
Abstract
Risk assessment for venous thromboembolism in pregnancy and the puerperium is currently limited to stratifying clinical surrogate risk factors without high-quality evidence. While the absolute risk of pregnancy-associated venous thromboembolism is low for the vast majority of women, associated morbidity and mortality remains significant. As guidelines for thromboprophylaxis vary widely, some women may be under- or over-anticoagulated, contributing to poor outcomes. New global coagulation assays provide a holistic view of coagulation and may have the potential to detect hypercoagulability in pregnancy, unlike clinically available coagulation assays. However, there are major technical challenges to overcome before global coagulation assays can be realistically proposed as an adjunct to risk assessment for pregnancy-associated venous thromboembolism. This review summarises the literature and controversies in the prediction and prevention of pregnancy-associated venous thromboembolism and outlines the new tools in haematology that may assist in our future understanding of hypercoagulability in pregnancy.
Introduction
Venous thromboembolism (VTE) is a leading cause of maternal morbidity and mortality. In Australia between 2008 and 2017, VTE accounted for 20.5% of all direct maternal deaths. 1 One of the key strategies in managing VTE risk in pregnant women is the use of low molecular weight heparin (LMWH), with a recommendation for up to 85% of women to receive postpartum prophylaxis after Caesarean section in some clinical guidelines. 2 This is despite a Cochrane review concluding there is insufficient data from randomised controlled trials to guide its use in this population. 3 Its liberal use under certain guidelines has generated some controversy, given the relative low risk of VTE (2870 per 100,000 person-years in 12 postpartum weeks) 4 and the real, albeit small, bleeding risk associated with the use of LMWH (estimated to be 0.0–0.3%). 5 Hence, there remains a need to further refine our risk assessment strategies to balance the numbers needed to treat and to harm in this setting. 4 While progress in risk prediction using clinical surrogate measures has been made, there remains significant variation in prophylactic management guidelines globally.2,6,7 Importantly, a lack of reliable laboratory assays to refine our risk assessment models has limited our ability to balance bleeding and thrombotic risk.
Although it has been well established that pregnancy generates a physiologically hypercoagulable state, current routine coagulation tests (activated prothrombin time (APTT) and prothrombin time (PT)), which only measure time to start of clot formation, are limited in their ability to detect hypercoagulable changes and cannot accurately assess VTE risk. Global coagulation assays (GCAs) such as thromboelastography, thrombin and fibrin generation, on the other hand, measure the characteristics of total clot formation as well as end-products of the coagulation cascade, and may be more representative of the coagulation process. 8 Changes in the elastic properties of whole blood during clot formation, propagation and dissolution can be measured with thromboelastography (TEG) and rotational thromboelastometry (ROTEM). Thrombin is a key protein in the coagulation process, previously shown to predict non-pregnant women at increased risk of VTE recurrence 9 and thrombin generation can be measured using the calibrated automated thrombogram (CAT). Fibrinolysis is less well studied but previous small studies have observed that hypercoagulable women have impaired fibrinolysis 10 as measured using the overall haemostatic potential assay (OHP). By providing a more comprehensive assessment of the haemostatic profile, GCAs may have the potential to adjunctively assess VTE risk and therefore guide individualised thromboprophylaxis. 11
This review briefly reviews current risk stratification strategies in pregnancy and the potential role for global coagulation assays as adjunct tools for VTE risk stratification.
Literature search strategy
A medical literature search was conducted in MEDLINE (Ovid) for studies evaluating the use of GCAs in pregnancy and the puerperium published in English between 1997 and 2019. Search terms included ‘pregnancy,’ ‘postpartum,’ ‘thromboelastography,’ ‘rotational thromboelastometry,’ ‘calibrated automated thrombogram,’ ‘thrombin generation assay’ and ‘overall haemostatic potential.’ Relevant supporting references cited within the results obtained were included.
Physiological changes to coagulation in pregnancy and the puerperium
Physiological changes during pregnancy and postpartum are well described and significantly impact the coagulation system. All three arms of Virchow’s triad are implicated in the tendency to clot during this time: hypercoagulability, endothelial damage and stasis. Procoagulant activity increases during pregnancy, notably through the elevation of factors VII, VIII, X, fibrinogen and von Willebrand factor.12,13 In addition, physiological anticoagulants such as protein S decrease during pregnancy and a resistance to activated protein C is acquired.12,13 Fibrinolysis becomes increasingly impaired throughout gestation but returns to normal shortly after delivery. 14 Endothelial damage occurs intrapartum, in particular to the uterine and pelvic blood vessels. 15 Venous stasis occurs in pregnancy due to a combination of decreased mobility and reduced venous return from the lower limbs due to the mechanical obstruction of the inferior vena cava and pelvic veins by the gravid uterus.3,15 These coagulation changes in combination contribute to a prothrombotic state during pregnancy, which is thought to be highest postpartum and resolves approximately 4–6 weeks after delivery.16,17
Current VTE risk stratification and prevention in pregnancy
While VTE in pregnancy is relatively rare, it remains an important cause of maternal morbidity and mortality and a major clinical focus during the peripartum period. The absolute risk of VTE is estimated around 1–2 in 1000 pregnancies,18–20 manifesting as deep vein thrombosis in 80% of cases. 20 There is a 4- to 5-fold increased thrombotic risk during pregnancy18,21 and this risk increases up to 22-fold in the puerperium. 22 There are a number of clinical risk factors, however, which further increase this physiological risk.
The strongest additional risk factors include a history of thrombosis (odds ratio (OR) 24.8, 95% confidence interval (CI) 17.1–36.0) and antiphospholipid syndrome (OR 15.8, 95% CI 10.9–22.8). 19 Heritable thrombophilias may also increase VTE risk; however, the magnitude of risk varies by the type of defect present. Obesity and maternal age are also significant contributors to pregnancy-associated VTE risk. Observational studies have estimated the odds ratio for antenatal and postpartum thromboembolism in obese pregnant women to be 3.6–4.4 (95% CI 2.9–4.6 and 3.4–5.7 respectively),19,23 which is particularly relevant given its increasing prevalence, with up to 20% of Australian women obese (body mass index (BMI) ≥30 kg/m2) at their first antenatal visit. 24 Given VTE is also associated with significant morbidities including post-thrombotic syndrome and venous insufficiency, 25 one of our key clinical challenges remains to prevent VTE during pregnancy.
Current methods of estimating risk of VTE in women before, during and after pregnancy are based on clinical risk factor stratification guidelines derived from case-control studies. The recently published 2018 guidelines from the American Society of Haematology provide some thorough recommendations about thromboprophylaxis in pregnant women with hereditary thrombophilia. 26 However, there remains no consensus in the guidelines and Table 1 provides clinical vignettes highlighting the differences in current major guidelines. These discrepancies were further demonstrated in a cross-sectional study reviewing 293 women undergoing Caesarean delivery in a UK tertiary hospital 2 where the proportion of women recommended for anticoagulation significantly varied based on different guidelines with 85%, 34% and 1% of women recommended for LMWH prophylaxis under Royal College of Obstetricians & Gynaecologists guidelines, 7 2012 American College of Chest Physicians guidelines27,28 and the 2011 American Congress of Obstetricians and Gynaecologists guidelines respectively. 29 The heterogeneity in VTE guidelines is further highlighted by the National Health and Medical Research Council guidelines for prevention of VTE in Australian hospitals, which do not provide definitive guidance on maternal thromboprophylaxis and suggest the use of clinical judgement. 30
Example clinical vignettes highlighting subtle differences in recommendations for low molecular weight heparin in major venous thromboembolism prevention guidelines.
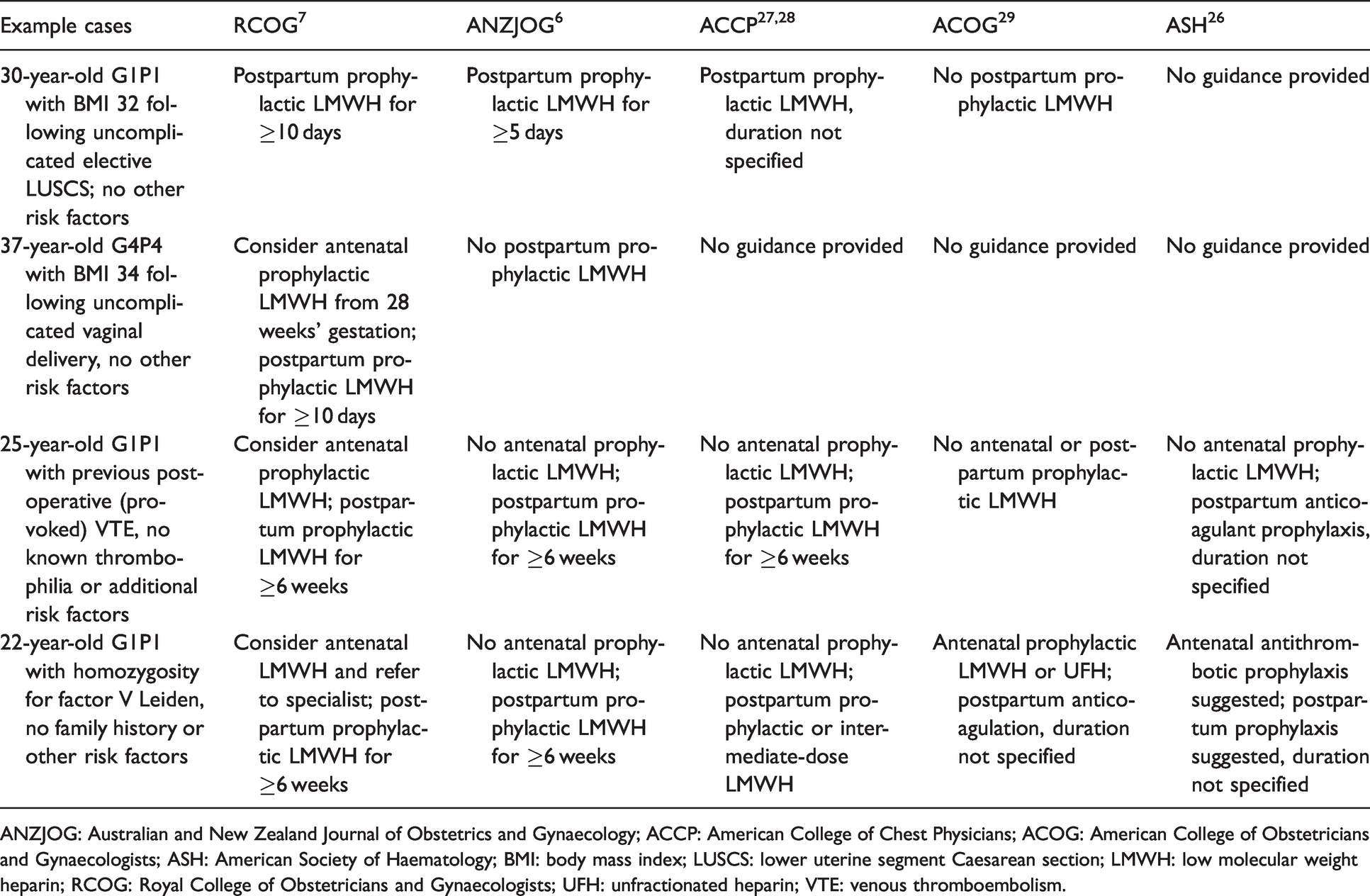
ANZJOG: Australian and New Zealand Journal of Obstetrics and Gynaecology; ACCP: American College of Chest Physicians; ACOG: American College of Obstetricians and Gynaecologists; ASH: American Society of Haematology; BMI: body mass index; LUSCS: lower uterine segment Caesarean section; LMWH: low molecular weight heparin; RCOG: Royal College of Obstetricians and Gynaecologists; UFH: unfractionated heparin; VTE: venous thromboembolism.
Furthermore, a Cochrane review has suggested there remains a lack of high-quality evidence used to guide practice, leading women to be overtreated under some guidelines and undertreated with others. 3 The review called for large-scale randomised controlled trials to evaluate postpartum LMWH prophylaxis, particularly where the overall effect of LMWH is unclear in women with common risk factors such as increased parity, age and BMI.2,4 These discrepancies amongst the VTE guidelines highlight the need for further risk tools to refine our risk stratification strategies. Some studies have developed risk score and prediction models using consensus opinions or absolute risks determined from large population studies.31,32 Additional risk tools could be better laboratory coagulation parameters which have been shown in some other conditions to predict higher risk populations. Hence, we explore these assays in greater detail in this review.
Traditional coagulation assays and their limitations in VTE risk assessment
Traditional coagulation assays such as APTT and PT were initially developed to monitor anticoagulant therapy rather than bleeding or clotting risks. These tests measure the time to the start of blood clot formation and do not reflect the complexity of dynamic in vivo haemostasis. APTT and PT are generally unchanged during pregnancy, hence they fail to reflect known hypercoagulability in pregnancy.33,34
The utility of other biomarkers of coagulation activation such as D-dimer have been investigated in pregnancy, with limited success. D-dimer, a fibrin degradation product used to rule out VTE in the non-pregnant population, is increased in pregnancy with longitudinal studies revealing that 98–100% of women have levels above the non-pregnant reference range at 34–36 weeks’ gestation.35,36 While D-dimer may have a role in guiding investigation of pregnant women in whom acute pulmonary embolism is suspected, as per the pregnancy-adapted YEARS algorithm, 37 it does not offer value in general VTE risk assessment in pregnancy. 38
Principles of global coagulation assays, current knowledge and potential role in obstetrics
The GCAs refer to a new generation of haematological assays that include viscoelastic testing with TEG and ROTEM, thrombin generation assay measured with CAT and fibrin generation assay using the OHP assay. GCAs provide a more holistic overview of coagulation including clot initiation, propagation, total clot formation and fibrinolysis compared to traditional coagulation assays. This section will discuss the different types of global coagulation assays, the current research applications in other fields and their potential role in the field of obstetrics.
Viscoelastic testing – thromboelastography and rotational thromboelastometry
TEG analyses the viscoelastic properties of whole blood during clot formation, propagation and dissolution. 39 Two common commercially available viscoelastic testing devices are TEG® (Haemonetics, USA) and ROTEM® (Haemoview Diagnostics, Australia). The principles of both devices are relatively similar and assess blood clot formation by measuring changes in torsion around a pin and cup as a clot is formed and subsequently lysed (Figure 1). Assay parameters provide information on the time to clot onset (R-time), time to achieve a certain clot strength (K-time), rate of clot formation (alpha-angle), maximum clot strength (maximum amplitude) and a measure of fibrinolysis (lysis 30). Specific activators allow evaluation of the extrinsic and intrinsic coagulation systems (e.g. EXTEM and INTEM for ROTEM respectively), as well as the contribution of fibrinogen to coagulation (FIBTEM).

(a) Principles of thromboelastography and (b) thromboelastometry. Reproduced with permission from Lim et al. 8
The main clinical utility of TEG currently is to guide transfusion support in trauma, cardiac surgery and massive transfusion situations, including obstetric haemorrhage. 39 Several studies including meta-analysis have shown that viscoelastic tests have led to reduction in transfusion of blood components, particularly with fresh frozen plasma and platelets with possible reduction in red blood cell products as well.40–42 Some studies have demonstrated that TEG-guided approach improves key patient outcomes including length of stay, bleeding rate and mortality. 42
However, the clinical utility of viscoelastic testing in the field of thrombosis remains under investigation. A prospective observational study demonstrated that patients with ischaemic strokes with higher maximum amplitude suffered from more severe strokes and poorer functional outcome (OR 1.92, p = 0.022). 43 Similarly, in a study of 313 non-cardiac non-obstetric major surgeries, pre-operative ROTEM assays detected hypercoagulability in the ten cases where a postoperative thromboembolic event occurred. 44 In addition, we have previously published that TEG is sensitive enough to detect hypercoagulability in some subsets of patients including in older healthy controls, 45 patients with plasma cell dyscrasia, 46 transgender women on oestrogen therapy 47 and patients with cardiovascular risk factors. 48 Further studies are ongoing to evaluate the role of TEG in predicting thrombotic and cardiovascular complications in these groups.
While the data in pregnancy may be sparse, several studies have described consistent findings of hypercoagulability in pregnancy using TEG,14,49–54 particularly decreased time to clot and fibrinolysis, and increased clot formation rapidity and strength. In studies which have included postpartum measurements, it has been determined that hypercoagulability persists until at least 24 h postpartum.50,55 Our recent study also demonstrated marked hypercoagulability in term pregnant women, 56 in particular increased alpha angle (rate of clot formation) (65.8 vs 54.1°, p < 0.001) and maximum amplitude (clot strength) (71.5 vs 60.6 mm, p < 0.001), consistent with published data.14,49–53 ROTEM has also demonstrated the hypercoagulability of pregnancy at term in several studies.17,57–59 A similar study in pregnant women undergoing Caesarean section would be of value in evaluating ROTEM’s ability to contribute to VTE risk assessment.
Thrombin generation with calibrated automated thrombogram
Thrombin is a factor central to the coagulation process and has numerous effects on various components of the coagulation system, including generating fibrin, activating platelets and triggering the anticoagulation pathways, typically through thrombomodulin.60,61 CAT allows a more comprehensive assessment of potential coagulability than routine coagulation assays, given that 95% of thrombin generation occurs beyond the time to clot formation. 60 CAT determines the rate and extent of thrombin generated after the addition of tissue factor stimulus. 62 The parameters include time to thrombin formation (lag time) and the rate (velocity index) and amount of thrombin (endogenous thrombin potential, ETP) generated (Figure 2).
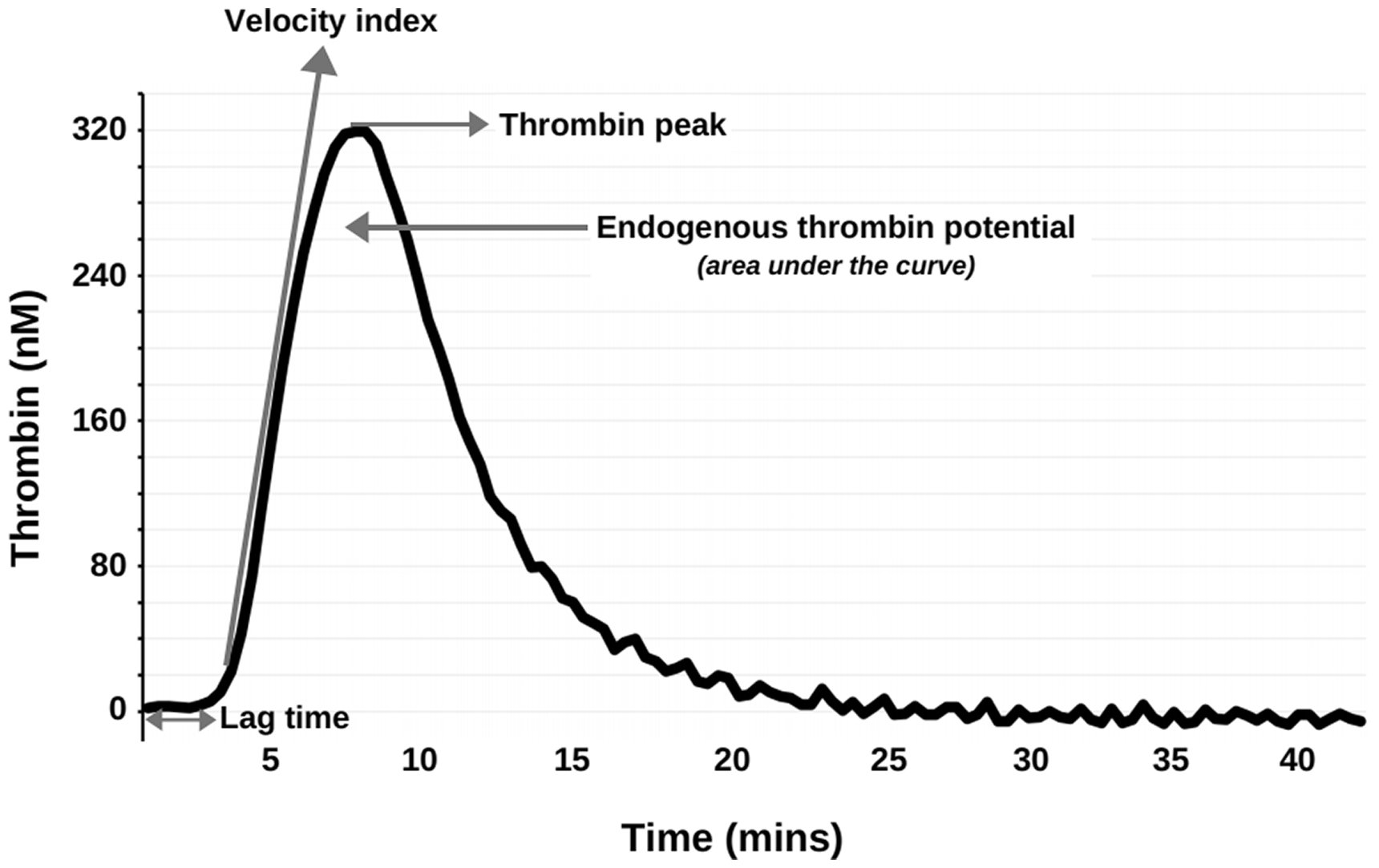
Example of calibrated automated thrombogram. The parameters measured are lag time (time required to reach 10-mM thrombin), peak height, velocity index (maximum slope of the initial part of the curve) and endogenous thrombin potential (ETP, total amount of thrombin generated i.e. area under the curve).
CAT has been shown in the non-pregnant population to assist with VTE risk assessment, with one study suggesting a high ETP could be considered an independent risk factor for VTE in patients with previous VTE but with no thrombophilia marker. 63 Tripodi et al. reported that patients with first unprovoked VTE and raised ETP or peak thrombin following discontinuation of anticoagulation had a greater risk of VTE recurrence (ETP, hazard ratio (HR) 3.41; peak thrombin, HR 4.57). 9 In addition to VTE risk prediction, there are emerging studies investigating the role of thrombin generation in cardiovascular disease with mixed findings to date – a French prospective cohort study of over 9000 subjects found that ETP correlated with risk of ischaemic stroke while the LURIC study demonstrated an inverse association between thrombin generation and event-free survival – demonstrating the complexity of the thrombin pathway.64,65 In a study of a heterogeneous cohort where 403 participants were stratified into risk categories based on their clinical VTE risk factors, pregnant women included, thrombin generation increased from no-risk to low-, intermediate- and high-risk participants. 66
Multiple studies with CAT demonstrate hypercoagulability in pregnancy, including a significant increase in peak thrombin generation and ETP early in pregnancy,67–72 consistent with our recent publication. 56 We reported that term pregnant women demonstrated markedly increased ETP (1895.2 vs 1399.4 nM/min, p < 0.001), thrombin peak (320.9 vs 240.0 nM) and velocity index (110.7 vs 83.4 nM/min, p < 0.001). Joly et al. reported that thrombin generation appears to increase early on in pregnancy and remained stable during pregnancy 67 although this differed to the findings by McLean et al. who reported the increase of thrombin generation with pregnancy progression. 71 Nevertheless, Bagot et al. hypothesised that the increased risk of venous thrombosis is likely to begin early in the pregnancy. 72 There is, however, currently a paucity of studies correlating the thrombin generation parameters with vascular pregnancy complications and thromboembolic disease in pregnancy.
Fibrin generation with the overall haemostatic potential assay
Fibrin, the final product of the coagulation cascade, is a protein which polymerises from fibrinogen under the influence of thrombin and, together with platelets, forms a haemostatic plug over damaged endothelium. While there are several assays available for fibrinolysis, for the purpose of this review, we will focus on OHP including reporting our recent findings in pregnant women using OHP. OHP provides a measure of fibrin generation and fibrinolysis in platelet-poor plasma over time using repeated spectrophotometric readings. 73 A graphical representation of fibrin aggregation is produced when fibrin generation is triggered by exogenous thrombin and fibrinolysis by tissue-type plasminogen activator (Figure 3). 73 This curve represents the balance between these processes, namely the overall haemostatic potential.
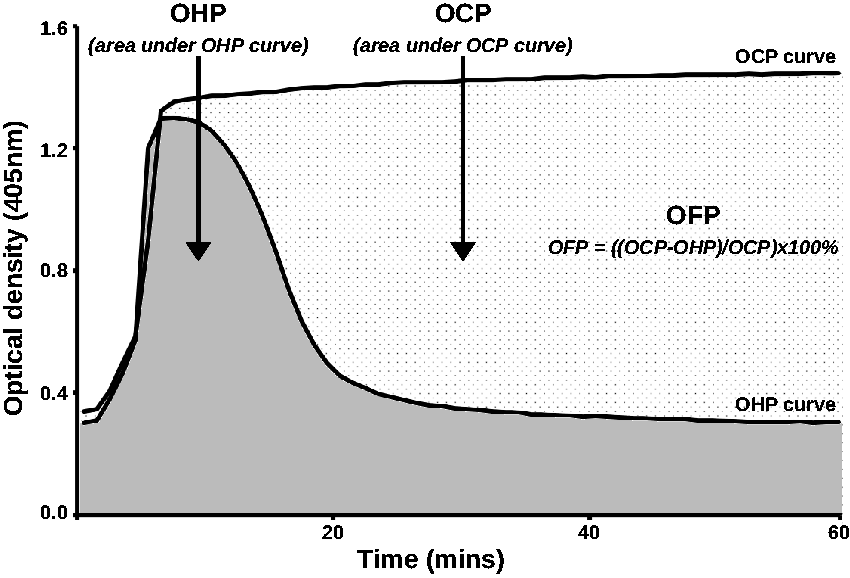
Example of typical curves generated by the overall haemostatic potential assay. The curves generated by the OHP assay represent the balance between the generation and proteolysis of fibrin. The overall haemostatic potential (OHP) curve is derived with the addition of tissue plasminogen activator and thrombin to a platelet-poor plasma sample. The overall coagulation potential (OCP) curve is derived with the addition of thrombin only. The overall fibrinolytic potential (OFP) is calculated using ((OCP−OHP)/OCP × 100%).
The data in OHP is limited and predominantly in small observational studies. In research settings, OHP has demonstrated the ability to characterise a number of hypercoagulable states such as antiphospholipid syndrome, pulmonary embolism, and coronary artery disease. 73 We recently reported the trend of OHP in term pregnancy in 60 women – compared to healthy controls, pregnant women had significant higher fibrin generation as measured with overall coagulation potential (57.6 vs 36.2 units, p < 0.001) and overall haemostatic potential (13.4 vs 6.7 units, p < 0.001) with reduced overall fibrinolytic potential; (76.3 vs 82.1%, p < 0.001). 56 Goldenberg et al. also demonstrated hypercoagulability in pregnant women using their assay, CloFAL (clot formation and fibrinolysis), which also utilised turbidimetric assay. 74 In addition, a study of 88 non-pregnant women who had experienced a prior pregnancy-related DVT revealed increased OHP levels compared with controls. 75 This suggests that increased fibrin generation and decreased fibrinolysis in some women may represent a prothrombotic phenotype. Nonetheless, fibrin generation assays such as OHP assays remain in their infancy and further obstetric and non-obstetric studies are required.76,77
Challenges ahead for the validation of global coagulation assays as biomarkers of pregnancy-associated VTE
GCAs appear to be more sensitive than traditional coagulation assays in detecting hypercoagulability and have shown some promising results in the VTE area, particularly using thrombin generation. However, while applying GCAs to the task of risk stratification for pregnancy-associated VTE is an attractive proposition, there is much work that needs to be done before GCAs could be considered for clinical use (Figure 4). While the techniques for viscoelastic testing have largely been optimised, particularly in the setting of massive transfusion, CAT and OHP are still in their infancy with regard to analytical validation. The analytical validation of each assay would require inter-operator and inter-operator standardisation and importantly the development of reproducible, robust pregnancy-specific reference values. The coagulation changes during each trimester and during the post-partum period should also be accounted for.
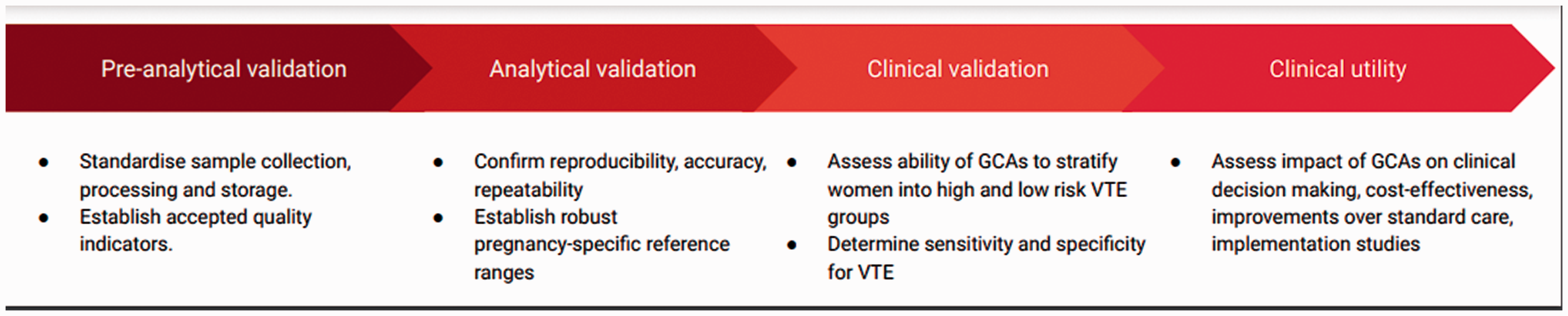
Translating global coagulation assays into clinical practice.
In addition, whilst detecting hypercoagulability is useful, it is critical to show correlation between GCA parameters and predicting clinical outcomes. This needs to take into account the various risk groups in pregnancy, including evaluating common higher risk scenarios like obesity. Finally, the incorporation of these assays in routine laboratory and clinical risk assessment models are required.
Conclusion
VTE risk assessment and prevention remains a major challenge during pregnancy and the puerperium with varying guidelines and lack of currently available biomarkers to assist with risk stratification. Early data on GCAs have been able to reflect the hypercoagulable state of pregnancy, which traditional coagulation assays are unable to do. The development of a multiple biomarker approach to individualise VTE thromboprophylaxis would be a significant advance from the traditional screening with clinical risk factors alone. However, whether GCAs will eventually be applied to pregnancy-associated VTE risk prediction will depend on a dedicated effort to demonstrate their analytical and clinical validity in the obstetric population.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Guarantor
PH is the guarantor of the present work.
Contributorship
HYL, LH and PH conceived the topic of review and researched the literature. DO researched the literature and drafted the review. All authors reviewed and edited the manuscript and approved the final version to be published.