
Abstract
Objectives:
Pregnancy represents a special situation where both the mechanical and hormonal instigating factors of varicose veins are reversible with the venous valve cusps preserved. Exostent venous valve repairs are a physiological alternative which minimises stimulus to collateral growth (recurrence). The study purpose was to assess the effect of pregnancy on the durability of valve repairs.
Methods:
In a prospective study of 36 limbs, 20 young females (30 ± 4.7 years) had an exostent implanted to the terminal valve of the saphenofemoral junction for varicose veins. At routine long-term follow up (9.7 ± 3.8 years), 38 pregnancies were completed (mean: 1.8, range: 1–4). The controls were a non-pregnant group of limbs (n = 386).
Results:
At 9.7 years, the internal diameter of the greater saphenous vein (GSV) changed from 7.8 ± 2.8 mm preoperatively to 4.5 ± 1.4 mm post-operatively. Recurrence was associated with reflux, preoperative deep system and ovarian vein involvement. Pregnancy induced 33.3% recurrences compared with non-pregnant controls (4.7%) similarly treated or 22.8% compared with non-pregnant ablative controls. At 9.7 years, symptomatic improvement continued with significantly better CEAP status (described later) (31CSEAP preoperative to 6CSEAP) with no further truncal ablation (strip, laser) required.
Conclusions:
Venous valve repairs can withstand the special stresses of pregnancy. There is no need to ablate the GSV. This approach is contrary to the traditional dictum; the treatment of varicose veins should be delayed until the family is completed.
Keywords
Introduction
Pregnancy, particularly multiple pregnancies, is a major factor in the development and exacerbation of varicose veins.1−4 However, pregnancy represents a special and different vascular status: many of its effects are essentially reversible and yet cumulative. The contributing factors are a mechanical obstruction of the venous outflow in the pelvis, increased circulating blood volume and hormonal effects causing smooth muscle dilatation with an inhibition of normal contractility.5−7 All of these factors summate to create dilatation of the venous valve rings rather than cusp degeneration which is a function of age. 8 The post-pregnant patient presents at an earlier age with tributary and perforator incompetence rather than truncal dilatation. 9 The perforating systems are often paravaginal and associated with new ovarian vein incompetence which also may be symptomatic in their own right. 9 These younger patients are more sensitive to the effects of varicose veins and tend to present earlier.
These differing, reversible etiological factors demand a different approach to simply destroying the greater saphenous system with radiofrequency, laser or stripping. A venous exostent is a simple valve support implant which decreases the internal diameter of the valve ring allowing apposition of the cusps with re-establishment of one way flow.8,9 The development of high quality ultrasonic venous valve imaging has improved the selection criteria for venous valve repair of the greater saphenous vein (GSV) system. 10 As the Australian Medicare Database 11 indicates, over recent times 3372 devices have been implanted with repair of the terminal and/or sub terminal valves of the GSV. The aims of this communication are to compare the effect of pregnancy on varicose veins and their recurrence compared with a non-pregnant control group. 12 Further to this, to report the incidence of recurrence and reversal of truncal dilatation with stent repair, to define the effect of ovarian vein incompetence and to highlight the differing anatomical distribution of post-pregnant recurrent varicose veins which suggests a physiological form of treatment related to the special reversible effects of pregnancy.
In summary, to report the 10-year durability of stent repair to the sapheno femoral junction (SFJ) and or sub-terminal valves implanted prior to or in between pregnancies.
Methods
Patients
Demographics.
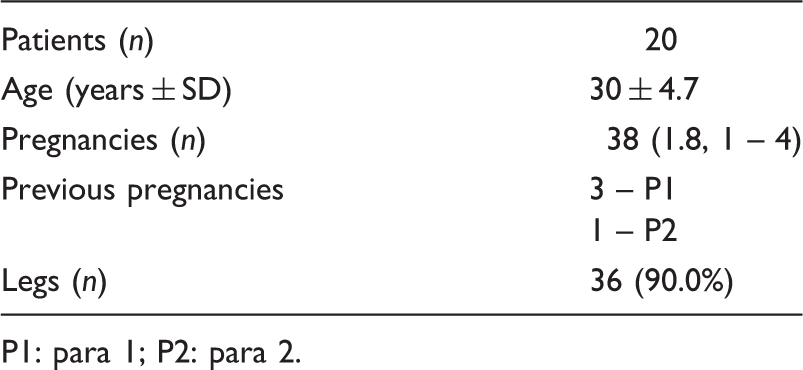
P1: para 1; P2: para 2.
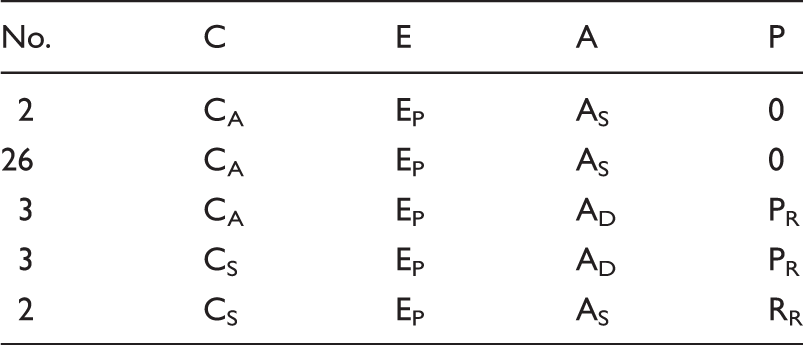
International CEAP classification (preoperative).
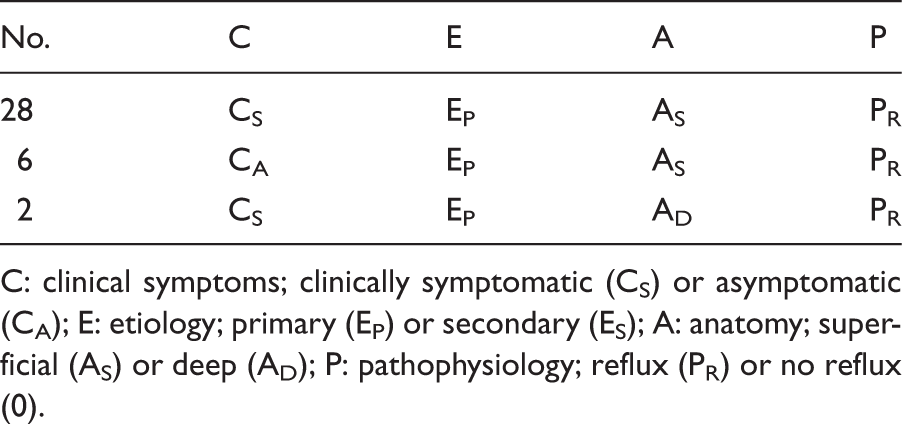
C: clinical symptoms; clinically symptomatic (CS) or asymptomatic (CA); E: etiology; primary (EP) or secondary (ES); A: anatomy; superficial (AS) or deep (AD); P: pathophysiology; reflux (PR) or no reflux (0).
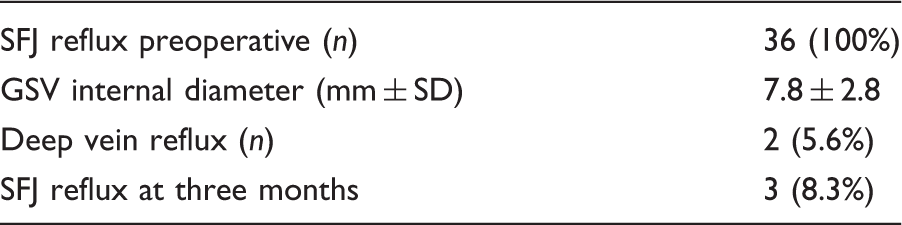
Preoperative valve repair and short-term follow-up.
Controls
From a database of a large venous clinic, 193 controls (121 females to 72 males with a mean age of 48.1 ± 7.2 years) were obtained. Controls were defined as patients with no recorded pregnancies with stripping on one side and a simultaneous stent repair to the SFJ of the other limb (386 limbs). These patients were enrolled as per Figure 1 and followed up clinically and ultrasonically for up to 12.7 years.
Enrolment process for pregnant and control patients.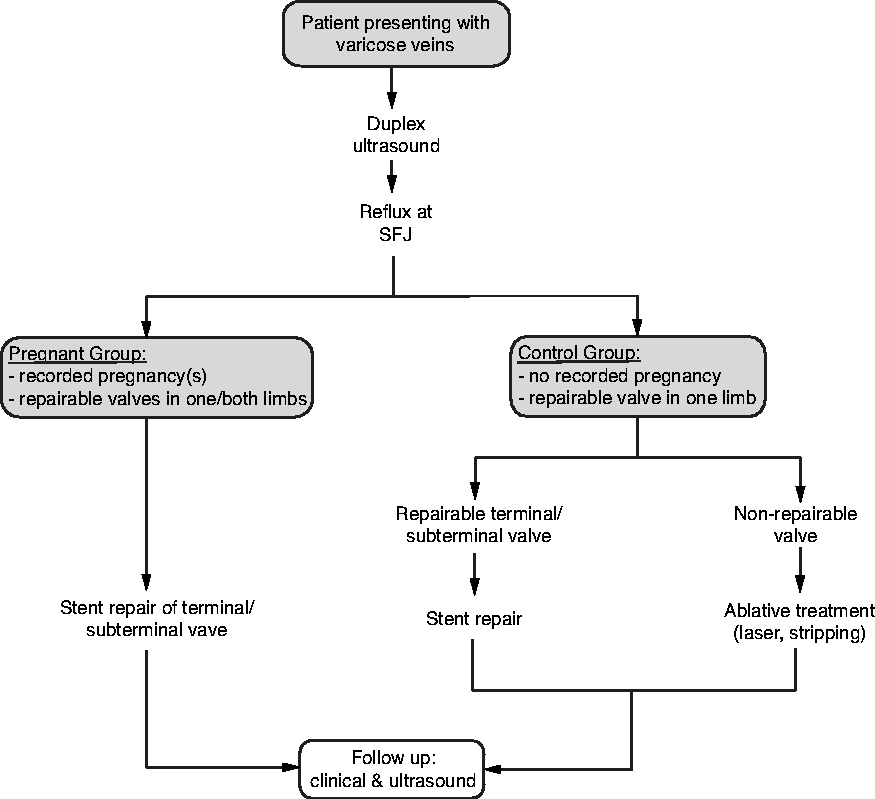
Materials
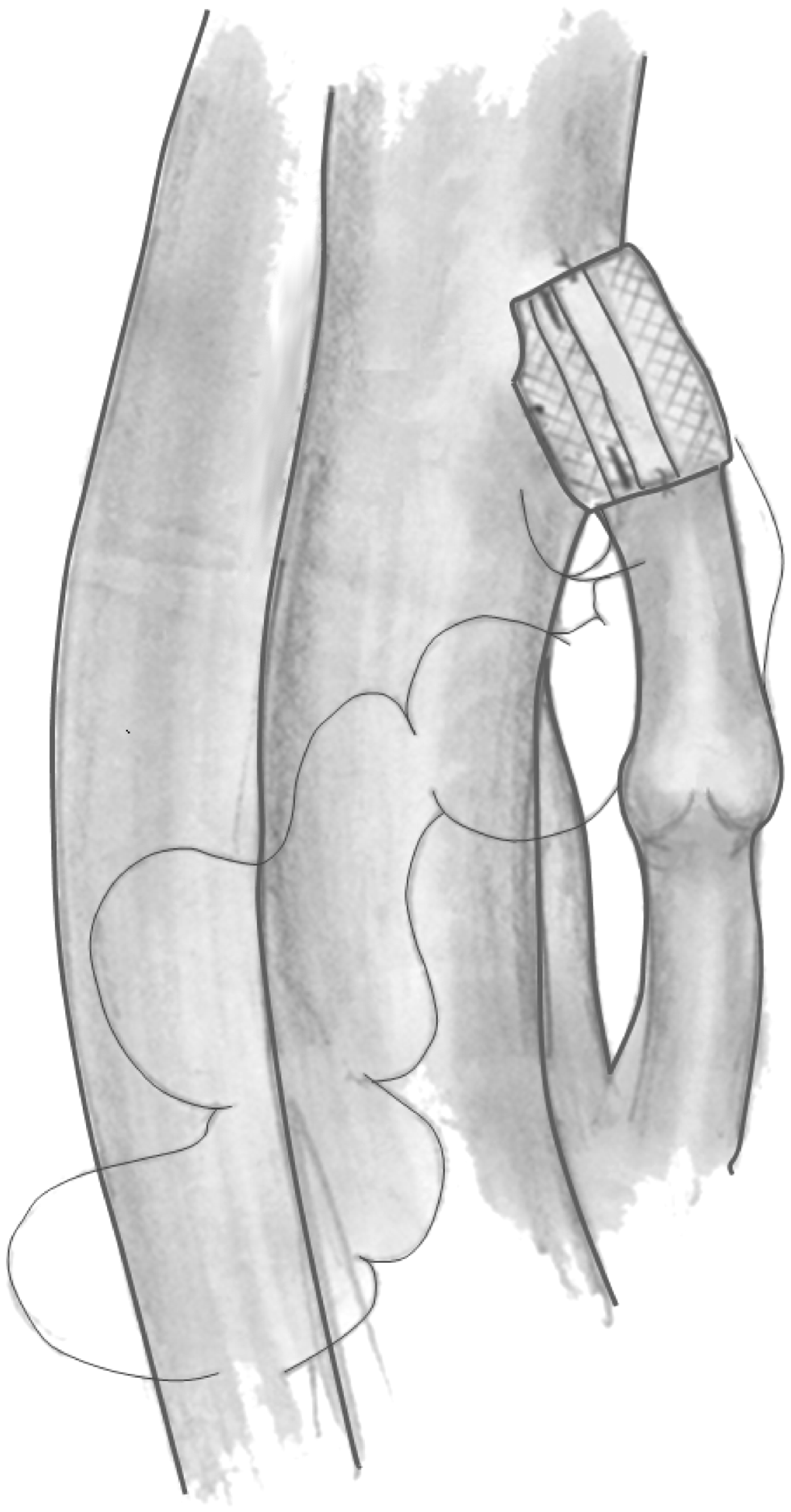
The Venocuff (Figure 2) is a Dacron reinforced variable diameter exostent manufactured by Allvascular, St Leonards, Australia. Figure 3 shows the basic concept of exostent venous valve repair. The left and right Venocuffs are designed specifically to externally plicate the SFJ. The un-notched version has been designed for the subterminal valves of the GSV or the deep venous system. There are three holes within the body of the stent indicating internal diameters (including the vein wall of 4.5, 5.5 and 6.5 mm). The smallest diameter is for a small woman (<160 cm) whilst the largest is for a large male (>180 cm).
The three different exostents: Left and right ones are notched; the un-notched stent is for the subterminal valve or the deep system. The holes in the body of the exostent indicate diameters 4.5, 5.5, 6.5 mm for various increasingly large phenotypes. Schematic of the standard venous exostent with the notch fitting snuggly at the SFJ. The diameter is fixed by sutures through the buckle and body combined both superiorly and inferiorly. The subterminal valve is shown as competent. In this case, the grossly dilated varicose veins are the lateral accessory system. As the remainder of the GSV is often normal, the result is to return to physiological normalcy.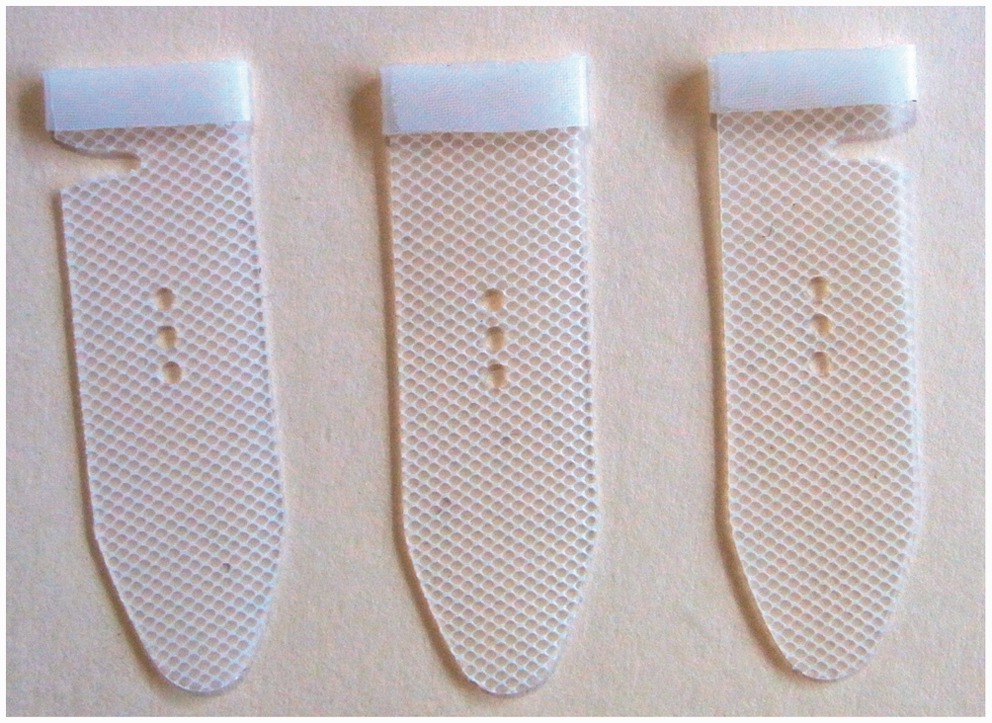
The preoperative assessment
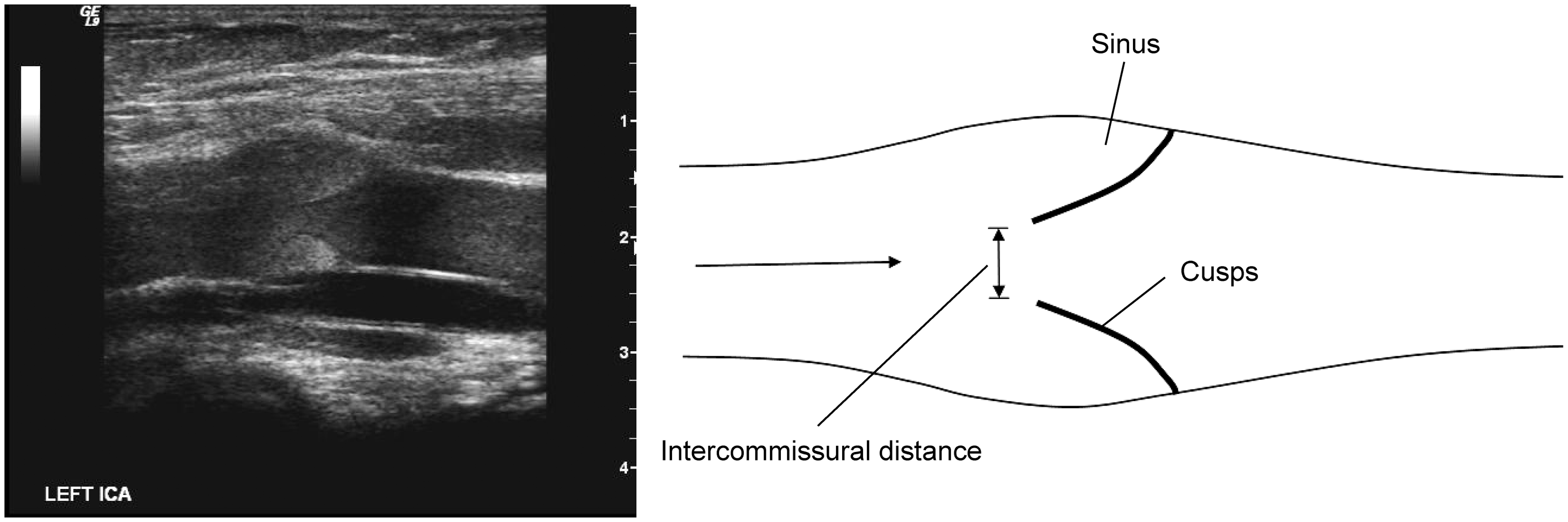
Ultrasonic assessment of the valve cusps intended for treatment is paramount. A typical sonographic worksheet is shown in Figure 4. The essential prerequisite is that there are two cusps that are present, mobile and incompetent (Figure 5). The degree of dilatation at the site of the subterminal valves is recorded. The distance from the SFJ is important to plan the site of the incision and also help recognition of the valves at operation. Ultrasound imaging delineates the degree of valve ring dilatation as well as how far the cusps are apart to estimate the degree of diameter reduction required by the external support. The contraindications of valve repair are cusp avulsion, fixation, extensive dilatation of the GSV >11 mm, excessive tortuosity of the remainder of the GSV and thrombophlebitis.
This is the ultrasonic worksheet. Important considerations are cusp, mobility and presence, and the dilatation of the valve ring. L1 is the distance of the SFJ to the terminal valve, D1 is the valve dilatation, D2 is the intervalvular diameter, L2 is the intervalvular distance and D3 is the intercommusural distance. Ultrasonic image of a typical venous valve with cusps visible but non-opposing, incompetent and mobile.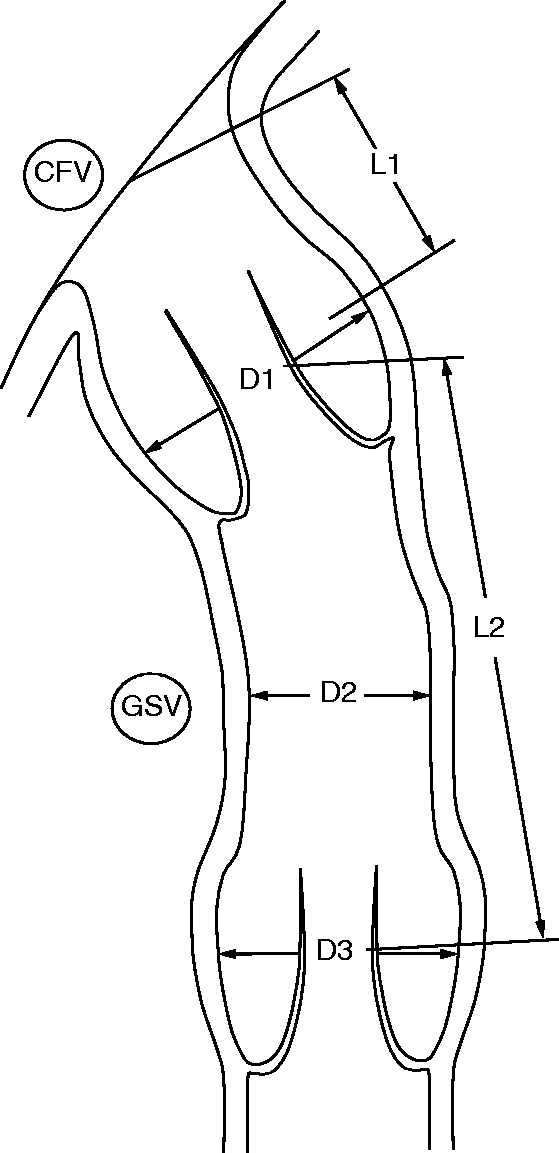
Operative method
The procedure can be performed under local or general anaesthetic depending on the concomitant proposed treatment of non-truncal veins (e.g. sclerotherapy, tributary avulsion or perforator ligation). A standard small groin incision (4 cm) is used to expose the SFJ and the tributaries of the termination of the GSV are ligated only for access of the stent. A vessiloop (Getz Bros, Chicago, IL, USA) is placed in the wound distally around the GSV. This is used to test the valve for reflux by obstructing upward flow. A right angle forceps is placed around the valve after identification. The valve insertion into the vein wall appears as a white line circumventing the SFJ (Figure 6). The tail of the Venocuff is inserted through the buckle and tightened to the appropriate diameter. The notch of the Venocuff must fit snugly between the end of the femoral vein and the inferior margin of the SFJ (Figure 3). A 5.0 prolene suture is then used to fix the vein wall to the body of the stent and the buckle. This through and through suture stabilises the diameter. The excess tail of the Venocuff is then removed. Testing is performed with valsalva if local anaesthetic is employed or in case of a general anaesthetic positive end expiratory pressure with maximum depression of the legs to induce the highest venous pressure possible. Competence is visualised when the segment between the vessiloop and the distal end of the stent remains completely flat after digital compression of the vein. An alternative test is to leave a tributary non-ligated so that blood can be seen emanating from the open vein, if incompetent. The wound is irrigated with antibiotic solution (first generation cephalosporin) and the wound closed in layers. Routine anticoagulation (heparin 2000 IV and enoxaparin 40–60 mg s.c.) and antibiotics (1 mg cefazolin) are given at the time of the procedure.
An operative photograph of the SFJ valve visible through the dilated vessel.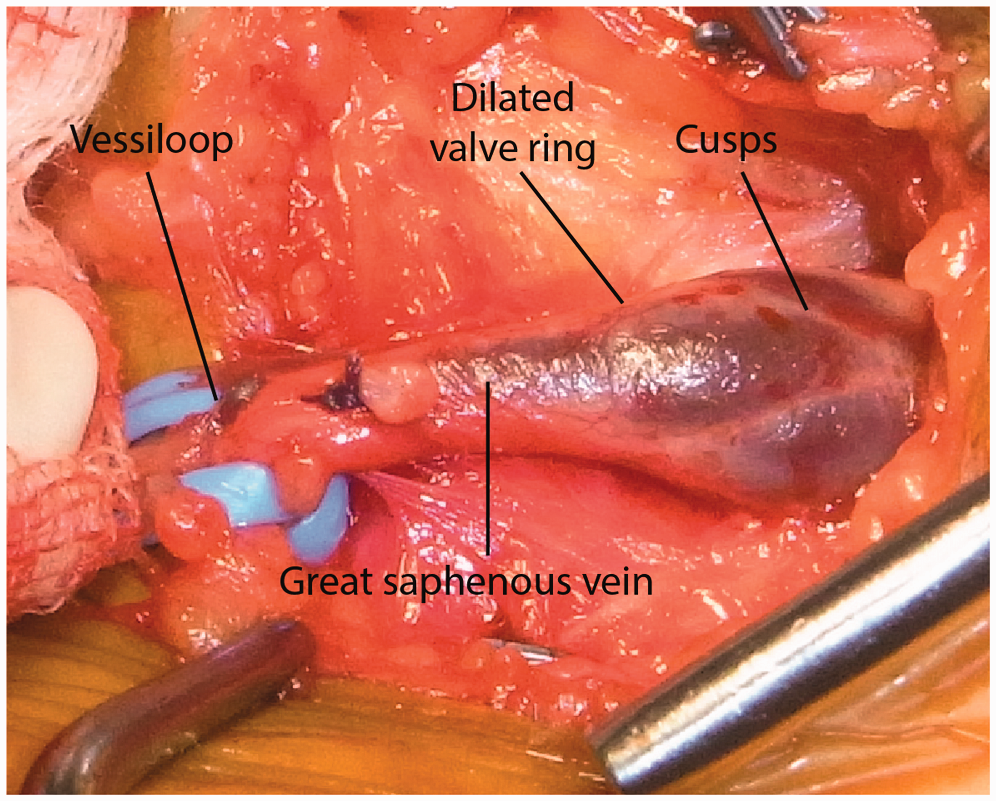
Results
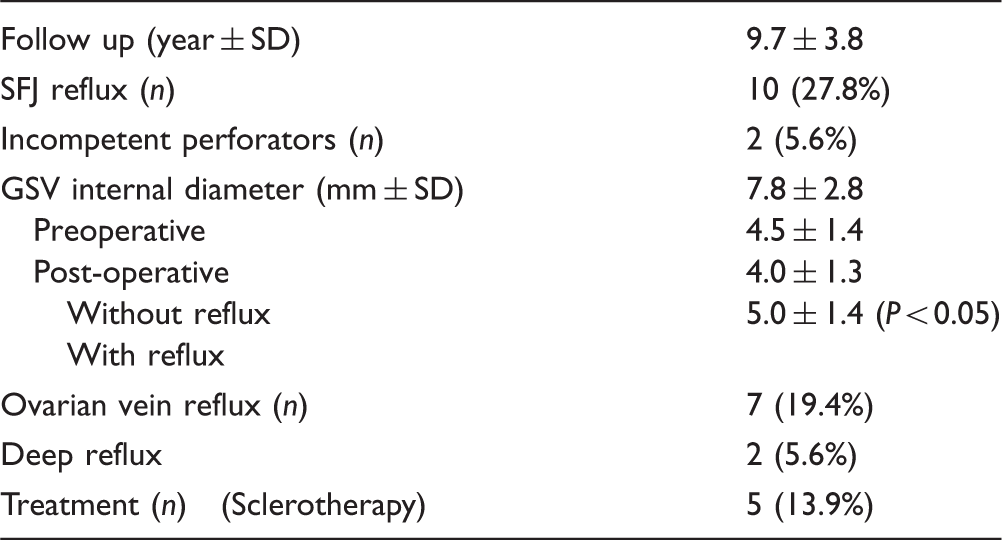
The outcomes at the short-term follow up (three months) for the pregnant group are shown in Table 3. SFJ reflux was defined by a delayed valve enclosure at the SFJ junction. The mean long-term follow up of patients in the pregnant group and control group were 9.7 ± 3.8 years and 5.7 ± 3.2 years, respectively. The recurrence rates in these two groups are summarised in Figure 7. All recurrences in the pregnant group were treated satisfactorily with ultrasound guided sclerotherapy. None have required ablation of the GSV. There were no post-operative infective or thrombotic complications. A detailed breakdown of the recurrences in the pregnant group is summarised in Table 4 and the post-operative CEAP classification is shown in Table 5. Recurrence was associated with reflux at the SFJ (P < 0.05), concomitant ovarian vein reflux (P < 0.05) and pre-existing deep venous disease (P < 0.05).
Recurrences in patients from the pregnant group and control group (*reflux at SFJ in ablated limbs not graphed due to neovascularisation). Valve repair long-term follow-up. International CEAP Classification at 9.7 years follow-up.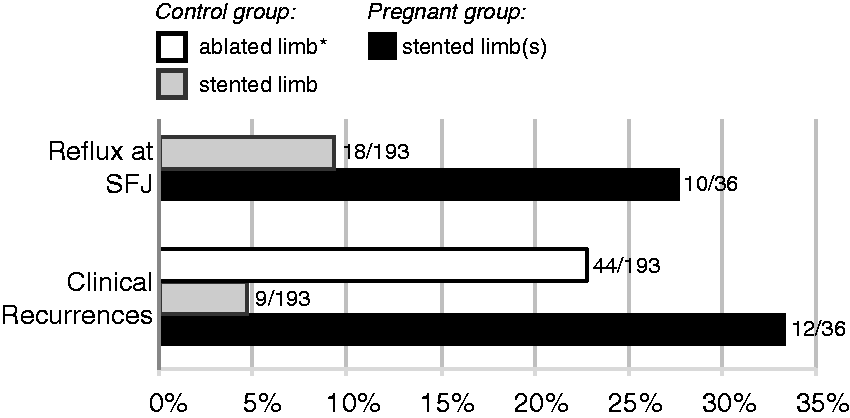
Discussion
Subsequent pregnancy is associated with an increased incidence of long-term recurrence of varicose veins compared with similarly treated non-pregnant controls (33.3% at 9.7 years versus 4.7% at 5.7 years). This trend is significant when age adjusted. Similarly, when compared with a non-pregnant control group, ablative procedures were performed where the difference was 33.3% in the pregnant group versus 22.8% in the non-pregnant group. The striking effect of pregnancy post-stenting on varicose veins is the type of recurrence following treatment. These are mainly tributaries of a mildly incompetent GSV where the truncal diameter remains significantly smaller than preoperatively; 7.8 mm versus 5.5 mm at 9.7 years post-operatively. The diameter remains 1 mm greater than the competent GSV and all of these veins could be used for bypass for arterial re-vascularisation procedures if required in the future. Most importantly, further treatment is primarily tributary sclerotherapy in a mildly dilated truncal trunk rather than further expensive ablative procedures. The etiology of recurrences is multifactorial with 19.4% being associated with new ovarian vein reflux, 5.6% deep disease (femoral vein incompetence) and 27.8% reflux at the SFJ. These factors often occurred in combination, compounding each other.
Women of child bearing age present at a younger age (30 ± 4.7 years) compared to the general population (45 years) 2 as valve deterioration is a function of age and the valve cusps are often preserved. 13 The reparative physiological approach is theoretically optimal in young patients contemplating or in between pregnancies. The results suggest that the often quoted dictum ‘that repair of varicose veins should be left until after all pregnancies have been completed’ is essentially incorrect.1,4 Valve repairs are almost always possible with a reduction in the risk of subsequent clinically significant varicose veins. A patient with varicose veins intending to have further pregnancies should be actively treated to reduce morbidity in the future. The varices predating pregnancy are often exacerbated by further pregnancies.
In this study, venous valve repair resulted in a relative absence of symptoms at 10 years 31CSymptomatic versus 6CSymptomatic, pre and post-operative, respectively. The motivation for presentation with recurrence for these patients is cosmesis.
Pregnancy is associated with progression of varicose veins and it is occasionally impossible for valve repairs to be performed and an ablative procedure is the only alternative. A prospective controlled trial of patients with earlier disease who had cusp preservation showed long-term results at least as good as the ablative procedure.12,14
Mechanism of recurrence in pregnancy
As the implanted stents incur a fixed diameter to the SFJ (4–5 mm) and the cusps are normal preoperatively, the development of new reflux at the SFJ is logically related to new cusp degeneration. Unfortunately, post-operative ultrasound cannot define cusp morphology related to the inability of ultrasound to penetrate the stent itself. The preoperative association with deep reflux and new ovarian vein reflux suggests the underlying problem is in the matrix of the cusp itself5,13 aggravated by the increased volume flow associated with pregnancy and the circular reflux pattern set up with ovarian vein incompetence and deep vein reflux.
Ovarian vein incompetence may produce a different mechanism of recurrence.15,16 The labial and paravaginal perforators connect to the distal GSV creating a functional bypass to the valve repairs. If patients are wishing to proceed with further pregnancies, the strong association with new reflux suggests that ovarian vein embolisation should be considered. Specifically, both SFJ incompetence and ovarian vein incompetence should be treated to avoid these etiological factors compounding each other.
The natural history of varicose veins in pregnancy indicates inevitable deterioration and therefore earlier intervention is logically a better approach. Up to 20% of varicose veins develop during pregnancy.16−19 Mullane showed an increasing severity with progressive numbers of pregnancies; 13% primiparous, 30% secundiparous and 57% multiparous. 20
The advantages of exostent repair
As the GSV is preserved, there is very little post-operative discomfort compared with ablative procedures. The repair is physiological and minimises collateral stimulation and preserves the normal conduit in patients with concomitant deep disease. The long-term results are satisfactory. 9 The procedure is quick, can be performed under local anaesthetic and is inexpensive. Valve repair, however, is selective and requires mobile cusps with the prime pathology being dilatation of the valve ring.
Conclusion
Although stent repairs have shown to be better than conventional ablative procedures, pregnancy remains a major contributing factor to recurrences. However, the underlying etiology, distribution and vein type in these recurring cases are different from standard varicose veins and in general require a less aggressive remedy. Stent repairs to the SFJ and or sub-terminal valve produce a durable alternative for women contemplating initial or further pregnancies. The reparative physiological approach is a reflection of earlier age and hence cusp preservation in pre-pregnant females compared to the normal population. This approach is contrary to the usual dictum that treatment of varicose veins should be delayed until the family is completed.