
Abstract
My CSA journey
I am a Nigerian-trained doctor who came to the UK 5 years ago. Coming from a background that is culturally different in the way that doctors and patients consult, I realised that I faced an extra challenge in meeting the requirements of the CSA. I discuss below how I worked with my trainer and fellow registrars to develop a patient-centred approach to consulting that allowed me to tackle the CSA confidently and successfully.
Preparation
Even during my induction phase, I focused on ways to develop my consultation skills. I was given the chance to observe experienced colleagues consult and picked up different ‘consultation gems’ that I felt I could use during my consultations. I practised using some of these key phrases and found that they helped me to develop communication tools that I could then adapt to different clinical scenarios. I soon realised that it was not good enough to simply repeat these phrases, but rather they had to flow naturally as I developed my own style.
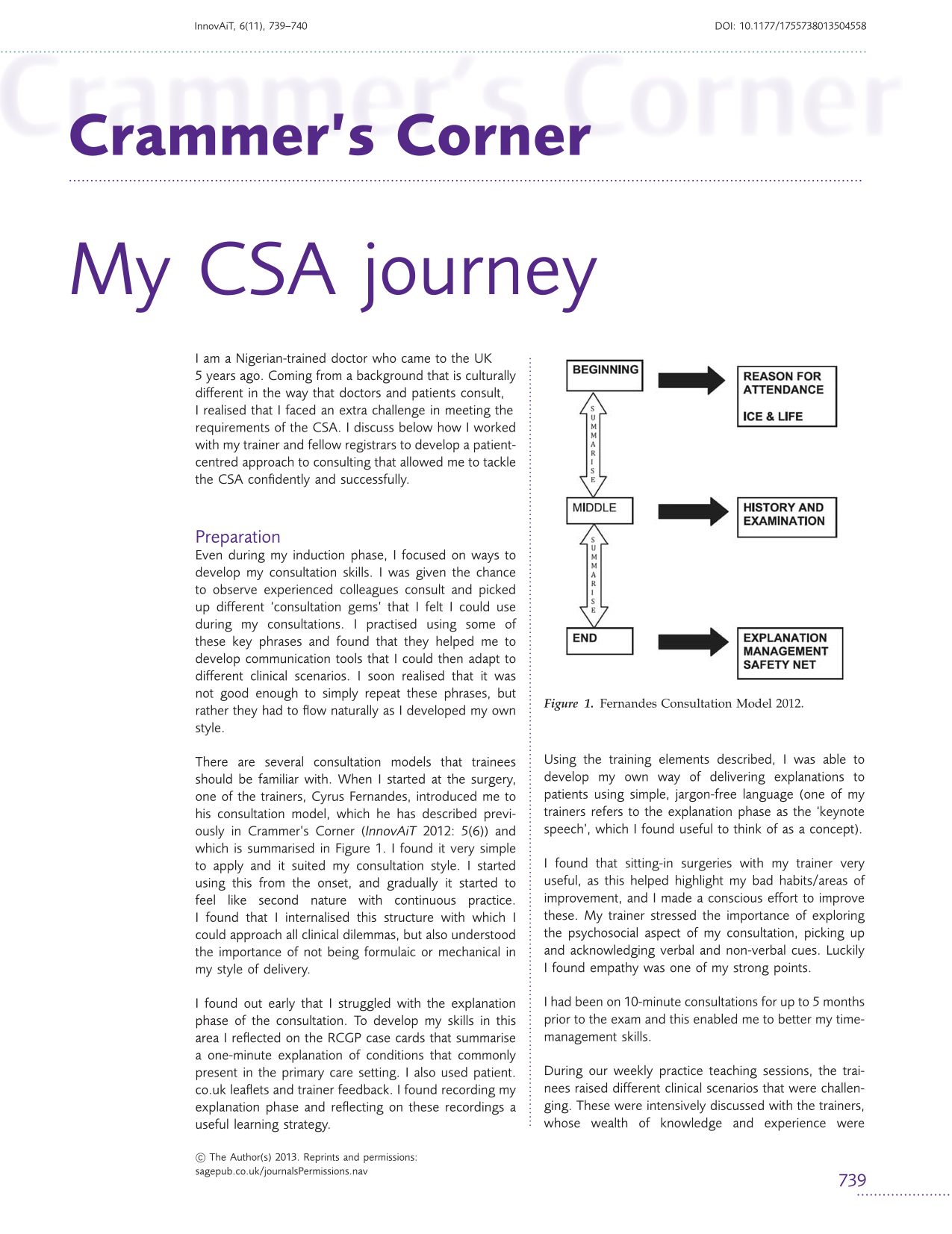
There are several consultation models that trainees should be familiar with. When I started at the surgery, one of the trainers, Cyrus Fernandes, introduced me to his consultation model, which he has described previously in Crammer’s Corner (InnovAiT 2012: 5(6)) and which is summarised in Figure 1. I found it very simple to apply and it suited my consultation style. I started using this from the onset, and gradually it started to feel like second nature with continuous practice. I found that I internalised this structure with which I could approach all clinical dilemmas, but also understood the importance of not being formulaic or mechanical in my style of delivery.
Fernandes Consultation Model 2012.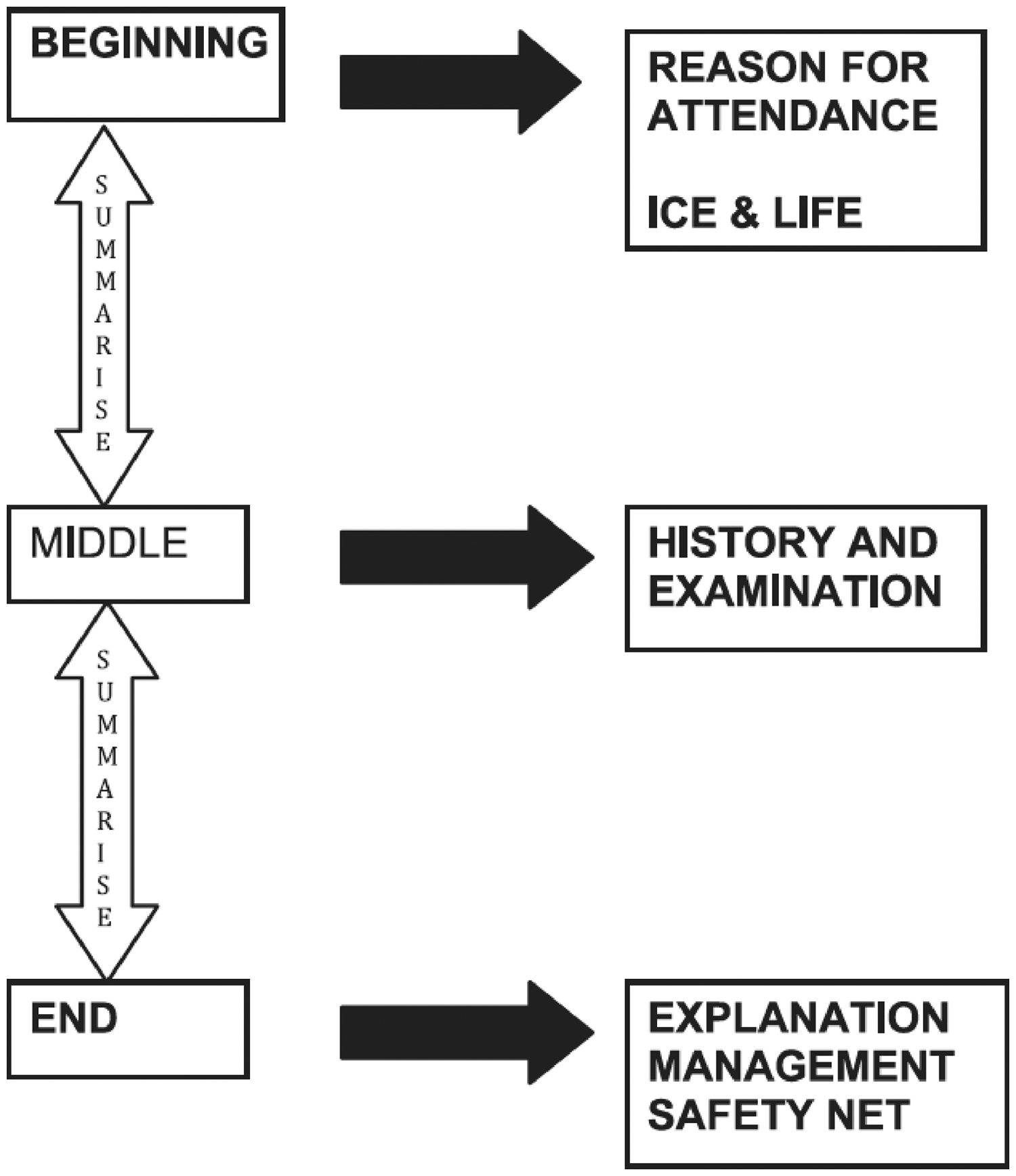
I found out early that I struggled with the explanation phase of the consultation. To develop my skills in this area I reflected on the RCGP case cards that summarise a one-minute explanation of conditions that commonly present in the primary care setting. I also used patient.co.uk leaflets and trainer feedback. I found recording my explanation phase and reflecting on these recordings a useful learning strategy.
Using the training elements described, I was able to develop my own way of delivering explanations to patients using simple, jargon-free language (one of my trainers refers to the explanation phase as the ‘keynote speech’, which I found useful to think of as a concept).
I found that sitting-in surgeries with my trainer very useful, as this helped highlight my bad habits/areas of improvement, and I made a conscious effort to improve these. My trainer stressed the importance of exploring the psychosocial aspect of my consultation, picking up and acknowledging verbal and non-verbal cues. Luckily I found empathy was one of my strong points.
I had been on 10-minute consultations for up to 5 months prior to the exam and this enabled me to better my time-management skills.
During our weekly practice teaching sessions, the trainees raised different clinical scenarios that were challenging. These were intensively discussed with the trainers, whose wealth of knowledge and experience were invaluable. I could then use these discussions to improve my management of patients in the consultation.
I formed a discussion group with some of my fellow trainees, and we met up twice a week on average and practiced and shared ideas together. As I did not go for any CSA course, I got the feel from my colleagues who had attended, and in hindsight I would have attended one to familiarise myself with what was to be expected, and reduce nerves on the day.
Conclusion
In a nutshell, CSA preparation should be a continual process and internalising a consultation model is an essential part of developing effective consulting. A lot of focus should be placed on one’s interpersonal skills as this can be an area of particular challenge for doctors that have trained and worked abroad and so have to adapt to the cultural expectations of patients in UK general practice. Finding out one’s areas of weaknesses early on and working on them is also important.
There is no shortcut to success, but the key to passing the CSA lies in the ability of a doctor to integrate all the knowledge and skills developed over time throughout the training. Giving that it is a timed exam, as much as one may want to be thorough, being structured yet adopting flexibility in approach, enables one cover the important aspects of each case. Good consultation skills make you an efficient as well as an effective GP!