
Abstract
Massive perivillous fibrinoid deposition is a rare placental pathology associated with significant adverse pregnancy outcome and can recur. We provide a detailed case review of a woman through 10 of her pregnancies, including 8 consecutive pregnancy losses and 2 live births. We also conducted a retrospective chart review of all massive perivillous fibrinoid deposition placenta specimens at our institution over an eight-year period. A total of 42 cases of massive perivillous fibrinoid deposition were identified from 2007 to 2015, yielding an incidence of 0.16%. Recurrence was seen in subsequent pregnancy in eight out of nine (88.9%) cases with more than one specimen. The clinical characteristics, perinatal outcomes and α-feto protein level of the 42 cases are presented. Also, presented is a review of the literature discussing placental pathology, pathogenetic mechanisms and management of this condition.
Introduction
Placental pathology offers insight into intrauterine experience, including both acute and chronic events. Histopathologic examination of the placenta has been increasingly recognized and accepted as an important clinical tool that can provide clues about in utero insults and help guide the management of both newborn and subsequent pregnancies. 1 Placental pathology is also gaining interest as a predictor of future maternal and neonatal health, i.e. the development of chronic disease later in life. Despite these well-known advantages of placental pathologic examination, this mode of investigation remains underutilized in perinatal medicine.
Certain pathologies that can recur in subsequent pregnancies, deserve particular attention as they may affect pregnancy management. Massive perivillous fibrin/fibrinoid deposition (MPFD) is a rare placental pathology, characterized by excessive perivillous deposition of fibrinoid material, with unclear aetiopathogenesis. It is associated with high perinatal morbidity, mortality, and can recur in subsequent pregnancies. 2
Our study aims to share a multidisciplinary experience at a single institute and provide updates on clinical association and management of MPFD. We present the detailed history of a case of this rare placental condition, followed by a retrospective review of cases of MPFD at our institution over the past eight years.
Methods
This was a single-institute retrospective study based on chart review. Our hospital is a tertiary care center for pregnant women and more than 80% of the deliveries in the state take place in our hospital. Placental pathology reports are completed by board-certified pathologists in Pediatric Pathology in the Perinatal Division following standard protocol. 3 Weekly audit is performed for 10% of the cases.
With approval from the Institutional Review Board (IRB No. 14-0067), placenta reports with diagnosis of “massive perivillous fibrin/fibrinoid deposition (MPFD)” were searched in Hospital Information System from 2007 to January 2015. The diagnosis of “Massive perivillous fibrin/fibrinoid deposition” was made when “perivillous fibrinoid material extending from the maternal surface to fetal surface, encasing ≥ 50% of the villi on at least one slide.” 3 From the identified specimens, selected placental gross and microscopic findings, gestational age (GA) at delivery, maternal laboratory testing results, prenatal testing results, birth weight, Apgar scores at 1 and 5 min, and adverse pregnancy outcomes including intrauterine growth restriction (IUGR) and intrauterine fetal demise (IUFD) were collected as data. The placental weight percentile by gestational age was also collected, with small-for-gestational age defined as weighing less than the 10th percentile.
Results
We describe below a clinical case study of a patient with MPFD and follow with the summary of a series of cases along with a review of the literature of this interesting placental pathology.
Case 1
A 27-year-old gravida 4 para 0 at 16 weeks’ gestation presented to the obstetric medicine clinic for ongoing management of anticoagulation in her pregnancy. She had been seen at the Reproductive Endocrinology clinic at our facility after three consecutive first trimester losses. A comprehensive work-up for various causes of recurrent miscarriage, including anatomical causes was negative. During the course of these investigations, she was noted to be homozygous for the MTHFR gene mutation and also reported a family history of venous thromboembolism. Her maternal grandmother had several deep vein thromboses (DVT) and multiple miscarriages. Several other family members were reported as having three or more miscarriages.
After establishment of her care at our institution, the patient had another five pregnancy losses. Karyotyping results for products of conception (POCs) #6–8 were normal. Following the 3rd loss, she started low dose aspirin (81 mg daily). A folic acid supplement was started after the 4th loss. Low-molecular weight Heparin (LMWH), enoxaparin, was started during the 7th pregnancy and given in all subsequent pregnancies.
In the 9th pregnancy, at 27 weeks’ gestation, the fetus was found to have severe intrauterine growth restriction (IUGR). The umbilical arterial Doppler showed persistent elevation of the systolic/diastolic (S/D) ratio, intermittent absent end diastolic flow (AEDF), and waveforms suggesting increased placental resistance and placental dysfunction. A cesarean section was performed at 31 weeks secondary to intermittent variable fetal heart rate decelerations and breech presentation. The birth weight was between 3 and 10th percentile, the placental weight was between 75 and 90th percentile, and the feto-to-placental (F/P) weight ratio was 2.75 (<3rd percentile).
Pathological examination of the placenta of the 9th pregnancy was consistent with MPFD. This included full-thickness “orange rind” appearance in cross sections (Figure 1(a)). Microscopically, in 10% of the parenchyma, hypermature but relatively normal chorionic villi (accelerated maturation) were seen. The remaining 90% of the parenchyma showed villi encased in diffuse fibrinoid material, with a prominent proliferation of extravillous trophoblast (EVT). There were multiple foci of chronic villitis (Figure 1(b)).
Gross and microscopic pathology of the uterine evacuation specimen and placentas from the case. (a) Placenta of the 9th pregnancy, representative cross section. (b) Placenta of the 9th pregnancy, H&E, 40×, showing diffuse perivillous fibrinoid deposition with extravillous trophoblastic (EVT) proliferation. (c) Evacuation specimen of the 7th loss, H&E, 40×, showing extensive perivillous fibrinoid deposition. (d) POC of the 8th loss, H&E, 200×, showing extensive perivillous fibrinoid deposition. (e) Placenta of the 10th pregnancy, representative cross section. (f) Placenta of the 10th pregnancy, H&E, 100×. On the left, chorionic villi with morphology consistent with the gestational age of 35 weeks; on the right, placental septa showing proliferation of EVT.
Placental specimens from this patient’s prior losses were retrieved from the Pathology archives and reexamined. Pathological examination of POCs #6–8 revealed viable immature chorionic villi embedded in perivillous fibrinoid material (Figure 1(c) and (d)). It is important to note that MPFD may not be correctly identified in POC where only a fragment rather than the whole placenta is submitted.
Clinical characteristics and pathological features of the pregnancy history of Case 1.
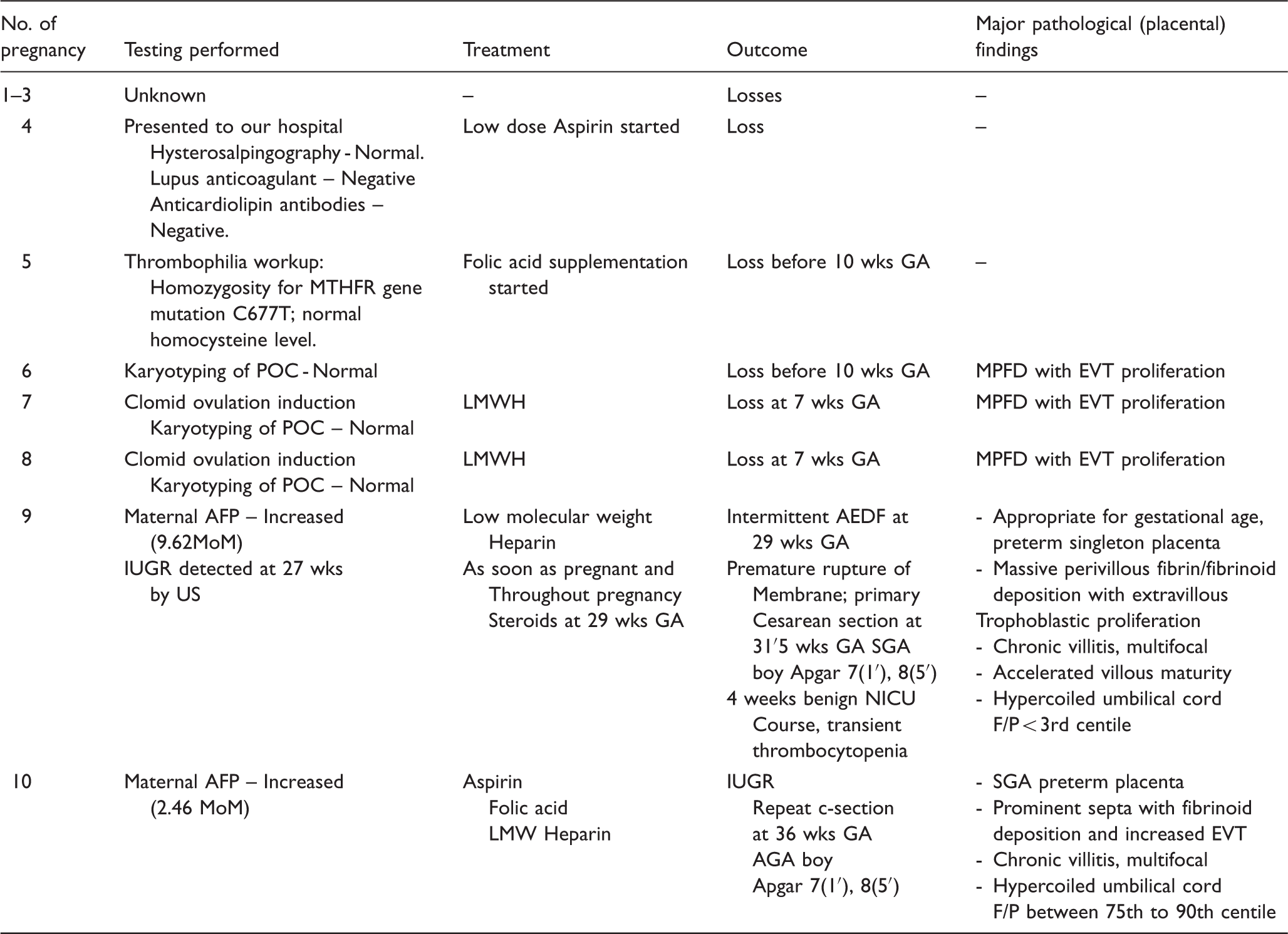
AEDF: absent end diastolic flow; AFP: alpha fetoprotein; AGA: appropriate for gestational age; EVT: extravillous trophopblast ; F/P: feto-placental weight ratio; GA: Gestational age; LMWH: low-molecular weight heparin; MoM: multiple of medium; MPFD: massive perivillous fibrinoid deposition; MTHFR: methylene tetrahydrofolate reductase; NICU: neonatal intensive care; POC: products of conception; SGA: small for gestational age.
Case series
Clinicopathologic features among MPFD/MFI placentas (n = 42) with clinical outcomes of IUFD, neonatal death, IUGR or neither.
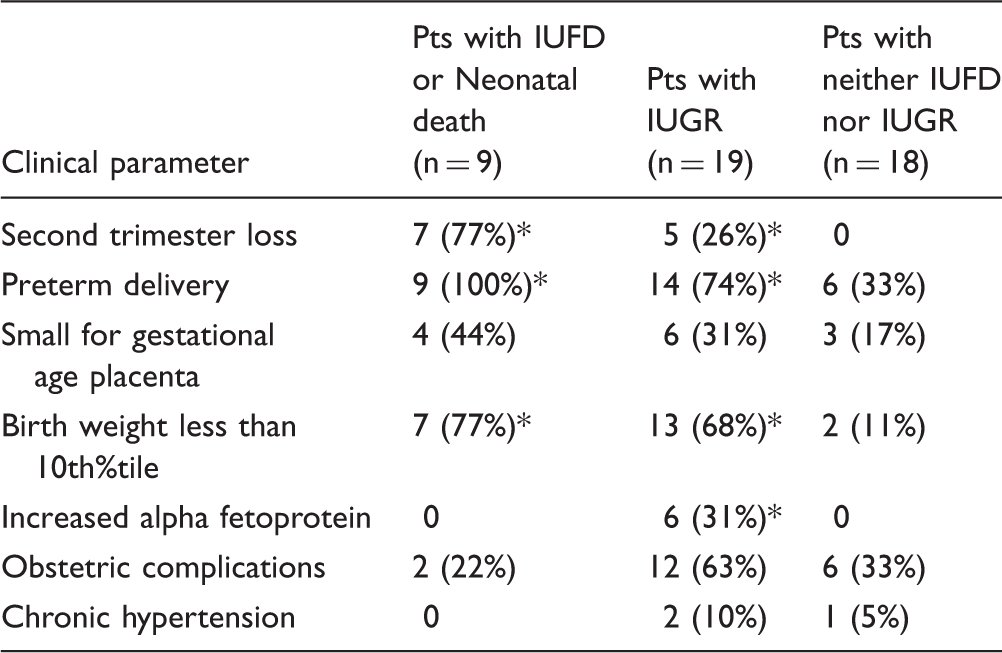
Note: Compared to the group with neither IUFD nor IUGR, *P < 0.05.
Obstetric complications: Acute fatty liver of pregnancy, gestational diabetes, gestational hypertension and preeclampsia, pregnancy-induced hypertension.
IGUR: intrauterine growth restriction; IUFD: intrauterine fetal demise; MPFD: massive perivillous fibrinoid deposition
Among these 42 cases, nine patients had more than one placenta or POC specimen submitted to Pathology. Review of the reports demonstrated increased perivillous fibrin/fibrinoid deposition in more than one placenta/POC for eight of these patients (8/9, 88.9%), confirming the recurrent nature of this pathology.
Table 2 summarizes clinicopathological correlations within the cases from our institute. Among the 42 cases, gestational age at delivery ranged from 17 to 41 weeks. There were 9 cases of IUFD or neonatal death (21.4%), 19 cases of IUGR (45.2%), and 25 cases of preterm birth (60%) including 12 pregnancies ending during the 2nd trimester (28.6%).
Eleven (11/42, 26.2%) cases had SGA placentas and seven (16.7%) had LGA ones. Eighteen (18/42, 42.9%) cases were associated with birth weight < 10th percentile but only one with birth weight >90th percentile. For 38 cases with available F/P weight ratios, 18 (47.3%) had F/P ratios < 10th percentile, suggestive of placental insufficiency. This result suggests that placental insufficiency is a common theme in placentas with MPFD.
When comparing the cases associated with IUFD or neonatal death (n = 9) to the ones without IUFD or IUGR (n = 18), those with IUFD were associated with preterm delivery (9/9 vs. 6/18, P < 0.001), usually ending in the 2nd trimester (7/9 vs. 0/18, P < 0.0001). Most of the IUFD cases (7/9, 77.8%) were also associated with SGA fetuses. Increased AFP was noted in a significant number of cases associated with IUGR (6/19 vs. 0/18, P = 0.012).
In summary, pregnancies complicated by MPFD in our institution were associated with significant adverse outcomes, likely secondary to placental insufficiency.
Discussion
Definition, incidence and pathology
MPFD and “maternal floor infarction” (MFI) are related idiopathic placenta disorders. MFI is more frequently used clinically, while MPFD is preferred by pathologists. MFI was originally described by Benirschke and Driscoll in 1967, while MPFD was first reported by Fox in 1976. The terms are often used interchangeably in the literature. While MFI has been used frequently, it is a misnomer since the nature of pathology is not infarct, rather intervillous fibrinoid deposition. The incidence of MPFD/MFI is reported to be from 0.028% to 0.5% with a reported recurrence rate of 30% or more. 2
MPFD/MFI has characteristic gross and microscopic morphologies, as reflected in our case. Placental cross sections may either present a diffuse yellow, firm (“orange rind” appearance) parenchyma or a lesion more concentrated around the basal plate (maternal floor) with histologic features of massive fibrin/fibrinoid deposition with extravillous trophoblast (EVT) proliferation and chorionic villi encased in a netlike pattern. The engulfed villi are abnormal, showing villous fibrosis and karyorrhexis. Intervening villi are relatively normal. Chronic nonspecific villitis, as noted in this case, can be seen occasionally. The fibrinoid material in the intervillous space obstructs maternal blood flow and interferes with oxygen and nutrient supply through the maternal-fetal interface, resulting in reduced placental efficiency, as exemplified by the placenta from the 9th pregnancy, which had an F/P ratio of < 3rd percentile. The F/P ratio is often used as a marker of placental efficiency. An F/P ratio of < 10th percentile is suggestive of placental insufficiency. Fibrinoid deposition in the placenta may be detected by prenatal ultrasound as increased echogenicity, but the finding is not specific for this lesion.5,6 Prenatal ultrasound may also reveal evidence of increased placental resistance and dysfunction as in our patient. 7
The histological differential diagnosis of MPFD usually includes intervillous thrombi (IVT), parenchymal infarct, and chronic non-specific villitis (villitis of unknown etiology (VUE)). Intervillous thrombi are usually focal or multifocal, but MPFD/MFI is diffuse in nature. In IVT, the material in the intervillous space is fibrin which has a layered appearance. In placental infarct, there is a collapse of intervillous space and a loss of distinct nuclear basophilia at later stages. Intervillous thrombi are considered suggestive of feto-placental hemorrhage, while parenchymal infarct is regarded as a feature related to uteroplacental malperfusion often seen in gestational hypertensive disorders.
Etiology and pathogenesis
The etiologies and pathogenic mechanisms of MPFD/MFI are not clear yet. Since the characteristic fibrinoid material consists of fibrin and other proteins such as products from the coagulation cascade, 2 most proposed mechanisms and explanations of etiology have therefore focused on maternal thrombophilia or autoimmune illnesses such as lupus anticoagulant. 8 Possible involvement of a defect in the trophoblastic protein C system has also been suggested in the pathogenesis of MPFD. 9 Our patient underwent a thrombophilia screen as was indicated by her recurrent miscarriages and a family history of thrombosis. Lupus anticoagulant testing was negative. She tested positive for a homozygous MTHFR mutation but with normal homocysteine levels. While there is an association between inherited thrombophilias and venous thromboembolism during pregnancy, there is no established link between inherited thrombophilias and uteroplacental thrombosis. In particular, MTHFR mutations are not considered to confer an increased thrombotic risk in pregnant women. 10
Autoimmune processes are considered possible etiologies for MPFD/MFI. Recently, Romero et al. 11 proposed that maternal anti-fetal rejection occurs in a subset of MPFD/MFI cases by demonstrating that MPFD placentas had a significantly higher frequency of plasma cell deciduitis and C4d deposition in the umbilical vein. MPFD cases exhibited substantially higher maternal anti-HLA class I sero-positivity, maternal antibodies against fetal HLA I and II antigens, and mean maternal plasma concentrations of CXCL-10.
Another proposed mechanism is the imbalance of angiogenic/anti-angiogenic factors, such as higher plasma concentrations of soluble vascular endothelial growth factor receptor (sVEGFR) and lower concentrations of placental growth factor (PlGF). 12 One study on perinatal autopsies associated with MPFD revealed the co-occurrence of recurrent renal tubular dysgenesis (RTD) in three consecutive pregnancies in one woman with MPFD, and a causal relationship was proposed. 13 This study shed light on the feto-placental unit as a whole in the pathogenesis of MPFD. MPFD has also been reported in association with Coxsackie virus infection and hypercoiling of a single-artery cord.14,15
Clinico-pathological correlation of MPFD/MFI
MPFD/MFI is known to be associated with intrauterine fetal death (13–50%), IUGR (24–100%) and preterm delivery (26–60%). 5 IUGR is noted early in the third trimester. Adverse neurodevelopmental outcome was also found to be a complication. 6
Neurodevelopmental outcome was not investigated in current study.
Is MPFD treatable?
Despite the lack of a clear understanding of the etiology of MPFD, different treatment strategies have been attempted. 16 There are reports of successful management of recurrent fetal loss due to MPFD/MFI using LMWH and immunoglobulin to address the potential thromboembolic and autoimmune etiologies, respectively.17,18 LMWH is often combined with low-dose aspirin. Makino et al. 17 reported a case of MPFD/MFI in which the use of oral low-dose aspirin and LMWH during subsequent pregnancy was associated with a reduction in the degree of perivillous fibrinoid deposition, similar to what was seen in our case. 17 In other studies, the benefit of LMWH has been noted to be independent of the presence of inherited thrombophilias or the concurrent administration of low dose aspirin. The beneficial functions of LMWH may include anti-inflammatory activity, trophoblast differentiation and invasion, angiogenesis, or reduction of vascular resistance. 19
Based on the previous report on the imbalance of angiogenic and anti-angiogenic factors, 12 another study reported the use of pravastatin to treat a patient with recurrent pregnancy losses, resulting in a live birth at 34 weeks. 20
Conclusion
In conclusion, our case is an example of recurrent pregnancy loss in eight consecutive pregnancies, with the same pathology identified in all four available consecutive specimens, and a disappearance of this pathology in the last successful pregnancy after clinical intervention.
Albeit rare, MPFD is a recurring pathology with significant adverse outcomes in pregnancy including recurrent loss, IUGR, and IUFD. In patient with such clinical scenarios, placental exam should definitely be performed and the identification of MPFD/MFI and other recurring pathologies should alert the pregnancy management team to the risk of recurrent complications in subsequent pregnancies. Closer monitoring should be provided, and other treatment options considered. The disappearance of the recurrent pathology in this patient’s 10th pregnancy with the use of LMWH is encouraging. However, more studies are necessary to investigate the benefits of LMWH in patients with recurrent pregnancy loss due to MPFD/MFI and related pathologies.
The adverse neurodevelopmental outcome associated with MPFD/MFI 5 suggests that, for children born with severe placental pathology, long-term follow-up should be provided, even if there are no significant problems during the perinatal and neonatal period.
Footnotes
Acknowledgement
This case report was included briefly in the following. Al-Khan JN, Bulmer FC, et al. IFPA Meeting 2012 workshop report III: trophoblast deportation, gestational trophoblastic disease, placental insufficiency and fetal growth restriction, trophoblast over-invasion and accreta-related pathologies, placental thrombosis and fibrinolysis. Placenta (34 Supplement): S11–S16.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Institutional Review Board (IRB No. 14-0067) at Women and Infants hospital as a retrospective chart review with waiver of patient consent.
Guarantor
MH.
Contributorship
Mai He is also the guaranteeing author and confirms the manuscript’s accuracy and the contributorship of all co-authors.