
Abstract
Disseminated amoebiasis in pregnancy, though rare, can be life-threatening and mimic bacterial sepsis or inflammatory bowel disease (IBD). We report a case of maternal near-miss at 18 weeks of gestation due to amoebic colitis and liver abscess. The woman presented with fever, bloody diarrhoea, and abdominal pain, initially suspected to be bacterial sepsis, and treated with ceftriaxone. Ultrasound revealed hepatic abscesses and caecal thickening. Following massive rectal bleeding and hypovolemic shock, colonoscopy confirmed Entamoeba histolytica infection. Liver abscess drainage yielded anchovy-sauce pus, and stool, blood, and aspirate cultures were negative. Metronidazole therapy led to clinical improvement. This case highlights the importance of considering disseminated amoebiasis in pregnant women with haemorrhagic diarrhoea and sepsis. Early histopathological confirmation and targeted anti-amoebic therapy are essential for effective management, preventing severe complications such as haemorrhagic shock and liver abscess.
Introduction
Amoebiasis, caused by Entamoeba histolytica, is a parasitic infection with global prevalence but is especially endemic in regions with inadequate sanitation. While most cases are asymptomatic, invasive forms can cause dysentery and extraintestinal complications such as liver abscesses. 1 In pregnancy, altered immunity increases susceptibility to severe infections, including amoebiasis. The clinical challenge lies in its mimicry of inflammatory bowel disease (IBD) and bacterial colitis. Misdiagnosis can result in inappropriate treatment – particularly steroid use – which can exacerbate amoebic infections, leading to fulminant colitis and mortality. Diagnosis relies on clinical suspicion supported by imaging, colonoscopy, histology, and occasionally serology or PCR-based stool tests. 2 We describe a rare and severe case of disseminated amoebiasis in the second trimester, initially misdiagnosed as bacterial sepsis, resulting in a maternal near-miss due to haemorrhagic colitis and severe anaemia.
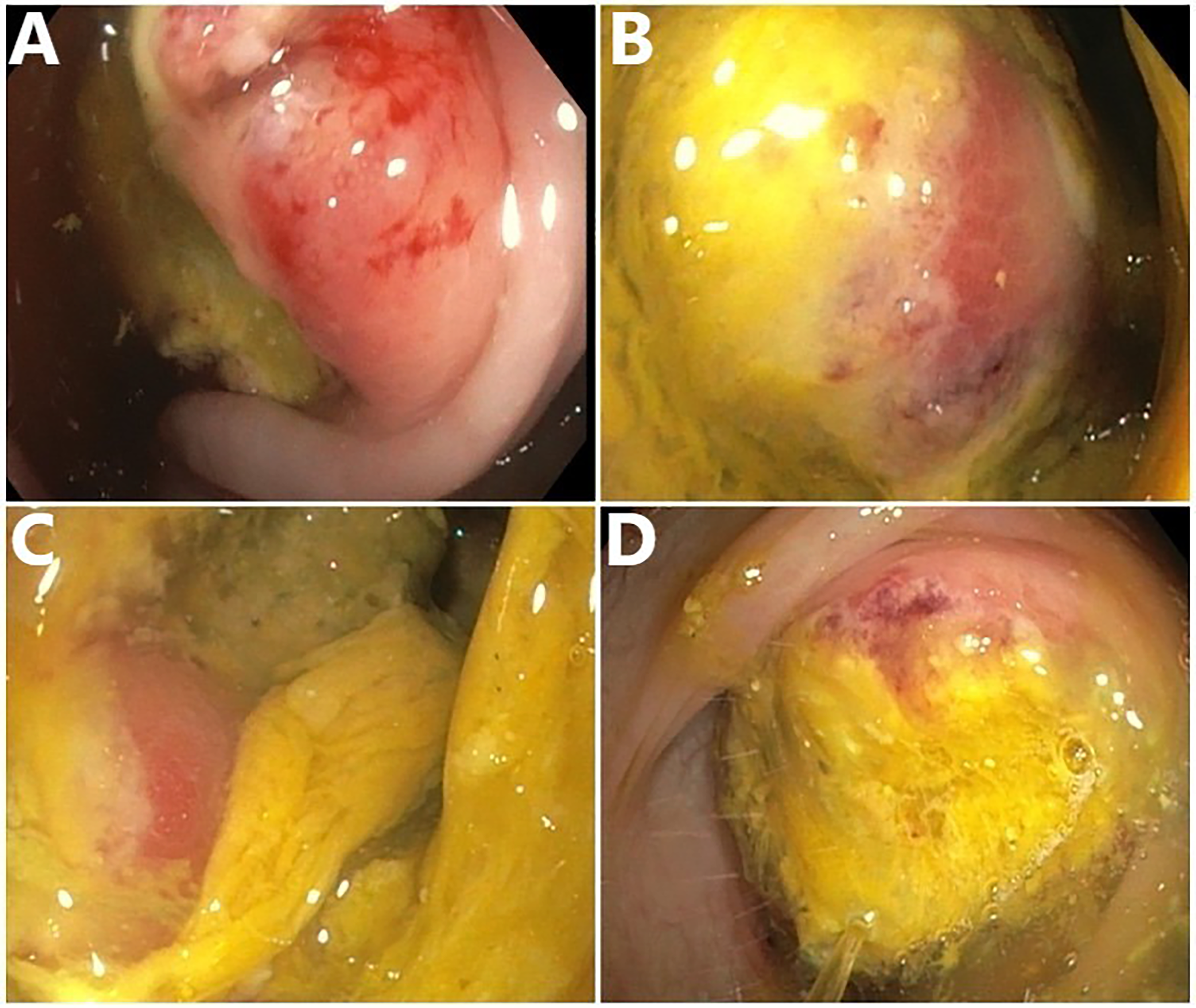
(A) Erythema and ulcerations seen at multiple colonic sites; (B–D) ulcers covered by thick yellowish exudate consistent with amoebic colitis.
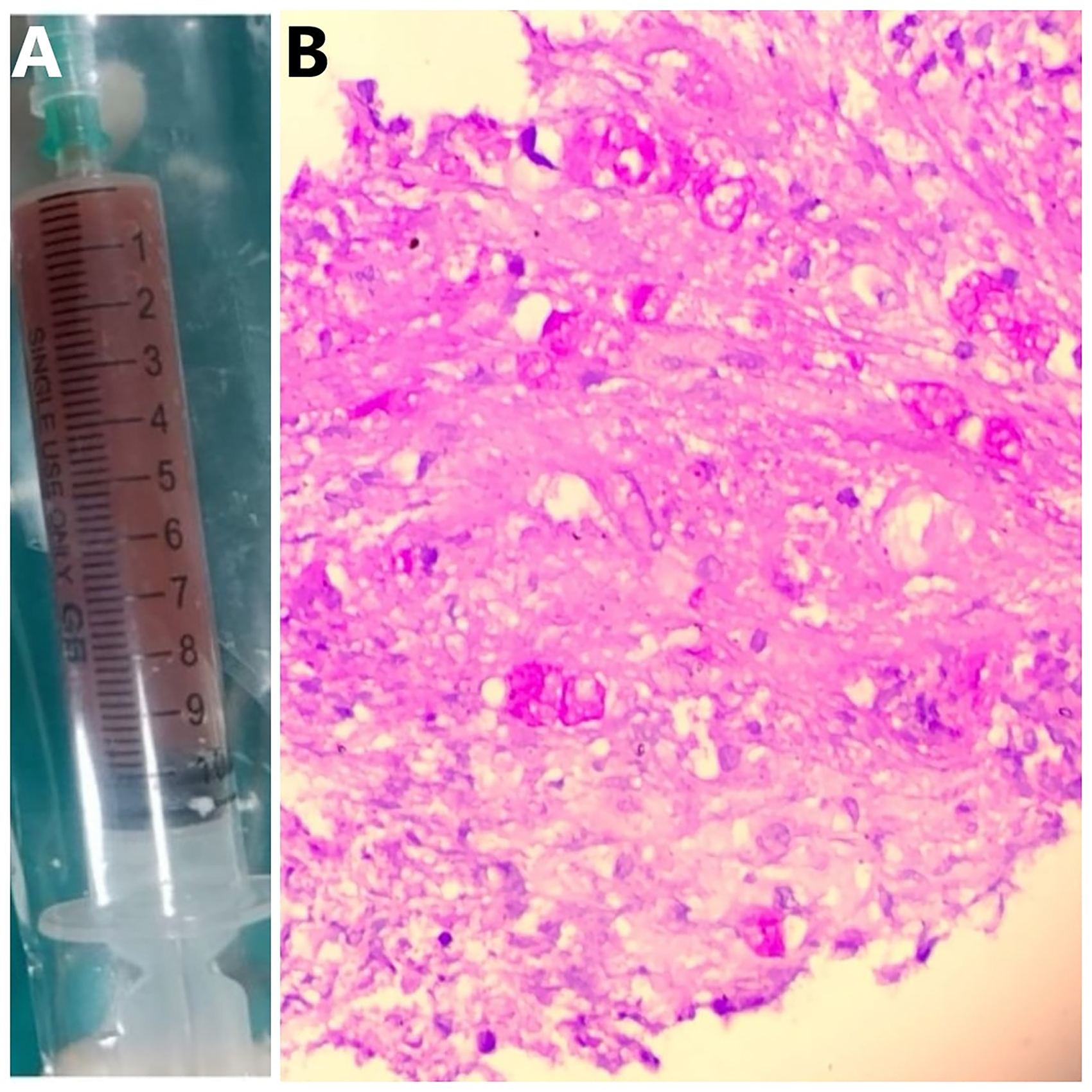
(A) Anchovy-sauce pus drained from the liver abscess, characteristic of amoebic aetiology; (B) histopathology of colonic biopsy: periodic acid–Schiff (PAS) stain highlights Entamoeba histolytica trophozoites (magenta) with granular ‘ground-glass’ cytoplasm and engulfed inflammatory cells, seen infiltrating the tissue.
Case presentation
A 34-year-old G2 woman in her second pregnancy, presented to the emergency department of our tertiary care hospital in India at 18 weeks of gestation, with a 10-day history of high-grade fever (101.4°F), bloody diarrhoea, lower abdominal cramps, and 2 kg weight loss. She also reported progressive breathlessness over the preceding 5 days. Shortly before admission, she experienced an episode of approximately 300 mL of fresh rectal bleeding. She had no significant past medical comorbidities. On examination, the woman was febrile, tachycardic (pulse 140/min), tachypnoeic (respiratory rate 40/min), and hypotensive (blood pressure 100/70 mmHg), with oxygen saturation of 95% on room air. She was clinically dehydrated and in compensated shock. Abdominal examination revealed hepatomegaly with tenderness in the right hypochondrium; there were no signs of peritonitis. Vaginal examination was unremarkable.
Initial laboratory evaluation revealed a haemoglobin of 8.2 g/dL and a total leukocyte count of 17,200/μL. Peripheral smear showed microcytic hypochromic anaemia. Serum lactate was elevated at 3.2 mmol/L, INR was prolonged at 2.0, and blood glucose was low at 3.9 mmol/L. Liver function tests showed mildly elevated AST (66.8 IU/L) with normal ALT (21.9 IU/L), total bilirubin of 1.3 mg/dL (direct 0.9 mg/dL), and normal renal function with serum creatinine of 43 μmol/L. A sepsis bundle approach was initiated with intravenous fluids, oxygen, correction of hypoglycaemia, and empirical broad-spectrum antibiotics (intravenous ceftriaxone). With resuscitation, lactate improved from 3.2 to 1.8 mmol/L. Ultrasound abdomen revealed two liver abscesses – one in segment 2 measuring 6.4 × 5.7 × 7.4 cm and another in segment 6 measuring 4.2 × 4.7 × 4.6 cm – along with diffuse circumferential thickening of the caecal wall. Obstetric ultrasound showed normal fetal parameters and amniotic fluid volume. Within 24 h, the woman had a second episode of massive rectal bleeding (∼500 mL), following which her haemoglobin dropped to 6.4 g/dL, and she developed hypovolemic shock. She was transfused with two units of packed red blood cells and four units of fresh frozen plasma. The bleeding stopped within 24 h following intravenous tranexamic acid.
Colonoscopy revealed extensive circumferential ulceration from the dentate line to 15 cm, with yellow slough and patchy erythema in the sigmoid colon (Figure 1). Histopathology of colonic biopsies showed flask-shaped ulcers with surrounding inflammation and multiple Entamoeba histolytica trophozoites on PAS staining (Figure 2B). Stool microscopy was negative for cysts or ova. Blood, liver aspirate, and sputum cultures were sterile. With a confirmed diagnosis of disseminated amoebiasis, ceftriaxone was discontinued and intravenous metronidazole was continued for 14 days. Both hepatic abscesses were drained under ultrasound guidance using pigtail catheters, yielding 400 mL of characteristic anchovy-sauce pus (Figure 2A). The woman's clinical status improved significantly, with the resolution of fever, bleeding, and abdominal pain. Fetal surveillance consisted of serial obstetric ultrasound examinations assessing estimated fetal weight and growth parameters, which consistently demonstrated appropriate interval growth for gestational age. She delivered at 38 weeks and 2 days of gestation by elective repeat caesarean section, a live female neonate weighing 2.06 kg, with no requirement for neonatal intensive care admission. The placenta was grossly normal on examination, and histopathological evaluation revealed no significant abnormalities.
Discussion
Amoebiasis due to Entamoeba histolytica is endemic in tropical and subtropical regions with poor sanitation. While often asymptomatic, it can manifest as invasive colitis or hepatic abscesses, especially in immunocompromised states like pregnancy.1–3 This woman presented with systemic inflammatory response, haemorrhagic colitis, and hepatic lesions, initially treated as bacterial sepsis. Ultrasound findings of liver abscesses and colonic thickening raised suspicion of amoebiasis, later confirmed histologically.
Systemic amoebiasis during pregnancy may have significant implications for both maternal and fetal health, primarily mediated through pregnancy-related immunological adaptations. Pregnancy is characterised by a shift toward a Th2-dominant immune response, with relative suppression of cell-mediated immunity, reduced macrophage activation, and altered cytokine profiles, which collectively increase susceptibility to invasive Entamoeba histolytica infection and more severe disease manifestations.4,5 Although direct placental invasion by E. histolytica has not been well established, systemic maternal illness can adversely affect placental function indirectly through severe inflammation, anaemia, hypovolemia, and hemodynamic instability. These factors may compromise uteroplacental perfusion, increasing the risk of fetal growth restriction, preterm birth, or fetal hypoxia. 1 In addition, prolonged maternal fever and systemic inflammatory response can further disrupt placental oxygen and nutrient transfer. Despite these theoretical risks, timely maternal stabilisation, appropriate antimicrobial therapy, and close antenatal surveillance can mitigate adverse fetal outcomes, as demonstrated in this case, where fetal growth remained appropriate, and a favourable neonatal outcome was achieved.
The clinical similarity between amoebic colitis and IBD or bacterial enteritis complicates diagnosis. Symptoms such as fever, abdominal pain, bloody diarrhoea, leukocytosis, and elevated liver enzymes are common to both. On colonoscopy, both can show mucosal ulceration and inflammation. However, amoebic colitis typically presents with discrete flask-shaped ulcers, while IBD shows continuous mucosal involvement with pseudopolyps in ulcerative colitis or skip lesions in Crohn's disease. Histopathological examination remains the gold standard for differentiation: E. histolytica trophozoites are PAS-positive and may be seen invading the colonic wall, which is not a feature of IBD.1,6,7 Misdiagnosis may lead to inappropriate use of corticosteroids, worsening amoebic infection and even precipitating fulminant disease, as documented in the literature. 8 This underscores the diagnostic importance of colonoscopy and biopsy, especially when stool microscopy is negative and cannot differentiate pathogenic from non-pathogenic Entamoeba species.
Massive rectal bleeding with hypovolemic shock in this woman met the WHO criteria for maternal near miss. Although rare in amoebic colitis, such bleeding has been reported. Colonoscopy remains essential, showing typical flask-shaped ulcers and PAS-positive trophozoites. The liver is the most common site for extraintestinal spread. While most abscesses respond to metronidazole, drainage is advised for large, left-lobe, or persistent lesions – as seen here with bilateral abscesses requiring drainage. Treatment includes metronidazole, a tissue amoebicide, followed by a luminal agent such as paromomycin. However, due to limited safety data regarding its use in pregnancy, paromomycin was not administered in this case. 1 Nonetheless, she responded well to systemic therapy alone. Invasive amoebiasis during pregnancy may cause adverse outcomes like preterm delivery; however, this woman recovered without fetal compromise, likely due to early diagnosis and multidisciplinary care. Timely recognition and intervention can be lifesaving for both mother and fetus.
Conclusion
Disseminated amoebiasis in pregnancy is a rare but critical differential diagnosis in women presenting with bloody diarrhoea and signs of sepsis. Misdiagnosis or delayed recognition may lead to catastrophic outcomes, particularly if immunosuppressive agents are erroneously administered. Clinicians in endemic areas must remain vigilant and consider invasive amoebiasis early, especially when conventional treatments fail or when liver abscess coexists with colitis. Colonoscopic biopsy and targeted antimicrobial therapy are cornerstones of effective management, and a multidisciplinary approach is essential to ensure maternal and fetal safety.
Footnotes
Acknowledgment
None
Ethical approval
This case report was conducted in accordance with institutional ethical standards.
Informed consent
Written informed consent was provided by the patient for publication of this article.
Authorship
All authors have made substantial contributions to the conception, design, clinical management, drafting, and/or critical revision of the manuscript. All authors reviewed and approved the final version and agree to be accountable for the work.
Contributorship
Avantika Gupta: conceptualisation, clinical management, supervision, and critical review of manuscript. Satish Choudhury: case documentation, literature review, manuscript drafting, and correspondence. Piyush Pathak: gastroenterological evaluation, colonoscopy, and interpretation of findings, review and input on gastroenterology-related content, and manuscript preparation. Diksha Singla: patient follow-up, data collection, and manuscript preparation. Aman Kumar: radiological assessment, liver abscess drainage guidance, imaging interpretation, and manuscript preparation. Tanya Sharma: histopathological analysis, photomicrograph preparation, interpretation of biopsy findings, and manuscript preparation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
Avantika Gupta is the guarantor of this manuscript and accepts full responsibility for the content.