
Abstract
Intravenous fluid given to women with pre-eclampsia may be a necessary form of treatment; however, intravenous fluid therapy can also cause iatrogenic pulmonary oedema. The indications for the use of intravenous fluids, the titration of the amount of fluid given and the use of invasive monitoring have not been subject to adequate examination in randomised studies. Clinical experience, combined with available evidence and a reasoned approach are the basis for a suggested management algorithm.
Introduction
In South Africa, a country with a high incidence of maternal mortality due to pre-eclampsia, the main causes of death are cerebrovascular haemorrhage and pulmonary oedema. 1 Pulmonary oedema is now recognized as the most common final cause of death in women with complications of hypertension (Saving Mothers 2008–2010). 1 Intravenous fluid given to women with pre-eclampsia may increase their risk of developing pulmonary oedema, although fluid administration is clearly necessary in certain circumstances including the management of renal failure and hypovolaemia as well as an adjunct to vasodilation. The benefits and risks of giving intravenous fluids to women with pre-eclampsia require individual assessment of patients based upon general principles. The South African Committee for Confidential Enquiry into Maternal Deaths have recommended that fluid balance be very carefully monitored before and following delivery in severe hypertension, imminent eclampsia, eclampsia and the HELLP syndrome. 1
This review examines the reasons why pre-eclamptic women go into pulmonary oedema following fluid administration. The indications for intravenous fluid administration are then discussed together with aspects of haemodynamic monitoring
The haemodynamic characteristics of pre-eclampsia and development of pulmonary oedema (Table 1)
The causes of pulmonary oedema in pre-eclampsia.
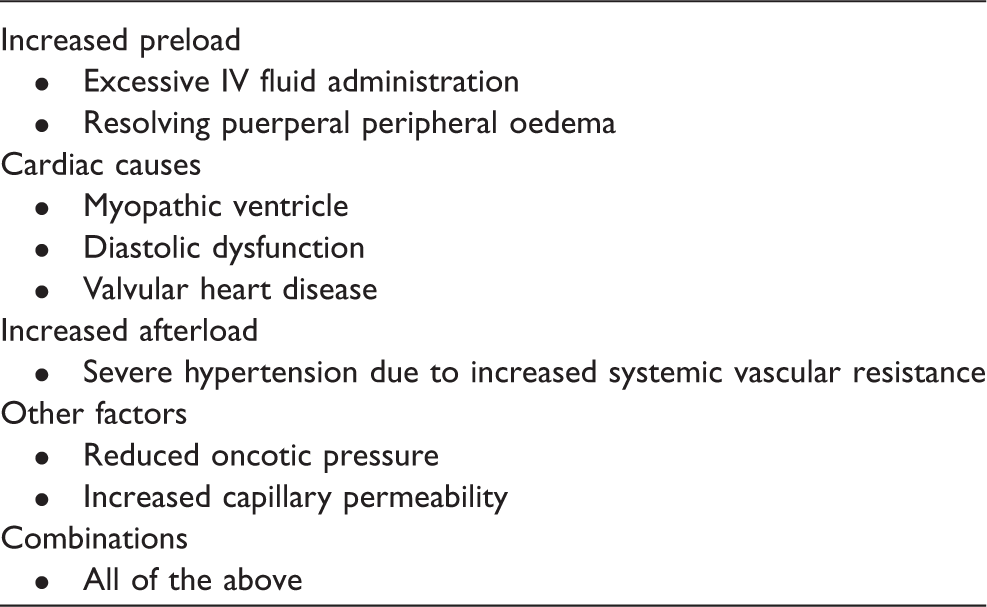
The hypertension of untreated severe pre-eclampsia in primigravid women is caused by raised peripheral vascular resistance. Ventricular function is usually normal and filling pressures for both the left and right side of the heart are in the normal range. 2 More diverse haemodynamic findings occur in women with pre-eclampsia who have co-morbid conditions (such as underlying chronic hypertension, other forms of cardiac disease or hypovolaemia). The effects of intravenous fluid administration and vasodilation also change the haemodynamic phenotype. 3 Studies using echocardiography have variably reported elevated cardiac output with mild vasoconstriction and reduced left ventricular diastolic function. The largest longitudinal series of such patients showed that the pattern of high cardiac output changed with the evolution of clinical disease into a vasoconstricted state and reduced cardiac output. 4,5 Clinical examination alone cannot discriminate between the different haemodynamic subsets found in treated severe pre-eclampsia.
Pulmonary oedema is due to interstitial fluid accumulation in the lungs. The development of interstitial oedema depends upon the hydrostatic pressure in the pulmonary capillaries, the oncotic pressure holding fluid in the intravascular space, the integrity of the semi-permeable capillary endothelium and the drainage of the lungs through the lymphatic vessels. In pre-eclampsia, oncotic pressure falls as protein is lost through urinary excretion and the capillary permeability may alter in some patients. 6 The hydrostatic pressure in the pulmonary capillary bed also changes and is proportional to left atrial pressure. This may be inferred from changes in the pulmonary capillary wedge pressure (PCWP). 7 Elevated PCWP is found in some women with pre-eclampsia for a number of reasons.
Any increase in peripheral vascular resistance (afterload) may increase the pulmonary capillary wedge pressure with vasodilation having the reverse effect. Abnormalities of ventricular function also cause elevated left-sided filling pressures. Abnormal systolic function (cardiomyopathy) or diastolic dysfunction (reduced compliance of the ventricular muscle during diastole) both increase pulmonary capillary wedge pressure. Valvular heart disease (commonly mitral stenosis) can lead to elevated left-sided filling pressures. Excessive intravenous fluid therapy on its own or together with one or more of the preceding mechanisms may also increase the hydrostatic pressure in the pulmonary vasculature leading to pulmonary oedema. 8
Abnormal left-sided cardiac filling pressures cannot be determined by any aspect of the clinical presentation; consequently, intravenous fluid administration must remain within a safe threshold or be guided by haemodynamic monitoring.
Monitoring the administration of intravenous fluid in pre-eclampsia
Intravenous fluid administration may be used as maintenance therapy or for replacement of lost intravascular volume. Maintenance therapy is commonly given slowly over 24 h and may be calculated to match the urinary output combined with insensible loss. The rate of administration can be controlled and in the presence of normal renal function is not likely to cause any complications. Replacement therapy is administered according to an estimated deficit and is usually transfused rapidly. Co-morbidity due to renal failure complicates intravenous fluid administration because the kidneys may not respond to diuretic therapy making over-transfusion an inevitable cause of pulmonary oedema. Haemodynamic monitoring in these cases may prevent iatrogenic complications.
Monitoring fluid therapy may be based upon clinical observation or the estimation of filling pressures. Clinical methods include observation of blood pressure, pulse rate and urinary output. The resolution of severe hypovolaemia is accompanied by a rising blood pressure, falling pulse rate and increasing urinary output. These clinical markers of euvolaemia may be inaccurate in women with severe pre-eclampsia. Oliguria may develop in pre-eclamptic women because of intrinsic renal disease (including acute tubular necrosis) and may not respond to plasma volume expansion with an increase in urinary output. 8 Tachycardia commonly complicates severe pre-eclampsia and a persistently rapid pulse rate may not be a reliable indication of intravascular volume depletion, especially when the systolic blood pressure is within normal limits.
Haemodynamic monitoring of intravascular blood volume may be achieved in different ways that include measurement of central venous pressure and by assessing pulmonary capillary wedge pressures. The adequacy of peripheral oxygen delivery and consumption, which is directly dependent on cardiac output and the circulating blood volume can be formally assessed using a pulmonary artery catheter although simpler measures of central venous oxygen saturation may also provide an indication of perfusion. 9 Of these methods, the two most commonly employed are monitoring right or left-sided cardiac filling pressures. A central venous pressure line provides right atrial pressure measurements that have been held to be a good guide to intravascular volume, allowing intravenous fluids to be given in bolus doses until a sustained rise in venous pressure can be demonstrated. 10 The utility of central venous pressure measurements has been questioned with a systematic review showing a poor correlation between these measurements and blood volume. 11 In pre-eclamptic women, the use of central venous pressure monitoring may be directly dangerous because bolus doses of fluid may lead to a sharp increase in pulmonary capillary wedge pressure before any rise in central venous pressure is observed. 12 There may be changes in left ventricular compliance that account for this occurrence, even when systolic ventricular function is normal. 4 A sharp rise in pulmonary capillary wedge pressure may precipitate pulmonary oedema due to increased hydrostatic pressure in the pulmonary vascular bed. Central venous pressure lines should therefore not be used as a guide to fluid therapy in severe pre-eclampsia. The use of pulmonary artery catheters should be confined to those circumstances where large volumes of intravenous fluid need to be given and in cases where such monitoring is not available, rapid volume expansion should be avoided.
The other techniques of assessing intravascular volume are also a guide to fluid replacement but do not measure left ventricular filling pressures and are consequently of as little value in the management of patients with severe pre-eclampsia as central venous pressure lines. Stroke volume variability may allow an assessment of fluid responsiveness in ventilated patients but is not tested in pregnancy. 13 Echocardiography has been used to assess left ventricular systolic function in patients with severe pre-eclampsia. 14 Transthoracic echocardiography also allows assessment of left ventricular diastolic function by measuring indices such as the ratio of the flow velocity across the mitral valve immediately after opening of the mitral valve and during atrial systole (E/A ratio). 15
Clinical experience has provided some evidence supporting the utility and safety of pulmonary artery catheterization; however, no randomized studies have been performed showing that the measures used to assess central haemodynamic changes are of benefit in the management of severe pre-eclampsia. 16,17 It is also unlikely that any statistically relevant conclusion will ever be attainable given the relative rarity of severe pre-eclampsia. In the light of this uncertainty, attention should be directed to causing no harm. It is clear that central venous pressure lines are an unreliable measure of central haemodynamic events and the insertion of pulmonary artery catheters, especially in inexperienced hands may result in morbidity and procedure related mortality. 18 –21 In the absence of adequate monitoring, the infusion of intravenous fluids is a recognized cause of iatrogenic pulmonary oedema. Consequently, the management of severe pre-eclampsia is best confined to referral hospitals where clinical expertise, multidisciplinary care and access to haemodynamic monitoring are all available. When this is not possible, clinical management should be conducted using a restrictive policy of fluid management based upon replacing fluid losses only. Because of the inherent risk of pulmonary oedema, all women who need to receive intravenous fluids in more than maintenance doses should also be monitored using pulse oximetry which may allow the early detection of pulmonary oedema.
Euvolaemia and the indications for intravenous fluid administration (Table 2)
Indications for intravenous fluids in preeclampsia.
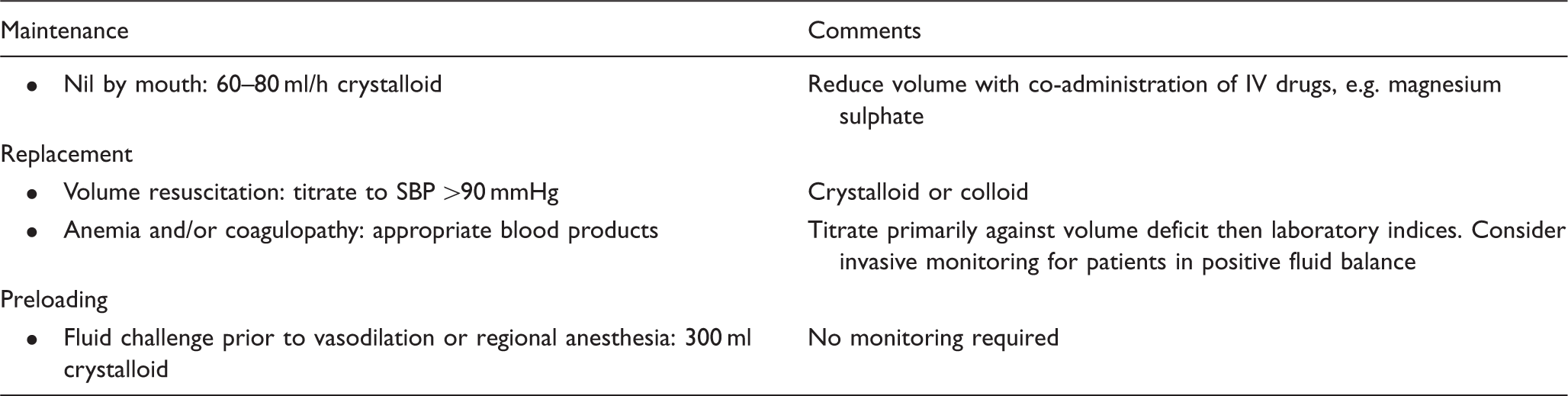
Intravenous fluids are given as maintenance fluids or to expand the intravascular volume prior to vasodilatation or during resuscitation. In each circumstance, principles uniquely associated with the diagnosis of pre-eclampsia apply.
Maintenance
The pre-eclamptic patient without complications may require intravenous therapy either because they are nil per mouth or as a vehicle for drug administration.
Maintenance fluid in women who are nil per os are given slowly over a 24 h period and can be given in a fixed regimen of 60–80 ml per hour (equivalent to 1.5 l of balanced salt solution) or can be titrated against output plus insensible losses. 24 The development of peripheral oedema entails a loss of fluid from the intravascular compartment making the latter calculation an inaccurate guide to euvolaemia. The slow administration of intravenous fluid is unlikely to lead to pulmonary oedema in a patient who has normal renal function; hence, a fixed regimen of 100 ml per hour can be safely used.
Drugs are often given as a diluted solution. Magnesium sulphate is often administered as a bolus dose of 4 g in 200 ml of dextrose over 30 min followed by the same dose every 4 h. The volume of fluid given should always be taken into account when calculating the total volume of fluids given during a 24 h period. In the latter case, it would have the effect of reducing other maintenance fluids to 50 ml per hour.
Pre-loading
Blood pressure is derived from the product of vascular resistance and cardiac output. When systemic vascular resistance is lowered, the maintenance of blood pressure depends upon an increase in cardiac output. This in turn requires changes in heart rate, stroke volume or both. An increase in stroke volume is attainable only when the preload (ventricular filling pressure) allows greater filling of the ventricle and ejection of a bigger volume of blood from the left ventricle.
Untreated severe pre-eclampsia is associated with peripheral vasospasm and hypertension. The haemodynamic effect of bolus-dose intravenous fluids in untreated severe pre-eclampsia is a reduction in systemic vascular resistance, an increase in cardiac output and improved rates of peripheral oxygen delivery and consumption. This is accompanied by little, if any change in blood pressure (the rise in cardiac output offsets the reduction in vascular resistance). 8
Vasodilation using any vasoactive drug will lower the blood pressure and may do so precipitously if vasodilators are given without prior intravenous fluid administration to increase the left ventricular preload. 25 The same considerations apply to the induction of regional anaesthesia. 26 Even in the absence of a precipitous drop in blood pressure, a reduction in systemic pressure that is not matched by sufficient increase in cardiac output may lead to a reduction in peripheral (including uterine) perfusion. Intravenous fluid pre-loading is a necessary intervention prior to vasodilation. Given the risks of pulmonary oedema and the difficulty of instituting adequate monitoring, a fluid challenge immediately prior to vasodilation is given as a bolus of 300 ml of intravenous fluid (usually a colloidal solution). This practice is based upon clinical experience and has not been tested in randomized studies.
Managing renal failure (Table 3)
Intravenous fluids for oliguric preeclampsia.
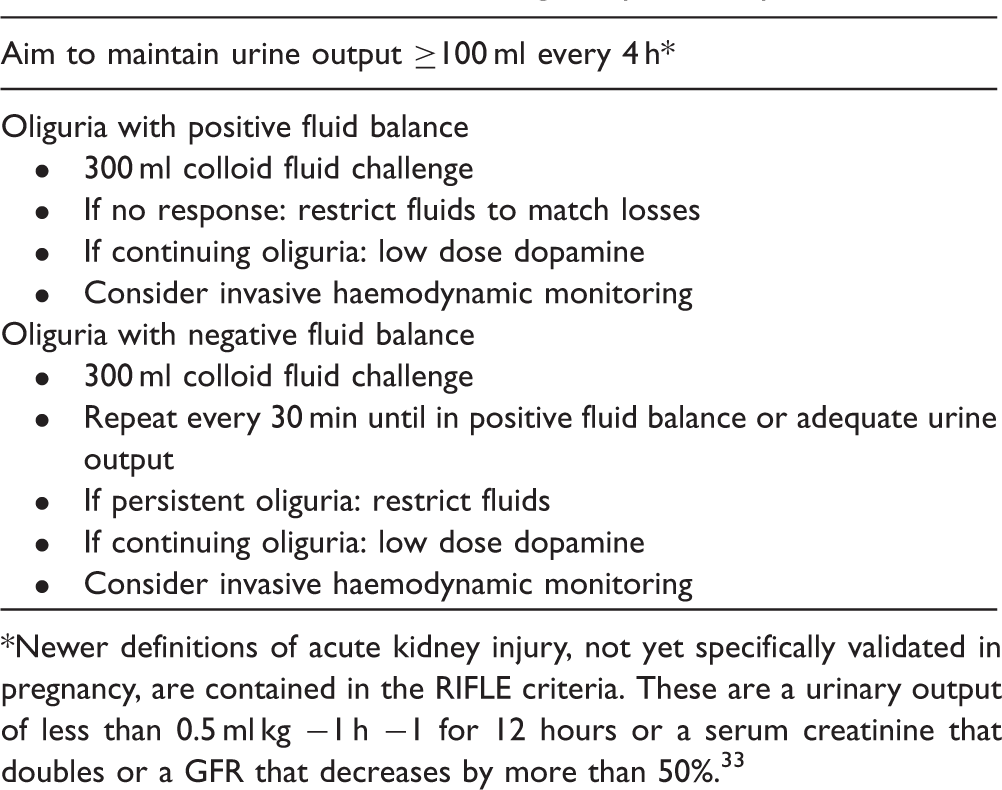
*Newer definitions of acute kidney injury, not yet specifically validated in pregnancy, are contained in the RIFLE criteria. These are a urinary output of less than 0.5 ml kg −1 h −1 for 12 hours or a serum creatinine that doubles or a GFR that decreases by more than 50%.33
In the absence of a hypovolaemic event, oliguria developing in pre-eclamptic women may be the consequence of both pre-renal and renal factors. The pre-renal cause may be reversed by vasodilation and increasing the cardiac output leading to improved perfusion. The intrinsic renal abnormalities include endotheliosus, ischaemic injury and damage related to haemoglobinuria, the effects of which cannot be reversed immediately. 28 It is also not clinically possible to distinguish between pre-renal mechanisms, intrinsic renal disease or a combination of the two as a cause for oliguria. Where vasodilation and improved perfusion lead to improved urinary output, it may be assumed that the dominant mechanism is pre-renal. Persistent attempts to restore urinary output by means of plasma volume expansion based upon the supposition that oliguria is exclusively due to pre-renal factors will lead to iatrogenic pulmonary oedema.
Because of the difficulty in diagnosing the cause of oliguric renal failure, a step-wise and limited approach to fluid therapy should be used. The goal of this therapy should be to ensure adequate renal perfusion with or without restoration of a normal hourly urinary output.
Women who are in positive fluid balance (intravenous fluids greater than measured output plus an insensible loss of 500 ml) should be distinguished from those whose losses exceed their input. The latter category may be given repeated fluid challenges until urinary output is restored or fluid balance has been established. Women who are in a positive fluid balance and who are oliguric may be given a limited fluid challenge to try to improve urinary output. The limits of this challenge are arbitrary and untested in clinical studies. The only way to ensure that the haemodynamic profile of severe pre-eclampsia is fully corrected in an oliguric patient despite fluid challenges is by means of invasive haemodynamic monitoring using a pulmonary artery catheter. This will only be attainable in a limited number of cases where patients have been referred to hospitals with obstetric intensive care facilities able to provide this type of monitoring. 27
The suggested guideline for unmonitored fluid challenges is 300 ml aliquots of intravenous fluid (usually colloid) given as a bolus dose and repeated once in those who fail to respond by passing an average of 30 ml of urine per hour. Women with pre-eclampsia who remain oliguric after this should either be referred for invasive monitoring or fluid therapy should be reduced to output plus insensible loss calculated over a 24 h period.
Low-dose dopamine (1–5 µg/kg/min) has been used in women with persistent oliguria following fluid challenges and may have a role in improving renal perfusion and urinary output. 29
Resuscitation
Patients with severe pre-eclampsia are at risk of developing hypovolaemia commonly because of abruptio placentae, occasionally because of operative blood loss or other causes of obstetric haemorrhage and rarely because of co-morbidity such as a ruptured subcapsular liver haematoma. The management of the individual causes of hypovolaemia need to be combined with an approach to fluid resuscitation. The general principles of resuscitation have reference to this and include the restoration of euvolaemia, correction of clotting defects and restoration of the oxygen carrying capacity of the blood.
Shocked pre-eclamptic women need to be resuscitated in the same way as any other hypovolaemic patient. The focus of resuscitation should be on restoring the systolic pressure to above 90 mm Hg with less attention paid to urinary output and pulse rate as a guide to the establishment of euvolaemia. Initial resuscitation with clear fluids should be superseded by blood component therapy. The possibility of over-transfusion and pulmonary oedema should be considered once the systolic blood pressure has stabilized and any further fluid therapy should be based upon replacement of losses or guided by appropriate haemodynamic monitoring. Inadequate resuscitation may prolong peripheral organ ischaemia and increase the likelihood of renal failure. 28 However, over-aggressive transfusion, especially in the absence of monitoring, will lead to iatrogenic pulmonary oedema which will be difficult to reverse if the patient has sustained a renal injury. Pulmonary oedema is an immediate and significant cause of maternal mortality whereas the effects of renal failure are usually reversible in the short-term. 1,27
Although the avoidance of pulmonary oedema is of overriding importance, early and complete resuscitation may limit the risk of renal injury. Patients who develop renal failure due to severe pre-eclampsia commonly recover normal renal function after delivery (measured as a normal serum creatinine) but there is also evidence that they are at statistically significantly increased risk of end-stage renal failure later in life. 27,30 It is likely that the development of oliguric renal failure in women who have a hypovolaemic event superimposed on a vasoconstricted peripheral blood supply is prone to ischaemic damage. Both tubular necrosis and cortical damage are described. 28 The rapid and adequate restoration of renal perfusion may be the only opportunity of preventing this from happening. To achieve this end, patients would need to have access to intensive care facilities and adequately trained clinical staff. The development of end-stage renal failure in many developing countries is a serious diagnosis because access to dialysis is highly restricted. 31
The choice of intravenous fluids: colloids versus crystalloids
Women with pre-eclampsia lose protein through renal excretion and may also extravasate protein into the interstitial tissues. Oncotic pressure falls because of this and the tendency to lose fluid from the intravascular space is partially determined by this mechanism. Filling the vascular space with fluid will lead to increasing peripheral oedema. Colloids will remain in the vascular compartment for longer periods than crystalloids although the loss of colloid into the interstitial tissues will also contribute to the development of oedema. 24 Changes in capillary permeability will have an independent influence. It is not clear that colloidal solutions would be more effective and less likely to cause harm than crystalloids. In general critical care there is no epidemiological evidence to support the choice of colloidal solutions over crystalloids; however, the meta-analysis specifically excludes pregnant women and neonates. 32 Consequently, there is inadequate evidence supporting one view or another in the management of pre-eclampsia.
As a matter of clinical practice, colloidal solutions are given where fluid therapy is specifically required whereas all other maintenance fluids are crystalloid solutions.
Conclusion
There is a paucity of evidence-based guidelines concerning intravenous fluid administration in pre-eclampsia. However, the decision to administer fluid to a pre-eclamptic woman is both a necessary and important judgement given the risk of iatrogenic pulmonary oedema. It should never happen by default but without an adequate evidence base, the principles of management have to be derived from clinical experience combined with a reasoned approach.
Footnotes
Ethical approval
None.
Declaration of Conflicting Interests
None.