
Abstract
Kasabach–Merritt syndrome (KMS) is a coagulopathy characterized by thrombocytopenia and hypofibrinogenemia associated with large vascular tumors. KMS can lead to disseminated intravascular coagulation which, if not treated promptly, can be life-threatening. There are few reported cases of this syndrome and its evolution in pregnant women.
Background
Kasabach–Merritt syndrome (KMS) is a life-threatening thrombocytopenic coagulopathy associated with vascular tumors. KMS is characterized by severe thrombocytopenia and hypofibrinogenemia, although anemia and elevated D-dimer may also be seen. 1 The basic pathophysiology of KMS is platelet trapping, activation, and consumption within the abnormal vascular structure, with consequent consumption of fibrinogen and coagulation factors, followed by fibrinolysis, leading to a high risk of bleeding.1–3 Initially, it was thought that KMS could occur in any fast-growing common infantile hemangioma. Subsequently, some authors almost exclusively attributed the development of this syndrome to more aggressive vascular tumors such as Kaposiform hemangioendothelioma and tufted angioma.1,4 However, it is now well described that this syndrome can be seen in other vascular tumors with this “aggressive” quality, such as large hemangiomas (>5 cm), angiosarcomas, or even smaller lesions such as arteriovenous fistulas.2,3,5–17
Pregnancy is a condition in which the development or growth of vascular tumors is favored, either by hormonal or mechanical factors.10,18,19 There are various locations and clinical manifestations derived from vascular tumors reported in pregnant women; with few reported cases of KMS in this group of patients.3,5,10–15,17 We describe the case of a pregnant woman with a giant infiltrating hemangioma of the colon who developed at six weeks of gestation.
Case report
35-year-old woman was pregnant for the second time. Her first pregnancy was 9 years prior and she required a caesarean delivery due to the presence of hemangiomas on the vulva. She had been diagnosed with cutaneous hemangiomatosis at the age of 1 year, and systemic involvement at the age of 30. This was in the spleen and colon that caused compressive symptoms and digestive tract bleeding, respectively (Figure 1). She underwent splenectomy (but did not consent to left hemicolectomy) but this was complicated by postoperative bleeding (hemoperitoneum and retroperitoneal hematoma) that required management in the intensive care unit (ICU) and transfusion of multiple units of packed red cells (PRC) and fresh frozen plasma (FFP).
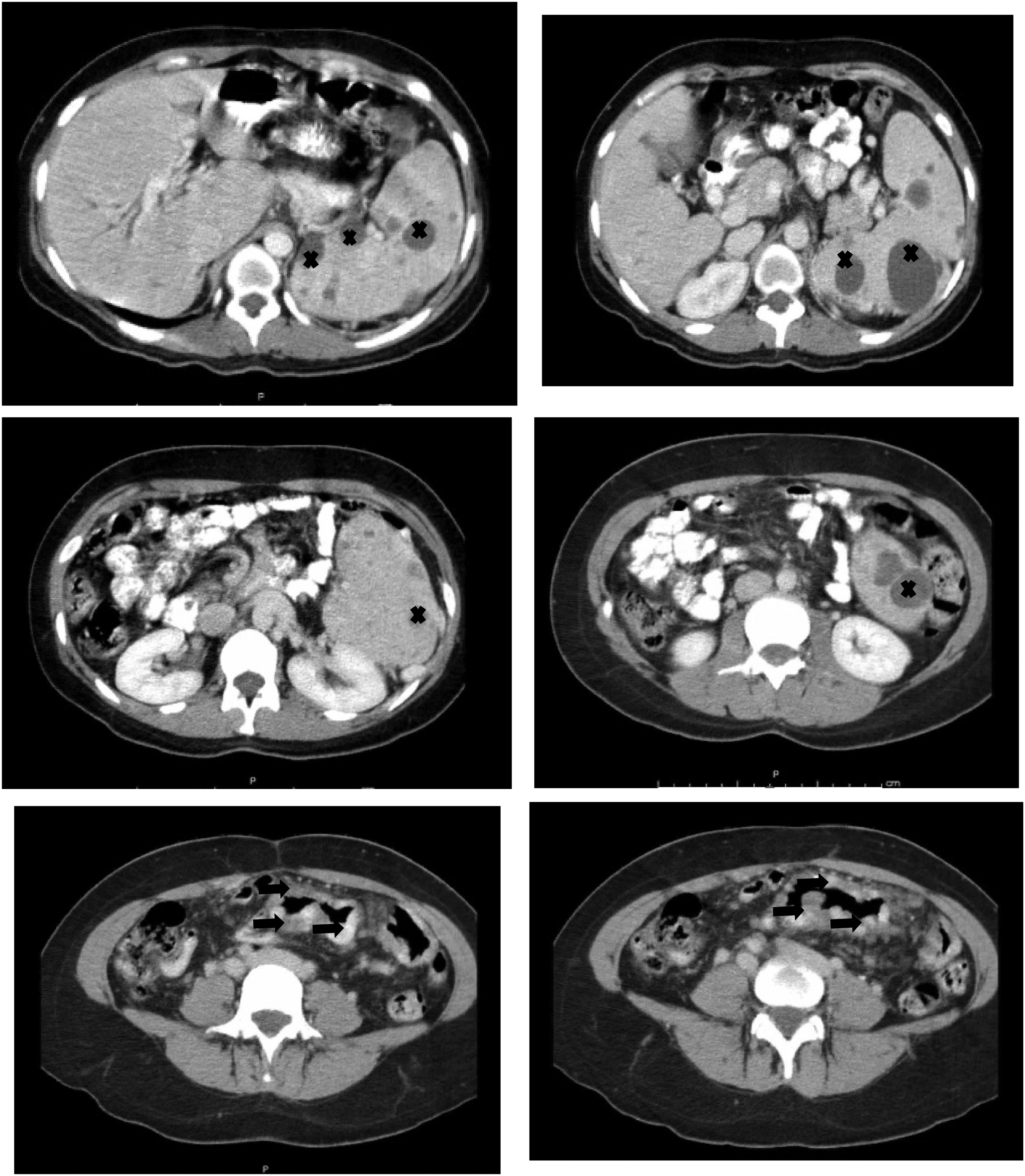
Abdominal computed tomography showing splenomegaly secondary to hemangiomas in the spleen (some are marked with crosses) and colon hemangiomas (arrows).
She was referred to our hospital due to threatened miscarriage at six weeks of gestation, with grade II hemorrhagic hypovolemic shock (HHS). The physical examination revealed pallor of the skin, tachycardia, cutaneous hemangiomas (legs, labia majora of the vulva, and perianal region), and transvaginal and transrectal bleeding. Due to the history of colon hemangiomatosis, hemangioma growth with secondary coagulopathy was suspected.
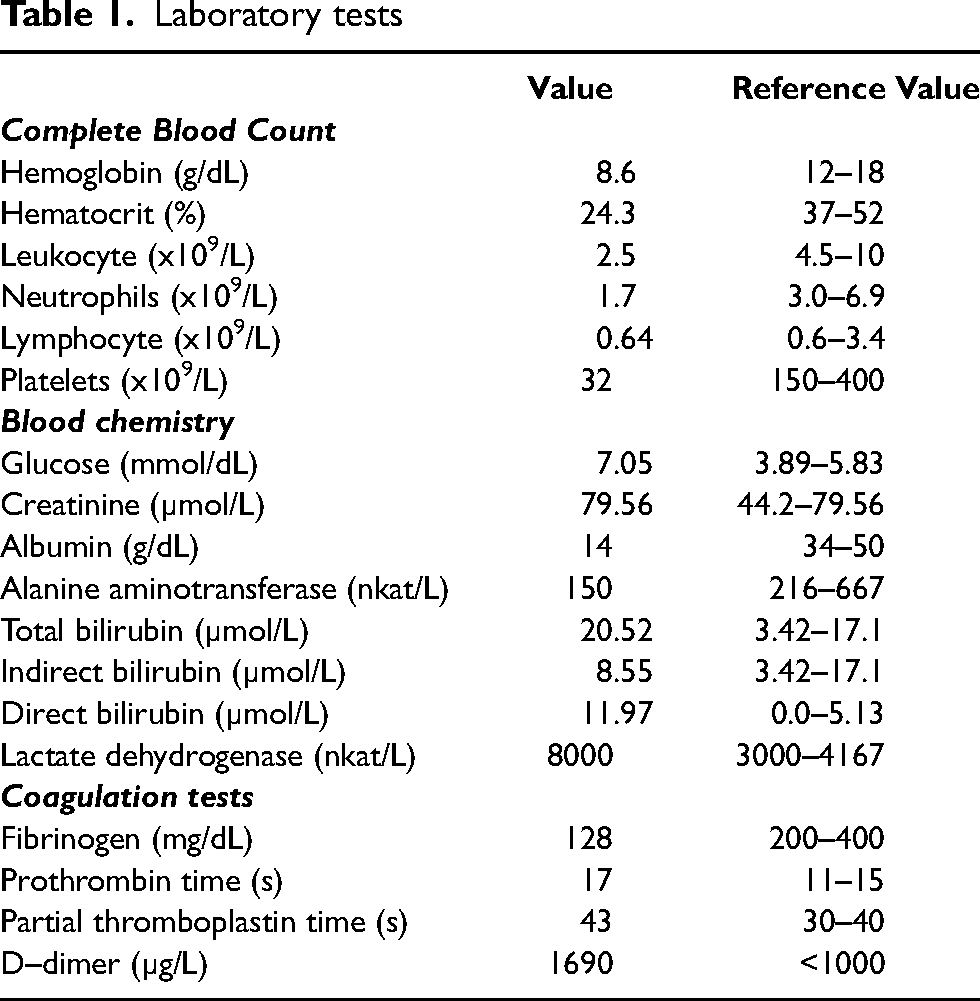
Her laboratory tests showed anemia, thrombocytopenia, and hypofibrinogenemia, consistent with KMS (Table 1). Abdominal computed tomography showed a colonic hemangioma, seen as a 23 × 6.5 × 7 cm left para-aortic lesion, which extended from the L2 vertebral body to the pelvic cavity consistent with a colonic hemangioma (Figure 2). The Doppler ultrasound confirmed that it was a hemangioma.
Laboratory tests
Treatment consisted of transfusion of PRC, FFP, cryoprecipitate, and epsilon aminocaproic acid (EAA), without achieving bleeding control. On her third hospitalization day, she presented with massive rectal bleeding that led to grade IV HHS. Hemodynamic stability goals were not achieved, so the patient accepted left hemicolectomy, understanding the poor prognosis for the embryo. Preoperative blood preparation continued with EAA to control fibrinolysis, and dexamethasone 24 mg daily. During surgery, a giant hemangioma was found involving two-thirds of the descending colon, sigmoid, and rectum, and infiltrating the uterus and bladder, with capillary bleeding. A left hemicolectomy was performed, (Figure 3) leaving part of the infiltrated hemangioma in the uterus and bladder, cauterizations were performed to control the bleeding, and a colostomy was performed. She continued to be monitored in ICU with mechanical ventilation and without recovery from HHS despite vasopressors, transfusion of blood components, EAA, and activated factor VII. A new surgical exploration was carried out, finding intestinal ischemia, hemoperitoneum (2000 cc), and capillary bleeding in the presacral plexus, omentum, peritoneum, and mesentery. Intra-abdominal packing was performed, and she returned to the ICU. The state of HHS persisted, leading to her death 24 h later.
Discussion
KMS is a life-threatening thrombocytopenic coagulopathy associated with a wide variety of vascular tumors. Abnormal vascular structure causes platelet entrapment, activation, and consumption, leading to hyperfibrinolysis by activation of the coagulation cascade, increasing D-dimer, and prolonging prothrombin and activated thromboplastin times, causing chronic disseminated intravascular coagulation.1–3
Pregnancy is a precipitating factor for the development or increase in the size of vascular tumors, either due to hormonal factors such as estrogens, vascular endothelial growth factor, basic fibroblast growth factor, and placental growth factor; or due to mechanical factors such as increased intravascular volume.10,18–20 There are several case reports of pregnant women with vascular tumors, and management is a challenge that requires a multidisciplinary medical team. Within these cases, we found only nine cases that developed KMS, and one of them died due to bleeding complications.3,5,10–15,17 Five of them had been diagnosed with a vascular anomaly since childhood and developed KMS in the first pregnancy3,11–14; two of them had a second pregnancy in which they presented in this way again.11,14 One patient presented with KMS in her fourth pregnancy, at which time a giant colonic hemangioma was diagnosed. 10 The patient who died was 17 days postnatal following a normal vaginal delivery and, as in our case, it was a colon hemangioma in which supportive treatment with transfusions and surgical treatment was unsuccessful. 17 It is very likely that in the rest of the patients, there were pre-existing undiagnosed hemangiomas and that during the pregnancies they grew enough to develop KMS. A similar situation occurred in our patient, who did not have additional studies, either in childhood or prior to the first pregnancy, to identify systemic disease. Therefore, we think that the first pregnancy favored the growth of pre-existing hemangiomas in the spleen and colon, the latter becoming an infiltrating hemangioma that, due to its size, favored the development of KMS in the second pregnancy.
Regarding treatment, KMS shows wide variation in its response to different treatment modalities, and therefore definite treatment guidelines have not been established to date, 2 which is even more difficult in pregnancy. Surgical excision is the definitive treatment, but most lesions are not well-circumscribed, and surgery is complicated by bleeding due to thrombocytopenia, therefore this treatment option is not appropriate in most cases. Alternative therapies have been tried with variable results, including high-dose systemic corticosteroids, vincristine, sirolimus, propranolol, cyclophosphamide, actinomycin-D, bevacizumab, interferon, aminocaproic acid, tranexamic acid, dipyridamole, pentoxifylline, aspirin, ticlopidine, transarterial embolization, and radiation therapy.1,2,16
To the best of our knowledge, this is the second reported case of KMS associated with a colonic hemangioma, in this case, an infiltrating giant colonic hemangioma, in relation to pregnancy resulting in a fatal outcome. We can conclude that women with a known diagnosis of a vascular tumor, and who wish to become pregnant, should receive treatment aimed at eliminating or reducing the size of this anomaly. If this treatment prior to pregnancy is not possible, a high risk of potentially life-threatening bleeding should be considered. Therefore, they should receive prenatal counseling to avoid pregnancy or adequate multidisciplinary medical surveillance to reduce the risk of morbidity and mortality in the woman and fetus/newborn.
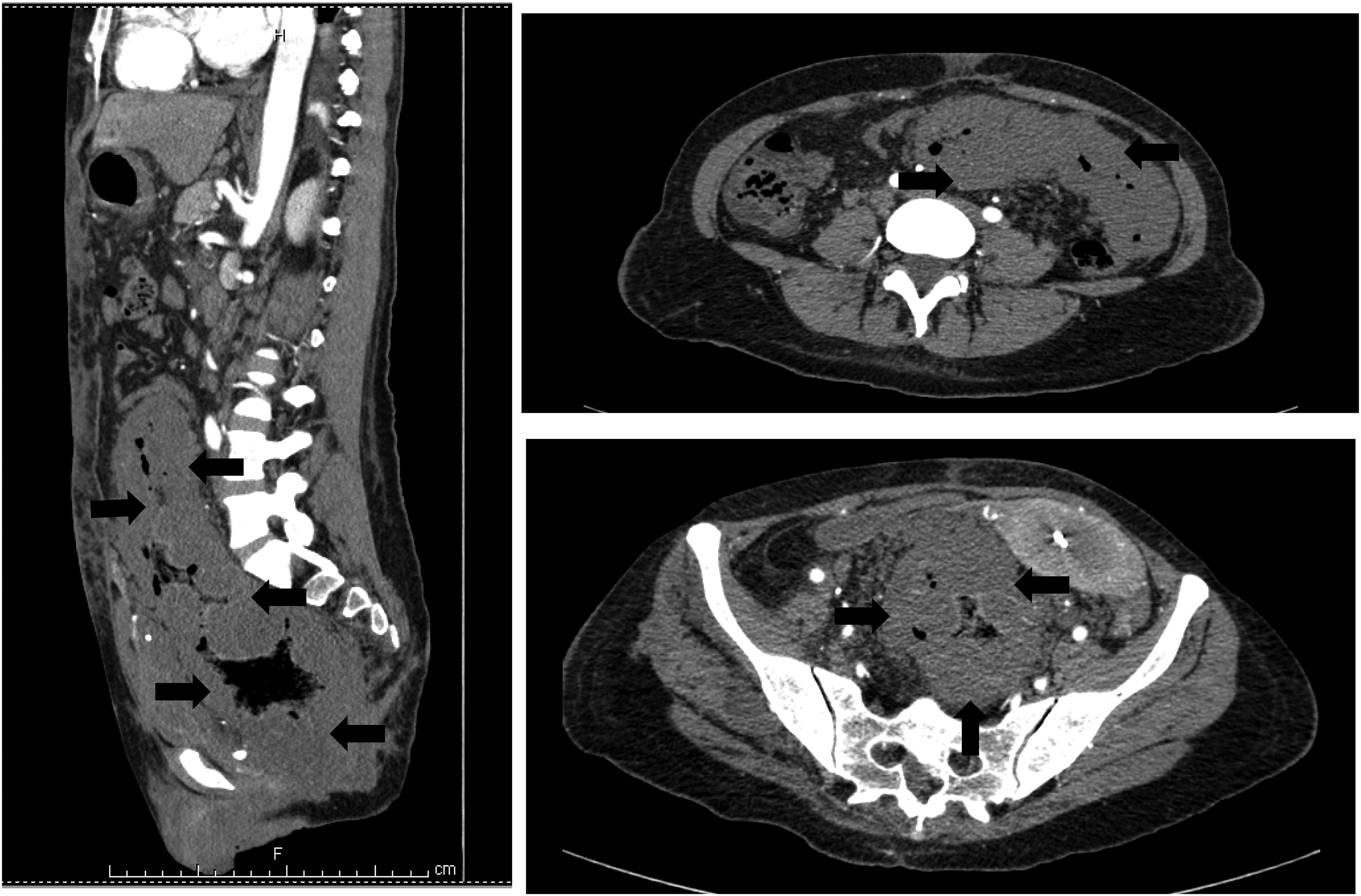
Simple and contrast-enhanced computed tomography of the abdomen showing diffuse thickening of the rectum and left colon consistent with hemangioma (arrows).

Hemicolectomy specimen showing the hemangiomas.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Guarantor
OLV is the guaranteeing author.
Contributorship
All authors participated in the acquisition and interpretation of data, as well as in the writing, revision, and final approval of the manuscript. All authors meet the International Committee of Medical Journal Editors authorship criteria.
Informed consent
Consent to publish was obtained from the patient.