
Abstract
Salmonella typhi in Australia is uncommon, with a reported incidence of less than 1 per 100,000. In pregnancy, untreated Salmonella can lead to complications including intrauterine fetal death and preterm labour. Described here is a woman who travelled home to India for a month in the second trimester of her pregnancy and contracted the illness there. She had a protracted incubation phase with the bacterium, initially having negative stool samples and then testing positive almost a month after her return. Despite a delay in antibiotic treatment, she went on to recover from her illness and have an uncomplicated vaginal delivery. S. typhi should be considered in the differential for a febrile patient with a recent travel history.
Introduction Case
A 27-year-old woman, was pregnant for the second time, and diagnosed with typhoid fever at 26 weeks of gestation. Her first pregnancy was an uncomplicated term forceps delivery, and she had no significant past medical history.
She travelled from Australia to her hometown in India from 16 + 0–20 + 1 weeks’ gestation. Her daughter developed an enteric illness while away and on return was stool culture positive for Salmonella typhi. Communicable disease contact tracing guidelines necessitated that household contacts be tested; our case was initially asymptomatic and both her and her partners’ stool samples were negative for Salmonella Sp (21 + 0 weeks).
One month later (25 + 0 weeks) she developed abdominal pain, back pain, fever, vomiting and a dry cough. She presented to hospital one week later with diarrhoea and reduced fetal movements. She was tachycardic, heart rate 133/min, febrile at 38.8°C and had bilateral upper abdominal pain. Chest X-ray demonstrated right lower lobe infective/inflammatory changes, and abdominal ultrasound was normal except for non-specific gallbladder sludge. Fetal ultrasound was reassuring. Laboratory investigations showed a normocytic anaemia, elevated CRP and elevated liver function tests (Table 1). An autoimmune and infective liver screens (ENA, ANA, neutrophil cytoplasmic antibody, SM Ab screen, cardiolipin, liver specific antibody, ceruloplasmin and alpha 1 antitrypsin) were negative except for raised bile acids 31 umol/L. Stool culture was positive for Giardia and Salmonella sp but no subtyping was performed. Given clinical improvement after four days of conservative management and rehydration, the Infectious Diseases service advised antibiotics were not required. She was discharged at 27 + 3 weeks with a plan for outpatient review with repeat laboratory investigations and stool culture.
Laboratory findings on admission and during second hospital stay.
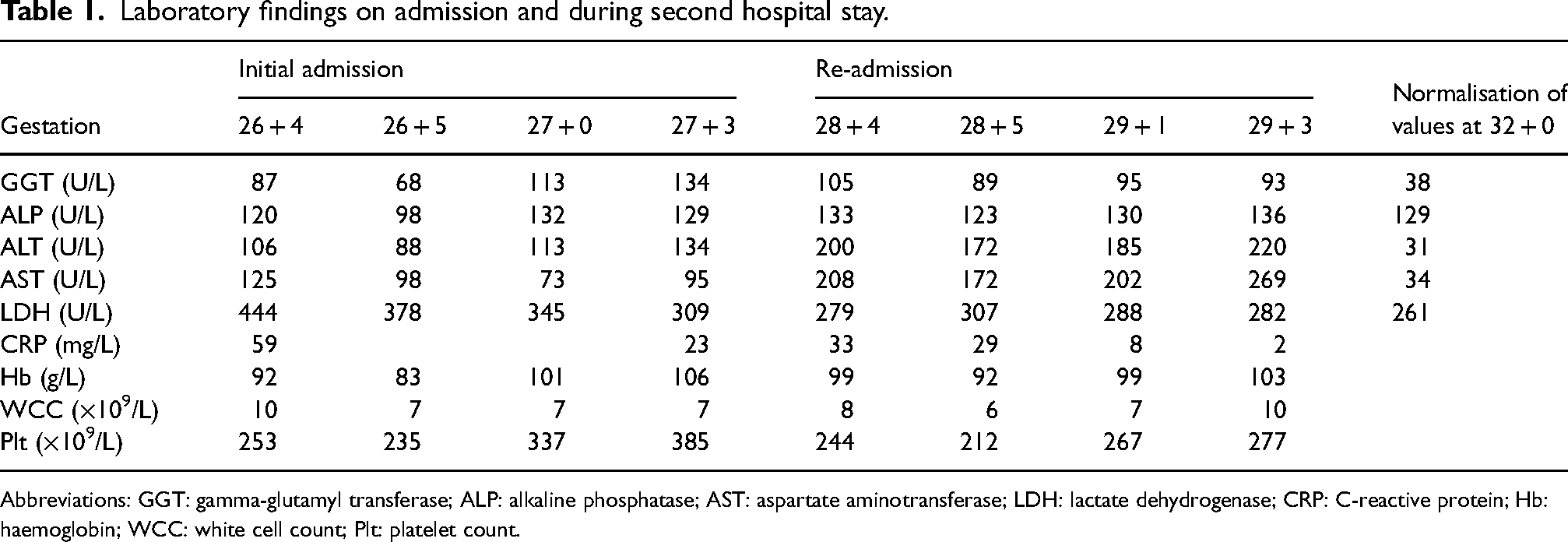
Abbreviations: GGT: gamma-glutamyl transferase; ALP: alkaline phosphatase; AST: aspartate aminotransferase; LDH: lactate dehydrogenase; CRP: C-reactive protein; Hb: haemoglobin; WCC: white cell count; Plt: platelet count.
She represented at 28 + 4 weeks, tachycardic, with a heart rate of 132/min, and bilateral upper abdominal pain. Laboratory investigations are in Table 1. Repeat abdominal US showed no liver abnormalities or features of cholecystitis. Given recent travel and cough, a QuantiFERON gold test was performed which was negative. Repeat blood cultures were taken which grew Salmonella Sp after one day and subsequently subtyped as S. typhi, likewise delayed subtyping of the initial stool sample was positive for S. typhi sensitive to ceftriaxone and azithromycin and resistant to ciprofloxacin.
She was initially commenced on ceftriaxone 2 g daily and metronidazole 500 mg twice daily; once S. typhi was confirmed she was commenced on oral azithromycin 1 g daily for four days. Regular growth ultrasounds were performed and no abnormalities were detected.
The remainder of her pregnancy was complicated by:
Cholestasis managed with ursodeoxycholic acid 250 mg twice daily as bile acids peaked at 46 umol/L (severe) and she experienced severe pruritus not relieved with antihistamines and non-pharmacological interventions. We were unable to differentiate between raised bile acids due to Salmonella infection versus true intrahepatic cholestasis of pregnancy. Anaemia with a nadir of 83 g/L with low grade haemolysis – attributed to the Salmonella bacteraemia and resolved with treatment (Haptoglobin < 0.1, DAT negative, LDH and bilirubin normal, DAT and reticulocytes normal, ADAMTs 103%, autoimmune screen normal). Gestational thrombocytopenia, with a nadir of 94 × 109/L rising to 125 × 109/L postnatally.
She was induced at 39 weeks and had an uncomplicated vaginal delivery of a live male infant. The placenta was unfortunately not sent for histopathology.
Discussion
Salmonella is a food-borne bacterium transmitted to humans through ingestion of contaminated food and water, with an estimated 90 million illnesses globally per year from Salmonella sp.1,2 Disease burden is highest in low- and middle-income countries, and in returning travellers from endemic areas.3,4 The reported incidence of S. typhi in Australia is less than 1 per 100,000, compared with an incidence of up to 35 per 100,000 in Nepal or 400 per 100,000 in Ghana. 3 Its mean incubation period is 7–21 days but has been recorded as long as 30 days, and as short as three days. 5 This is interesting as the case described here was initially negative on stool testing, but developed symptoms and a subsequent positive stool sample a month later, exceeding the average incubation period of Salmonella.
The most common presenting symptom of Salmonella infection is fever (in children almost universally present, vs in 43% in adults), followed by abdominal pain (32–60%) and diarrhoea (35–84%).6–9 Other symptoms can include cough, headache, myalgia and arthralgia.7,8,10–12 Common laboratory findings include anaemia (14–44%), elevated CRP (80–100%), transaminitis (47–82%) and thrombocytopenia (16–32%).13–16 Rapid treatment of S. typhi infections reduce the chance of progression to severe disease, with complications occurring more commonly after day 10 of untreated infections – these include gastrointestinal bleeding, intestinal perforation, and cholecystitis.4,17,18 Less commonly patients can experience haemodynamic shock, bone and joint infections and myocarditis.17,19
Infection with Salmonella results from ingestion of the bacterium, after which it crosses the intestinal epithelium and disseminates systemically. Uniquely, S. typhi once inside host cells release a toxin which is then able to infect a wide range of cells. 20 In the case of pregnancy, Salmonella is hypothesised to affect fetal trophoblasts which would normally act as an additional barrier to infection. 21 Once this has occurred and the placenta is colonised, it increases the risk of placental abruption and chorioamnionitis likely due to overwhelming host immune response. 21 Thus, infection with S. typhi in pregnancy remains of concern as vertical transmission to the fetus can cause miscarriage, intrauterine fetal death, preterm labour and neonatal sepsis.21,22 Fetal outcomes appear related to gestation at the time of infection,21,23 and whether or not rapid antibiotic treatment has been initiated.23,24 There was significant delay in commencement of antibiotics in our case, because of delays in the subtyping of the Salmonella species on samples taken at presentation. Studies report rates of <5% risk of progression from gastrointestinal Salmonella infection, to Salmonella bacteraemia but this is associated with more severe complications. 25 Our case became blood culture positive on her representation to hospital.
It is well known that pregnancy reduces gut motility and biliary tract peristalsis; these adaptations also make gastroenteric infections so potent in pregnancy. The literature describes key differences between pregnant and non-pregnant females with typhoid fever with liver transaminases more commonly raised in the pregnant cohort. 26 This was seen in our case, with liver function derangement taking three weeks to resolve following completion of treatment. Pregnant women are also more likely to present with a cough than non-pregnant women. 26 The symptom of cough was a distractor in our work up, with a prominent differential initially being tuberculosis.
Conclusion
This case highlights the importance of casting a wide differential net when assessing women with fever of unknown origin in pregnancy. It is important to consider the travel history and conditions that may be endemic to the countries visited. In this case, perhaps treatment with antibiotics earlier may have prevented Salmonella bacteraemia and the prolonged hospital stay.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
Madalina Oprea
Informed consent
The patient provided verbal consent for the case to be written up and published.