
Abstract
Background
Female childhood cancer survivors with history of bone marrow transplant with or without total body irradiation have increased pregnancy risks. Preconception counselling and early referral to appropriate clinical pathways may improve pregnancy outcomes.
Methods
UK-wide survey of clinicians, promoted via social media and conferences, jointly funded by Action Medical Research/Borne.
Results
Forty responses received between 22 October 2020 and 21 October 2021:
43% reviewed this group monthly, 15% annually, 15% less than annually, and 27% never (for O & G only: 13%, 13%, 26%, and 48%, respectively). Pre-pregnancy, most discussed potential fertility/pregnancy implications. Early pregnancy discussions included late miscarriage (34%), preterm birth (44%), fetal growth restriction (31%), and health risks other than cancer (30%). During pregnancy: 80% refer to specialist clinics; 87% offer extra investigations; 33% prescribed aspirin; 20% offered cervical cerclage; and 13% prescribed progesterone.
Conclusions
Evidence of variation in care. As previous observations suggest pregnancy outcomes improve when managed in specialist clinics, clearer guidance is required.
Keywords
Introduction
Haematopoietic stem cell transplantation (HSCT), also known as bone marrow transplant (BMT), has evolved over the past 70 years to become standard for many malignant and non-malignant haematological conditions. 1 The two main types of HSCT are autologous (transplant of a person's own stem cells) and allogeneic (transplant of donor haematopoietic stem cells and immunological repertoire). 1 HSCT for the treatment of haematological childhood cancers was first performed in 1968. 2 Conditions which may require HSCT include acute lymphoblastic leukaemia, acute myeloid leukaemia, chronic myeloid leukaemia, myelodysplastic syndromes, Hodgkin and non-Hodgkin lymphoma, severe aplastic anaemia, and Fanconi anaemia. 2 In the United Kingdom, between 1997 and 2016, an average of 1645 cancers were diagnosed among children aged 0–14 years, and a further 2110 among teenagers and young adults (TYA, 15–24 year olds). 3 Leukaemia accounted for 31% of the cancers diagnosed in children, and lymphomas 10%. In TYA, lymphomas accounted for 20% and leukaemias 9% of cancers. 3 To decrease the risk of graft rejection and tumour burden, conditioning regimens are administered prior to HSCT. 4 Previously, allogeneic HSCT involved intensive myeloablative radiation, with or without chemotherapy, to eradicate cancer cells, suppress the immune system to prevent graft rejection, and to facilitate donor stem cell engraftment.1,5 Although these regimens have subsequently been modified to reduce toxicity, myeloablative conditioning remains standard for many to reduce the risk of relapse in younger people.1,6
With such advances in treatment, the life expectancy for those who require HSCT for the treatment of childhood and TYA cancers has increased over recent decades. 4 Overall, the 5-year survival rate for childhood cancers now exceeds 80% in many countries.7,8 This is largely due to earlier diagnosis, effective multimodal therapies, and good supportive care.7,9 However, the combination of the conditioning treatment and HSCT are often associated with side effects related to organ toxicity.6,7,10 The term ‘late-effects’ refers to longer-term effects, which may be secondary to the underlying disease process or to an aspect of the HSCT treatment.6,10,11 One group found the cumulative incidence of late effects among 162 survivors was 93.2%, with associated risk factors including older age at HSCT and receiving a conditioning regimen that included irradiation (OR 2.2, 95% CI [1.1–4.7], p = .03). 10
Subfertility and infertility are important late effects associated with HSCT, 12 and having children is known to be a quality of life determinant for cancer survivors. 13 Childhood and TYA cancer survivors are estimated to have an 80% reduction in fertility.14,15 Many of the conditioning regimens, including alkylating agents and total body irradiation (TBI), can impair fertility through gonadotoxicity or via a direct effect on tissues.4,9 Late-effect endocrine dysfunction particularly affects children who survive HSCT, even if these regimens do not contain radiation. 6 This can affect the onset of puberty and impact fertility, although the hypothalamus–pituitary axis appears to remain intact for many, and delayed puberty is associated with increased luteinising hormone and follicular stimulating hormone. 6 Other contributing factors to the late effect of subfertility include sociopsychological and sexual effects of cancer. 16 The rate of primary ovarian insufficiency (POI) in girls and women who are treated for haematological malignancies either pre-pubertal or during reproductive years has been shown to be up to 50% following chemotherapy, and 70–100% for those who receive SCT, 17 and alkylating agents have been shown to cause most effect.17–19 The American Society of Clinical Oncology recommend clinicians explain the risk for infertility when consenting to these treatments.17,20
Studies indicate that pregnancy outcomes for cancer survivors are worse than those for the general population, including miscarriage, low birth weight infants, preterm birth and stillbirth, 4 and that these may be secondary to uterine damage.12,21 A retrospective cohort study performed in Scotland calculated a standardised incident ratio (SIR) of 0.62 (95% CI [0.60–0.63]) for cancer survivors achieving pregnancies when compared with matched controls. This group investigated associations with specific cancers, including an SIR of 0.48 (95% CI [0.42–0.54]) for those who had leukaemia and 0.67 for both those who had Hodgkin lymphoma (95% CI [0.62–0.73]) and non-Hodgkin lymphoma (95% CI [0.58–0.77]). Although the authors did not have access to detailed treatment regimes for the women included in the study, they observed adjusted hazard ratios for subsequent first pregnancy for those who received chemotherapy alone, radiotherapy alone, or combined chemotherapy and radiotherapy of 0.43 (95% CI [0.34–0.53]), 0.66 (95% CI [0.50–0.86]), and 0.36 (95% CI [0.29–0.47]), respectively. 16
Relatively little is known about pregnancy outcomes for women with a history of HSCT, with or without TBI. The European Group for Blood and Marrow Transplantation estimated a low annual birth rate for BMT survivors at 1.7 per 1000. 22 TBI is associated with disruption to uterine vasculature and uterine volume, 12 and has been shown to reduce uterine volume to 40% of a normal adult size.23,24 Iskender et al. (2022) recently reported on pregnancy and pregnancy outcomes for 83 people who had undergone SCT between 2009 and 2020. Sixty-nine of these women did not have a pregnancy, of which 48 reported that they did not want to become pregnant, 21 of these had tried to conceive, and 11 had entered menopause following HSCT. The study compared outcomes of 18 pregnancies among the 14 women who did conceive with a control group of 180 women who were randomly selected from the maternity database for those who had birthed at their hospital between 2016 and 2021, and found an increase in the cumulative incidence of obstetric complications in the HSCT group. 4
The aim of this study was to determine current prenatal and antenatal care offered to women in the United Kingdom who conceive or plan to conceive having had a BMT, with or without TBI, through dissemination of a UK-wide survey of clinicians. We hypothesised that there would be a wide variation in knowledge of the specific pregnancy risk factors for these women and the prenatal and pregnancy care provided.
Methods
Funding
This study is jointly funded by Action Medical Research/Borne.
Design
A cross-sectional survey to explore current prenatal and antenatal care offered to women in the United Kingdom who conceive or plan to conceive having had a BMT, with or without TBI. The survey consisted of 11 questions (Figure 1), accessed via an electronic link and created and managed using Research Electronic Data Capture (REDCap) software, hosted at the University of Bristol. REDCap is a secure, web-based software platform which has been designed to support data capture for research studies.25,26 The items included in the survey were devised following review of the literature and consensus between the co-authors, who are experts in the specialities caring for women who conceive following BMT ± TBI. The electronic link for the survey was shared on social media, at relevant conferences, clinical groups and societies, including British Maternal and Fetal Medicine Society, British Society of Blood and Bone Marrow Transplant, Children's Cancer and Leukaemia Late Effects Group and MacDonald Obstetric Medicine Society.
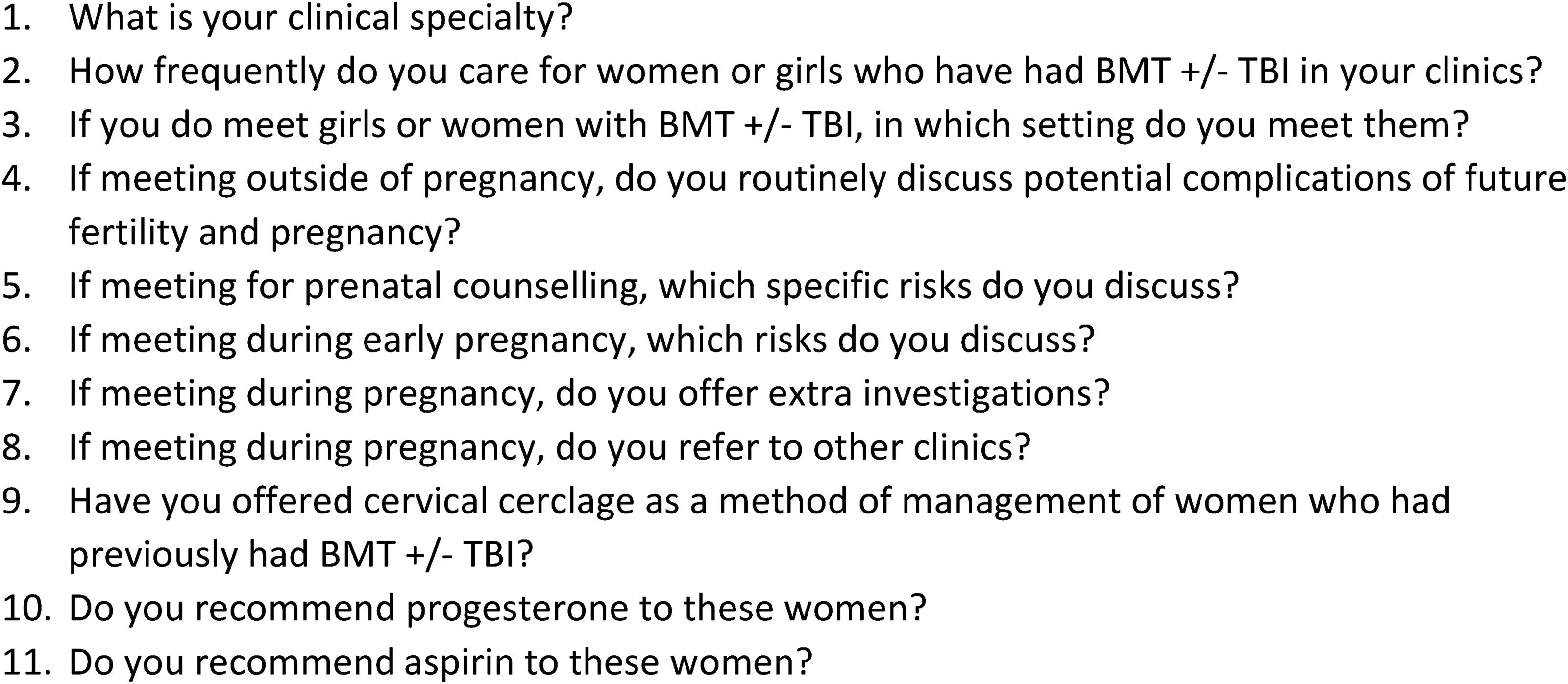
Questions included in the survey.
The study target was to collate at least 40 responses from those involved in the care of women who had previously had BMT ± TBI, including haematologists, obstetricians, gynaecologists, and reproductive medicine specialists. The survey was opened on 22nd October 2020 and closed on 21st October 2021.
Data analysis
Descriptive statistics (counts and proportions) were used to analyse the data.
Results
Participants
Forty-seven participants anonymously completed the online survey between 22nd October 2020 and 21st October 2021. Participants had a range of relevant clinical experience and backgrounds (Figure 2).
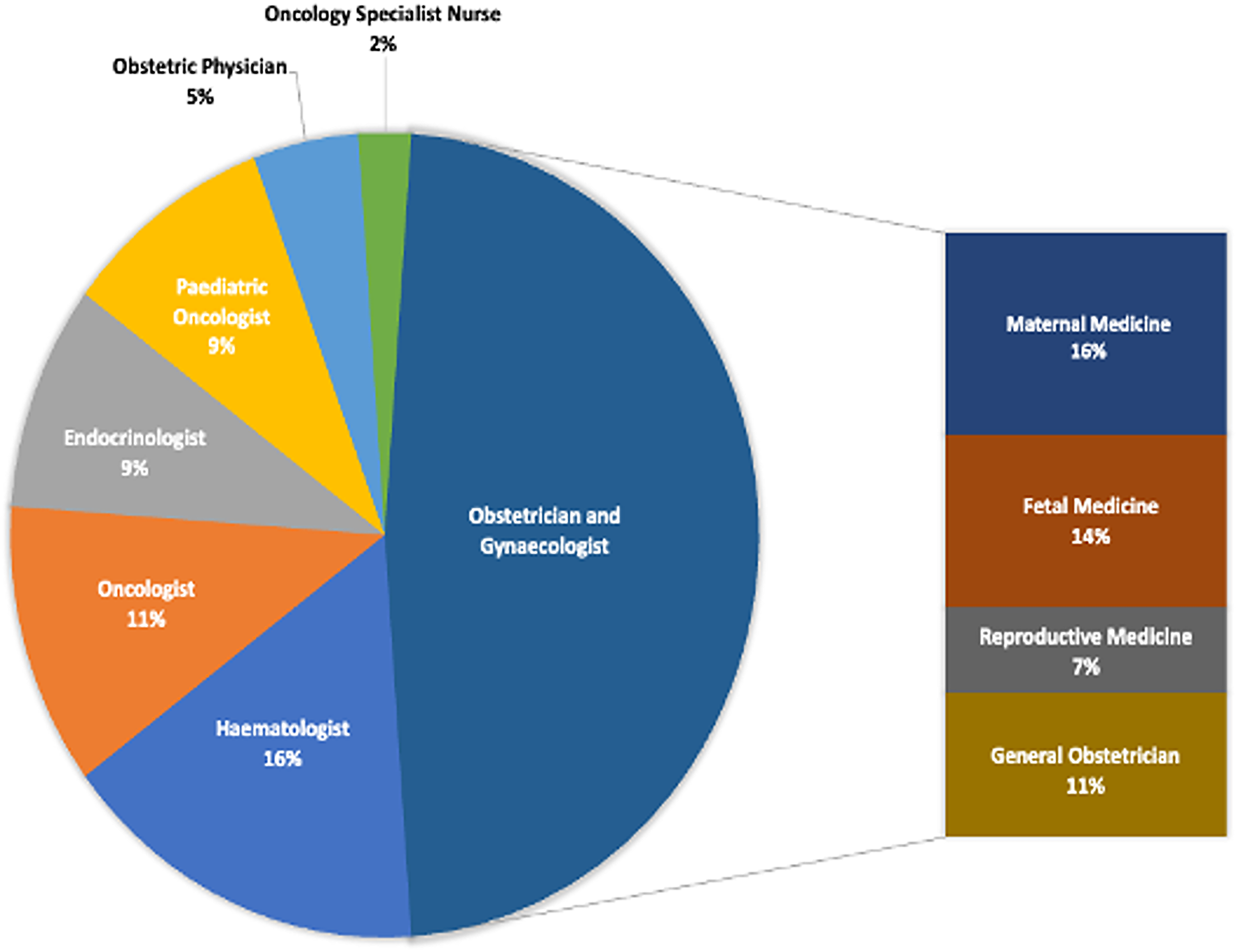
Clinical specialty of responders.
How frequently do you care for women or girls who have had BMT ± TBI in your practice?
Of all responders, 43% (20/47) saw women or girls with previous BMT ± TBI at least monthly, 15% (7/47) at least annually, 15% (7/47) less than annually, and 27% (13/47) never. Of those responders who were specialists in obstetrics and gynaecology, 13% (3/23) met this women or girls group at least monthly, 13% (3/23) at least annually, 26% (6/23) less than annually, and 48% (11/23) never. Those who report reviewing these women monthly were from the following specialties: haematology (5/20), oncology (4/20), paediatric oncology/late effects (4/20), endocrinology (4/20), paediatric and adolescent gynaecology (1/20), fetal medicine (1/20), and subfertility/reproductive medicine (1/20). Of the 13 responders who reported never seeing these women: five (5/13) were fetal medicine specialists, three maternal medicine specialists (3/13), two obstetrician and gynaecologists (2/13), two oncologists (2/13), and one subfertility/reproductive medicine specialist (1/13).
In which setting do you meet them?
Of the 34 participants who did review women following BMT ± TBI, eight (24%) consulted in antenatal clinics (two obstetric physicians, four maternal medicine specialists, one subfertility specialist, three obstetricians, one fetal medicine specialist), one in paediatric and adolescent gynaecology (PAG) clinic, five in preconception clinic (two obstetric physicians, one MM, one FM, one obstetrician), 19 reviewed this women or girls group in late effects clinics (four oncologists, four endocrinologists, four haematologists, three paediatric oncologists, specialist nurse, two reproductive medicine specialists, and one PAG specialist), eight in haematology clinics (five haematologists, one endocrinologist, one oncologist, and one paediatric oncologist), two oncology clinics (paediatric oncologist, one endocrinologist), and two in reproductive medicine clinics (two reproductive medicine specialists).
If meeting outside of pregnancy, do you routinely discuss potential complications of future fertility and pregnancy?
Of the 34 participants who did review this women or girls group outside of pregnancy, 23 (68%) routinely discussed potential complications of future fertility and pregnancy (three endocrinologists, five haematologists, two subfertility specialists, one general obstetrician, one fetal medicine specialist, two obstetric physicians, and three paediatric oncologists, one consultant nurse, one PAG, four oncologists). Specific responses to this question included: “Ovarian function; premature ovarian insufficiency (POI) and avoidance of fertility delay; hormone replacement therapy; contraception; effects of radiation on the endometrium and uterus; risk of midtrimester pregnancy loss; current understandings of implications of treatment; impact of pregnancy on late effects and vice-versa; options for having children.” “Egg donation in the majority” “Risk of infertility” “If receiving TBI I would discuss with women or girls, infertility and early menopause” “Chemotherapy and/or radiotherapy (TBI) may impair fertility, it can reduce the ovarian reserve and lead to an earlier menopause. TBI can cause complex pregnancy.”
If meeting for preconception counselling, which specific risks do you discuss?
Fourteen participants provided a response for this question. One remarked that as they work with children under 17 years of age, they do not perform preconception counselling; one that they would refer to a specialist fertility clinic post-transplant for preconception discussions and one that they would refer to maternal medicine colleagues for preconception counselling. Risks discussed included need to optimise their health before conception, risk of preterm birth, fetal growth restriction, early and late miscarriage, need for increased surveillance of the pregnancy.
A further response was: “I only look after children and prior to transplant discuss risks of infertility and if they do become pregnant need for specialist input but at this time point do not go into further details as there are so many other issues to discuss and for many families, pregnancy seems something very far away for their daughter at that time. I am likely to discuss it in more detail in situations where the girl is an older teenager or where the decision to proceed with transplant is not essential, for example with thalassaemia.”
If meeting during early pregnancy, which risks do you discuss?
Twenty-five of the participants responded to this question, and of these 84% (21/25) would discuss the risk of preterm labour; 64% (16/25) late miscarriage; 60% (15/25) fetal growth restriction; 56% (14/25) risks for maternal health other than cancer; 28% (7/25) need for irradiated blood if transfusion required; 24% (6/25) risk to their cancer; 16% (4/25) fetal cancer risk (Figure 3).
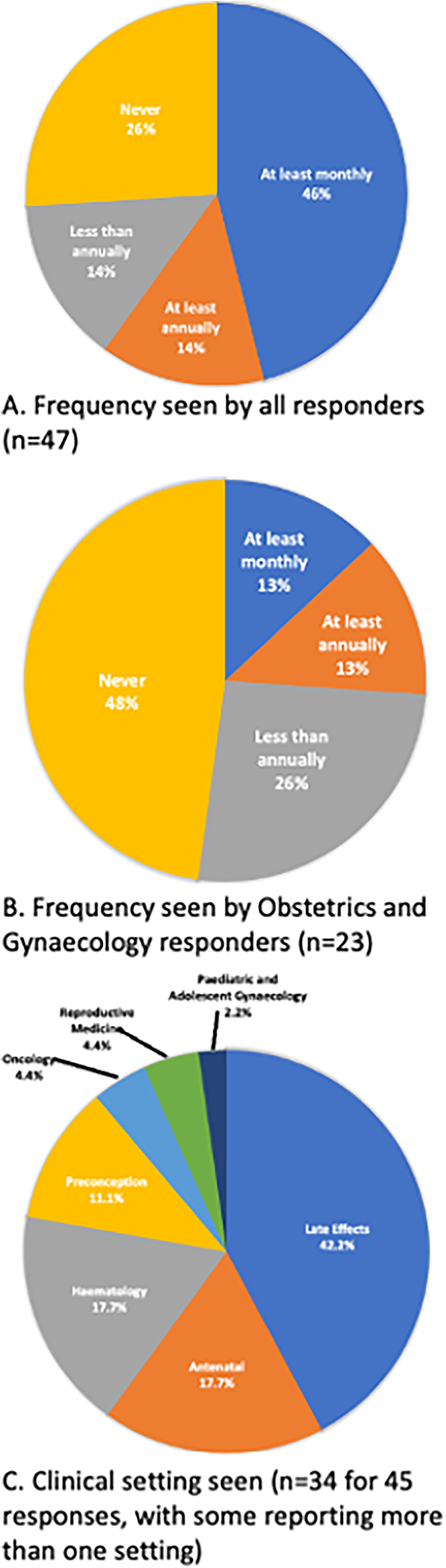
(A). Frequency seen by all responders (n = 47: 43% (20/47) saw women or girls with previous BMT ± TBI at least monthly, 15% (7/47) at least annually, 15% (7/47) less than annually, and 27% (13/47) never); (B). Frequency seen by obstetrician and gynaecologist responders (n = 23: of those responders who were specialists in obstetrics and gynaecology, 13% (3/23) met this patient group at least monthly, 13% (3/23) at least annually, 26% (6/23) less than annually, and 48% (11/23) never); (C). Clinical setting seen (n = 34 for 45 responses, as some reported review in more than one setting): Late Effects Clinic 42.2% (19/45: four oncologists, four endocrinologists, four haematologists, three paediatric oncologists, specialist nurse, two reproductive medicine specialists, and one PAG specialist); antenatal clinic 17.7% (8/45: two obstetric physicians, four maternal medicine specialists, one subfertility specialist, three obstetricians, one fetal medicine specialist); Haematology Clinic 17.7% (8/45: five haematologists, one endocrinologist, one oncologist, and one paediatric oncologist); Preconception Clinic 11.1% (5/45: two obstetric physicians, one MM, one FM, one obstetrician); Oncology Clinic 4.4% (2/45: paediatric oncologist, one endocrinologist); Reproductive Medicine Clinic 4.4% (2/45: two reproductive medicine specialists); and Paediatric and Adolescent Gynaecology Clinic 2.2% (1/45: PAG specialist).
If meeting during pregnancy, do you offer extra investigations?
Thirty participants responded to this question, and of these, 87% would offer extra investigations and these included: 81% (21/26) maternal echocardiogram; 50% (13/26) renal and liver function; 50% (13/26) serial fetal growth scans; 27% (7/26) cervical length measurement; 27% (7/26) midstream urinalysis; 15% (4/26) high vaginal swab; 15% (4/26) NAAT test for Chlamydia; 11% (3/26) low vaginal swab; and 4% (1/26) bone density (DEXA) scan (Figure 4).
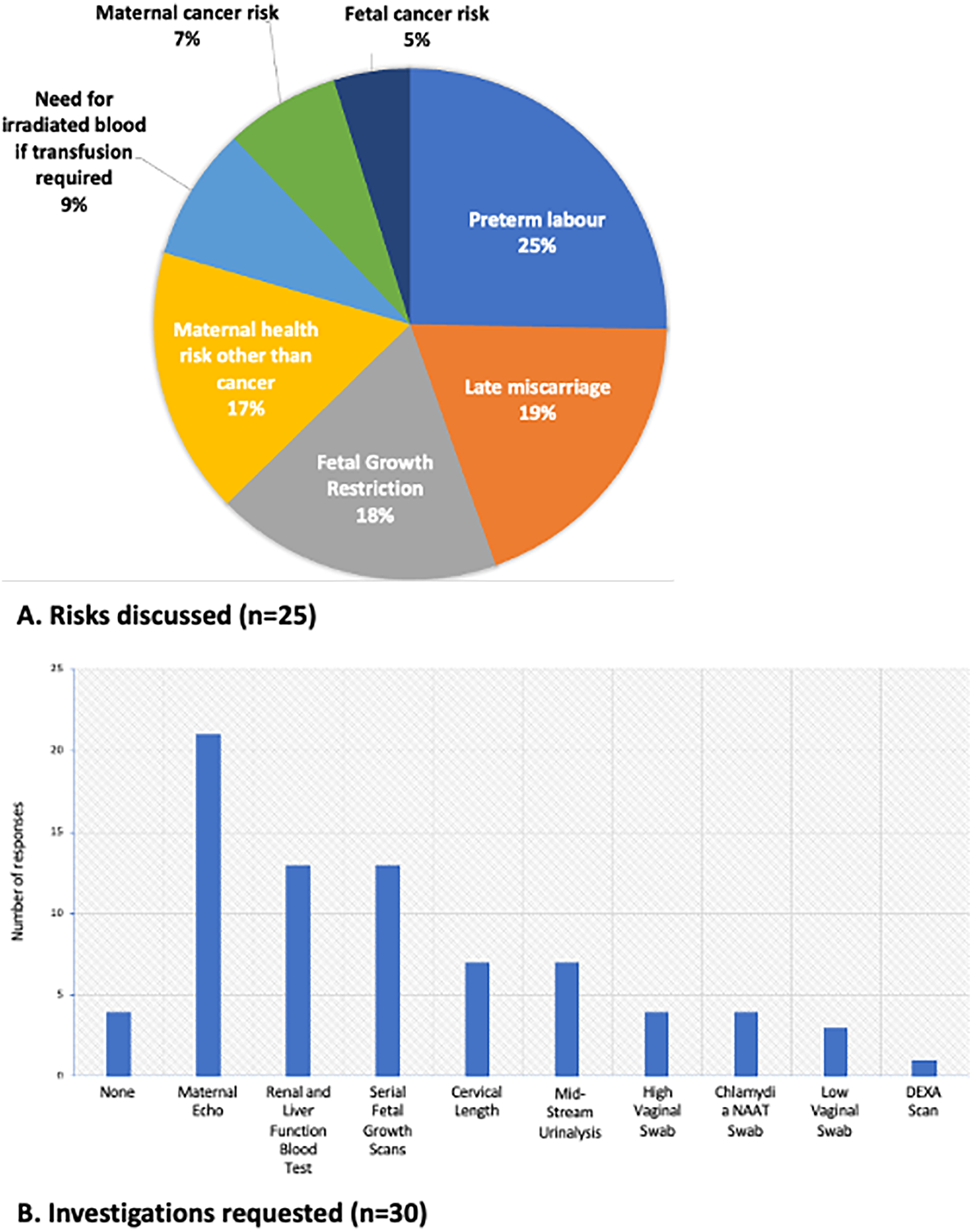
(A). Risks discussed in early pregnancy (n = 25); (B). Investigations requested (n = 30).
If meeting during pregnancy, do you refer to other clinics?
Eighty percent of the 30 participants who replied to this question answered that they do refer this women or girls group to specialist clinics: 88% (21/24) maternal medicine clinic; 58% (14/24) preterm birth prevention clinic; and 26% (6/24) general antenatal clinic.
Have you offered prophylactic interventions for preterm birth and fetal growth restriction in women with previous BMT ± TBI?
Of 30 participants who responded to this question, only six (20%) had previously offered cervical cerclage to reduce the risk of PTB to women who had previously had BMT ± TBI (Figure 5).
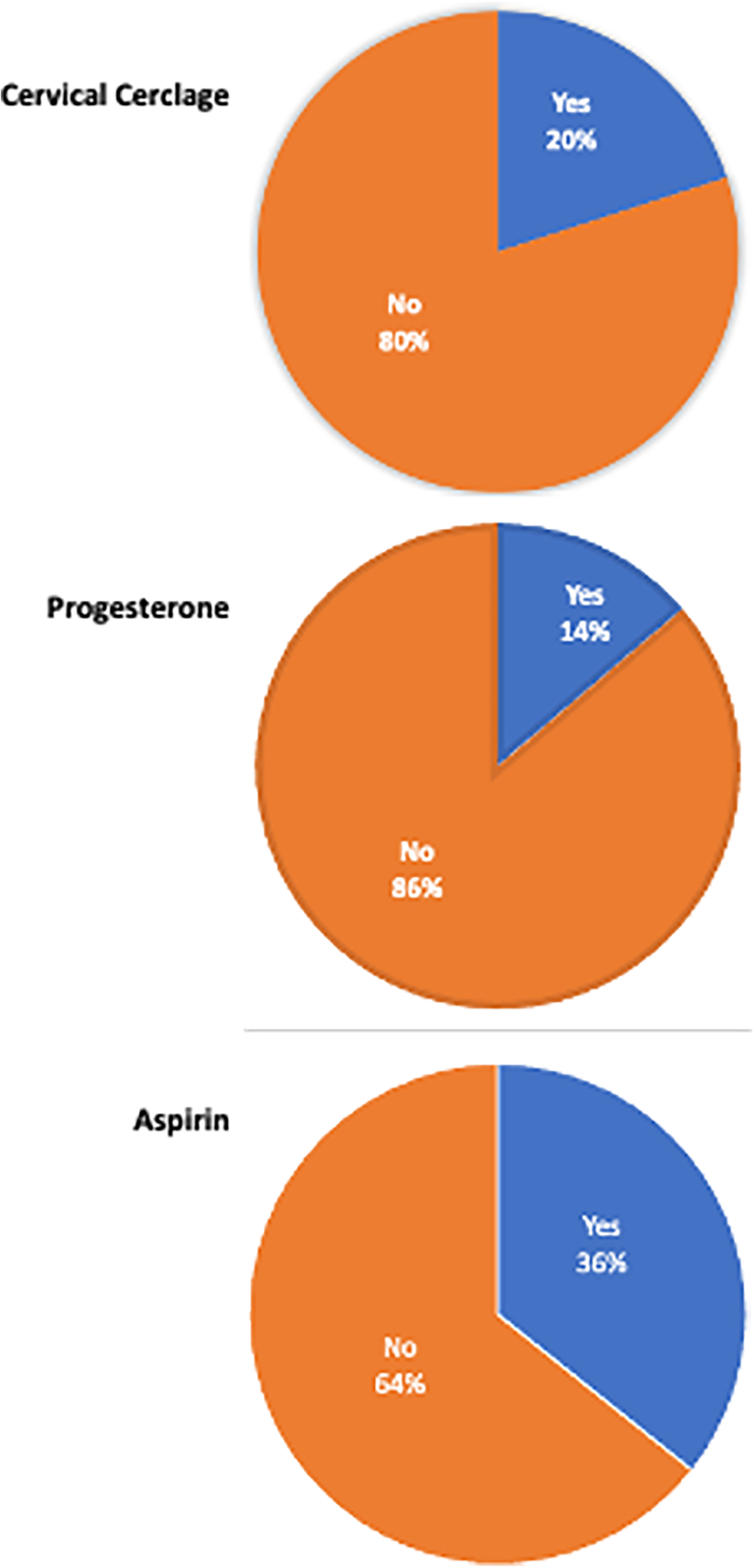
Use of cervical cerclage, progesterone and aspirin.
Fourteen percent (4/29) prescribed progesterone and 36% (10/28) prescribed low dose aspirin in this women or girls group (Figure 5).
Conclusion
To our knowledge, this is the most extensive survey of preconception and antenatal care offered to this high-risk group, with evidence of good care across the United Kingdom by clinicians. Amongst responders, early discussion regarding fertility and pregnancy was frequently reported. However, in aiming to achieve a response rate in excess of 40 participants, we adopted a targeted approach of dissemination via specialist organisations and social media groups, which may have contributed to clinicians with an interest in looking after this women or girls group being more likely to have completed the survey, and this may have influenced the results. Thirteen respondents reported that they did not review these women in their clinical practice, and therefore did not have further comments for the rest of the survey; however, this remains useful data as these respondents included oncologists, and maternal medicine, subfertility/reproductive medicine, and fetal medicine specialists, all of whom it may be expected to have reviewed these women at some point. Therefore, it is possible that women are going through maternity services without being identified as being at higher-risk. Since conducting this survey, several factors, including presentation of our pregnancy datasets to increase awareness of complications in this group, and establishment of maternal medicine networks, may have improved this identification rate.
Those who worked within the field of late effects reviewed this group most frequently, but not during pregnancy. Of those who reviewed women outside of pregnancy, it was reassuring that 68% routinely discussed potential complications of future fertility and pregnancy. Nearly half of the total responders (48.9%) were obstetricians and gynaecologists, of whom nearly half (48%) reported that they never met this women or girls group. It is not clear whether this is because they do not have women with previous BMT passing through their service, or because this risk factor is not identified during their pregnancy. The wide heterogeneity in counselling and management of women who conceive following BMT ± TBI may lead to variation in pregnancy outcomes, particularly regarding PTB prevention, and of the 30 responders who met these women antenatally, few had offered prophylactic interventions such as progesterone or cervical cerclage. This may be explained by there being limited information and recommendations available for pregnancy in this group.
It is possible that there are differences in how effects on fertility are discussed between girls and boys. A 2019 worldwide survey of the opinion and practice of 150 HCT specialists with regard to fertility preservation showed that most (87%) informed women or girls that chemotherapy, radiotherapy and SCT could impair fertility, and that 56% referred male patients for fertility preservation. Only 36% of respondents however referred their female patients, and reported that many pre-pubertal and women of reproductive age were not referred. Thus there may be barriers preventing referral of women to these services, and that referral protocols and pathways should be established. 17 This is important, as assisted reproductive technologies, including oocyte donation, can improve chances of pregnancy for those with impaired fertility secondary to cancer treatment. Options for fertility preservation prior to treatment have improved in recent decades and include oocyte cryopreservation, embryo cryopreservation, ovarian tissue cryopreservation, and transposition of ovaries.4,17
There is a need for more research and for raising awareness and the recommendations for optimised prenatal and antenatal care to be standardised in pregnant women with a history of HSCT/TBI. It is likely that there is variation from site to site; and it is possible that there is some gender inequality in how the potential impact on fertility is discussed between girls and boys, and this may impact decisions and plans regarding fertility preservation. This is important, as with improved treatments, more girls and women are surviving childhood cancers and will conceive, and it is essential that we can offer them the best care. In response to this, and funded by AMR/Borne, we are conducting retrospective data analysis and a prospective U.K. Obstetrics Surveillance Survey to further evaluate pregnancy outcomes following BMT ± TBI, and data from these studies will assist us in formulating recommendations for optimal service provision and management of pregnancies in this high-risk women or girls group. Such information is likely to be of benefit to those who receive TBI for other conditions.
Footnotes
Contributorship
MG conceived the study. All researched literature and developed the study. KB wrote the first draft of the survey and wrote the first draft of the manuscript. All authors reviewed and edited the survey and the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Action Medical Research and Borne with a generous donation from the James Tudor Foundation (Grant No. GN2818).
Guarantor
Katherine Birchenall.