
Abstract
Background:
Current guidelines lack instruction on fluid administration for patients with critically ill heart failure (HF) in the intensive care unit.
Objectives:
This study aims to compare the risk of mortality and acute kidney injury (AKI) outcomes among unlimited intake, restrictive intake, and negative balance.
Design:
Retrospective cohort study.
Methods:
A total of 3267 patients with HF not receiving renal replacement therapy were included from the Medical Information Mart for Intensive Care-IV (MIMIC-IV) database and were grouped into restrictive fluid intake (the first 24-h fluid intake from 1500 to 2000 mL), negative fluid balance management (the first 24-h net output >1000 mL), and unlimited fluid control groups. The primary endpoint was 28-day mortality, and the secondary endpoints were morbidity of 48-h AKI, 7-day AKI, and AKI progression from 48 h to 7 days. The odds ratio (OR) and the 95% confidence interval (CI) were estimated by multivariable logistic regression, and mediation analyses were performed.
Results:
Negative fluid balance, not restrictive fluid intake, was correlated to a lower risk of 28-day mortality (OR: 0.750 (0.570–0.987), p = 0.040), 48-h AKI (OR: 0.207 (0.169–0.255), p < 0.001), and 7-day AKI (OR: 0.261 (0.207–0.330), p < 0.001) but was correlated to a higher risk of AKI progression (OR: 2.284 (1.835–2.843), p < 0.001) compared to unlimited fluid control after multivariable adjustment. The 24-h net output mediated AKI incidence and progression.
Conclusion:
Negative fluid balance was related to lower risk of 28-day mortality, 48-h AKI, and 7-day AKI but a higher risk of AKI progression, which requires further clinical trials for validation.
Plain language summary
The first 24-hour negative fluid balance is correlated to lower 28-day mortality. Acute kidney injury progression should be cautioned in the first 24-hour negative fluid balance. Lower fluid output and more fluid input may prevent acute kidney injury incidence. The first 24-hour net output mainly contributes to the mediation effect.
Introduction
Heart failure (HF), represented by left and/or right ventricular dysfunction, is one of the most important global public health issues with a high death rate and financial burden.1,2 HF characterized by high fluid overload is associated with pulmonary edema, which can be alleviated by a negative fluid balance. 3 Fluid administration plays an important role in hemodynamic rescue measures for patients with HF, and fluid balance is delicate to maintain. An adequate fluid support in HF patients ensures increased blood volume for cardiac output and peripheral organ perfusion, but inappropriate dehydration or overhydration can promote inadequate perfusion in the heart, kidneys, and other organs. 4
The debate on the benefits of restrictive fluid intake and liberal fluid intake in HF patients remains controversial. Restrictive fluid intake decreases heart burden with potential impaired kidney perfusion, while liberal fluid intake increases peripheral perfusion with potential heart overburden. A recent randomized controlled trial (RCT) demonstrated that liberal fluid administration for the first 24 h after major abdominal surgery can lower the risk of acute kidney injury (AKI) without a decrease in disability-free survival, which overturns the highly contended concept of fewer complications owing to more restrictive fluid intake. 5 On the other hand, restrictive fluid intake showed no advantages in relieving congestion symptoms or improving the prognosis of patients with HF compared to liberal fluid administration.6,7 Fluid balance considers both fluid intake and output, but is less investigated in clinical trials. Previous studies validated that positive fluid balance renders a higher risk of short-term death rate and severe kidney impairment.8,9 Current guidelines for HF provide only an approximate range of fluid intake from 1500 to 2000 mL with insufficient high-quality evidence.10,11 The potential benefit of restrictive fluid intake could be contributed by the negative fluid output, which has not been studied. Whether the negative fluid balance reduces the risk of adverse events or increases the risk of AKI morbidity remains unclear. In this study, we combined the fluid intake and net output to categorize fluid administration strategies to further investigate the impact of restrictive fluid intake and negative fluid balance without restrictive intake on prognosis compared to unlimited fluid control. The first 24-h hemodynamics determines the prognosis of patients hospitalized in intensive care units (ICUs).12,13 A quick and appropriate emergent treatment helps ICU patients to recover from their dangerous hemodynamic dysfunction. Fluid balance is difficult to maintain well in patients with HF hospitalized in ICUs, and this unsettled problem largely depends on various fluid administration strategies selected by different clinicians. 14
This retrospective cohort study aimed to compare mortality, AKI incidence, and its progression among restrictive fluid intake, negative fluid balance, and unlimited fluid control strategies to help inform decision making on clinical fluid management.
Methods
Data source
The retrospective cohort data analyzed in this study were obtained from the publicly accessible MIMIC-IV database, which contains de-identified health information of patients admitted to the ICU of the Beth Israel Deaconess Medical Center (BIDMC) in the United States from 2008 to 2019. 15 The database comprises comprehensive data, including demographic information, clinical features, laboratory results, medication details, and vital signs. Data for analysis were extracted from the institutional electronic health record system, using the Structured Query Language (SQL). The project was approved by the Institutional Review Board of both BIDMC and Massachusetts Institute of Technology. Informed consent is not necessary for the secondary utilization of this de-identified database. The Collaborative Institutional Training Initiative (CITI) license (No. 9024783) and the necessary permissions to utilize the database were obtained. The reporting of this study conforms to STROBE guidelines. 16
Study cohort and data extraction
The SQL was used for data extraction. 17 Adult patients with HF hospitalized in ICU were included for International Classification of Diseases (ICD) code filtration by two independent investigators (Table S1), and only the initial admission was considered if there were multiple ICU admission records. Patients were excluded if they received renal replacement therapy or lacked 24-h records of fluid intake or output. A total of 3267 patients were finally enrolled. The following variables were further analyzed: (1) basic demographics and physiological conditions, including age, sex, heart rate fluctuation (defined as the maximum heart rate in the first 24 h minus the minimum heart rate in the first 24 h), 12 mean arterial pressure (MAP) fluctuation (defined as the maximum MAP in the first 24 h minus the minimum MAP in the first 24 h), 13 and weight; (2) Simplified Acute Physiology Score II (SAPS-II) and Sequential Organ Failure Assessment (SOFA) score; (3) serum potassium, sodium, and chloride levels and blood urea nitrogen (BUN), bicarbonate, and creatinine concentrations; and (4) comorbidities, including diabetes, obesity, acute HF, cardiogenic shock, valvular heart disease, hypertension, chronic obstructive pulmonary disease, renal disease, and coronary artery disease.
The definitions of fluid administration strategies and outcomes
The fluid administration strategies were categorized based on the first 24-h fluid intake and net output, calculated as the urine output minus the fluid intake (Figure S1). Specifically, the restrictive fluid intake was defined as the 24-h fluid intake with 1500–2000 mL according to the current European Society of Cardiology guideline for HF management. 10 The negative fluid balance was defined as the first 24-h net output >1000 mL based on the average daily fluid output from previous studies,9,18 but the first 24-h intake was unrestricted to 1500–2000 mL. The unlimited fluid control was defined as the rest of patients with the first 24-h net output ⩽1000 mL, but the first 24-h intake was unrestricted to 1500–2000 mL.
The primary outcome was short-term 28-day all-cause mortality, and the secondary outcome was 48-h AKI, 7-day AKI, and AKI progression from 48 h to 7 days diagnosed by the Kidney Diseases: Improving Global Outcomes (KDIGO) creatinine and the criteria of urine output. 19 AKI was defined as a rise of ⩾26 mmol/L or 0.3 mg/dL within 48 h or more than 50% of creatinine from baseline creatine within 7 days, and the stage of AKI is described in Table S2. AKI could be gradually developed after the first-day treatment, and the severity change from the 48-h AKI and the 7-day AKI should be monitored for temporal progression. AKI progression was defined as an elevation of at least one AKI stage from 48 h to 7 days.
Statistical analysis
Variables with more than 10% missing values from 3267 patients were excluded, including type B natriuretic peptide (BNP), troponin, creatine kinase, lactate, central venous pressure, partial pressure of oxygen, partial pressure of carbon dioxide, and pH. Variables with less than 10% missing values, including weight, bicarbonate, chloride, BUN, sodium, creatinine, and potassium, were imputed by the random forest model. Although the missing rate of body mass index (BMI) was 21.61%, it was kept for imputation for further analyses because it represented metabolic conditions better than body weight (Figure S2). All continuous variables were nonnormal-distributed and are provided as medians (interquartile ranges, IQRs). Differences in continuous variables were verified by the rank-sum test. Categorical variables were expressed as numbers (percentages) and were verified by the chi-square test. Logistic regression models were performed to demonstrate the correlation of fluid administration strategies to the incidence of 28-day mortality, 48-h AKI, 7-day AKI, and AKI progression. Both the univariable logistic regression model and the multivariable logistic regression model adjusted by age, sex, weight, heart rate fluctuation, furosemide use, potassium, hypertension, and renal disease were established. Odds ratios (ORs) and 95% confidence intervals (CIs) in restrictive fluid intake and negative fluid balance management were calculated and compared with unlimited fluid control. Subgroup analyses were performed for age, sex, cardiogenic shock, acute HF, heart rate fluctuation, and furosemide use. Moreover, Spearman’s rank correlation analysis was performed between weight/BMI and the 24-h fluid intake/fluid output/net output.
The mediation analysis was performed by the “mediation” package from R software (v4.5.0, R Foundation for Statistical Computing, Vienna, Austria). Total effect, average causal mediation effect, average direct effect, and proportions of mediation were evaluated for the mediation effect of 24-h fluid intake/fluid output/net output/body weight-adjusted fluid output on the association between fluid administration strategies and four outcomes.
A two-tailed test was performed, and a p value <0.05 indicated statistical significance. SPSS software (version 25.0; IBM, New York, NY, USA) and the R tool (version 4.1.1; R Foundation for Statistical Computing, Vienna, Austria) were used for statistical analysis.
Results
The comparison of baseline characteristics in HF population treated by different fluid administration strategies
Among the 3267 included patients with HF, there were 548 patients in the restrictive fluid intake group, 675 patients in the negative fluid balance group, and 2044 individuals in the unlimited fluid control group (Figure 1). During the median 3.41-day follow-up, the overall 28-day mortality rate was 14.3%, the 48-h AKI rate was 78.5%, the 7-day AKI rate was 86.0%, and the AKI progression rate was 16.2% (Table 1).
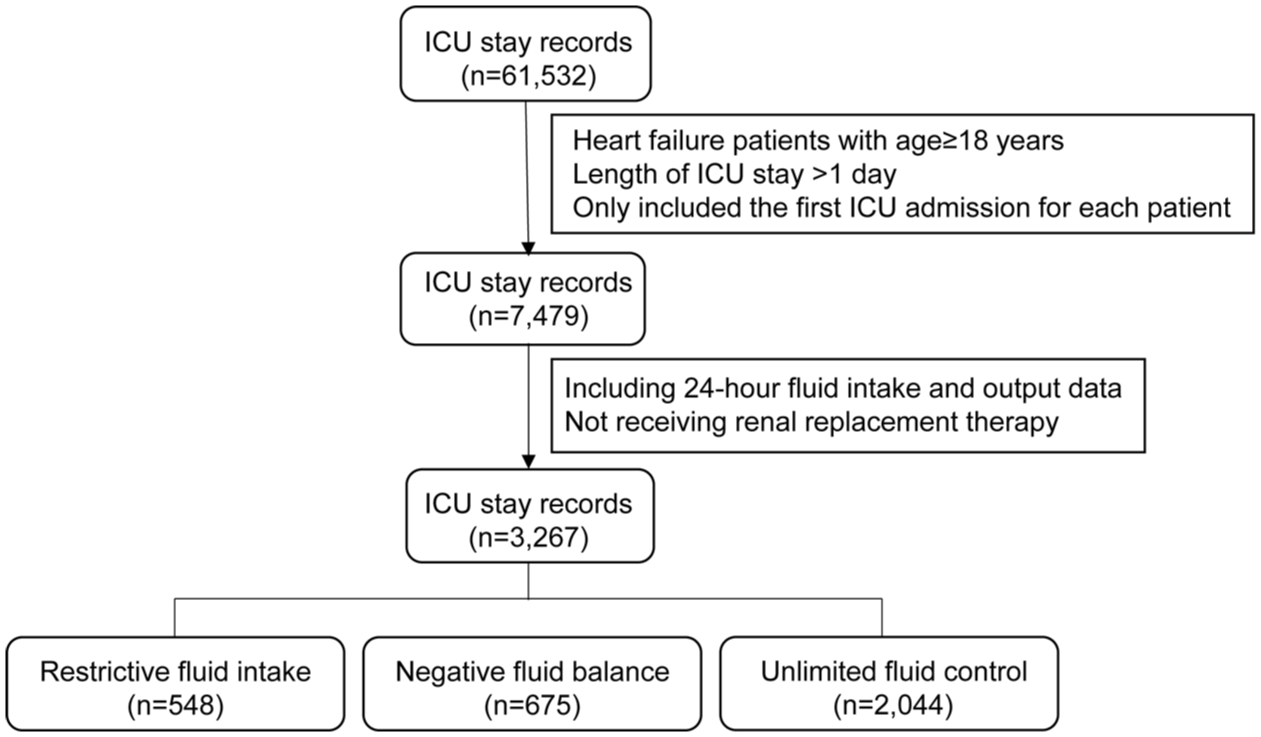
Flowchart of the inclusion of critically ill heart failure patients receiving restrictive, negative fluid balance, and unlimited fluid control in the intensive care unit.
Baseline characteristics of heart failure patients receiving restrictive fluid intake, negative fluid balance, and unlimited fluid control.
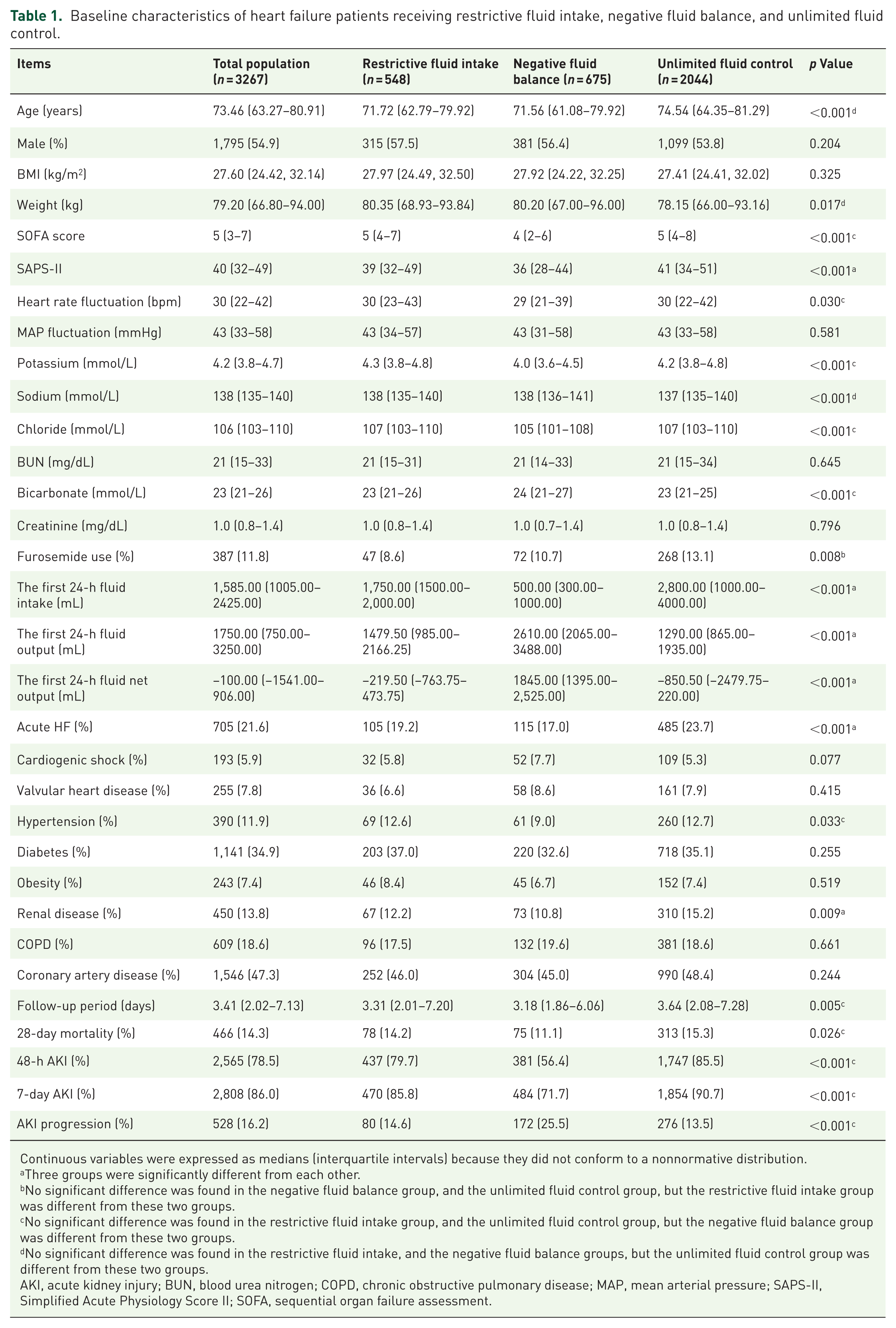
Continuous variables were expressed as medians (interquartile intervals) because they did not conform to a nonnormative distribution.
Three groups were significantly different from each other.
No significant difference was found in the negative fluid balance group, and the unlimited fluid control group, but the restrictive fluid intake group was different from these two groups.
No significant difference was found in the restrictive fluid intake group, and the unlimited fluid control group, but the negative fluid balance group was different from these two groups.
No significant difference was found in the restrictive fluid intake, and the negative fluid balance groups, but the unlimited fluid control group was different from these two groups.
AKI, acute kidney injury; BUN, blood urea nitrogen; COPD, chronic obstructive pulmonary disease; MAP, mean arterial pressure; SAPS-II, Simplified Acute Physiology Score II; SOFA, sequential organ failure assessment.
Age, SAPS-II score, sodium concentration, the ratio of furosemide use, and the prevalence of acute HF and renal disease were higher, while weight was lower, in the unlimited fluid control group compared to the restrictive and negative fluid balance groups (p < 0.05). The SOFA score, heart rate fluctuation, WBC, potassium concentration, chloride concentration, 28-day mortality, the incidence of 48-h and 7-day AKI, and the prevalence of hypertension were decreased in the negative fluid balance group compared to those in the restrictive and unlimited fluid control groups, while hemoglobin, platelet count, bicarbonate concentration, and the morbidity of AKI progression were higher in the negative fluid balance group compared to the restrictive and unlimited fluid control groups (p < 0.050). The morbidity of AKI progression from stage 0 to higher stages and from stage 1 to stage 2 was higher in the negative fluid balance group compared to the other two groups. The morbidity of AKI progression from stage 1 to stage 3 and from stage 2 to stage 3 was similar among the three groups (Table S3). Moreover, the first 24-h fluid intake in the negative fluid balance group (500.00 (300.00–1000.00) mL) was the lowest of the three groups, while the first 24-h fluid output (2610.00 (2065.00–3488.00) mL) and net output (1845.00 (1395.00–2525.00) mL) in the negative fluid balance group were the highest of the three groups (Table 1).
The relationship between fluid administration strategies and 28-day mortality and morbidity of 48-h AKI, 7-day AKI, and AKI progression identified by the logistic regression analysis
The multivariable logistic regression models were performed for the relationship between different fluid administration and mortality or AKI outcomes, which were adjusted by age, sex, weight, heart rate fluctuation, furosemide use, potassium, hypertension, and renal disease. Compared to unlimited fluid control, negative fluid balance was independently correlated to a lower 28-day mortality risk (OR (95% CI): 0.750 (0.570–0.987), p = 0.040), while restrictive fluid intake was not. Negative fluid balance and restrictive fluid intake were inversely associated with 48-h AKI (Negative fluid balance: OR (95% CI): 0.207 (0.169–0.255), p < 0.001; Restrictive fluid intake: OR (95% CI): 0.639 (0.498–0.819), p < 0.001) and 7-day AKI risk (Negative fluid balance: OR (95% CI): 0.261 (0.207–0.330), p < 0.001; Restrictive fluid intake: OR (95% CI): 0.589 (0.439–0.783), p < 0.001). Moreover, compared to unlimited fluid control, negative fluid balance was independently associated with AKI progression risk (OR (95% CI): 2.284 (1.835–2.843), p < 0.001), while restrictive fluid intake was not (Figure 2). The results from univariable models were consistent with those from the multivariable models (Figure S3).
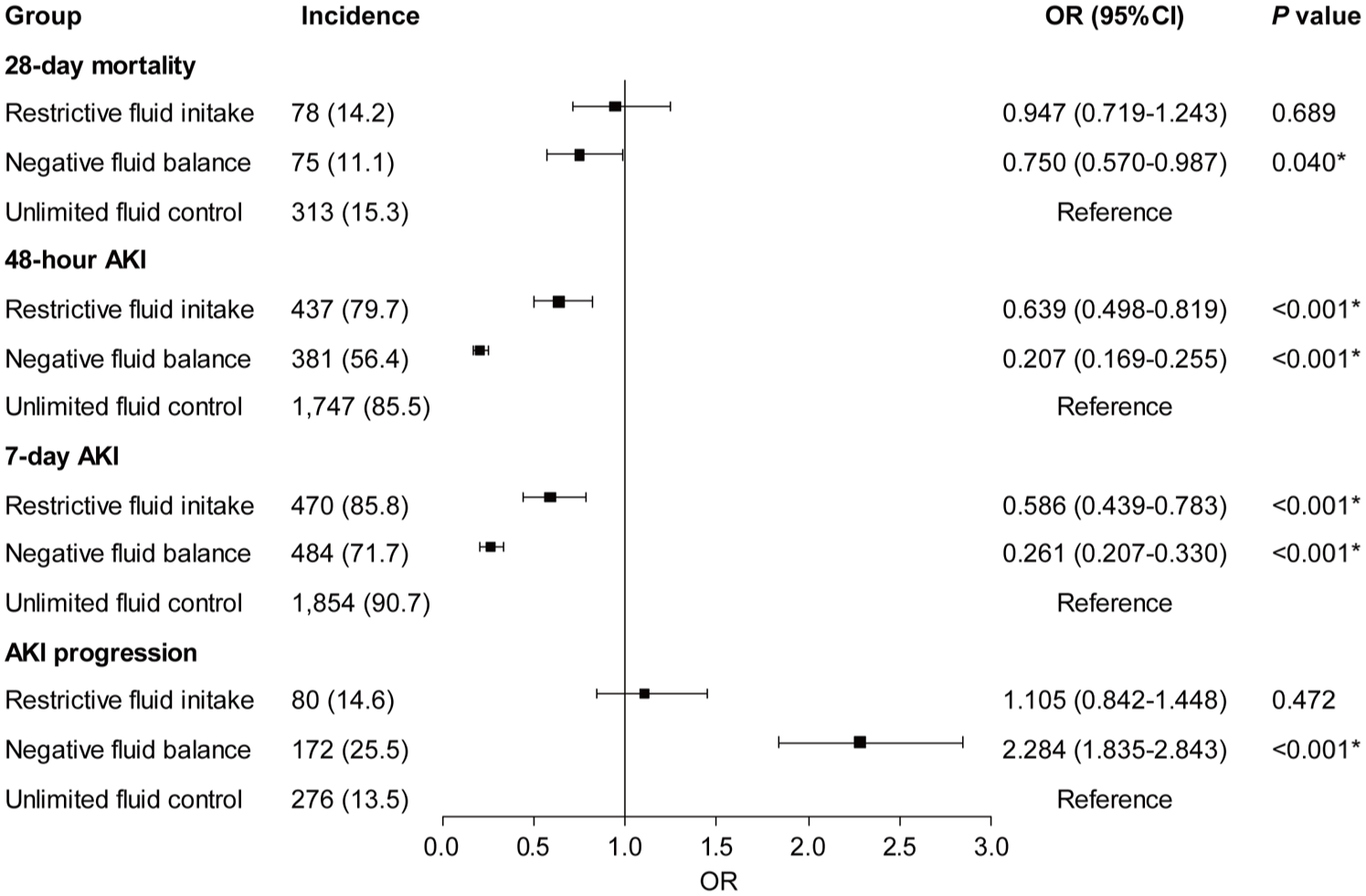
Forest plot for the multivariable logistic regression model of the association of fluid administration strategies with 28-day mortality, 48-h AKI, 7-day AKI, and AKI progression from 48 h to 7 days in critical ill patients with heart failure.
Subgroup analyses of the risk of four outcomes among three different fluid administration strategies
Only in subgroups of age ⩾60 years, female sex, patients without cardiogenic shock, patients without acute HF, and patients without furosemide use, negative fluid balance was inversely related to 28-day mortality compared to the unlimited fluid control group (Figure S4(A)). In all subgroups, negative fluid balance was inversely related to 48-h AKI and 7-day AKI compared to unlimited fluid control. Except for subgroups of age <60 years, male sex, cardiogenic shock, acute HF, heart rate fluctuation ⩾30 bpm, restrictive fluid intake was inversely related to 48-h AKI compared to unlimited fluid control (Figure S4(B)). Except for the subgroups of cardiogenic shock, acute HF, and furosemide use, restrictive fluid intake was inversely related to 7-h AKI compared to unlimited fluid control (Figure S4(C)). Moreover, negative fluid balance was positively related to AKI progression regardless of sex, cardiogenic shock, acute HF, heart rate fluctuation, and furosemide use (Figure S4(D)).
The first 24-h fluid output, correlated to weight, mediated the association between fluid administration strategies and outcomes
Body weight is an important indicator for fluid overload in HF and critical care, while BMI reflects more about metabolic conditions. To figure out whether weight or BMI was correlated to 24-h fluid intake/fluid output/net output, we performed the correlation analysis. Only weight was positively associated with 24-h fluid output. BMI showed no correlation to 24-h fluid intake or fluid output, or net output (Table 2).
The correlation of weight and body mass index with the first 24-h fluid intake, output, and net output.
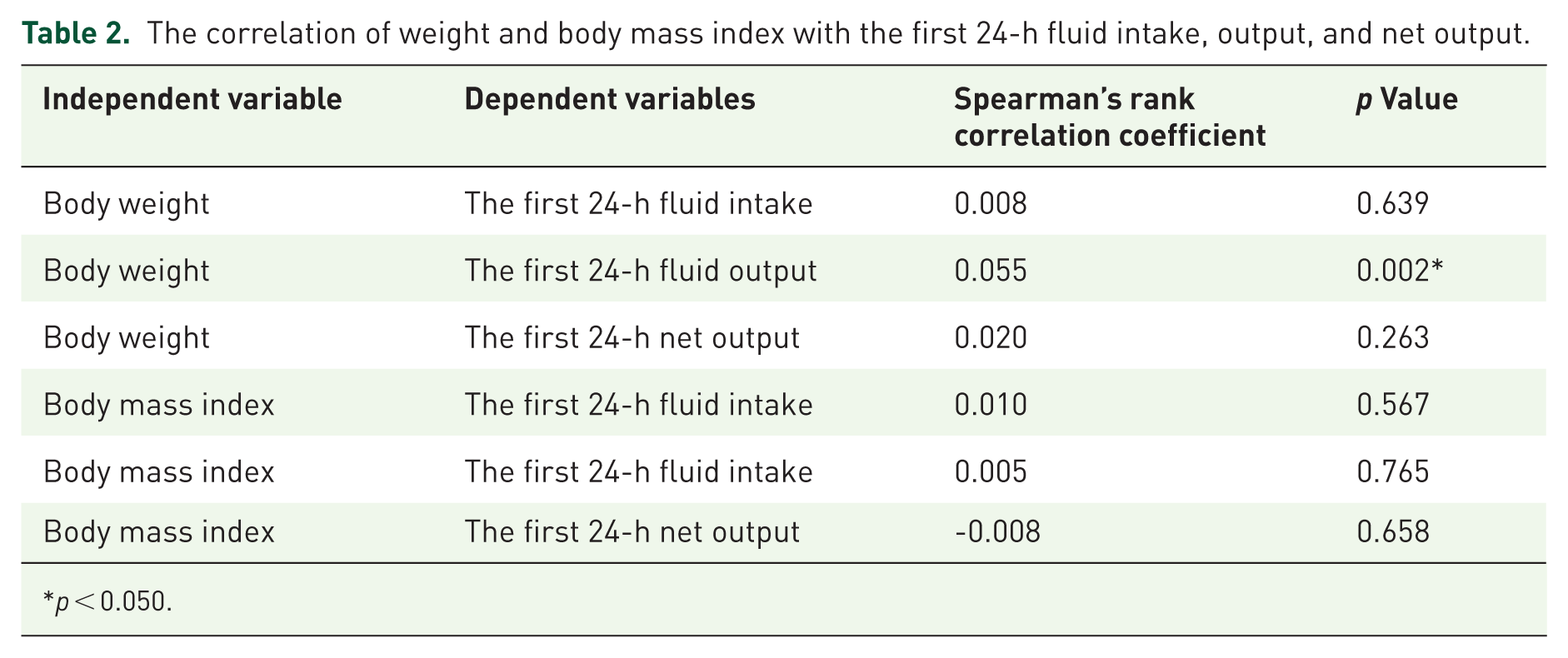
p < 0.050.
Since there was a positive correlation between weight and 24-h fluid output, the mediation effect of 24-h fluid output adjusted by weight, the ratio between these two variables, was also measured. We further investigated direct associations between 24-h fluid intake/fluid output/net output/body weight-adjusted output and four outcomes. The first 24-h fluid intake was inversely related to 28-day mortality but positively associated with 48-h AKI and 7-day AKI. The first 24-h fluid intake was not associated with AKI progression. The first 24-h fluid output, net output, and body weight-adjusted output were inversely related to 28-day mortality and 48-h AKI and 7-day AKI but positively associated with the incidence of AKI progression (Figure 3). The results from univariable models were consistent with those from the multivariable models (Figure S5).
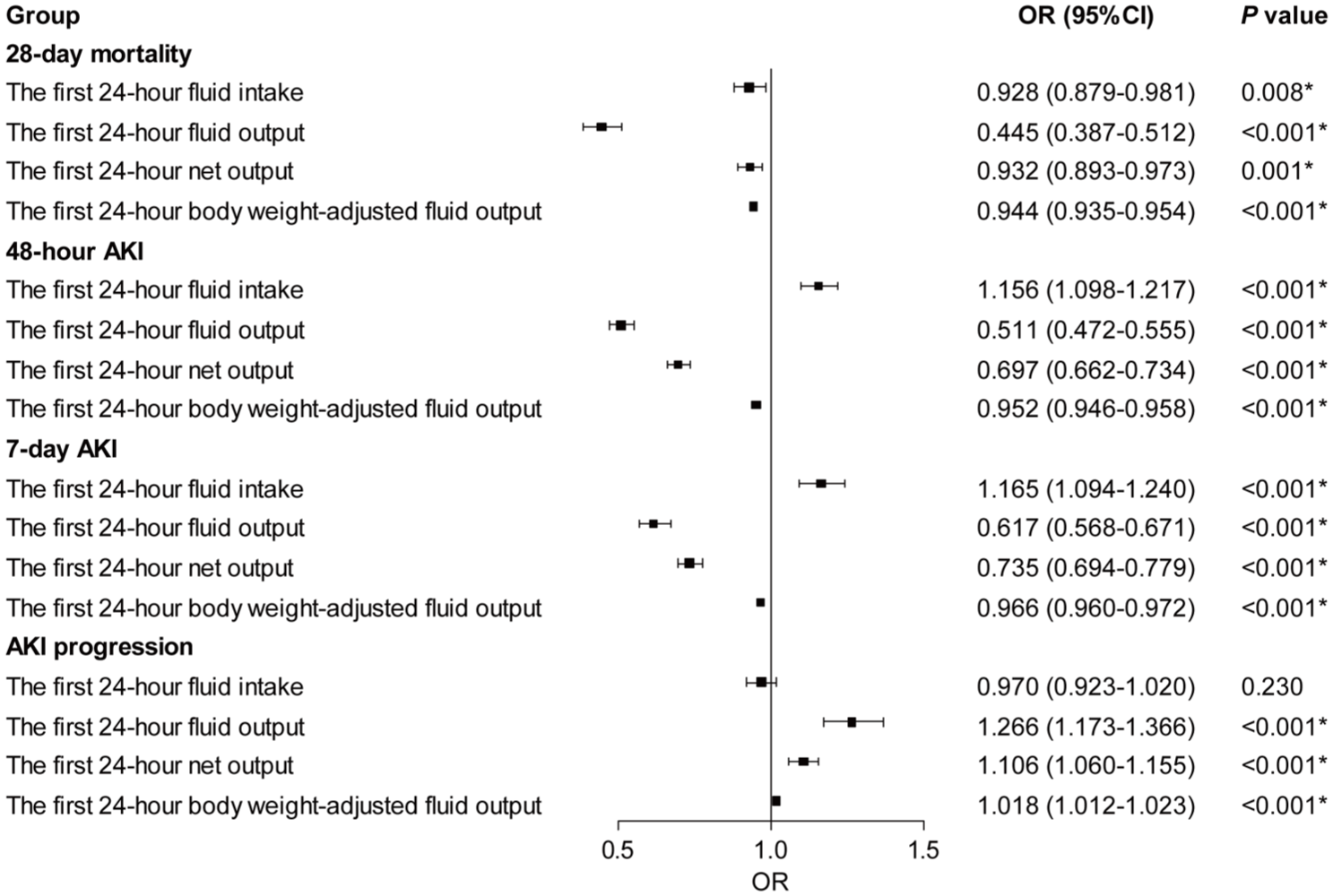
Forest plot for the multivariable logistic regression model of the association of the first 24-h fluid intake/fluid output/net output/body weight-adjusted output with 28-day mortality, 48-h AKI, 7-day AKI, and AKI progression from 48 h to 7 days in critical ill patients with heart failure.
To compare the contributions of 24-h fluid intake/fluid output/net output to the impact of fluid administration strategies on outcomes, mediation analyses were performed. The 24-h fluid output mediated the association between fluid administration and 28-day mortality risk. The 24-h fluid intake, the 24-h fluid output, and the 24-h net output all mediated the association between fluid administration strategies and 48-h AKI, 7-day AKI, and AKI progression. The proportions of mediation of 24-h net output were the highest among the three groups: 59.7% for 48-h AKI, 52.8% for 7-day AKI, and 59.6% for AKI progression. The proportions of mediation of 24-h fluid output were 43.1% for 48-h AKI, 13.1% for 7-day AKI, and 22.8% for AKI progression. The mediation effect of 24-h fluid intake was the lowest among the three groups. The proportions of mediation of 24-h body weight-adjusted fluid output were 33.3% for 48-h AKI and 27.5% for 7-day AKI. The mediation effect of 24-h fluid intake/fluid output/net output on the association between fluid administration strategies and outcomes was not significant with either negative effect values or proportion of mediation >1 (Table 3).
The mediation effect of 24-h fluid intake/fluid output/net output on the association between fluid administration strategies and outcomes.
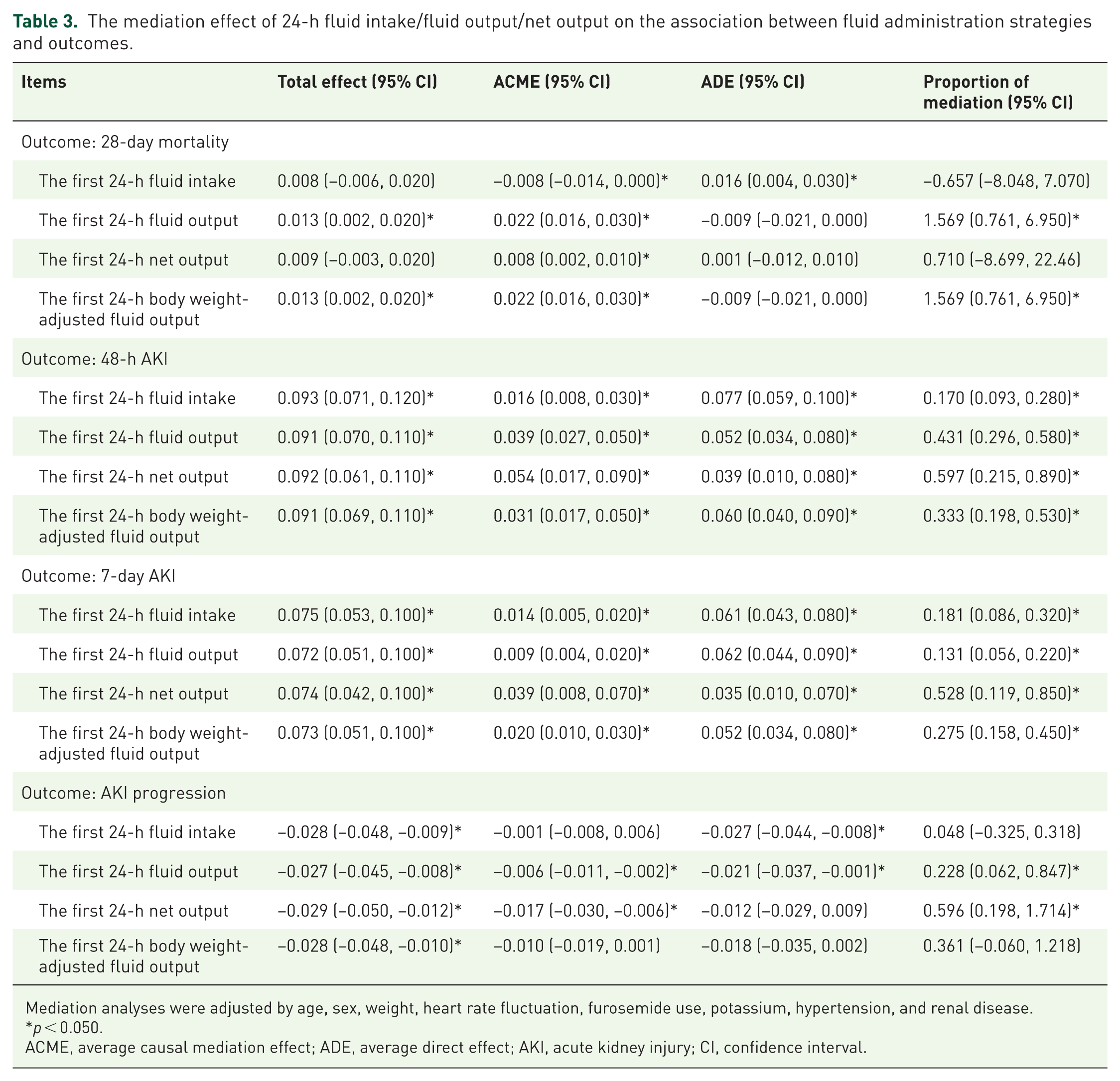
Mediation analyses were adjusted by age, sex, weight, heart rate fluctuation, furosemide use, potassium, hypertension, and renal disease.
p < 0.050.
ACME, average causal mediation effect; ADE, average direct effect; AKI, acute kidney injury; CI, confidence interval.
Discussion
The benefit of negative fluid balance has seldom been considered in previous studies comparing restrictive and liberal fluid administration, although it is important in clinical decisions on fluid administration. In this retrospective cohort of patients with critically ill HF, negative fluid balance was independently related to lower 28-day mortality and lower 48-h AKI and 7-day AKI but higher AKI progression compared to the unlimited fluid control group after adjustment for age, sex, weight, heart rate fluctuation, furosemide use, potassium, hypertension, and renal disease. Restrictive fluid intake was associated with a lower risk of 48-h and 7-day AKI, but was not associated with mortality or AKI progression. All the 24-h fluid intake, output, and net output mediated the association between fluid administration and AKI incidence. However, only the fluid output mediated the association with short-term mortality, while the net output mediated the association with AKI progression. Hence, the first 24-h negative fluid balance may be a better option for prognostic improvement in critically ill patients with HF, mainly benefits from fluid output, but the impact of net output on AKI progression should be monitored. This study provided supportive evidence for the benefit of the negative fluid balance decision to improve cardio-renal prognosis, but the monitoring for renal function should be considered to prevent potential AKI progression. The retrospective data-based evidence exhibited important reference value but required further validation by prospective interventional studies.
Restrictive fluid intake and liberal fluid control are two common fluid management strategies for patients with HF.6,7 Current clinical guidelines and consensus statements suggest restricting fluid to 1500–2000 mL per day in patients with severe HF to relieve congestive symptoms, but the recommendation was downgraded.10,20 Evidence from meta-analyses of RCTs did not demonstrate different risks of HF-related hospitalizations, death, duration of diuretic drug, or serum sodium concentrations between restrictive and liberal fluid administration strategies in patients with HF.6,7 Previous RCTs revealed that aggressive fluid and sodium restriction was unnecessary for patients with acute or chronic HF due to increased thirst and no improvement of weight loss, congestion symptoms, or readmission rate.21,22 A meta-analysis on RCTs demonstrated that fluid restriction only reduced fluid intake but did not improve prognosis of mortality, hospitalization, or AKI incidence. 23 The result was consistent with our results of similar mortality risk between restrictive fluid intake and unlimited fluid control. A reduced risk of 48-h and 7-day AKI by restrictive fluid intake compared to the unlimited fluid control was also identified in this study, although AKI progression was not affected. Among patients undergoing major abdominal surgery, the mortality and AKI incidence were also higher in patients receiving restrictive fluid intake than those receiving liberal fluid intake. The need for renal replacement therapy was also higher in the restrictive fluid intake group. 5 Current evidence did not support fluid restriction to reduce mortality or AKI risk for patients with HF or other non-cardiovascular diseases. Restrictive fluid intake could aggravate the insufficient renal filtration in patients with HF who tended to be treated with enhanced decongestive drugs, which was also revealed by the unaffected 7-day AKI risk in the subgroup with furosemide use. Shen et al. reported a reduced mortality risk associated with increasing fluid intake and output in critically ill patients achieving negative fluid balance, 24 indicating the stronger mediation effect of fluid output over intake in acute medical management. Net fluid output was not considered in fluid management in these studies, and the benefit to enhance output rather than fluid restriction for negative fluid balance has raised more attention in clinical practice. However, the impact of the negative fluid balance strategy on short-term mortality and AKI incidence in patients with HF has not been fully investigated.
Negative fluid balance has not been compared with restrictive fluid intake due to different focuses on net output and fluid intake. In this study, we were the first to combine the net output and fluid intake into categorization for fluid administration to investigate the efficacy of negative fluid balance management with a net output >1000 mL without fluid restriction compared to restrictive fluid intake and unlimited fluid control. Negative fluid balance was associated with an increasing mortality risk, a reduced AKI risk in 48 h and 7 days, but an increasing risk of AKI progression. The first 24-h intake in patients treated with negative fluid balance was less than that in patients treated with restrictive fluid intake in this study, and less fluid intake was inversely related to lower 48-h and 7-day AKI. The positive fluid balance was positively related to a more severe AKI stage and a lower possibility of renal function recovery. 8 A reduction of cardiac output by HF causes low kidney perfusion and low peripheral blood pressure. Increased early fluid reduction was demonstrated to be related to a shorter length of hospital stay and improvement in the estimated glomerular filtration rate at 72–96 h. 25 Negative fluid balance helps to relieve circulatory volume load, and increase cardiac output to improve kidney perfusion. However, the risk of AKI progression was increased by negative fluid balance, which has not been identified currently. The incidence of AKI is decreased by negative fluid balance, but the remnant acute kidney dysfunction may not be fully recovered. 26 Potential mechanisms and manifestations could be: (1) Inadequate decongestion: The cardio-renal interplay in the acute phase of HF was unstable, making the inadequate decongestion unidentified. A <30% decrease in BNP could worsen the renal function in patients with acute HF 27 ; (2) Susceptibility to sepsis: Although over 80% patients could be recovered from AKI, about 50% had high susceptibility to sepsis related to cardio-renal dysfunction 28 ; (3) Time-related kidney injury: early and sustained reversal of AKI decreased mortality risk compared to relapses after reversal, 29 indicating an irreversible renal change contributing to recurrent kidney injury. These potential pathophysiological changes could promote the short-term AKI progression even the AKI risk was reduced. Existing studies showed no significant differences between restricted and liberal fluid intake, but the heterogeneity and small-study effect hindered the interpretation. 30 The mediation of the fluid output on the negative relationship between 24-h intake and 28-day mortality could not be excluded in this study because the net output was less in the unlimited fluid control than the restrictive fluid intake. Furthermore, an elevation of the very early diuretic response in patients admitted to the emergency department has been demonstrated to be independently correlated with 60-day mortality, and the change in diuretic response provided additional prognostic ability. 31 The 28-day mortality risk was not reduced by negative fluid balance in the subgroup receiving furosemide use in this study, which might be partially affected by the early diuretic response. The reduced risk of AKI incidence and the increasing risk of AKI progression remained significant irrespective of the diuretic use. Hence, the negative fluid balance should be considered prior to the mere restrictive fluid intake in early fluid administration of critically ill HF, but the monitoring of kidney function should be aware.
The interaction between fluid intake and output determines the extent of fluid balance, but the contribution of the intake and the output to HF prognosis has not been clarified. In this study, we investigated the impact of the first 24-h fluid intake, urine output, and net output on 28-day mortality and AKI incidence. Indicated by the positive association of the first 24-h fluid intake with the AKI risk but the negative association with the mortality risk, the fluid output could also mediate the fluid balance-related prognosis. Both the first 24-h urine output and net output were positively correlated with lower 28-day mortality, 48-h AKI, and 7-day AKI but higher AKI progression, which indicated that a risk of a potential development of renal impairment might exist in the negative fluid balance group, although the incidence of AKI was low. A pilot trial of patients with AKI comparing the efficacy between restrictive fluid intake with negative fluid balance and usual care revealed a lower use of renal replacement therapy, cumulative fluid balance at 7 days, and adverse events in AKI patients receiving restrictive fluid intake. 18 The increasing fluid intake in addition to negative fluid balance also reduced the mortality risk among critically ill patients with increasing fluid output. 24 These findings supported the effective combination of restrictive fluid intake with negative fluid net output to protect renal function in critically ill patients. Moreover, 24-h net output and 24-h fluid output contributed higher proportions of mediation effect on the impact of fluid administration strategies on 48-h AKI and 7-day AKI outcomes than 24-h fluid intake, emphasizing the importance of negative fluid balance in fluid management. Both fluid intake and output correlated with and participated in the association with AKI outcome risk, but the fluid output and the net output could further mediate mortality risk and AKI progression risk. The distinct role in the associations with mortality and AKI outcomes reflected the different importance of the impact of fluid intake and output, and the fluid output might play a dominant role in affecting mortality. The AKI progression might be mediated by the negative fluid balance, and thus, monitoring of renal functions under the negative fluid balance should be considered to avoid unexpected adverse events in the rescue of critically ill HF.
Body weight is an important indicator for evaluating fluid overload in HF and critical care, but the interpretation of volume response and nutrition status could be indistinguishable. There were controversial results about whether weight loss worsened the prognosis among HF patients.32,33 In this study, body weight was higher in restrictive fluid intake and negative fluid balance groups, indicating that higher body weight required a fluid net output against congestive symptoms. Body weight, not BMI, was positively associated with 24-h fluid output, indicating that fluid overload contributed to acute HF more than metabolic conditions. Previous studies used to adjust the fluid intake by body weight, and found a positive relationship between fluid intake and mortality risk in patients with cardiac arrest. 34 A rapid transition to negative fluid balance helps to reduce mortality risk in these patients, irrespective of the complication with myocardial infarction.35,36 However, both body weight and fluid intake were dynamically changed during the acute phase of HF, and were affected by several factors, in which the fluid output might mainly contribute. Previous studies did not adjust the fluid balance by body weight, and the unadjusted positive fluid balance predicted an increase in in-hospital mortality in critically ill patients with cardiac diseases.37,38 In this study, the 24-h fluid intake, output, and net output were selected because of the importance of the first-day treatment and the high mortality risk. 39 The 24-h fluid output mediated the impact of fluid administration strategies on mortality risk, 48-h AKI, and 7-day AKI outcomes after being adjusted by body weight or unadjusted in patients with HF, indicating the independent mediation effect of 24-h fluid output. Hence, although the body weight provided important references, the levels of fluid output and net output should be priorly focused on in the emergency treatment for critically ill patients with HF.
Subgroup analyses showed a stable association between fluid administration and outcomes in most subgroups, but also discovered distinct associations of fluid administration with the risk of mortality and AKI incidence in some specific subgroups. The protective effect of negative fluid balance against 28-day mortality risk was compromised in subgroups with age <60 years, male, cardiogenic shock, acute HF, heart rate fluctuation <30 bpm, and furosemide use. Age, sex, and multimorbidity did not affect the negative association between fluid balance and mortality risk in critically ill patients with HF and sepsis. 40 The division thresholds of age, heart rate fluctuation, and furosemide use in the negative fluid balance group were lower than the median levels in the included patients, and the relatively small sample might neutralize the protective effect of negative fluid balance. On the contrary, the high mortality risk associated with the presence of cardiac shock and acute HF could offset the benefit of negative fluid balance. 41 Moreover, the AKI risk associated with the restrictive fluid intake was also compromised in the subgroups with cardiogenic shock and acute HF. AKI is a common and early complication of cardiogenic shock and acute HF, mainly caused by venous congestion and severe hypoperfusion. 42 The hemodynamic dysfunction could be aggravated by the fluid restriction in severe cardiac diseases. An aggressive fluid resuscitation is necessary for cardiogenic shock patients to reduce the risk of mortality and post-arrest AKI, which has an early onset and is prevalent, 43 but a large fluid intake for patients after cardiac arrest should be guided by hemodynamic monitoring to reduce the total fluid intake and the incidence of AKI. 44 Fluid restriction did not affect the risk of 48-h AKI in the subgroup with heart rate fluctuation over 30 bpm, which also represented an unstable cardiac function to increase mortality risk as revealed by our previous study. 12 Among patients aged <60 years, negative fluid balance was not associated with AKI progression. The better kidney recovery in younger adults than in patients aged over 65 years could possibly contribute to reduce the negative fluid balance-associated AKI progression. 45 Hence, the cardio-renal benefits of fluid administration strategies were impaired in patients with cardiogenic shock and acute HF. The fluid resuscitation was important for emergency treatment in these patients, but required strict monitoring to avoid drastic hemodynamic fluctuation. The negative fluid balance might be effective in younger critical ill patients with HF with low risk of AKI progression, but the effectiveness needs prospective validation.
Previous studies mainly focused on the single evaluation of fluid intake and fluid balance for the prognosis of either mortality or AKI incidence in critically ill patients with cardiac diseases. This study novelly combined fluid intake and net output to directly compare the prognostic differences in mortality and AKI outcomes among restrictive fluid intake, negative fluid balance, and unlimited fluid control, which emphasized the important role of fluid output to mediate the prognostic association between fluid administration and outcomes. Nevertheless, there were some limitations in this study. First, the retrospective cohort study design limited the interpretation of the causal relationship between fluid administration and outcomes without randomized allocation. The unbalanced distribution of different fluid administration strategies was inevitable because the decision could be affected by complex clinical situations. Over 10% missing values of furosemide dose, BNP, and left ventricular ejection fraction made it difficult to assess whether the efficacy of the negative fluid balance strategy was affected by diuretic therapy or cardiac function in patients with HF. A prospective and randomized controlled validation is required for the effectiveness of the negative fluid balance. Second, the selection of the fluid intake and output was limited to the first 24 h, which was commonly used by previous studies for the importance of this treatment timing.38,40 The use of the first 24-h fluid intake and output to predict AKI progression could not reflect the dynamic modulation of fluid balance to renal function. The trajectory of fluid balance provided additional information for the cumulative fluid load during the AKI development,35,36 but the extent and high-risk duration should be determined in future studies. Third, the AKI definition was based on creatinine and urine output, and the creatinine-based criteria could be associated with a delayed identification of renal recovery. 46 Baseline lower AKI stages were susceptible to AKI progression associated with negative fluid balance, but the advanced baseline AKI were not significantly progress by fluid administration in this study. A more sensitive marker to detect the continuous AKI progression could better reflect the quantitative relationship between fluid balance and renal function changes. Novel metrics for renal function with high sensitivity were needed for a comprehensive and early evaluation of renal function recovery and progression. The AKI progression was assessed by the changes from 48 h to 7 days, and a serial monitoring of renal function was not performed, which should be considered for the precise tracking on AKI in future studies. Moreover, the renal replacement therapy was not considered because their hemodynamics and fluid burden were affected differently from those not receiving renal replacement therapy, making the application of fluid administration complicated. The benefits of negative fluid balance under complex hemodynamic dysfunction induced by severe cardiac diseases, combined with renal replacement therapy required well-designed investigation in the future. Hence, the efficacy and safety of first-day fluid administration is worth investigating to reduce short-term mortality and avoid renal function impairment.
Conclusion
A first-day negative fluid balance is associated with lower short-term mortality and AKI incidence but a higher risk of AKI progression in critically ill patients with HF. Both 24-h fluid output and net output mainly mediated the impact of fluid administration strategies on AKI incidence and progression. The protection and monitoring of renal function during the emergent fluid administration should be considered, and novel renal injury measurement might provide additional information for comprehensive evaluation. Further RCTs are needed for the efficacy and safety assessment of negative fluid balance.
Supplemental Material
sj-docx-1-tak-10.1177_17539447261457542 – Supplemental material for The first 24-h negative fluid balance is related to lower short-term mortality but higher AKI progression in critically ill heart failure: a retrospective cohort study
Supplemental material, sj-docx-1-tak-10.1177_17539447261457542 for The first 24-h negative fluid balance is related to lower short-term mortality but higher AKI progression in critically ill heart failure: a retrospective cohort study by Wenhao Liu, Qian Chen, Tucheng Huang, Juanzhang Liu, Hongwei Li and Qi Guo in Therapeutic Advances in Cardiovascular Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.