
Abstract
Background
Renal tubular acidosis (RTA) is a disorder of renal acid–base regulation causing normal anion gap metabolic acidosis. Among its three types, distal RTA (dRTA) is the most common form.
Methods
This retrospective case series included pregnancies complicated by RTA managed at Fernandez Hospital, Hyderabad, India, between 2008 and 2024. Maternal and perinatal outcomes data were obtained from medical records.
Results
Among 133,542 deliveries, 19 pregnancies were complicated by RTA, giving an incidence of 0.014%. All cases were Type I dRTA, with 84% secondary to connective tissue disorders, predominantly Sjögren's syndrome. Recurrent hypokalaemic periodic paralysis was the most common complication. With early diagnosis and meticulous metabolic correction, most women achieved term deliveries with favourable maternal and neonatal outcomes.
Conclusions
Renal tubular acidosis in pregnancy may worsen due to physiological changes. Untreated disease poses risks from chronic acidosis and electrolyte imbalance. Early recognition and multidisciplinary management are crucial for optimal outcomes.
Introduction
The kidneys, together with the lungs, constitute the principal buffering systems responsible for maintaining acid–base homeostasis in the body. Renal tubules play a pivotal role in regulating fluid and electrolyte balance as well as acid–base equilibrium. Under normal physiological conditions, the kidneys maintain acid–base balance through efficient reabsorption of filtered bicarbonate and excretion of acid, primarily in the form of ammonium (NH4+).
Renal tubular acidosis (RTA) is a diverse group of inherited or acquired disorders in which the glomerular function of the kidney is well preserved, but impairment of tubular function prevents adequate hydrogen ion excretion and/or bicarbonate reabsorption, resulting in normal anion gap metabolic acidosis. 1 This results in a hyperchloremic metabolic acidosis in which more chloride anions are reabsorbed to offset the lower serum bicarbonate level and maintain electrolyte balance.
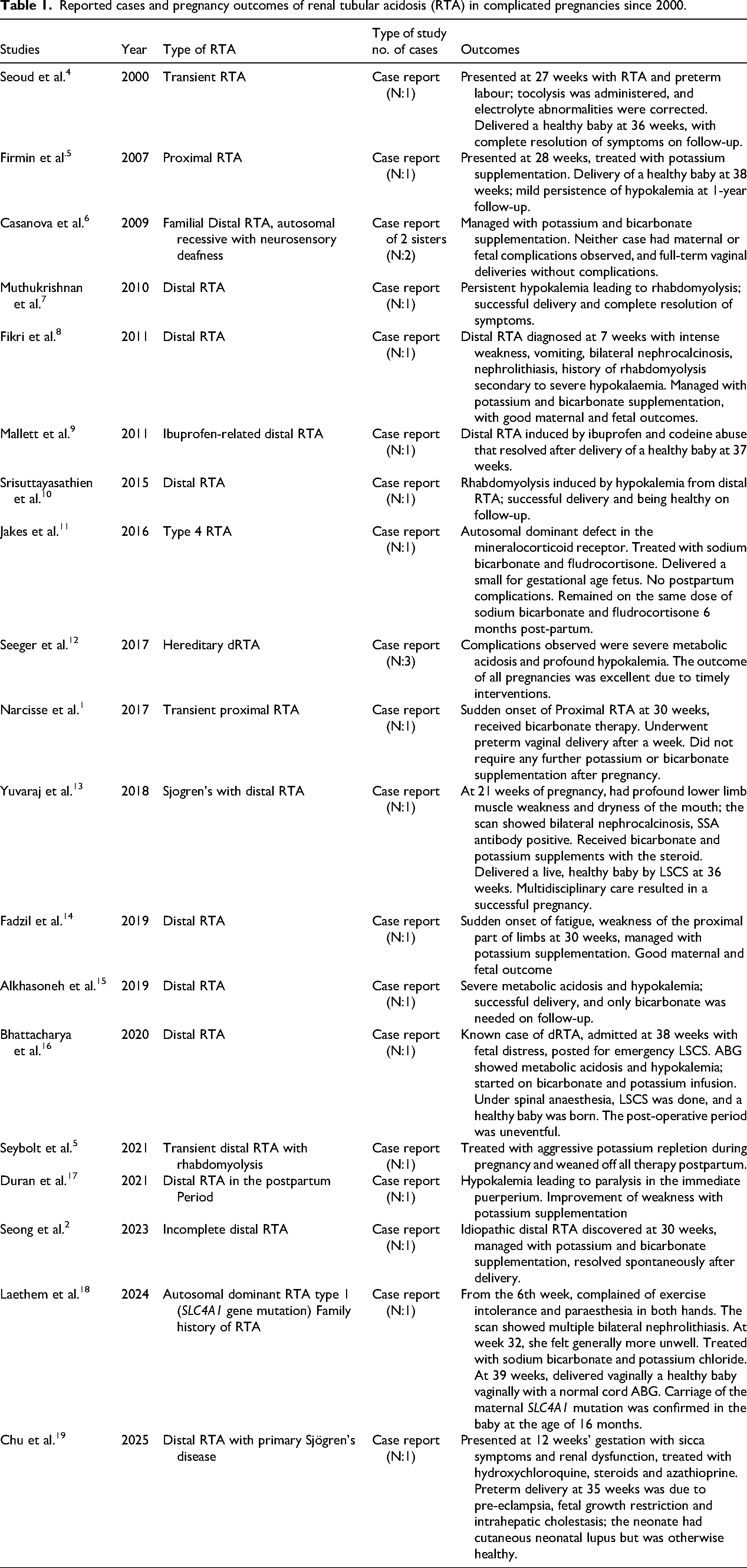
Based on its pathophysiology, RTA is divided into four subtypes, three of which are major and related to the mechanisms of renal acid–base handling: Type I or distal RTA (dRTA), Type II or proximal RTA and Type IV hyperkalaemic RTA. 2 Distal RTA (type 1) is the most common form of primary RTA. Whatever the types and causes of RTA, there is a relative or absolute acid build-up in the blood that manifests as a metabolic acidosis. The incidence of RTA is approximately 4–5 per 100,000 in the general population, and it is rarely encountered during pregnancy. But RTA, if left untreated, may cause potential risks for the mother and fetus due to chronic maternal acidosis and electrolyte imbalance. 3 Unfortunately, there is sparse literature and no standard follow-up guideline prevails in this regard. For this study, a comprehensive review of the existing literature was conducted using PubMed, Embase and Google Scholar. The search was performed using the keyword “renal tubular acidosis complicated pregnancy.” Only recent studies published after the year 2000 were included, with a focus on reported maternal and fetal outcomes. To date, the available published literature on this topic consists predominantly of isolated case reports, most of which include only one to three cases (Table 1).
Reported cases and pregnancy outcomes of renal tubular acidosis (RTA) in complicated pregnancies since 2000.
This study aims to look for the maternal and perinatal outcomes in pregnancies complicated by RTA to aid further information for this untapped region of medicine.
Methods
This retrospective case series includes pregnancies complicated by RTA that were managed and delivered at Fernandez Hospital, Hyderabad, India, from January 2008 to December 2024. As per our hospital policy, all patients are informed at the time of booking that their clinical data may be used for future research purposes, if required, and informed consent has been obtained from all participants included in the study. This approach was approved by our hospital's Institutional Ethics Committee (IEC Ref. No.: 44_2023).
The inclusion criteria comprised pregnancies complicated by RTA that were managed and delivered at our institution; cases lost to follow-up or delivered elsewhere were excluded.
Detailed data were retrospectively extracted from medical records, including maternal demographic characteristics, relevant medical and surgical history and comprehensive laboratory parameters. Information on the antenatal course, intrapartum management and postpartum follow-up was reviewed, along with maternal outcomes and perinatal outcomes such as gestational age at delivery, mode of delivery and neonatal status. The collected data were systematically analyzed to characterize the clinical profile, management strategies and outcomes of RTA-complicated pregnancies in this tertiary care setting.
Results
During the 17 years of this study, a total of 133,542 pregnant women have been delivered at our hospital. Among them, we diagnosed and managed 19 pregnancies affected by RTA, corresponding to an incidence of 0.014%. These 19 pregnancies occurred in 15 mothers.
The median age at the time of RTA diagnosis was 23 years (range: 18–28 years), while the median maternal age during pregnancy was 28 years (range: 21–33 years). In our study, all cases were Type I or dRTA, which is the most commonly encountered variant of RTA in pregnancy according to the literature. Of the 19 pregnancies, 17 cases (89%) had RTA diagnosed before conception (Figure 1). The remaining two cases had onset during pregnancy, both of which were diagnosed following an acute presentation with hypokalemic quadriparesis.
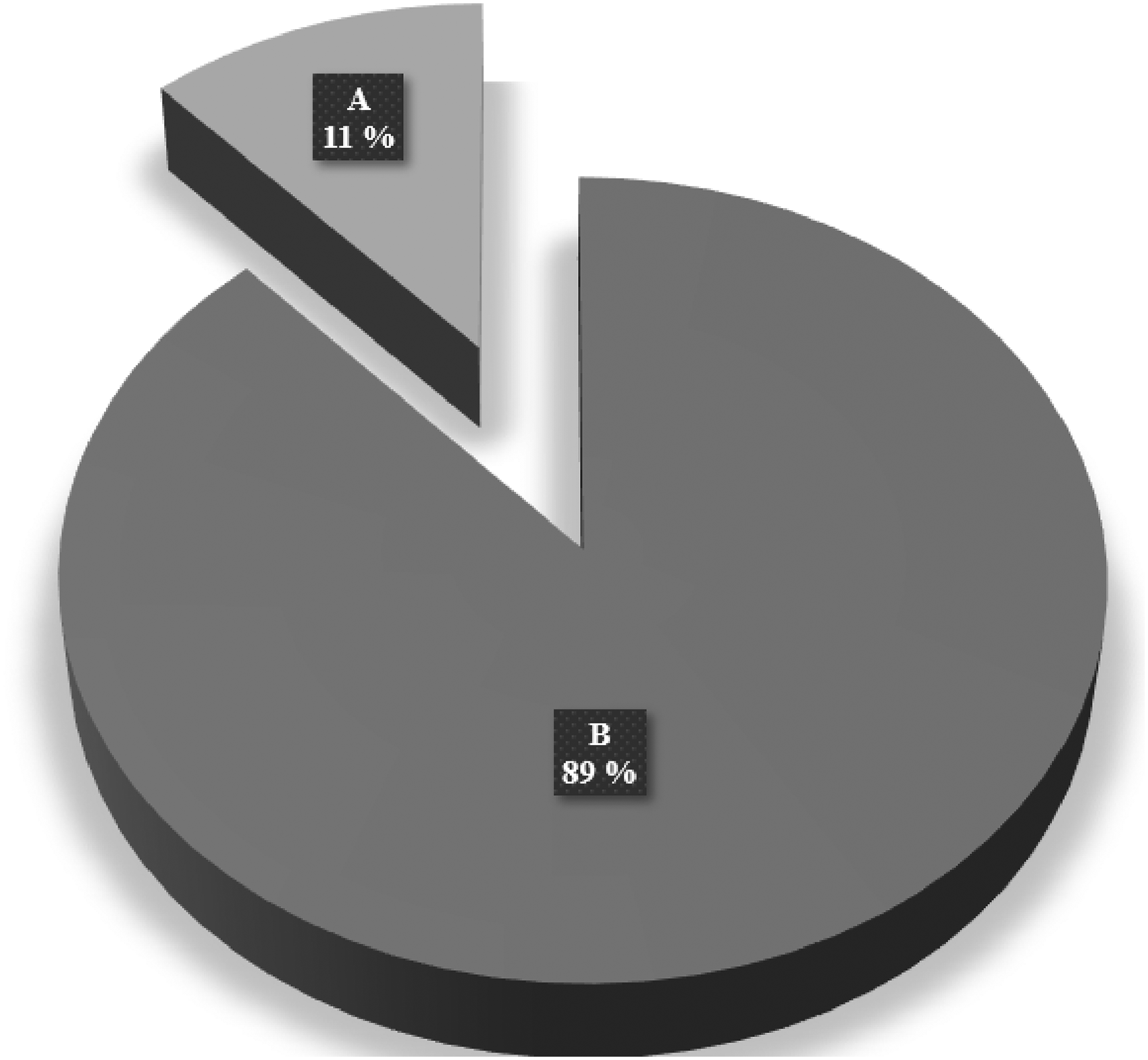
Period of onset of dRTA (A) RTA developed before conception 02/19, 11%; (B) Onset of RTA during pregnancy 17/19, 89%. dRTA, distal RTA; RTA, renal tubular acidosis.
In our study, 16 cases (84%) of RTA were secondary to connective tissue disorders, primarily Sjögren's syndrome, and three cases had an unknown aetiology (Figure 2).
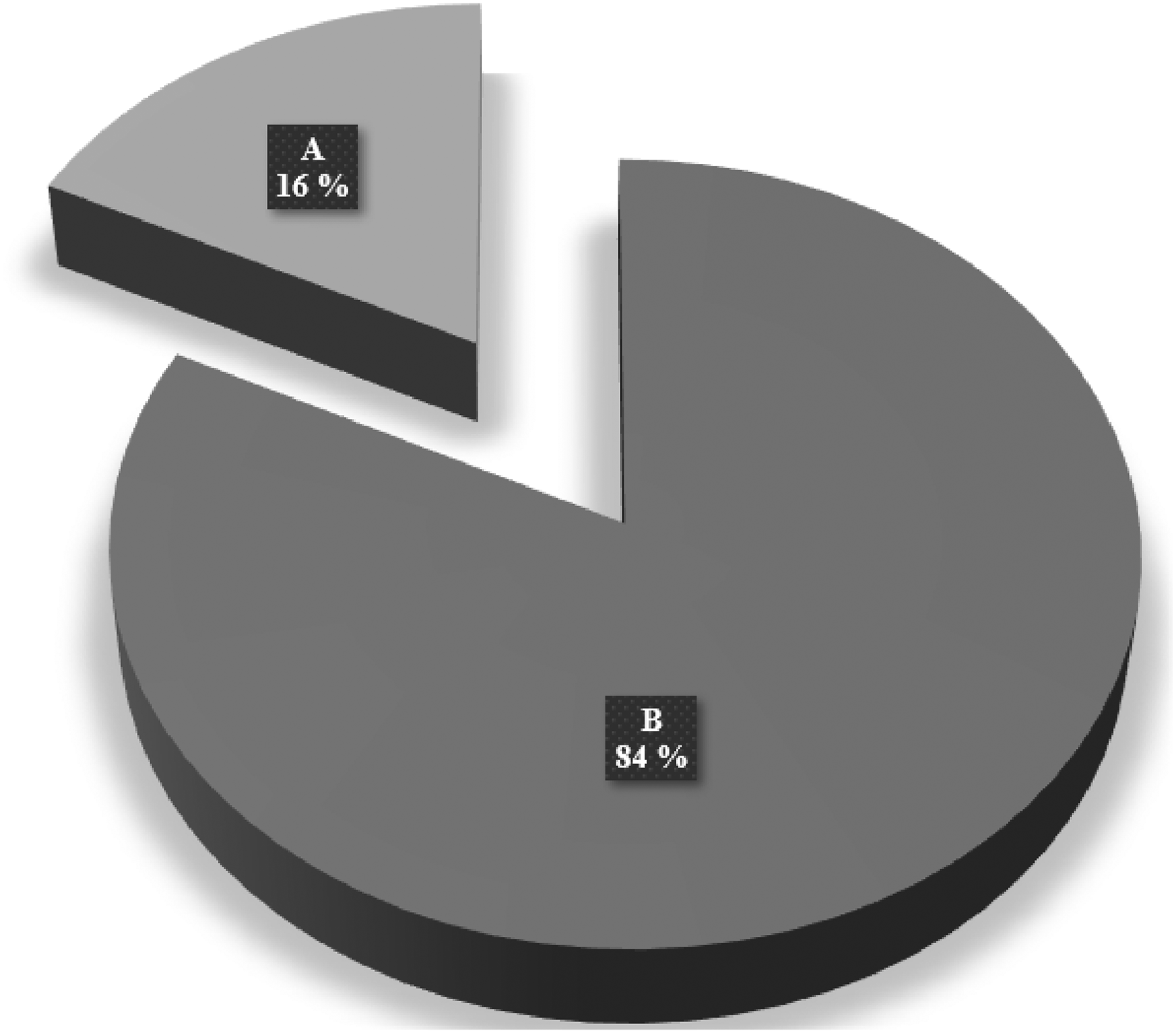
Causes of dRTA (A) unknown aetiology 03/19, 16%; (B) RTA secondary to connective tissue disorders 16/19, 84%. dRTA, distal RTA; RTA, renal tubular acidosis.
Three women (15%) had a documented history of acute kidney injury (AKI), all of which had been appropriately managed, and one patient had evidence of mild, chronic kidney disease at presentation.
The most common RTA-related complications were recurrent hypokalemic periodic paralysis, 17/19, 89%. Skeletal complications were also notable. Nearly one-third of the cases (6/19) reported a history of fractures, with pelvic fractures occurring more frequently than fractures of the long bones. This pattern is consistent with the chronic metabolic disturbances of RTA – particularly metabolic acidosis and calcium loss – leading to bone demineralization and increased fracture risk. In addition, five women (26%) had evidence of renal calculi, nephrocalcinosis or secondary hyperparathyroidism, reflecting the typical renal and metabolic complications associated with chronic dRTA, including hypercalciuria and calcium phosphate deposition (Figure 3).
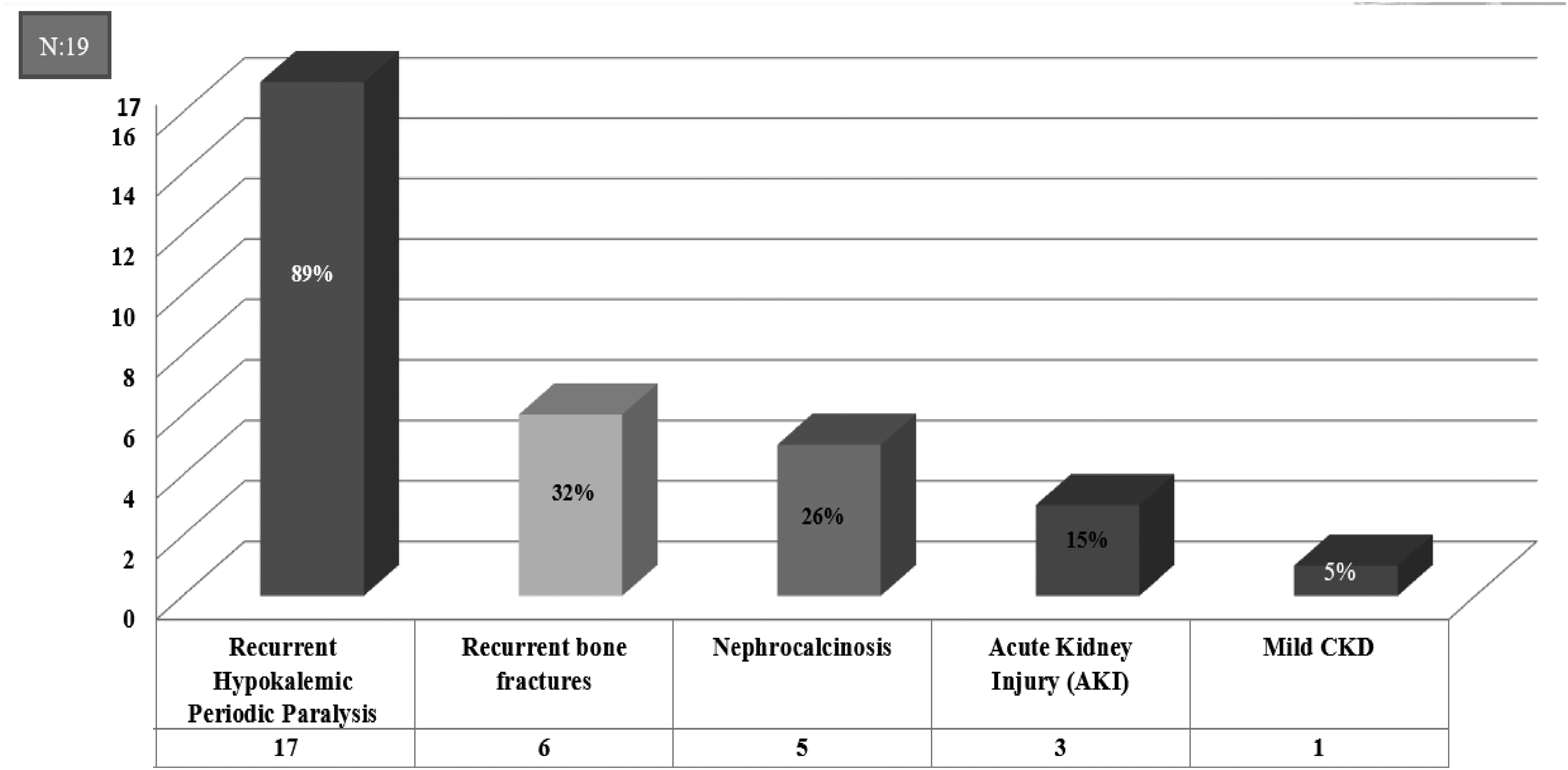
Renal tubular acidosis (RTA)-related complications: Recurrent hypokalemic periodic paralysis 17/19, 89%; Recurrent bone fracture 6/19, 26%; Nephrocalcinosis 5/19, 26%; Acute Kidney Injury 3/19, 15%; Mild CKD 1/19, 5%. CKD, chronic kidney disease.
Among the medical comorbidities, gestational diabetes mellitus was observed in 7 patients (37%), and hypothyroidism was present in 11 patients (58%). These conditions were more common than hypertensive disorder of pregnancy, which occurred in 2 cases (10%).
Of the 19 pregnancies, 10 women (53%) delivered by elective caesarean section (CS). Among these, five cases had elective CS due to renal osteodystrophy, where significant bone fragility and pelvic structural concerns made vaginal delivery unsafe. The remaining five elective CS cases were performed for the indication of a previous CS. An additional five women (27%) required emergency lower-segment CS (LSCS), most commonly for non-reassuring fetal heart rate patterns (pathological CTG). Spontaneous vaginal delivery occurred in four mothers (21%) (Figure 4).
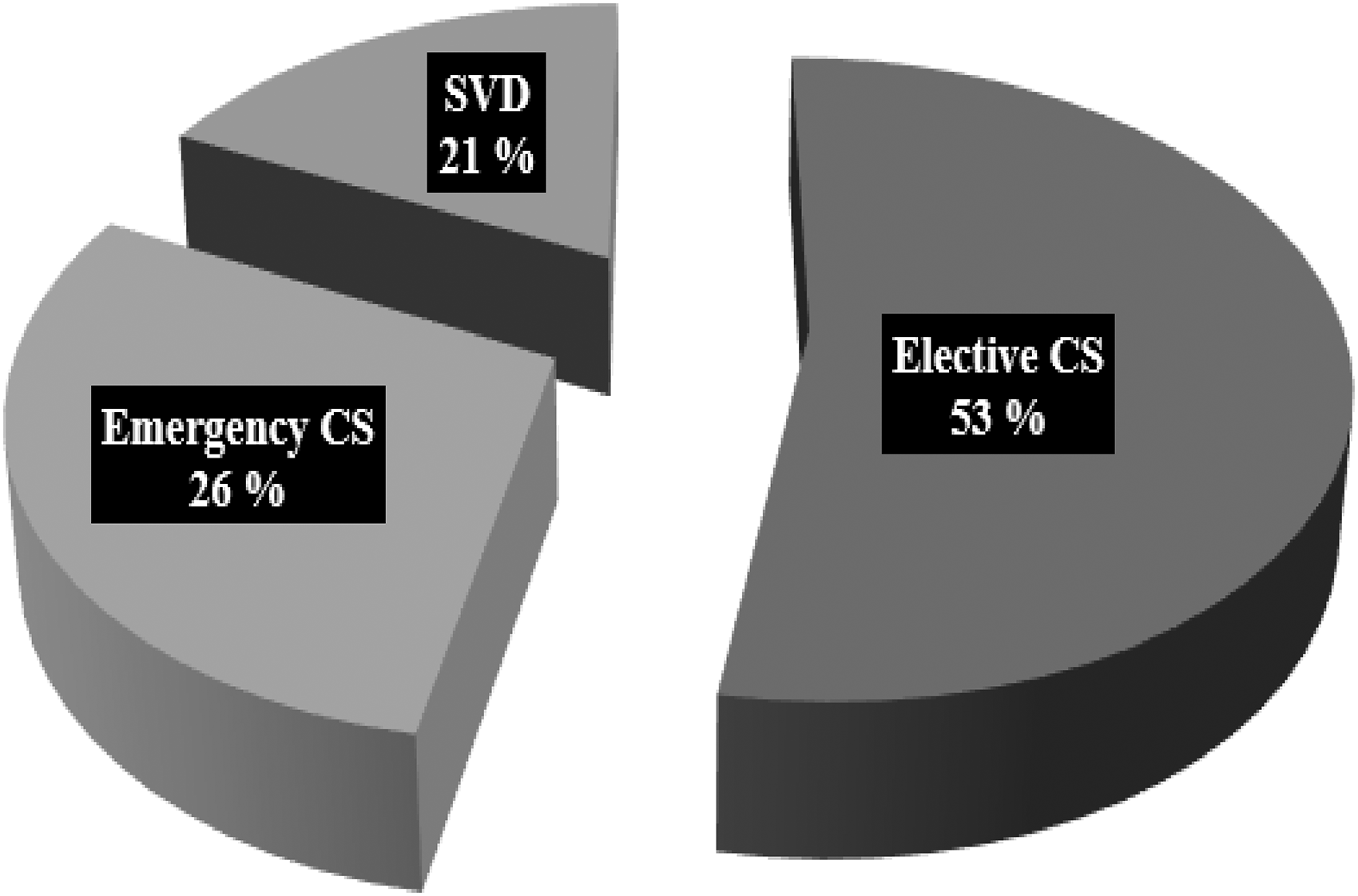
Mode of delivery: SVD 4/19. 21%; Emergency LSCS 5/19.26%; Elective LSCS 10/19, 53%. LSCS, lower-segment CS; SVD, spontaneous vaginal delivery.
Fetal outcomes were generally favourable. Only two babies were diagnosed with fetal growth restriction (FGR) and required NICU admission for observation (Figure 5).
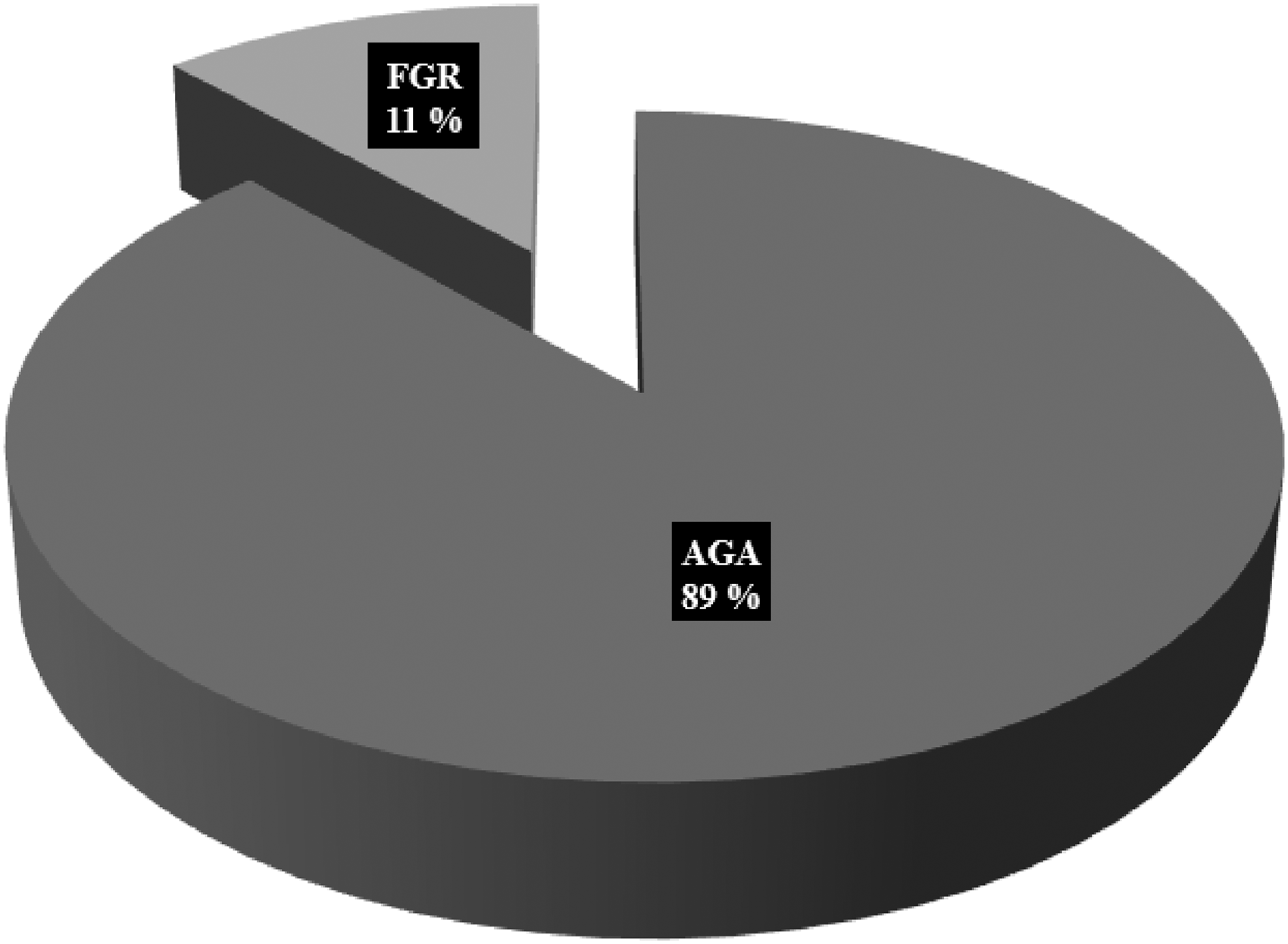
Fetal outcome: fetal growth restriction 2/19, 11%; average for gestational age 17/19, 89%.
Two mothers experienced placental abruption, and notably, both were ANA- and SS-A-positive, suggesting a possible association between autoimmune antibody positivity and placental complications.
Regarding autoimmune markers, ANA and SS-B antibodies were more frequently associated with dRTA, detected in 13 out of 19 cases (68%), whereas SS-A antibodies were present in 9 cases (47%) (Figure 6).
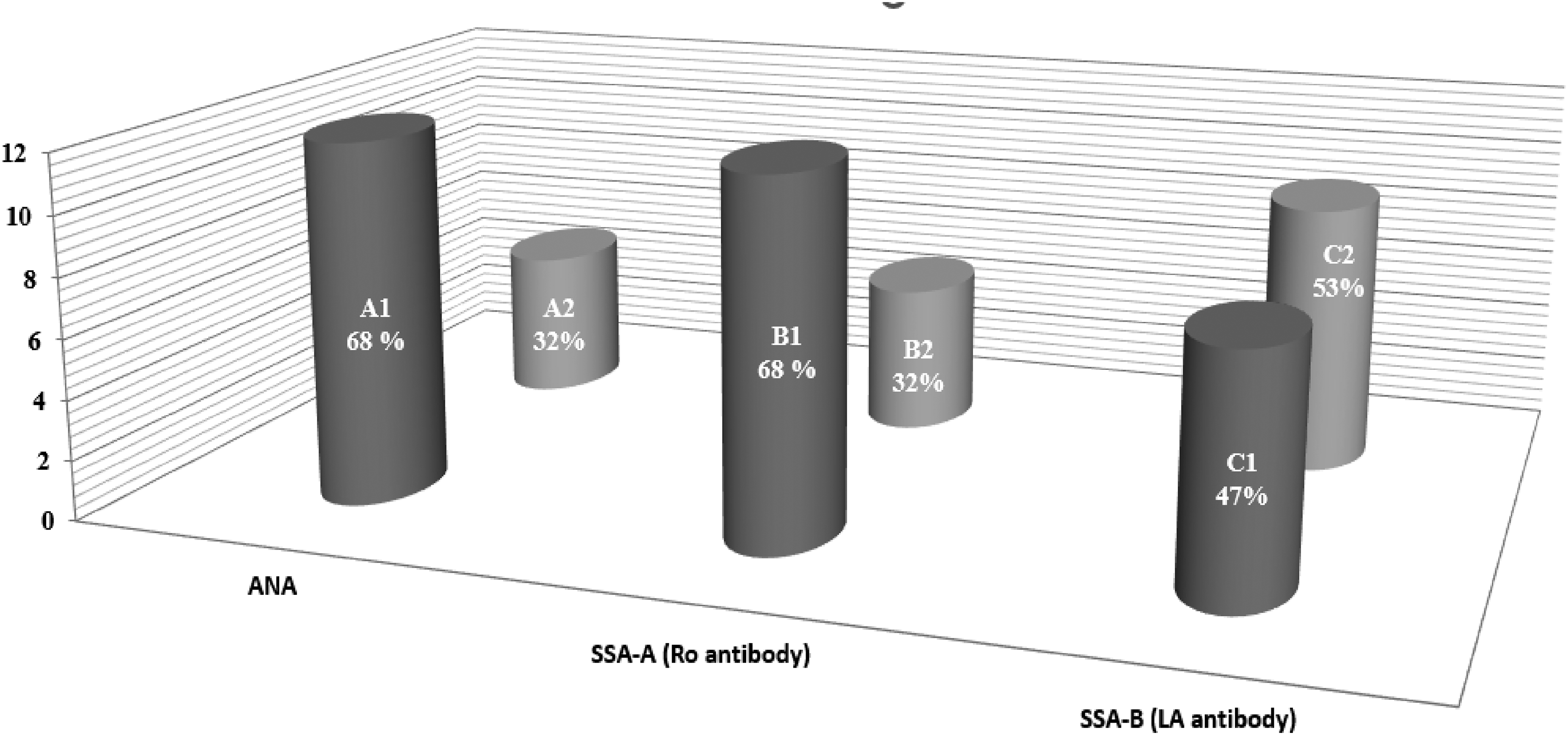
Antibodies associated with dRTA (A1) ANA present 13/19, 68%; (A2) ANA absent 06/19, 32%; (B1) SSA-A antibody present 13/19, 68%; (B2) SSA-A antibody absent 06/19, 68%; (C1) SSA-B antibody present 09/19, 47%; (B2) SSA-B antibody absent 10/19, 53%. dRTA, distal RTA; RTA, renal tubular acidosis.
In our study, maternal and fetal outcomes were largely favourable. Nearly all mothers were able to carry their pregnancies to full term and delivered appropriate-for-gestational-age (AGA) babies.
Discussion
Distal RTA (dRTA, Type I) is the most common form of primary RTA. 5 It arises from the inability of the distal renal tubules to adequately excrete hydrogen ions and ammonium (NH4+), leading to persistent hyperchloremic metabolic acidosis, typically accompanied by hypokalemia. 16
Type I RTA (dRTA) may be primary (inherited), acquired or idiopathic in origin. 3 Inherited forms are associated with several genetic disorders, such as Bartter syndrome and Gitelman syndrome. 20 Hereditary RTA typically presents in childhood, often manifesting as rickets, growth retardation and failure to thrive. 3
Acquired dRTA is frequently associated with systemic conditions. Hypergammaglobulinaemic states such as monoclonal gammopathy, multiple myeloma, amyloidosis, cryoglobulinaemia and chronic liver disease have been implicated. In addition, exposure to nephrotoxic agents – including lithium, amphotericin B, non-steroidal anti-inflammatory drugs, lead, thiazide diuretics and certain antiviral medications – can impair distal tubular function and result in RTA.
Autoimmune diseases represent the most common cause of dRTA in adults. 21 These include systemic lupus erythematosus (SLE), Sjögren's syndrome, rheumatoid arthritis, systemic sclerosis, autoimmune thyroiditis, chronic active hepatitis and primary biliary cirrhosis. Among these, Sjögren's syndrome is particularly notable, with acquired Type I RTA reported in approximately 5–25% of affected patients. 22 Management of Primary Sjögren's disease with dRTA in a pregnant patient may require potassium/bicarbonate supplementation and immunosuppression, with azathioprine. In our study, 84% of RTAs were secondary to connective tissue disorders, primarily Sjögren's syndrome.
In some cases, RTA may be transient, with no identifiable underlying aetiology, and can show complete resolution following delivery. 4 Additionally, RTA secondary to maternal substance abuse – most notably inhalation of toluene – has been associated with adverse perinatal outcomes, including FGR, preterm labour, dysmorphic features and perinatal mortality.
Proximal RTA (Type II RTA) results from an impaired ability of the proximal tubule to reabsorb filtered bicarbonate. As a consequence, excess bicarbonate is lost in the urine, leading to hyperchloremic metabolic acidosis. However, the degree of acidosis is generally less severe than in dRTA, as the distal nephron retains the capacity to reabsorb bicarbonate and partially compensate for the proximal defect. 23 Proximal RTA is most commonly inherited and is frequently associated with Fanconi syndrome, a generalized proximal tubular dysfunction characterized by urinary loss of glucose, phosphate, calcium, amino acids and other electrolytes. 3
Type IV RTA is characterized by hyperkalaemic metabolic acidosis and is associated with hypoaldosteronism or renal resistance to aldosterone. 16
Irrespective of the underlying type or aetiology, RTA ultimately results in an inappropriately alkaline urine (urine pH > 5.5) despite the presence of sustained systemic metabolic acidosis or induced acidosis (blood pH < 7.35). This reflects the inability of the renal tubules to appropriately acidify the urine. These abnormalities are typically accompanied by disturbances in serum potassium levels and a positive urinary anion gap, which together support the diagnosis of RTA. 6
Normal pregnancy is associated with well-recognized physiological adaptations in acid–base and electrolyte balance. Progesterone-mediated stimulation of the respiratory centre leads to an increased respiratory rate and minute alveolar ventilation, resulting in mild chronic hyperventilation and a compensated respiratory alkalosis. Concurrently, the expansion of plasma volume and a pregnancy-related increase in renal blood flow result in glomerular hyperfiltration, with the glomerular filtration rate rising by approximately 50%. This enhanced renal clearance contributes to lower serum bicarbonate and potassium levels. 4
As a consequence of these changes, maternal arterial blood pH increases slightly by about 0.02 units, the base excess rises to approximately 2 mEq/L, and serum bicarbonate (HCO3−) levels decline modestly from non-pregnant values of 24–28 mEq/L to around 18–22 mEq/L. Serum potassium levels also show a small physiological reduction, typically by 0.2–0.3 mmol/L, during normal pregnancy. Importantly, the healthy fetus is well adapted to these subtle alterations in maternal acid–base status, largely due to the efficiency of the placental unit, which facilitates effective exchange of oxygen and carbon dioxide between the mother and fetus, thereby maintaining fetal acid–base homeostasis. 3
Chronic, untreated maternal acidosis in RTA during pregnancy may ultimately lead to a reduction in maternal plasma oxygen-carrying capacity. This occurs partly because maternal haemoglobin acts as a buffer for retained hydrogen ions during systemic acidosis, thereby reducing the fraction of haemoglobin available for oxygen transport across the placenta. Consequently, fetal oxygen delivery may be compromised. Blechner et al. 24 further demonstrated that maternal acidosis is associated with reduced uterine blood flow during pregnancy, which may contribute to fetal distress and adverse perinatal outcomes as a result of hypoxic–acidotic injury.
Both distal and proximal RTA can lead to significant electrolyte disturbances, most commonly hypokalemia. One proposed theory behind it is that since hydrogen is not excreted, potassium is wasted to maintain electroneutrality in urine, which results in low serum potassium. 25 During pregnancy, physiological glomerular hyperfiltration further enhances the renal loss of electrolytes. Consequently, both types of RTA worsen. 3
In this study, patients were treated with sodium bicarbonate tablets and potassium chloride syrup to correct metabolic acidosis and hypokalemia, respectively. The sodium bicarbonate dose ranged from 500 to 1500 mg three times daily, while potassium chloride syrup was given at 10–20 mL three times daily or four times daily. Monthly monitoring of serum bicarbonate and electrolyte levels was performed to adjust supplement doses, with target levels of serum bicarbonate 19–24 mmol/L and serum potassium 3.5–4.5 mEq/L. However, most patients maintained potassium levels closer to 3.5 mEq/L, as the metallic taste of potassium chloride syrup often reduced compliance. Ensuring treatment adherence was a major challenge and required rigorous counselling, particularly regarding the maternal risks and adverse effects on fetal survival associated with poor control of hypokalemia and metabolic acidosis.
Clinical manifestations of hypokalemia may range from mild muscle weakness and episodes of hypokalemic periodic flaccid paralysis to severe complications such as profound diffuse muscle weakness, acute rhabdomyolysis, life-threatening cardiac arrhythmias, respiratory failure and even cardiac arrest in a rare occurrence. 26 In quite a few instances, undiagnosed asymptomatic RTA-1 is later uncovered and reported during pregnancy due to hypokalemia and associated complications. 27 It can be speculated from these cases that physiologic changes in pregnancy might have incited otherwise occult RTA-1. In our study, recurrent hypokalemic periodic paralysis was observed in 89% of the mothers, making it the most common complication identified. Yuvaraj et al., Alkhasoneh et al. and Fadzil et al. reported a case of dRTA secondary to Sjögren's syndrome with positive SSA antibodies, presenting with episodes of profound hypokalemic lower limb muscle weakness and bilateral nephrocalcinosis. The patient was treated with bicarbonate and potassium supplements along with steroids, resulting in good maternal and fetal outcomes.
Rhabdomyolysis represents a potentially life-threatening complication due to profound hypokalemia (K < 2.5 mEq/L). Potassium plays a major role in regulating skeletal muscle blood flow. Local elevation in the potassium concentration during muscle activity causes vasodilatation, which enhances regional blood flow. This cellular release of potassium is impaired in a potassium-depleted state, leading to relative muscle ischemia, which manifests as muscle cramps and, in severe hypokalemia, as muscle necrosis and rhabdomyolysis, especially during exertion. 14 Pregnancy is a high-risk state for predilection to hypokalaemia-induced rhabdomyolysis. In pregnancy, there is an increased incidence of hypokalemia-induced rhabdomyolysis as seen in different case reports where cases of rhabdomyolysis, patients presented with muscle pain and severe cramps. 7 Electrolyte abnormalities, renal function and liver enzymes all need to be monitored and corrected quickly, especially in pregnant patients, to prevent adverse outcomes. Muthukrishnan et al. reported a pregnancy with dRTA secondary to connective tissue disease with persistent hypokalemia, who presented with recurrent rhabdomyolysis in her consecutive pregnancies, treated with intravenous saline with potassium followed by oral potassium citrate, with a good outcome.
During the management of pregnancies complicated by RTA, it is crucial to avoid conditions that may exacerbate pre-existing hypokalemia, such as prolonged vomiting. Therefore, pregnant women with RTA who develop hyperemesis gravidarum require close surveillance, with particular emphasis on meticulous electrolyte monitoring and strict adherence to prescribed therapy. 18 These aspects were carefully addressed in the management of patients in our series.
Pre-term labour is a common complication in RTA, mostly associated with substance abuse. If tocolysis is required in these patients, terbutaline should be avoided. Due to β-adrenergic stimulation, terbutaline causes maternal hyperglycemia and subsequent transient hypokalemia, exacerbating preexisting hypokalemia in RTA. The agent of choice for tocolysis would be nifedipine (a calcium channel blocker).
Excessive loss of urinary calcium, which is frequently seen in dRTA (type 1) disorders, may lead to osteopenia, osteomalacia and secondary hyperparathyroidism. This hypercalciuria is the compensatory mechanism in bone aimed at buffering the retained hydrogen ions (hydrogen ions are exchanged for calcium in bone, and tubular reabsorption of calcium decreases). In the present study, nearly one-third of the cases had a history of fractures, with pelvic fractures occurring more frequently than fractures of the long bones.
Renal tubular acidosis–related hypercalciuria, alkaline urine and hypocitraturia predispose to renal lithiasis, most commonly calcium phosphate calculi, either as isolated stones or in association with nephrocalcinosis, including medullary sponge kidney with secondary hyperparathyroidism. In our study, nephrocalcinosis was observed in 26% (5/19) of mothers. Both nephrocalcinosis and renal calculi may increase the risk of urinary tract infections (UTIs). When combined with the physiological changes of the urinary tract during pregnancy, these conditions further predispose pregnant women to recurrent UTIs, including pyelonephritis and ureteric obstruction, which may ultimately lead to renal impairment. 28 Accordingly, in our patients, urine culture and sensitivity testing were performed in each trimester.
Nephrocalcinosis, due to RTA, can be progressive, and hence vitamin D and calcium supplementation during pregnancy should be done under strict monitoring. 13
Although glomerular function is typically preserved in the early stages of RTA, regular monitoring of renal function is essential, as renal insufficiency may develop over time, particularly in patients with progressive nephrocalcinosis. 13 Delayed diagnosis and inadequate treatment can result in disease progression to chronic renal failure secondary to nephrocalcinosis. In our study, 15% of mothers experienced episodes of AKI related to recurrent UTIs and pyelonephritis; all were managed appropriately with complete recovery. Only one mother had evidence of mild chronic renal failure, most likely attributable to nephrocalcinosis. With appropriate treatment and close monitoring, this patient also achieved favourable maternal and perinatal outcomes.
Rowe et al. 29 suggested that pregnant women with RTA may be at an increased risk of developing pregnancy-induced hypertension, attributable to the underlying renal pathology and its potential exacerbation by the physiological hypervolemia of pregnancy. Apart from this report, the available literature does not document a clear association between RTA and hypertension. Consistent with these observations, our case series did not demonstrate an increased incidence of hypertensive disorders in pregnancies complicated by RTA when compared with the general obstetric population.
In addition to its maternal implications, RTA may also adversely affect the fetus. Maternal metabolic acidosis associated with RTA can lead to reduced uterine blood flow, thereby potentially predisposing to fetal distress. In our study, however, cord blood venous and arterial analyses at delivery were within normal limits, with no evidence of either acute or chronic fetal hypoxia.
Fetal growth restriction is another potential complication, particularly when maternal acidosis is inadequately corrected. Although FGR has been reported as a relatively common complication in RTA – mainly in cases related to substance abuse – it appears to be uncommon in RTA due to other etiologies. 28 Overall, fetal outcomes in our study were favourable. Only two neonates were diagnosed with FGR and required short-term NICU admission for observation; both remained stable and recovered well, likely reflecting timely correction of maternal electrolyte imbalances and metabolic acidosis.
Chronic severe metabolic acidosis can adversely affect bone mineralization in both the mother and the fetus. Although the fetus is relatively protected from hypocalcemia because calcium is actively transported across the placenta, 30 neonatal hyperparathyroidism secondary to maternal hypocalcemia due to RTA has been reported. 31 Importantly, these skeletal changes are reversible once the neonate is no longer exposed to the maternal metabolic milieu and calcium balance is restored. In our study, antenatal ultrasound assessment did not reveal any abnormal fetal bone findings, and postnatal neonatal bone evaluation was also normal in all cases. These favourable outcomes likely reflect timely diagnosis and appropriate management of pregnancies complicated by RTA.
Whether there are any long-term adverse effects from the pregnancy on the course of maternal disease remains unresolved. Since treatment is based on electrolyte replacement to maintain normal pH and ionic balance, and there is no decrease in renal function, we speculate that as long as serum pH and ionic balance are maintained within normal limits, there should be no adverse effect from the pregnancy on the course of the disease. 28
Renal tubular acidosis is a chronic disorder that requires lifelong therapy; however, with appropriate treatment, symptoms can be effectively minimized. Management typically involves supplementation with potassium and sodium bicarbonate to maintain normal acid–base and electrolyte balance. 23
Physiological changes during pregnancy, particularly increased glomerular hyperfiltration, lead to enhanced renal losses of electrolytes, thereby significantly increasing the requirement for potassium and bicarbonate. Consequently, careful adjustment of therapy is essential to prevent both obstetric and renal complications. In our cohort of pregnancies complicated by RTA, we observed a clear increase in the need for alkali and potassium supplementation. Dose escalation was required during pregnancy, particularly in the third trimester, with doses increasing by approximately 1.5–2 times compared with pre-pregnancy requirements.
In our study, maternal and fetal outcomes were largely favourable. Nearly all women were able to carry their pregnancies to term and birth AGA babies. These favourable outcomes can be attributed to timely diagnosis, optimal metabolic control and consistent treatment within a multidisciplinary care framework involving obstetricians, nephrologists and neonatologists, along with the fact that most mothers with Sjögren's syndrome and SLE conceived during periods of disease remission. 15 Furthermore, early recognition and prompt correction of electrolyte imbalances, vigilant antenatal surveillance and individualized delivery planning were pivotal in optimizing both maternal and neonatal outcomes in pregnancies complicated by RTA.
Optimization of peripartum acid–base status and electrolyte balance is essential, as affect anaesthesia management and post-operative recovery. Bhattacharya et al. reported a mother with dRTA with hypokalemic periodic paralysis with familial hypokalemic periodic paralysis presented with fetal distress at term gestation, treated with bicarbonate and potassium infusion. Under spinal anaesthesia, LSCS was done, and a healthy baby was born. The post-operative period was uneventful. Duran et al. reported a woman, first time diagnosed with dRTA, as she presented in immediate post-caesarean puerperium with progressive proximal. There was an improvement in weakness with potassium supplementation.
In this case series, the majority of RTA pregnancies were attributable to acquired causes, most commonly secondary to connective tissue disorders. There was no family history of RTA in any cases. Following birth, before discharge from the hospital, all neonates were carefully evaluated for clinical features suggestive of RTA, including persistent vomiting and dehydration. During this period, baseline investigations, such as blood pH, urine pH and serum electrolytes, were performed, and all results were within normal limits.
Parents were counselled regarding the warning signs of RTA, including failure to thrive, persistent vomiting and dehydration and were advised to monitor for these symptoms at home. The infants were subsequently followed up at 1 month, 3 months and 6 months of age. At each visit, laboratory evaluations were repeated to assess for metabolic abnormalities, including low serum bicarbonate, elevated urine pH (>5.5), hypokalaemia and unexplained metabolic acidosis. All infants remained clinically and biochemically normal throughout the follow-up period. Brainstem Evoked Response Audiometry testing was performed to rule out sensorineural hearing loss, and all babies showed normal results; therefore, genetic testing was not deemed necessary.
Recommendations
Based on findings from our study, we propose the following structured monitoring and management plan for pregnancies complicated by RTA:
Multidisciplinary care involving both an obstetrician and a nephrologist is essential throughout pregnancy. Women with RTA secondary to autoimmune disorders such as SLE or Sjögren's syndrome should plan pregnancy during disease remission for better maternal and fetal outcomes. As pregnancy increases the risk of hypokalemia and metabolic acidosis, regular monitoring of serum potassium and bicarbonate is essential, at least monthly, and more frequently if clinically indicated. Target levels should be potassium 3.5–4.5 mEq/L and bicarbonate 19–24 mEq/L. Alkali and potassium supplementation often need dose escalation, especially in the third trimester, with requirements increasing up to 1.5–2 times. Factors worsening hypokalemia, such as hyperemesis, beta-mimetic tocolytics and loop diuretics, should be avoided to prevent serious complications. Urine culture should be done every trimester due to the increased risk of recurrent UTI and pyelonephritis in women with nephrocalcinosis or renal calculi. Vitamin D and calcium supplementation should be carefully monitored if nephrocalcinosis is present. Enhanced fetal surveillance, including first-trimester screening, anomaly scan and serial growth scans four weekly. Timing and mode of delivery should follow standard obstetric indications in well-controlled cases. Peripartum acid–base balance and electrolyte optimization are crucial, as metabolic acidosis and hypokalemia-related muscle weakness have implications for anaesthesia and post-surgical recovery. Cord blood gas analysis at delivery is recommended to assess neonatal acid–base status, as maternal metabolic acidosis may predispose to fetal distress.
Strength of the study
To date, this study represents the largest case series of RTA-complicated pregnancies, comprising 19 cases, compared with previously published reports that typically include only one to three cases.
Limitations
Retrospective nature of the study.
Conclusion
If a pregnant woman presents with symptoms such as recurrent fainting episodes, fatigue, muscle weakness or repeated bone fractures – particularly in the presence of autoimmune conditions such as Sjögren's syndrome or SLE – clinicians should maintain a high index of suspicion for non-traditional causes such as RTA and investigate accordingly.
Although RTA in pregnancy is rare, active disease can result in substantial maternal and perinatal morbidity due to chronic maternal acidosis. However, timely diagnosis, early initiation of appropriate therapy, close monitoring, strict treatment adherence and a multidisciplinary management approach can markedly improve both maternal and pregnancy outcomes.
Footnotes
Acknowledgements
The authors wish to acknowledge the Departments of Obstetrics, Fetal Medicine, and Neonatology of the Fernandez Hospital for their support.
Ethical approval
The study was approved by the Ethics Committee of Fernandez Hospital (IEC ref. No: No 44_2023).
Patient consent
All participants gave written informed consent
Contributorship
Conceptualization, methodology, Data curation, original draft, formal analysis: Arati Singh; Project administration, visualization, Validation, supervision: Tarakeswari Surapaneni; Visualization, investigation, validation: Hemamalini Vadlamani. All authors reviewed and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author, Dr Arati Singh, upon reasonable request.
Guarantor
Arati Singh is the guarantor of this manuscript and takes responsibility for the integrity of the work as a whole.
Trial registration
Trial registration is not applicable because this was not an interventional study.