict the statistical power of some analyses, highlighting the need for future prospective validation in larger cohorts. It should also be noted that dynamic biomarker monitoring was not conducted and that external validation of the ICU admission prediction model for AECOPD patients with SCAP is required. Potential biases arising from missing variables such as pre-admission hypercapnia, body mass index (BMI), cause of death, lung function within 1 year prior to admission, physical or respiratory rehabilitation treatments during hospitalization and long-term medication use also warrant consideration.
Conclusion
Our study revealed that hypercapnia was not significantly associated with the requirement for IMV, in-hospital mortality or 30-day mortality in patients with AECOPD and SCAP, while it was linked to greater disease severity, an increased risk of ICU admission (particularly in patients with concomitant acidosis) and impaired anti-infective capacity—a mechanism largely independent of acidosis. Hypercapnia, combined with the PaO2/FiO2 ratio, lactate, and RDW-CV, achieved good accuracy comparable to the severity scores (qSOFA, PSI, CURB-65 and SMART-COP) in predicting ICU admission risk for AECOPD patients with SCAP. Therefore, we believe that hypercapnia could be a promising indicator of the severity of AECOPD with SCAP.
Supplemental Material
sj-doc-1-tar-10.1177_17534666261467258 – Supplemental material for Hypercapnia is associated with an increased risk of ICU admission and reduced inflammatory responses in AECOPD patients with severe pneumonia
Supplemental material, sj-doc-1-tar-10.1177_17534666261467258 for Hypercapnia is associated with an increased risk of ICU admission and reduced inflammatory responses in AECOPD patients with severe pneumonia by Shan Mou, Qi Cai, Wei Xu, Xiaohao Wang, Lei Mao, Lijuan Li, Li Zhang and Yan Zhang in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-doc-2-tar-10.1177_17534666261467258 – Supplemental material for Hypercapnia is associated with an increased risk of ICU admission and reduced inflammatory responses in AECOPD patients with severe pneumonia
Supplemental material, sj-doc-2-tar-10.1177_17534666261467258 for Hypercapnia is associated with an increased risk of ICU admission and reduced inflammatory responses in AECOPD patients with severe pneumonia by Shan Mou, Qi Cai, Wei Xu, Xiaohao Wang, Lei Mao, Lijuan Li, Li Zhang and Yan Zhang in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-docx-1-tar-10.1177_17534666261467258 – Supplemental material for Hypercapnia is associated with an increased risk of ICU admission and reduced inflammatory responses in AECOPD patients with severe pneumonia
Supplemental material, sj-docx-1-tar-10.1177_17534666261467258 for Hypercapnia is associated with an increased risk of ICU admission and reduced inflammatory responses in AECOPD patients with severe pneumonia by Shan Mou, Qi Cai, Wei Xu, Xiaohao Wang, Lei Mao, Lijuan Li, Li Zhang and Yan Zhang in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-docx-2-tar-10.1177_17534666261467258 – Supplemental material for Hypercapnia is associated with an increased risk of ICU admission and reduced inflammatory responses in AECOPD patients with severe pneumonia
Supplemental material, sj-docx-2-tar-10.1177_17534666261467258 for Hypercapnia is associated with an increased risk of ICU admission and reduced inflammatory responses in AECOPD patients with severe pneumonia by Shan Mou, Qi Cai, Wei Xu, Xiaohao Wang, Lei Mao, Lijuan Li, Li Zhang and Yan Zhang in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-docx-3-tar-10.1177_17534666261467258 – Supplemental material for Hypercapnia is associated with an increased risk of ICU admission and reduced inflammatory responses in AECOPD patients with severe pneumonia
Supplemental material, sj-docx-3-tar-10.1177_17534666261467258 for Hypercapnia is associated with an increased risk of ICU admission and reduced inflammatory responses in AECOPD patients with severe pneumonia by Shan Mou, Qi Cai, Wei Xu, Xiaohao Wang, Lei Mao, Lijuan Li, Li Zhang and Yan Zhang in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-docx-4-tar-10.1177_17534666261467258 – Supplemental material for Hypercapnia is associated with an increased risk of ICU admission and reduced inflammatory responses in AECOPD patients with severe pneumonia
Supplemental material, sj-docx-4-tar-10.1177_17534666261467258 for Hypercapnia is associated with an increased risk of ICU admission and reduced inflammatory responses in AECOPD patients with severe pneumonia by Shan Mou, Qi Cai, Wei Xu, Xiaohao Wang, Lei Mao, Lijuan Li, Li Zhang and Yan Zhang in Therapeutic Advances in Respiratory Disease
Footnotes
Appendix
Acknowledgements
The authors gratefully acknowledge the invaluable support provided by the staff of the Department of Infectious Diseases at the Second Clinical Hospital of Chongqing Medical University and The First People’s Hospital of Shuangliu District, Chengdu.
Declarations
Supplemental material
Supplemental material for this article is available online.
Use of artificial intelligence
No artificial intelligence(AI) tools were used to generate, analyze, or modify any data, figures, or results in this manuscript. All data collection, statistical analysis, interpretation of results, and conceptual writing were independently completed by the authors. We fully comply with the journal’s editorial policy on AI use.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.