
Abstract
Background
Pregnancy following bariatric surgery requires tailored care. The current Australian care provision and its alignment with consensus guidelines is unclear.
Methods
Antenatal care clinicians were invited to complete a web-based survey assessing multidisciplinary referral, gestational diabetes mellitus (GDM) and micronutrient management practices.
Results
Respondents (n = 100) cared for pregnant women with a history of bariatric surgery at least monthly (63%) with most (54%) not using a specific guideline to direct care. GDM screening methods included one-week of home blood glucose monitoring (43%) or the oral glucose tolerance test (42%). Pregnancy multivitamin supplementation changes (59%) with bariatric surgery type were common. Half (54%) screened for micronutrient deficiencies every trimester and conducted additional growth ultrasounds (50%).
Conclusion
The care clinicians report providing may not align with current international consensus guidelines. Further studies with increased obstetric clinician response may aid increased understanding of current practices. The development of workplace management guidelines for pregnancy in women with a history of bariatric surgery may assist with providing consistent evidence-based care.
Introduction
Bariatric surgery is an increasingly popular approach to treating obesity. 1 A significant portion of bariatric surgeries occur in women of childbearing age, with women aged 35–44 years receiving the highest number of episodes of care involving bariatric surgery in Australia in 2014–2015. 2 As improved fertility is a known outcome of weight loss, more women are becoming pregnant following bariatric surgery.2,3
Pregnancy in women with a history of bariatric surgery can lead to a higher risk of maternal malnutrition and associated adverse perinatal outcomes. 4 Malabsorptive procedures like Roux-en-Y gastric bypass, biliopancreatic diversion and gastric bypass typically incur greater risk of micronutrient deficiency than solely restrictive procedures, such as sleeve gastrectomy and laparoscopic gastric banding. 5 At-risk micronutrients following bariatric surgery include thiamine, folate, iron, Vitamins A and D, and calcium, with deficiency risk varying with procedure type. 6 Maternal malnutrition risk may be exacerbated if post-bariatric surgery weight loss is still occurring during pregnancy, considering the increased micronutrient requirements for healthy placental and fetal growth. 5 Adverse neonatal outcomes associated with these deficiencies potentially include neural tube defects, blindness, small for gestational age and intra-uterine growth restriction.4,5,7,8 Screening for gestational diabetes mellitus (GDM) may also be challenging due to altered glucose absorption and metabolism following bariatric surgery with the standard oral glucose tolerance test (OGTT) poorly tolerated in many women. 9 The potential for complications in women and the growing baby following bariatric surgery suggests that enhanced monitoring and surveillance may be needed alongside detailed recommendations for care.
Consensus-level evidence-based recommendations exist for the care of pregnant women with a history of bariatric surgery, most recently Shawe et al. 2019 International Consensus Guidelines.3,8,10–14 These include guidance in multiple areas, such as nutrition advice, micronutrient supplementation and monitoring, and GDM screening. No guidelines have been endorsed by a professional obstetrics body and few studies report on current management practices for pregnant women with a history of bariatric surgery. A 2017 survey of obstetricians (n = 106) in the United States (US) 15 found respondents were comfortable in caring for these women, however acknowledged a gap between the 2009 American College of Obstetricians and Gynaecologists practice bulletin 16 and obstetrician knowledge and recommendation of such practices. In line with the widely understood delay between research emerging and its implementation into practice, 17 such results may be expected in areas of emerging evidence.
With the increase in pregnancies in women with a history of bariatric surgery and potential implications for pregnancy outcomes, a better understanding of the care being provided to these women is needed to develop interventions for uptake of evidence into practice and to identify areas where stronger evidence is needed. The current study aimed to assess care and management practices of antenatal practitioners caring for pregnant women following bariatric surgery in Australia.
Materials and methods
Study design and ethics
A cross-sectional, national survey was disseminated via purposive and snowball sampling methods. The survey was hosted on the online survey platform, Qualtrics (Qualtrics, Provo, UT) and distributed via weblink to professional bodies. Dietitians Australia (DA) and the Society of Obstetric Medicine of Australia and New Zealand (SOMANZ) sent out a survey invitation to members in the weekly emailed newsletter. SOMANZ emailed a reminder to members a week before the survey closed. DA sent an email to members of special interest groups for bariatric surgery and maternal health as a reminder email two weeks after the initial invitation. Invitations were also sent to members of the Australian Diabetes in Pregnancy Society (ADIPS) and the Queensland Maternity and Neonatal Clinical Network. The researchers emailed the survey link to their professional networks and contacts across Australia who were invited to forward the link on to other relevant professionals.
No incentive was offered for survey completion. The survey was open from March 16th to May 8th, 2020 and again from 1st November to 15th December 2020, due to low survey response in the initial phase. Ethical approval was obtained from The Prince Charles Hospital Human Research and Ethics Committee (#60719) with an administrative review by the University of Queensland.
Eligibility criteria
Eligible respondents were health professionals currently working in, or with recent experience in, outpatient antenatal services in Australia or New Zealand, who had not previously completed the survey. Respondents were excluded if they answered sociodemographic questions only.
Survey development and data collection
The survey was developed using the recently released International Consensus Guidelines 14 and researcher professional experience, and revised according to stakeholder feedback in the pilot phase. The survey was reviewed and piloted on the Qualtrics platform by eight professionals, including obstetricians, an obstetric physician and dietitians, to assess content and face validity, establish user experience and provide feedback. The survey included multiple choice and open-ended questions to assess the care and management of pregnant women following bariatric surgery.
Ten questions assessed demographic and workplace characteristics of respondents, including gender, age, years of clinical experience, recency of practice in maternity services, hours per week in employment, locations of work, and size and type of facilities that respondents have worked in. One question asked respondents to identify their practising discipline, with available responses including obstetric doctor, obstetric medicine doctor, dietitian and midwife. Dependent on practitioner type, respondents were directed down one of two survey arms. Both arms included similar questions by content but were tailored to the professional responsibilities of either dietitian (34 questions) or obstetric doctor, obstetric medicine doctor, midwife and other health professionals (37 questions). Questions investigated care and management practices of pregnant women with a history of bariatric surgery, including: frequency of referrals received, referral to dietitian and how this was impacted by gestational weight gain (GWG) and GDM status, screening and diagnosis methods for GDM, micronutrient screening practices, micronutrient supplementation type and dosage, ultrasound monitoring of fetal growth, how practices differ with regard to bariatric surgery type, trends observed and expected regarding number of presentations of pregnant women following bariatric surgery, and whether guidelines had previously been used when treating pregnant women with a history of bariatric surgery and what these addressed. Two additional questions assessed respondent awareness of the recent Consensus Guidelines 14 and whether these had impacted management practices for pregnant women with a history of bariatric surgery. For many multiple-choice questions, respondents could select more than one option and opt to leave a free text comment. The final question enabled respondents to leave additional comments about the management and care of pregnant women following bariatric surgery. Questions regarding fetal growth ultrasounds and changing of micronutrient testing with bariatric surgery type were only displayed in the medical/midwifery arm of the survey.
A summary of survey results was emailed to respondents who opted to provide their contact email address in an external survey that did not link to the original survey.
Statistical analysis
Responses were exported from Qualtrics to Microsoft Excel Version 16.33 (Microsoft Corp., Redmond, WA, USA) for cleaning. Data were analysed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA). Descriptive analyses are reported as proportions of eligible responses (n, %), or median and range where applicable. Free text responses were summarised by common themes Table 2.
Summary of free text responses by question and theme
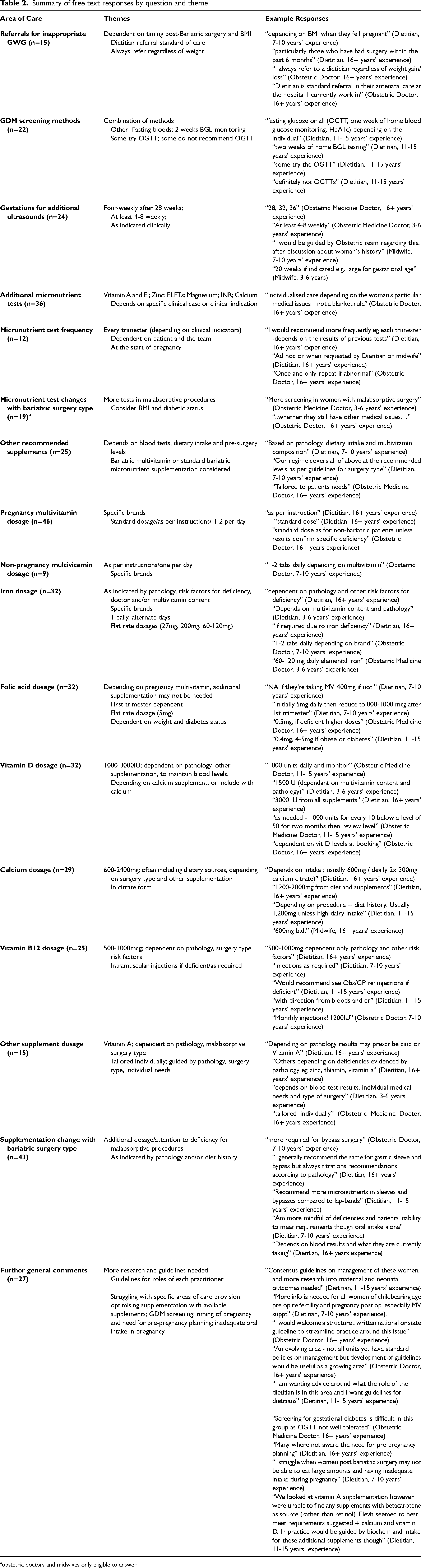
obstetric doctors and midwives only eligible to answer
Results
Of 116 submitted survey responses, 16 were ineligible as they had only completed sociodemographic questions. Eighty-four percent of eligible respondents (n = 84/100) answered the survey to completion. Around the time of survey distribution, SOMANZ, DA and ADIPS had respectively 401, 18 over 7000, 19 and 291 members. 18 As the number of eligible participants was unable to be confirmed (i.e. members working in antenatal care), survey response rate was unable to be determined.
Dietitians (46%), obstetric doctors (16%), obstetric medicine doctors (18%), and midwives (18%) responded (Table 1). The sample was majority female (93%), was currently working clinically in maternity services (82%) and had worked in Queensland (66%).
Respondent characteristics and clinical responses by total sample.
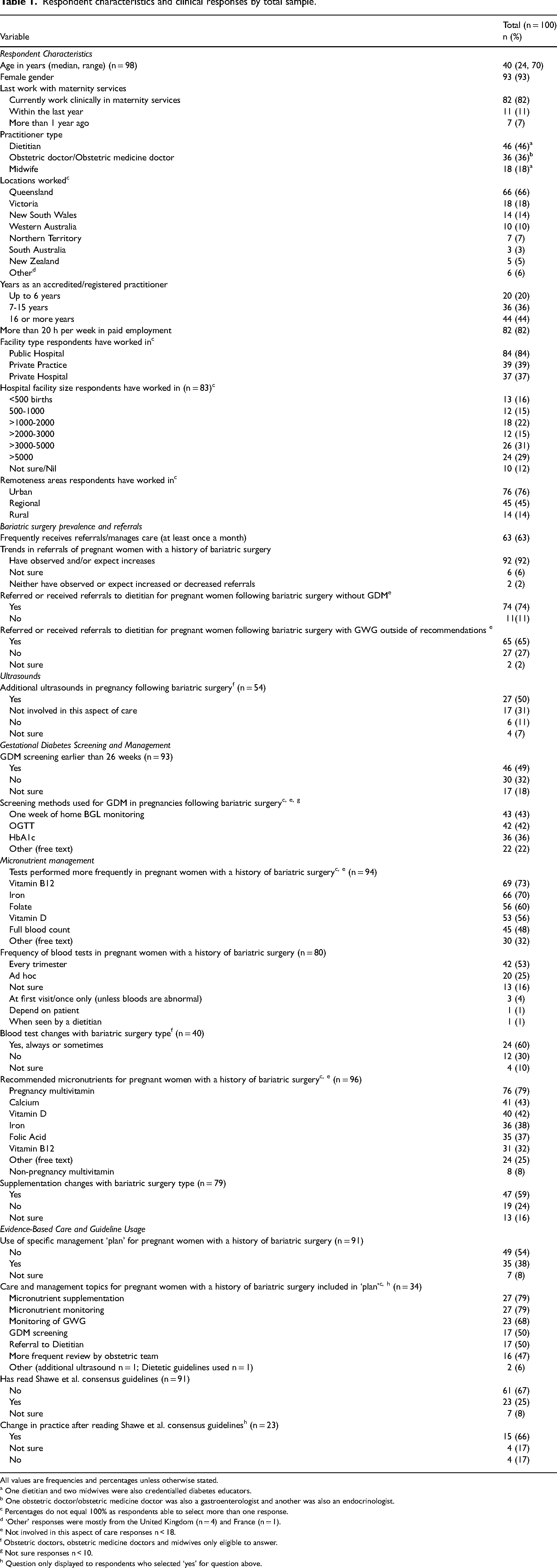
All values are frequencies and percentages unless otherwise stated.
a One dietitian and two midwives were also credentialled diabetes educators.
b One obstetric doctor/obstetric medicine doctor was also a gastroenterologist and another was also an endocrinologist.
c Percentages do not equal 100% as respondents able to select more than one response.
d ‘Other’ responses were mostly from the United Kingdom (n = 4) and France (n = 1).
e Not involved in this aspect of care responses n < 18.
f Obstetric doctors, obstetric medicine doctors and midwives only eligible to answer.
g Not sure responses n < 10.
h Question only displayed to respondents who selected ‘yes’ for question above.
Bariatric surgery prevalence and referrals
Over half of respondents had received referrals at least once a month for pregnant women with a history of bariatric surgery (63%, Table 1). Most respondents (92%) had observed and/or expected increased referral rates. Many respondents had received or created a dietetics referral in the absence of GDM (74%), or when GWG was outside of recommendations (65%).
Respondents indicated (n = 15, Table 2) that dietetic referrals related to GWG were often made for pregnancies that occurred soon after bariatric surgery, “particularly those who have had surgery within the past 6 months” (Dietitian, 16 + years’ experience). A dietetics referral was sometimes a component of standard care: “always refer(ing) to a dietitian regardless of weight gain loss” (Obstetric doctor, 16 + years’ experience).
GDM management
Almost half of respondents reported screening for GDM in pregnant women with a history of bariatric surgery earlier than 26 weeks’ gestation (49%, Table 1). One-week of home blood glucose monitoring was the most common GDM screening method (43%), followed by the OGTT (42%) and HbA1c (36%). Some respondents (n = 22, Table 2) reported using a combination of GDM screening methods: “fasting glucose or all of the above [OGTT, HbA1c, one-week home blood glucose monitoring], depending on the individual” (Dietitian, 11–15 years’ experience).
Fetal growth ultrasounds
Half of respondents performed additional ultrasounds to monitor fetal growth in pregnant women following bariatric surgery (50%, Table 1). Additional ultrasounds were commonly indicated (n = 24, Table 2) at 28, 32 and 36 weeks’ gestation.
Micronutrient management
Most respondents assessed Vitamin B12 (73%), iron studies (70%), folate (60%) and vitamin D (56%) more frequently for pregnant women with a history of bariatric surgery than other pregnant women, with 53% testing every trimester (Table 1). Other requested tests (n = 36, Table 2) included vitamin A, zinc and calcium. Blood test requests changed with bariatric surgery procedure (60%), with tests ‘more frequent with malabsorptive’ surgeries (Obstetric medicine doctor, 16 + years’ experience).
A pregnancy multivitamin was widely recommended (79%). Other recommended supplements included calcium (43%), vitamin D (42%), iron (38%) and folic acid (37%). Most respondents (59%) changed supplementation advice depending on the woman's bariatric surgery type. Increased micronutrient monitoring or additional supplementation was reported where malabsorptive surgery had occurred (n = 43, Table 2).
In general, respondents said dosing for micronutrient supplementation was guided by the specific clinical situation, pathology results, diet, weight, diabetes status and the medical team they were working with. Specific dosages given for individual micronutrients are summarised in Table 2.
Evidence-based care and Guideline usage
Half of respondents had not used a specific guideline for managing the care of pregnant women with a history of bariatric surgery (54%, Table 1). When available, guidelines most commonly included advice on monitoring micronutrient supplementation (79%), micronutrient status (79%) and GWG (68%).
A third of respondents (33%) had read the Shawe et al. consensus guidelines, 14 with many changing their practice after reading (66%).
Further general comments (n = 27, Table 2) supported the development of a national guideline: “a simple national guideline would be good” (Obstetric doctor, 3–6 years’ experience) and “…useful as (pregnancy after bariatric surgery) a growing area” (Obstetric doctor, 16 + years’ experience). Other issues reported included the difficulties in screening for GDM, wanting more guidance around the role of the dietitian in this area, and optimising supplementation according to recommendations (Table 2).
Discussion
This is the first study to examine care and management practices of a multidisciplinary sample of antenatal professionals providing care to pregnant women with a history of bariatric surgery. Care varied between respondents and in some areas did not align with current consensus guidelines. 14
There was wide variation in reported GDM screening methods, potentially indicating a gap between existing guideline recommendations and current practice. Just under half of respondents indicated using the OGTT for GDM screening, which is inconsistent with current recommendations due to potential adverse effects on the woman and inaccurate blood glucose level readings.9,14 Many respondents provided alternatives to the OGTT or employed a range of screening methods depending on individual clinical situations, which is similar to a 2017 survey of US obstetricians, with 71% reporting always or sometimes practicing GDM screening methods other than the OGTT. 15 Whilst practice in this area is inconsistent, the difficulty of screening for GDM in this population has been acknowledged as an area needing further investigation. 20 Promoting more standardised methods across the professions involved in GDM screening may encourage optimal, evidence-based and safe care.
Micronutrient monitoring was not consistently aligned with current evidence. Whilst most respondents tested for micronutrients of concern as per the consensus guidelines, only half of respondents followed the recommendation that micronutrient levels should be tested every trimester.13,14 Many respondents acknowledged micronutrient management practices differed based on the clinical situation, such as malabsorptive procedures warranting increased micronutrient monitoring. This theme continued into dosing practices, with most respondents altering individual micronutrients dosages according to specific clinical indications and identified deficiencies, which aligns with published advice.13,21 A pregnancy multivitamin was commonly recommended, however multivitamin brands cited did not meet all of the minimum micronutrient amounts specified in the consensus guidelines. 14 Of particular note in these pregnancy multivitamins was the insufficient levels of folic acid and vitamin A, which persons undergoing malabsorptive procedures are prone to deficiency in following surgery. 22 This is concerning as further individual micronutrient supplementation was reported by some respondents as unnecessary if a woman was taking a multivitamin, meaning some women may be consuming less than the minimum micronutrient recommendations. As pregnant women with a history of bariatric surgery are vulnerable to micronutrient deficiencies, which may lead to poor outcomes for neonates,4,5 supplementation regimens meeting minimum requirements may assist in avoiding complications and promote optimal health in infants and women after bariatric surgery.
Over half of respondents had referred women to a dietitian or received a referral as a dietitian for women without GDM, aligning with recommendations for the close monitoring of nutritional status in these women. 14 Referral rates for GWG outside recommendations were lower, potentially indicating an area where interdisciplinary collaboration could be increased to optimise outcomes. This is particularly pertinent for women who have undergone bariatric surgery less than 12 months prior as they may still be losing weight and thereby at increased nutritional risk.14,21,23 Reported dietitian referral rates were similar to the high rates previously reported in an US obstetric sample (74% vs. 72%). 15 However, respondents commented on the need for clarification of practitioner roles, especially for dietetics, indicating a potential area for further development.
Respondents observed an increase in presentations of pregnant women following bariatric surgery and predicted this would increase in the future. While this is unsurprising given that women of childbearing age represent the largest population undergoing bariatric procedures in Australia, 2 there appears to be a lack of guideline development that provides evidence-based, consistent care recommendations to this growing high-risk cohort.
Less than half of respondents had either used a specific guideline for managing care of pregnant women with a history of bariatric surgery or had read the most recent consensus guidelines. 14 The development of a national guideline was raised in this study, potentially indicating a need for evidence around pregnancy after bariatric surgery to be synthesised for the Australian context. The dearth of evidence in this practice area, particularly with regards to GDM screening and micronutrient management, 14 may mean that developing and reaching consensus on a national guideline would be challenging. 24 Improved dissemination of existing evidence and implementation of local workplace multidisciplinary instructions may be useful strategies in overcoming such barriers. 25 This approach may address the research implementation delay that is experienced across many areas of health care. 17 It may further encourage safer practices, such as using multiple methods to screen for GDM 14 and could additionally strengthen relationships within and facilitate the provision of comprehensive care from multidisciplinary antenatal teams, as is currently recommended.3,10,11,21
Several limitations of this study restrict generalisability of findings across Australia and clinical professions. Two-thirds of respondents had practised in Queensland, likely due to snowball recruitment methods and researcher professional networks being localised to south-east Queensland, meaning results may not indicate national practice patterns. Respondent demographic data is unable to be examined to show if multiple respondents were practicing in the same facility, meaning some care practices may have been overrepresented in the current sample. While the dietitian sample size may be reflective of the small antenatal dietetics workforce, 26 the representation of obstetric doctors, obstetric medicine doctors, and midwives was low. Reasons for low response from these professions may be due to survey dissemination during the COVID-19 pandemic, length of the survey and clinician time burden. Additionally, a response rate for the survey was unable to be calculated. Whilst consensus guidelines are available, 14 these were published recently with no Australasian representation. More work is needed to assist with standardisation of models of care for pregnancies after bariatric surgery, whilst also facilitating the flexibility needed for practitioners to respond to each woman's individual clinical presentation.
This is the first study to explore antenatal multidisciplinary staff care and management practices for pregnant women with a history of bariatric surgery in Australia. Management practices varied amongst clinicians. Discrepancies were also observed between care practices and consensus guidelines with regards to GDM screening practices and micronutrient monitoring, potentially due to a lack of awareness of consensus guidelines. Further research targeting practices of individual professions, as well as the experiences of joint multidisciplinary teams, may provide further insight into the variety of current practices. The development of multidisciplinary workplace management guidelines for pregnant women with a history of bariatric surgery may assist with providing timely and consistent evidence-based care to these women.
Footnotes
Acknowledgements
With thanks to Queensland Health for their support with this project. SDJ is supported by a Metro North Hospital and Health Service Clinician Fellowship.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics
Ethical approval was obtained from The Prince Charles Hospital Human Research and Ethics Committee (#60719) with an administrative review by the University of Queensland.
Informed consent
Written informed consent was not obtained because of the survey design utilised in the study. Respondents were notified on the cover page of the survey, that by completing the survey they were consenting to the participate in the research.
Guarantor
Dr Michelle Palmer, Research Dietitian and Team leader – Logan Hospital, Armstrong Rd &, Loganlea Rd, Meadowbrook QLD 4131.
Contributorship
MP, HP, SH and SDJ conceived of the study. MP and EE were responsible for ethical approval. All authors contributed to study design and participant recruitment. EE collected the data. EE and MP were responsible for data management and analysis. EE wrote the first draft of the manuscript with support from MP and SDJ. All authors reviewed and edited the manuscript and approved the final version.