
Abstract
Eplerenone is a mineralocorticoid receptor antagonist with minimal affinity for androgen receptors. Mineralocorticoid receptor antagonists are efficacious in the management of resistant hypertension, obstructive sleep apnea, cardiac dysfunction, renal tubular disorders, hepatic cirrhosis, portal hypertension, diabetic nephropathy, proteinuric kidney disease, and chronic central serous chorioretinopathy in the general population. Five cases describing the use of eplerenone in pregnancy are discussed, the previous literature reviewed, and potential indications for the use of eplerenone in pregnancy discussed.
Introduction
Spironolactone is currently not recommended for use in pregnancy because of potential anti-androgenic effects on the male fetus. Prior to a study by Hecker et al. in 1980 demonstrating demasculinization of male rat fetuses following maternal exposure to a human equivalent dose of 2581 mg/day, spironolactone had been used extensively during pregnancy for the treatment of hypertension, preeclampsia, edema, liver disease, and myasthenia gravis. 1 Other animal studies have demonstrated absence of demasculinization of male fetuses following maternal exposure to the human equivalent of 200 mg spironolactone/day.2,3 A single human case of ambiguous genitalia in the newborn of a mother treated with spironolactone was reported in a conference abstract in 2011. 4 In this case, however, maternal exposure had ceased at 5 weeks’ gestation, prior to male sex development which occurs between 7 and 12 weeks gestation. 5 Since 1980, a further 21 pregnancies have been described with maternal spironolactone therapy at doses ranging from 25 to 400 mg/day, producing eight male infants, all with normal external genitalia.6–15
Eplerenone is a mineralocorticoid receptor hypertension and with 100- to 1000-fold lower binding affinity to androgen, glucocorticoid, and progesterone receptors compared with spironolactone. 16 In non-pregnant individuals, eplerenone has a greater effect in reducing mortality in heart failure with reduced ejection fraction (HFrEF) compared with spironolactone, is efficacious in the management of resistant hypertension, and improves apnea-hypopnea index in obstructive sleep apnea (OSA).17–20 Eplerenone appears to be less effective than spironolactone in managing hypokalemia and blood pressure with primary aldosteronism (PA). 21
Eplerenone undergoes placental transfer, with cord blood levels 67.8% of maternal levels. 22 Relative infant dose via breast milk was 3% of maternal daily dose. 22 Eplerenone has a biological half-life of 3 to 4 hours, and primary routes of excretion are via feces (32%) and urine (67%). 23 Steady-state plasma concentration of eplerenone is achieved within 4 days of dosing. Dose should be reduced where estimated glomerular filtration rate (eGFR) is less than 50 ml/minute/1.73 m2, and eplerenone is not recommended in individuals with eGFR less than 30 ml/minute/1.73 m2 due to increased risk of severe hyperkalemia. 24 Serum potassium and renal function should be measured 1 week after initiation or any change in dose, and then at monthly intervals for the first 3 months.
The outcome of five further pregnancies with maternal eplerenone therapy are described.
Case 1
A 27-year-old woman with Gitelman syndrome had been treated with eplerenone for 7 years, having been intolerant of all oral potassium supplements, amiloride, non-steroidal anti-inflammatory drugs, and spironolactone. She had elected to conceive while taking eplerenone and continued this throughout her first pregnancy, with healthy maternal and infant outcome. 25 In her second pregnancy, she again elected to conceive while continuing eplerenone 100 mg/day and continued this dose throughout her pregnancy with satisfactory potassium levels, delivering a female birthweight 3630 g, who has normal development at age 19 years.
Case 2
A 38-year-old multiparous woman was admitted to hospital at 35 weeks’ gestation because of poorly controlled essential hypertension in the setting of morbid obesity and severe obstructive OSA. Previous testing for PA, pheochromocytoma, and renal artery stenosis had been negative. Blood pressure was 160–190/90–105 mmHg while taking nifedipine extended-release (ER) 120 mg/day, labetalol 1600 mg/day, and methyldopa 1500 mg/day as an inpatient. Urine protein: creatinine ratio (PCR) was normal. Additional antihypertensives considered included hydralazine, clonidine, prazosin, and thiazide diuretics. Addition of oral hydralazine was thought less likely to be of benefit given the woman was already receiving a maximal dose of a peripheral vasodilator with nifedipine therapy. Both clonidine and methyldopa are centrally acting alpha-2 agonists. Combining clonidine and methyldopa has not been recommended due to risks of somnolence and bradycardia. 26 Substitution of clonidine for methyldopa was not attempted given equivalent efficacy as monotherapy and in combination therapy with diuretic therapy, with greater adverse effects with clonidine.27–30 The antihypertensive effect of prazosin was only modest when used in combination with methyldopa, clonidine, and beta-blockers, and doxazosin was less effective than spironolactone as fourthth-line therapy in individuals with resistant hypertension.31,32 Thiazide diuretics have the potential to reduce maternal intravascular volume potentially leading to decreased uteroplacental perfusion, as well as causing electrolyte abnormalities. Eplerenone was discussed with the patient given the evidence for mineralocorticoid receptor antagonists in improving blood pressure and parameters of sleep disordered breathing in individuals with OSA.20,33–36 Following written informed consent, eplerenone 25 mg twice daily was added, the dose increased to 50 mg twice daily at 36 weeks’ gestation. The woman's blood pressure improved to 130–140/60–80 mmHg. She proceeded to elective induction of labor at 37 weeks’ gestation, delivering a healthy male birthweight 3214 g with normal external genitalia.
Case 3
A 42-year-old multiparous woman was admitted at 27 weeks’ gestation because of poorly controlled essential hypertension in the setting of morbid obesity, severe OSA, and long QT syndrome (LQTS). Previous testing for PA, pheochromocytoma, and renal artery stenosis had been negative. Blood pressure was 150–180/100–120 mmHg as an inpatient while taking metoprolol-XR 95 mg/day and nifedipine-XR 120 mg /day. Urine PCR was normal. She had previous intolerance to methyldopa, and alpha-blockers were undesirable in view of LQTS. Eplerenone 25 mg mane was commenced following written informed consent, with blood pressure improving to 130–140/80–95 mmHg over the subsequent 4 days. At 32 weeks’ gestation blood pressure again rose and urine PCR was elevated at 79 mg/mmol (normal < 30) consistent with superimposed preeclampsia. Eplerenone was gradually increased to 75 mg mane as an outpatient until the development of worsening hypertension, a rise in urine PCR to 1074 mg/mmol Cr, and fetal concerns prompted delivery of a 1990 g female infant at 34 weeks’ gestation.
Case 4
A 27-year-old multiparous woman with a history of peripartum cardiomyopathy diagnosed six years previously, and previous pulmonary embolism, presented at 7 weeks’ gestation of an unplanned pregnancy, while taking bisoprolol 1.25 mg twice daily and enalapril 5 mg daily. No significant variants had been identified in a cardiomyopathy gene panel. Left ventricular ejection fraction (LVEF) was 45% on echocardiography. The woman elected to continue the pregnancy. Enalapril was ceased, prophylactic dose enoxaparin was commenced, and bisoprolol increased to 2.5 mg twice daily. Eplerenone 12.5 mg in the morning was added by her cardiologist at 11 weeks’ gestation following written informed consent. Bisoprolol was subsequently increased to 3.75 mg twice daily, and eplerenone to 25 mg in the morning. The LVEF and cardiac dimensions remained stable until 29 weeks’ gestation on monthly echocardiography, when there was a fall in LVEF to 35-40%. Further increase in bisoprolol and eplerenone were not possible because of maternal blood pressure. Echocardiography continued to be performed weekly, and at 34 weeks' gestation dyspnea and orthopnea with a fall in LVEF to 25% prompted induction of labor, delivering a 2670-g male infant with normal external genitalia.
Case 5
A 35-year-old primigravid woman with idiopathic dilated cardiomyopathy, morbid obesity, essential hypertension with proteinuria, previous pulmonary embolism, moderate-severe OSA, and gestational diabetes mellitus presented to another health service at 12 weeks’ gestation with pulmonary edema in the setting of poorly controlled hypertension and medication non-adherence. Echocardiography revealed global hypokinesis with LVEF 40% to 45%. No significant variants were identified in a cardiomyopathy gene panel. The woman was commenced on bisoprolol, methyldopa, frusemide, and prophylactic dose enoxaparin. PA and pheochromocytoma were excluded. At 33 weeks’ gestation repeat echocardiography revealed LVEF 20% to 25%. Following written informed consent, methyldopa 1 g/day was changed to eplerenone 25 mg twice daily for potential benefits on left ventricular function. Enoxaparin was increased to treatment dose in view of the increased risk of left ventricular thrombus formation with decline in LVEF to less than 35% as per international guidelines. 37 Bisoprolol 10 mg daily was continued. Eplerenone was increased to 37.5 mg twice daily at 35 weeks’ gestation. Labor was induced at 39 weeks’ gestation; the women delivered a 2800-g female. Postpartum, enalapril was added to bisoprolol and eplerenone. Cardiac magnetic resonance imaging 6 months’ postpartum showed LVEF 45%.
Discussion
Sixteen previous case reports have described the use of eplerenone during pregnancy (Table 1). No cases described adverse infant outcomes attributed to eplerenone therapy.
Summary of cases of eplerenone use in pregnancy.
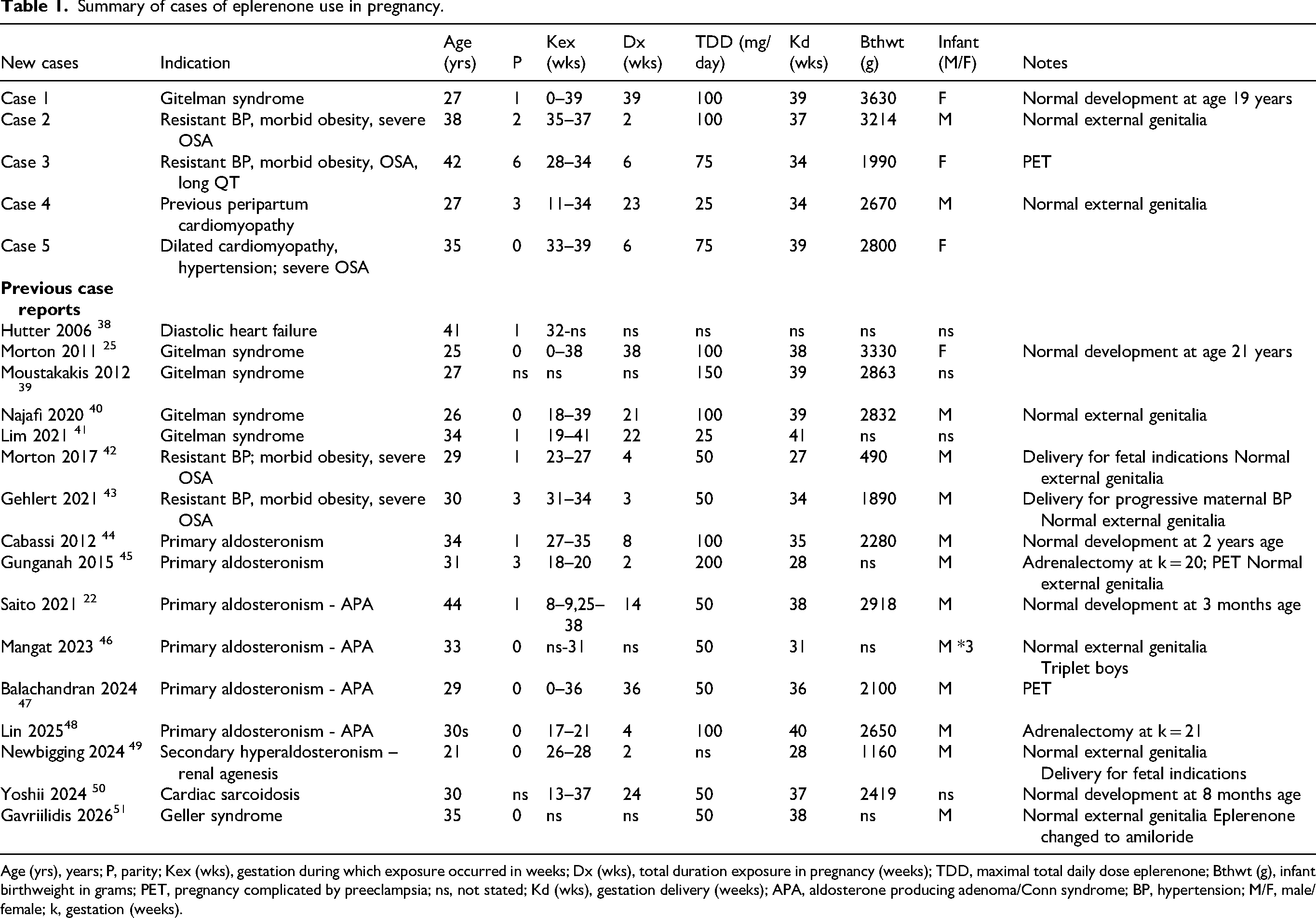
Age (yrs), years; P, parity; Kex (wks), gestation during which exposure occurred in weeks; Dx (wks), total duration exposure in pregnancy (weeks); TDD, maximal total daily dose eplerenone; Bthwt (g), infant birthweight in grams; PET, pregnancy complicated by preeclampsia; ns, not stated; Kd (wks), gestation delivery (weeks); APA, aldosterone producing adenoma/Conn syndrome; BP, hypertension; M/F, male/female; k, gestation (weeks).
In addition, Downie et al. reported four women with PA who received eplerenone during pregnancy where optimal blood pressure control could not be achieved with multiple pregnancy-appropriate agents. 52 While individual infant outcome was not described, the authors stated the study added to the body of literature where use of eplerenone was not associated with adverse neonatal outcomes or neonatal death. One of the four eplerenone-treated women developed preeclampsia. 52 In a conference abstract, Lopez et al. described two women with biochemically confirmed PA who were commenced on eplerenone 50 mg/day in late second trimester, with improvement in hypertension and hypokalemia. 53 Both pregnancies resulted in preterm delivery with birthweights appropriate for gestational age.
Six case reports described the use of eplerenone in the management of PA in pregnancy, together with the four cases described in the series by Downie et al. In two of the cases eplerenone was used for 2 and 4 weeks, respectively, before proceeding to adrenalectomy. There are no consensus guidelines regarding the management of PA during pregnancy. A systematic review concluded adrenalectomy for aldosterone-producing adenoma (Conn syndrome) did not improve maternal or fetal outcomes over medical treatment alone. 54 The surgically treated group, however, required more antihypertensive medications prior to surgery than the medically treated group. The course of PA in pregnancy is also extremely variable, and the medically treated group is likely to have included those women whose hypertension and hypokalemia improved spontaneously during pregnancy, postulated to be due to the physiological increase in progesterone blocking the effects of aldosterone on mineralocorticoid receptors. No randomized trials have compared outcomes with MRAs, epithelial sodium-channel inhibitors, and other antihypertensive medications in the general population. Recommendations from the Endocrine Society Clinical Practice Guideline and from a systematic review for the use of PA-specific medical therapy in non-pregnant individuals with PA are based on two observational studies.21,55–57 The recommended initial dose of eplerenone in non-pregnant individuals with PA is 25 mg twice daily, with gradual titration to the lowest effective dose, up to a maximum of 200 mg twice daily. 55 It is unclear as to whether MRAs are superior to conventionally used antihypertensives in managing PA in pregnancy.
Five case reports described the use of eplerenone in the management of Gitelman syndrome. An open-label randomized crossover study comparing the efficacy and safety of 6-week treatments with once-daily 75 mg slow-release indomethacin, 150 mg eplerenone and 20 mg amiloride in non-pregnant individuals with Gitelman syndrome found increases in serum potassium of 0.38 mmol/L, 0.15 mmol/L, and 0.19 mmol/L, respectively. 58 The prolonged use of indomethacin is associated with increased risk of oligohydramnios and constriction of the fetal ductus arteriosus with maternal exposure in third trimester, persistent pulmonary hypertension of the newborn in extremely preterm infants, necrotizing enterocolitis, periventricular leukomalacia, and effects on maturation of the fetal kidneys.59–61 Unlike eplerenone, amiloride increases serum magnesium with renal tubular disorders through reducing urine magnesium excretion. 62 Thirty cases of maternal amiloride therapy have been described during pregnancy, with adverse outcomes in two cases likely related to uncontrolled hypertension rather than amiloride treatment. 63 Amiloride may be preferable to eplerenone in the management of Gitelman syndrome given its effect in raising serum magnesium as well as potassium.
Single case reports describe the use of eplerenone in pregnancy with previous peripartum cardiomyopathy with persistent reduced LVEF preconception, preconception idiopathic dilated cardiomyopathy with severe OSA and hypertension, and cardiac sarcoidosis, respectively, The 2025 European Society of Cardiology Guidelines for the management of cardiovascular disease and pregnancy recommend the use beta-1-selective blockers for dilated cardiomyopathy and HFrEF in pregnancy, and a class III level C recommendation against the use of angiotensin converting enzyme inhibitors, angiotensin II receptor blockers, angiotensin receptor neprilysin inhibitors, MRAs, ivabradine, and sodium–glucose co-transporter-2 inhibitors in pregnancy because of adverse fetal effects. 37 Oral hydralazine and isosorbide dinitrate in combination and the use of intravenous ferric carboxymaltose in individuals with iron deficiency (serum ferritin less than 100 μg/L, or 100–300 μg/L with transferrin saturation less than 20%) may be a consideration in pregnant women with left ventricular dysfunction based upon efficacy in non-pregnant individuals.64,65 A meta-analysis of six randomized controlled trials found that eplerenone therapy significantly reduced cardiovascular mortality, heart failure hospitalization, and all-cause mortality in non-pregnant individuals across heart failure phenotypes. 19 Naser et al. reported eplerenone significantly improved left ventricular systolic function while reducing cardiovascular and all-cause mortality compared to spironolactone in the treatment of HFrEF. 66 Initial dose of eplerenone in non-pregnant individuals with heart failure with preserved or reduced ejection fraction is 25 mg once daily, with increase of dose to 50 mg daily after 4 weeks provided serum potassium and renal function are stable. 67 More data is required to clarify whether eplerenone has a role in managing cardiac dysfunction in pregnancy.
Four cases described the use of eplerenone in the management of preterm resistant hypertension in pregnancy in the setting of morbid obesity and severe OSA. Eplerenone therapy enabled continuation of pregnancy for 2, 3, 4, and 6 weeks, respectively. A Scientific Statement from the American Heart Association recommended the use of long-acting thiazide diuretics, or addition of spironolactone or eplerenone in the management of resistant hypertension in non-pregnant individuals. 68 Obesity, OSA, and sympathetic overactivity may be contributing factors to resistant hypertension. 69 The prevalence of OSA increases from early to later stages of gestation.70,71 A randomized controlled trial assessed the efficacy of eplerenone 50 mg/day added to standard antihypertensive therapy on parameters of 24-hour ambulatory blood pressure and polysomnography over a 6-month period in non-pregnant individuals with OSA and resistant hypertension. 35 Eplerenone therapy resulted in significant reductions in 24 hours, daytime and nighttime systolic, diastolic and mean arterial pressure. The greatest reduction was seen overnight, with reductions in systolic, diastolic and mean nighttime blood pressure of 14.4, 6.4, and 9.5 mmHg, respectively, resulting in a 45.1% reduction in the number of non-dipper patients. Apnea-hypopnea index reduced by 34.5% in the eplerenone add-on therapy group compared to baseline and standard antihypertensive group. Initial dose of eplerenone in non-pregnant individuals with hypertension is 50 mg once daily, increasing on a monthly basis to a maximum of 50 mg twice daily. 72
Currently, only 27 pregnancies have been described during which there was maternal treatment with eplerenone. No fetal or neonatal malformations were described in the 29 offspring, although the amount of detail varied considerably between case reports. No demasculinization of external genitalia was reported in 15 male infants, although only three were exposed in utero during the gestation at which male sexual differentiation occurs.
Based upon efficacy in non-pregnant individuals, consideration of eplerenone therapy in pregnancy may be worthwhile in women with hypertension which remains poorly controlled despite maximal tolerated doses of antihypertensive medications more conventionally used in pregnancy, particularly in the setting of morbid obesity and OSA. Eplerenone use resulted in continuation of pregnancy for 2 to 6 weeks to achieve greater fetal maturity in the four cases presented where blood pressure was poorly controlled despite maximal doses of the commonly used antihypertensives in pregnancy.
Whether eplerenone is superior to amiloride or conventionally used antihypertensives in PA in pregnancy is unclear. Randomized controlled trials of eplerenone in the management of heart failure in pregnancy may be worthwhile given the efficacy of eplerenone in non-pregnant individuals and the contraindication to multiple other anti-failure medications in pregnancy. Amiloride may be preferable to eplerenone in renal tubular disorders associated with hypokalemia and hypomagnesemia.
Footnotes
Ethical approval
Mater Health Human Research Ethics Committee waived the requirement for ethical approval QACR/MML/115905.
Informed consent
Written informed consent was obtained from all patients for their anonymized information to be published in this article.
Author contributorship
AM did project development, data collection, manuscript writing, and editing.
All authors read and approved the final manuscript.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
Adam Morton.