
Abstract
Diagnostic medical errors represent a significant cause of morbidity and mortality, and reflecting on the causes behind them can be a great source of learning to practitioners. Adverse medical events are costly and can have a dramatic impact, not only on patients themselves but also their loved ones. In addition, diagnostic interventions are becoming increasingly complex, potentially opening the door for greater iatrogenic harm. Health care services have recognised the need for action to improve patient safety and have implemented system-wide changes that have had far reaching benefits. However, measures focused on streamlining the thought processes required for accurate diagnosis have been more difficult to implement. Many cognitive errors are modifiable, making it possible for physicians to improve their diagnostic reliability. This article describes the types of errors that may be made when forming a diagnosis and suggests some strategies to reduce diagnostic error, hence improving clinical practice.
The GP curriculum and diagnostic error
The Manage primary contact with patients and deal with unselected problems Develop the clinical skills needed to ensure that a thorough history-taking leads to the correct diagnosis Be aware of subjectivity in the medical relationship, from both your patient’s side (feelings, values and preferences) and from your side (self-awareness of values, attitudes and feelings) Develop your skills in specific decision-making (using tools such as clinical reasoning and decision rules) Understand and accept the inevitable uncertainty in primary care problem- solving and the need for development of strategies that demonstrate this
Introduction
In the past decade or so there has been an increased focus on patient safety in health care organisations such as the National Health Service. Although significant medical errors occur in less than 5% of patient contacts, this is still significantly higher than that recorded in comparable industries such as aviation (Berner & Graber, 2008). It has been estimated that errors occur in around 1 in 120 general practice consultations in the UK (Bowie, Pope, & Lough, 2008). Moreover, medical errors may be under-reported due to the prevailing culture in medicine that medical adverse events are exceptional and occur primarily by chance. This may be partly because of the difficulty experienced by medical staff in coming to terms with the consequences of such errors (Leape, 2009).
Errors can generally be viewed according to one of three models:
The ‘legal model’ of error describes the duty of care that one individual has to another and the consequences if that duty is breached The ‘system model’ adopts an organisational view of error and considers that the individual making the error only does so because of defects in the system that allows them to occur Lastly, the ‘personal model’ considers individual human fallibility as the source of the erroneous act (Reason, 2000)
Making mistakes is part of human nature thus we would do well to adopt a personal- and system-based view of errors that have happened, as the legal view demands perfection at all times. This would focus our collective efforts on the positive aim of reducing harm rather than merely fixating on the negative consequences of errors. This strategy has certainly served the airline industry well in its quest to improve safety, and has steadily gained momentum in medical circles (Kassirer & Kopelman, 1989).
Diagnostic errors are costly. They account for a significant proportion of litigation in medicine, carry a high morbidity and are often preventable. The diagnostic process is multifactorial and complex, and is therefore open to a wide variety of errors. Recognising the common errors of diagnosis can be especially beneficial to junior doctors who are usually the first point of contact for new patients in the hospital setting. However, some diagnostic errors are independent of experience and apply to all physicians (Croskerry, 2003a).
The types of diagnostic error are summarised in Fig. 1. Unsurprisingly, the clinical situations that are most likely to cause diagnostic delay or error are general practice and accident and emergency. Physicians in these specialities are often the first point of contact with patients who present acutely with new symptoms - and who represent the greatest diagnostic challenge.
A summary of the classification of diagnostic error.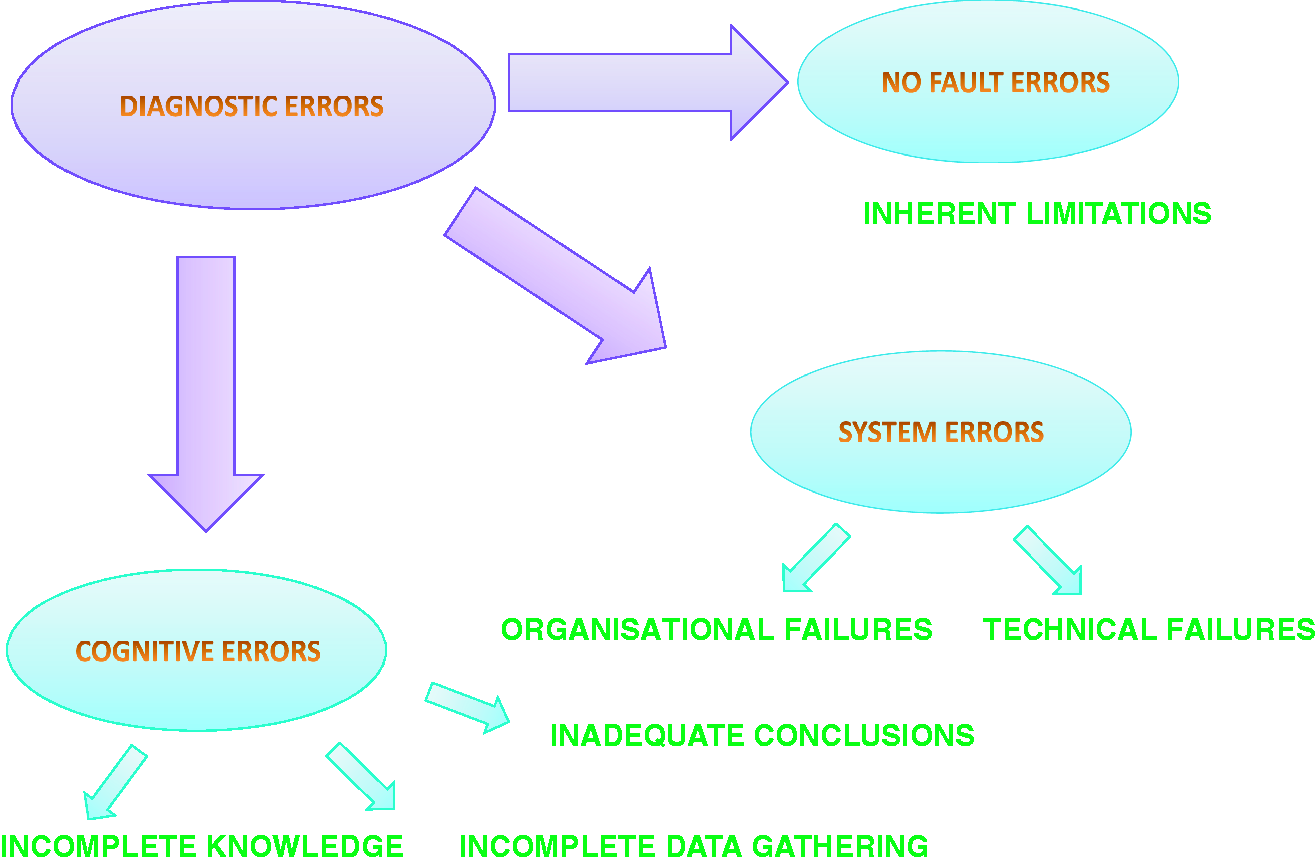
The diagnostic process
The process of making a diagnosis from the available data can be complex. In the real world, diseases present over time in a dynamic fashion and therefore not all the data is available from the outset. Diagnosis differs from events in other safety-conscious professions (such as aviation) because of this, and the human factors involved can make it difficult to draw direct comparisons. Physicians must make a diagnosis by integrating what they already know on a personal level and what they can source from knowledge-based resources (Friedman et al., 2005). This process is partly automatic (like driving a car) and partly a function of higher-order consciousness (Graber, 2009).
The two main cognitive processes in making a diagnosis are essentially pattern recognition and hypothetico–deductive reasoning. In the early stages of their careers, physicians are more likely to employ hypothetico–deductive reasoning, which is scientifically valid but requires greater higher-order processing skills. As physicians gain experience they are more likely to employ subconscious pattern recognition, as they will be more familiar with the variety of ways that a disease can present. Pattern recognition is beneficial in that it requires less cognitive effort, but it is more likely to be subjective and becomes less reliable when the presentation fails to fully fit into a recognised pattern.
Ideally, the diagnostic process should involve a flexible combination of pattern recognition and hypothetico–deductive reasoning with constant reflection between the thought processes (Kuhn, 2002). Croskerry’s model of how the diagnostic processes change over time is given in Fig. 2.
A summary of how the process of formulating a diagnosis changes with time.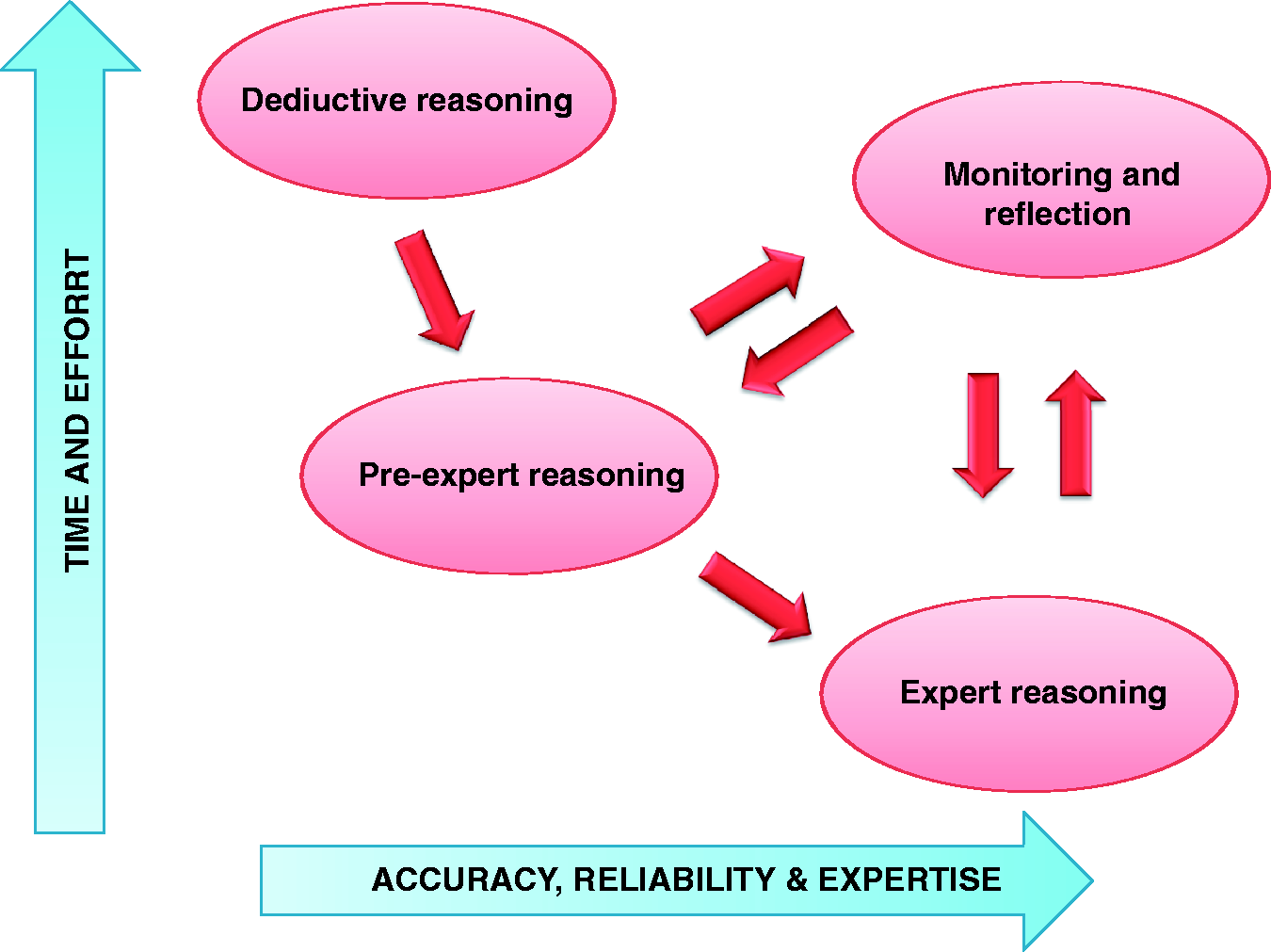
The formation of a hypothesis occurs at different rates, depending on which thought process is employed. It typically begins within the first 10 seconds if pattern recognition is employed and within 30 seconds if hypothetico-deductive reasoning is used. As such the hypothesis is subject to bias and error, which will only increase with the complexity of the data being analysed. An accurate impression from the patient history and examination is essential to order the appropriate diagnostic tests. Flawed assumptions from the early part of the consultation may explain why advances in medical technology have not fully correlated with similar advances in diagnostic accuracy (Kuhn, 2002).
Types of diagnostic error
No fault errors
‘No fault errors’ are difficult to eradicate completely as they occur primarily as a consequence of limitations of medical knowledge. They may also occur when a disease presents in an unusual fashion, such as an atypical presentation of myocardial infarction in an elderly patient. It is only advances in scientific research that can reduce these errors, by providing increased knowledge of how diseases present.
Other ‘no fault errors’ can be considered to be patient- or physician-based events. An example of a physician-related error would be making a working diagnosis based on the most likely explanation for a cluster of symptoms when the patient actually has a much more rare cause. Patient-related errors could be due to human factors, such as being lost to follow up, or patients failing to mention a key symptom because they are unaware of its importance. These variances are attributed to the world being imperfect and are referred to as a ‘necessary fallibility of the human condition’ (Gorovitz & MacIntyre, 1975).
System errors
System errors occur due to imperfections that exist within the healthcare organisation. These imperfections may be attributed to an individual at the point of patient contact, to the organisation as a whole, or to any subset of personnel between these two extremes. System errors may be further subclassified into technical failures and organisational failures.
Technical failures occur when an investigation fails to answer the clinical question being asked. Examples of this include negative blood tests due to the margins of error of the laboratory tests or inconclusive imaging due to the limits of resolution of the equipment. Fortunately, these errors are becoming less of an issue as manufacturers address concerns and make tests more accurate.
A summary of some common system-based errors.
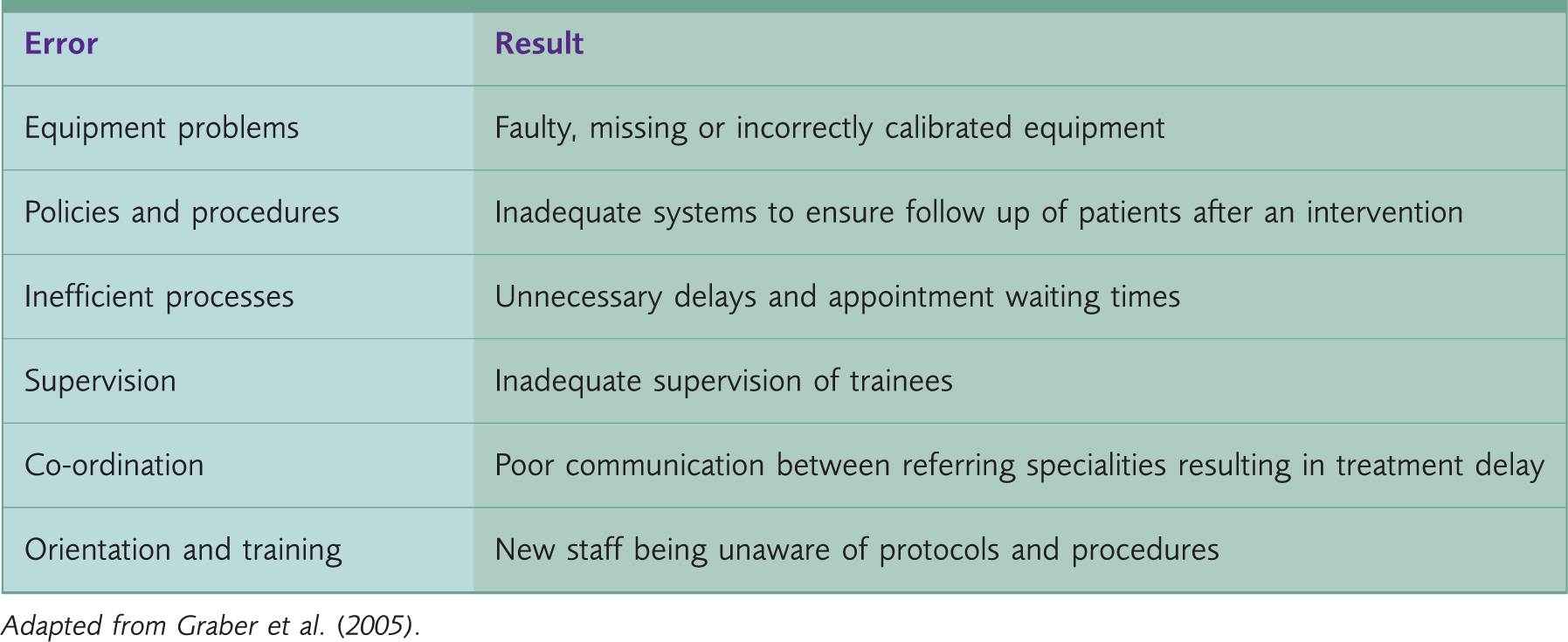
Adapted from Graber et al. (2005).
Cognitive errors
Three types of cognitive processes apply to medicine – skill-based (procedures such as catheterisation), rule-based (e.g. following clinical guidelines) and knowledge-based (such as diagnostic reasoning). The degree of higher-order input, and therefore the potential for error, escalates with the complexity of the task at hand. However, as clinicians gain competence, the degree to which knowledge-based decisions utilise cognitive processes declines due to the development of pattern recognition, which can only come with experience (Croskerry, 2003a).
A summary of some important cognitive errors in diagnosis.
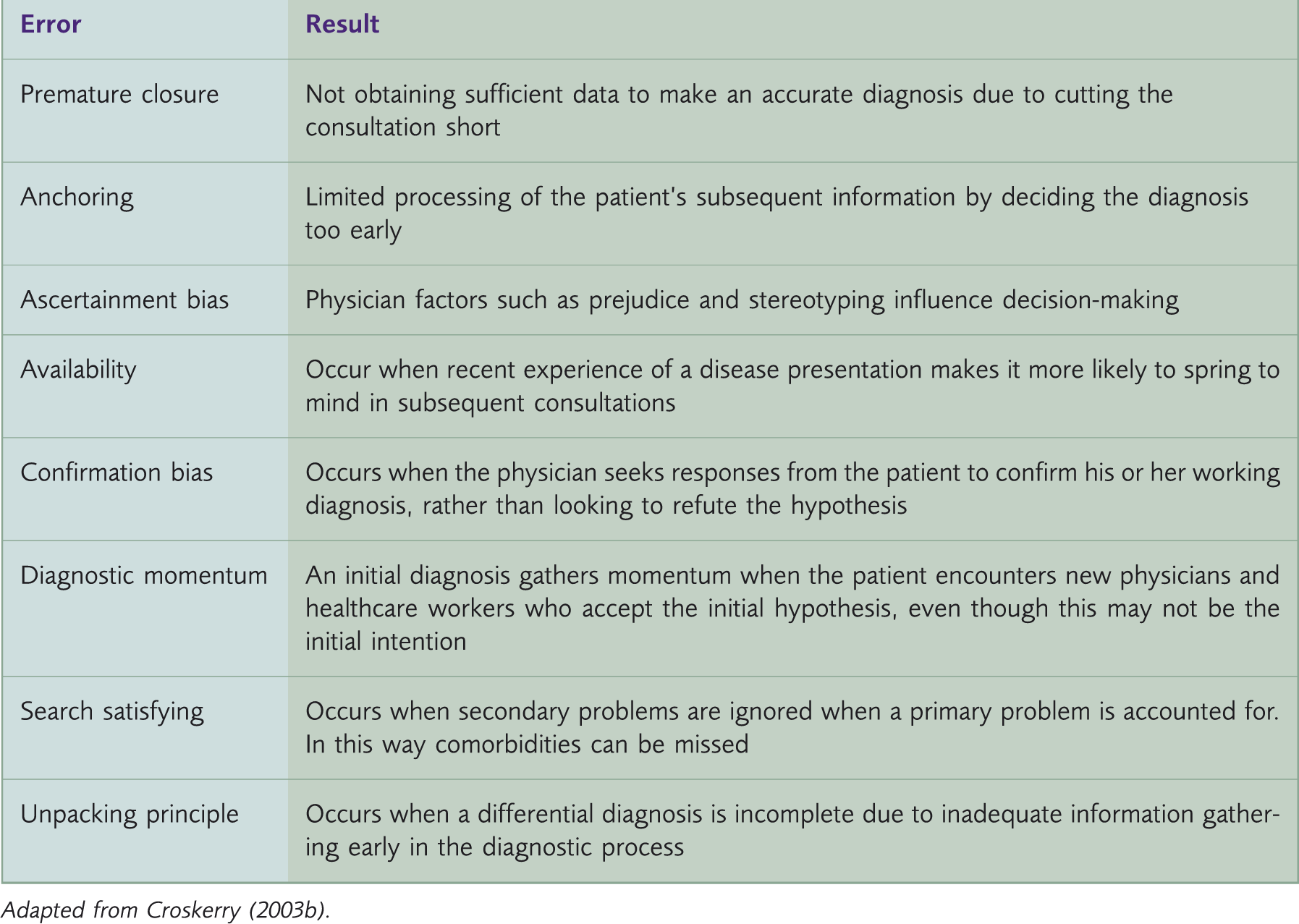
Adapted from: Croskerry (2003b) .
Interestingly, the cognitive errors of omission and inadequate synthesis of data are more likely to be committed by junior physicians, while premature closure of the consultation stems from the increased time pressure and overconfidence more likely to be seen in more experienced physicians (Graber et al., 2002). Furthermore, premature closure is more likely to occur in pressure situations where there is a need for a rapid diagnosis, such as in an emergency, and is the most frequently encountered cognitive error overall (Graber, Franklin, & Gordon, 2005). Anchoring is another cognitive error that has been shown to be independent of experience and is therefore the subject of much interest, as senior physicians are as likely to fall into this trap as junior physicians (Kuhn, 2002).
Methods of reducing system-based error
Naturally, the first step in improving patient safety is analysing the mechanisms of how adverse events occur. Health care organisations have taken great strides in reducing system-based errors and continue to make progress in this regard. For this to continue, we must all accept that errors are inevitable and to veer away from the prevailing culture of perfectionism and blame. Some interventions are simple such as ensuring that staff are not overworked and therefore in the best frame of mind to make clear decisions. Others can be more nebulous, including attempts to modify the organisational culture. Unfortunately, improvements in one aspect of the organisation can adversely affect another, for example, reducing shift length may improve a clinician’s clarity of thought but may also create difficulties in coordinating work rotas (Graber et al., 2002).
Systems are designed to reduce error in three ways:
Preventing errors from occurring in the first place Highlighting errors when they do occur; and/or Limiting the damage caused by an error which has taken place (Nolan, 2000).
Strategies used to reduce system-based errors.
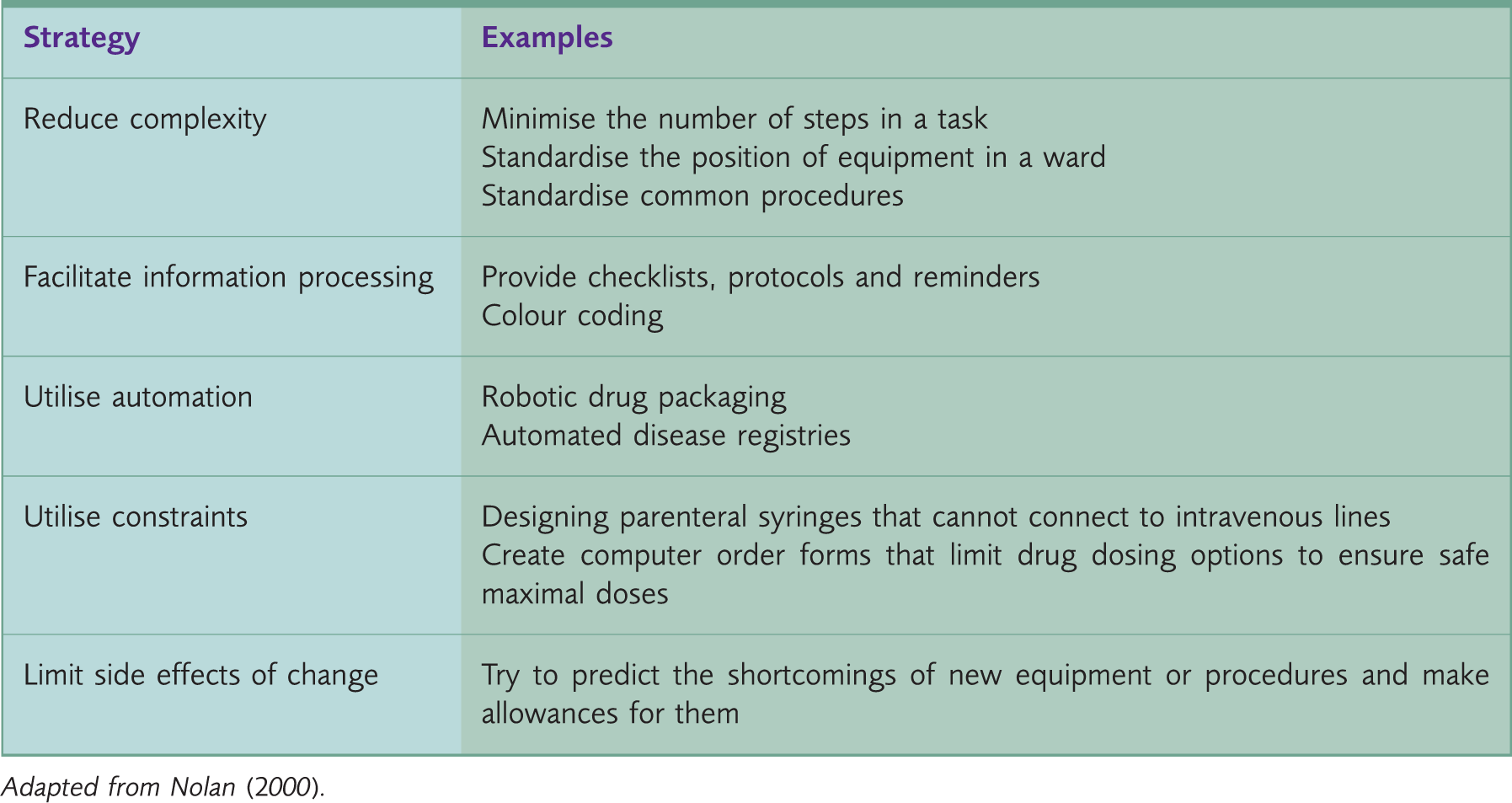
Adapted from Nolan (2000) .
Methods of reducing cognitive diagnostic error
The task of reducing cognitive error can be tackled in many ways. It needs to be multifactorial as the processes involved in patient care are complex (Leape, 2009). A discussion of some of the methods used to reduce cognitive errors follows.
Education
Learning about how to reduce medical error can begin at Medical School. Research has shown that knowledge transfer to the clinical environment is much easier if learning is case-based (Kuhn, 2002). Lectures, for example, are particularly effective when a case is introduced at the start of the lecture, providing food for thought and enabling students to see the relevance of the didactic content that follows. This is because transfer of knowledge is facilitated when the gap between theory and practice is as small as possible (Kuhn, 2002). Furthermore, it should be reinforced that not all of the clinical signs in a disease are seen in every case. Where possible the relative frequency of each sign should be illustrated, reinforcing the message that uncertainty is part of the diagnosis and acknowledging the need to develop strategies to manage this uncertainty (Kuhn, 2002).
It is becoming increasingly clear that diagnostic theory and strategy should be taught at undergraduate level, and that such programmes are effective when it is made realistic and is relevant to clinical situations (Wachter, 2010). Some medical schools have begun to teach students to consider the process of analysing data to reach a diagnosis and several now teach through a ‘problem-based learning’ approach. Problem-based learning is thought to augment clinical decision-making, and has been shown to improve diagnostic accuracy and clinical management plans in some studies (Graber et al., 2005).
Of course, professional education does not stop at graduation. Learning continues in the workplace, often through personal reflection upon previous experiences, which can be further enhanced through peer discussion and review of the sequence of events. Learning in the workplace can also occur in real-time as practitioners directly observe the effects of their actions and how this alters the course of the consultation. In addition, recognising future learning opportunities can augment acquisition of knowledge through planning and rehearsing for these scenarios. These mechanisms can provide the impetus to improve clinical acumen and therefore enhance diagnostic accuracy as the clinician matures (Eraut, 2000).
Feedback
One of the shortcomings of practising medicine within a healthcare organisation is that physicians may not always find out about the consequences of an error that they have committed. Feedback regarding errors has often been opportunistic, and may be unwelcome due to the potential for medico-legal consequences (Schiff, 2008).
Some institutions have developed information technology (IT) systems to notify physicians when a patient is readmitted within a short space of time, alerting them to changes in the clinical picture to allow a greater understanding of the dynamic course of disease. It has also been suggested that hospitals should be financially rewarded for diagnostic accuracy, encouraging such feedback to become more routine so that system-level improvements can be made (Leape, 2009; Wachter, 2010).
In primary care, significant event analysis and audit constitute an important part of the feedback process. This form of analysis provides structure to the process of reflection upon a critical incident, allowing for improvements to be made to the provision of care, including in transferable situations (Robinson, Stacy, Spencer, & Bhopal, 1995). It is important that the culture of these meetings is one of shared accountability rather than the apportioning of blame to an individual.
Furthermore, patients themselves are an invaluable source of feedback. They evaluate the effectiveness of healthcare delivery and can report back on their experiences. In this way, a patient’s unmet needs provide feedback to practitioners and influence the provision of safe and effective healthcare, helping to highlight future educational needs. Methods of gaining such feedback include patient satisfaction questionnaires, and these or more specific feedback can be expanded upon during discussions with mentors or peers (Wensing, Jung, Mainz, Olesen, & Grol, 1998).
Cognitive strategies
Metacognition is the reflective process in which one analyses one’s own thought processes i.e. thinking about what you think. The most common cognitive errors are anchoring and premature closure (see Table 1). Utilising conscious metacognitive reflection to remind oneself of this potential oversight can be a useful exercise. Step back, look at the data you have collected, and check that there are no other questions you could ask or any other diagnostic possibilities that could fit the data (Croskerry, 2003b; Wachter, 2010). Anchoring can be a powerful fault in cognition and can lead the physician to believe strongly that they are right about a diagnosis. This reinforces the need for feedback as discussed previously (Friedman et al., 2005).
Clinicians use subconscious rules of thumb in the diagnostic process that are often based on their previous experience of a cluster of symptoms. Although these are generally efficient, they can lead to overconfidence and a lack of consideration of other possible differentials. The extent of overconfidence is liable to increase with experience, so that a trainee is likely to have a greater awareness of diagnostic uncertainty than a more senior clinician. Reflective practice therefore enhances diagnostic accuracy in all clinicians regardless of experience, as the process reminds one of what the facts are - whether or not they fit with the diagnosis - and the potential consequences of a diagnostic error. Seeking second opinions and engaging in case discussions with colleagues are also useful in challenging assumptions and helping reveal unconscious blind spots and incomplete knowledge (Berner & Graber, 2008).
Information technology
One of the most effective methods of challenging cognitive errors is ‘forcing’. Forcing is used in a number of day-to-day practical situations, such as drawing money from a cash machine; money is only dispensed after the card is removed, thereby ‘forcing’ the individual to remember to collect their card. Forcing mechanisms are also found in everyday clinical practice, such as an automatic computer alert if a prescribing error has been made, and drug safety alerts from the National Patient Safety Agency which caution the prescriber about high-risk mediations such as methotrexate (Croskerry, 2003a). While these systems are well utilised in the prevention of medication errors, they are currently underutilised in the prevention of cognitive errors.
For example, hospital IT systems could be used to produce checklists, decreasing physicians’ reliance on memory by suggesting to them which tests might be appropriate. However, concerns have been raised that such systems may in fact disadvantage cognitive processing (and thereby lead to more errors) by promoting automated responses and inhibiting free flow of thought. Nonetheless, there is still much hope that IT systems can improve patient care by integrating data and improving the transfer of information between physicians (Wachter, 2010).
In addition, there are several commercially available diagnostic software products available on the market. These allow the user to list a variety of presenting symptoms, which the programme then matches to the most likely diagnosis. While these products provided much initial promise, they have fallen out of favour to an extent (Wachter, 2010). However, the concept that such systems are helpful is sound – there is so much new data being produced in medicine that it is impossible for clinicians to keep up. IT-based systems could be used to circumvent this problem if they were user friendly and accepted by physicians (Smith, 2010).
Points for practice
Strategies used to reduce cognitive diagnostic errors.
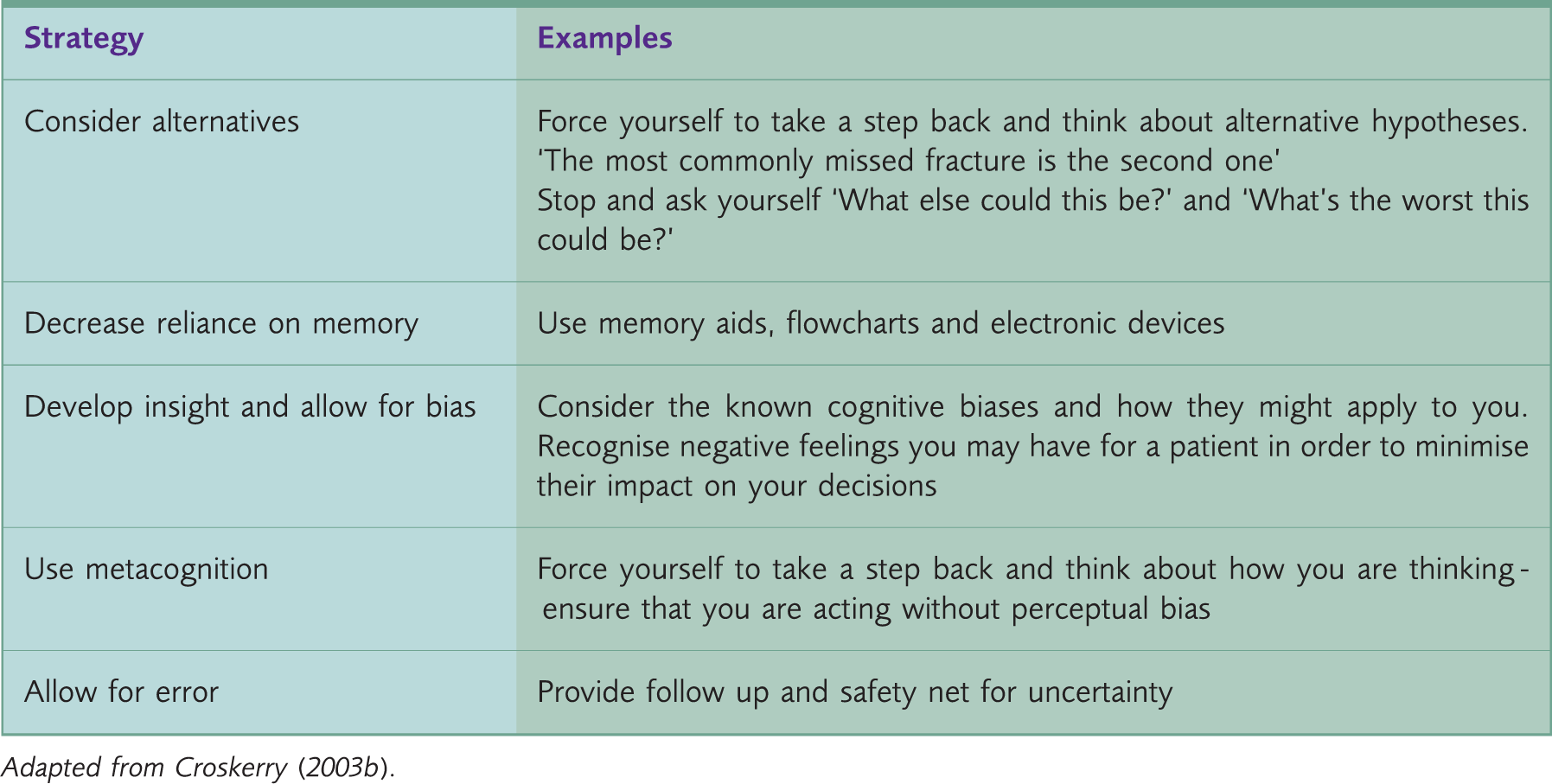
Adapted from Croskerry (2003b).
Conclusions
Reducing diagnostic error is both a collective and an individual responsibility. Healthcare organisations reduce medical errors by making system-wide improvements and monitoring trends in how errors and near misses are commonly made. Arguably, such system-wide improvements are so widespread that further improvements will follow the law of diminishing returns. Individuals now need to play their part in challenging their own thought processes in order to continue to improve patient safety and to drive healthcare forward. Many cognitive processes to reduce error are already ingrained in physicians, but others can still be learnt. Streamlining the accuracy of diagnostic thought processes can occur if the process of making a diagnosis and the diagnosis itself, are considered simultaneously.
Key points
Diagnostic errors are a significant cause of morbidity and mortality Efforts to reduce diagnostic error focus either on the health care organisation as a whole or on the cognitive processes of the individual practitioner Metacognitive processes can be used to reflect on the process of forming a diagnosis, thereby also reflecting on your own diagnostic skills and helping to improve your accuracy The commonest cognitive errors of diagnosis are premature closure (cutting the patient short) and anchoring (fixing the diagnosis too early) Important strategies to reduce cognitive error are to use memory aids (to allow increased focus on higher-order thinking) and to safety net