
Abstract
Squint is a common childhood condition that, if not picked up early, can have a detrimental effect on a child’s visual development and later quality of life. In the majority of cases the exact cause remains unknown, although it may be the presenting symptom of a serious ocular or neurological disease. GPs need to appreciate the range of causes of squint, its potential consequences, and hence know when and how urgently a specialist referral is required.
The GP curriculum and squint
Manage primary contact with all patients who have an eye problem Understand the common eye problems in primary care and manage them appropriately Make timely, appropriate referrals on behalf of patients to specialist and community eye services Appreciate the importance of the social and psychological impact of eye problems on the patient Recognise ophthalmic emergencies and refer appropriately Recognise ocular manifestations of neurological disease Develop their understanding of how one might organise screening for eye problems in their practice, e.g. squint Be aware of major advances in therapy for eye conditions
Squint, also known as strabismus, is a misalignment of the eyes when focusing on an object, such that both eyes are not simultaneously directed at that object. This results in an image not being formed on the fovea of the strabismic/squinting eye. Before the age of 6 weeks the co-ordination of eye movements is poor. The eyes of normal infants may therefore be misaligned, making it difficult to diagnose squint before 6 weeks of age. However, by 3 to 4 months of age alignment is stable, making it possible to accurately diagnose abnormalities if the infant is cooperative and alert.
Squint is a common condition in childhood, with a prevalence of 2.1% by 3 years of age (Pathai, Cumberland, & Rahi, 2010). It can, rarely, be due to serious underlying disease, requiring urgent referral to secondary care for further management. However, even common squint is problematic. It is the most common cause of amblyopia (lazy eye), in which decreased visual acuity occurs due to abnormal visual development in infancy or early childhood. It can also result in failure to develop binocular vision (the ability to simultaneously perceive images from both eyes). This in turn impairs the ability to develop stereopsis - the ability to perceive images from both eyes to produce a single image with depth perception.
Because of these effects, a failure to correct squint can have detrimental effects on a patient’s physical, social and psychological well-being. From a psychological point of view, having a squint may have a negative impact on an individual’s portrayal of him- or herself and can hinder the development of a positive self-image (Satterfield, Keltner, & Morrison, 1993). People with a squint have been shown to have reduced employment opportunities (Coats, Paysee, Towler, & Dipboye, 2000) and to experience problems with social interactions (Mojon-Azzi, Kunz, & Mojon, 2011). Early recognition and subsequent treatment of squint is advocated to avoid the lifelong problems with sight, psychological well-being, relationships and job opportunities.
Classification
Squint can be broadly classified into two main categories: non-paralytic and paralytic. In the former a full range of motion is possible in both eyes, but only one eye is directed towards the fixated target. In the latter one or more of the eye muscles is underactive due to either a nerve palsy, extra-ocular muscle disease or tethering of the globe.
Non-paralytic squint
Esotropia is a convergent misalignment of the visual axes (see Fig. 1). The condition is associated with prematurity, maternal smoking during pregnancy, anisometropia (eyes are of unequal refractive power) and hyperopia (long-sightedness).
Esotropia.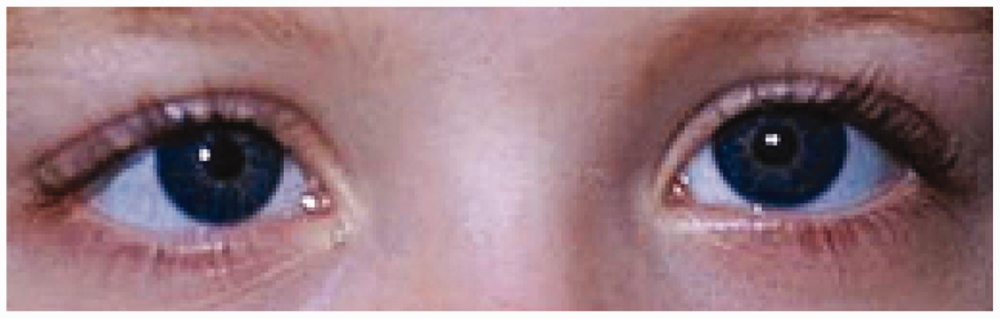
Infantile esotropia presents before the age of 6 months. It is common during the first 3 months of life and, if intermittent, does not always persist to become a permanent squint.
Acquired esotropia develops in infants after the age of 6 months. It is more common than infantile esotropia and usually presents between the ages of 1 and 8 years with most patients presenting by 2–3 years of age. Acquired esotropia caused by excessive convergence in a patient who is long-sighted (hyperopia) may be eliminated by correction with spectacles.
Exotropia is a divergent misalignment of the visual axis (see Fig. 2). The non-paralytic variety has a prevalence of 1% in the population, and has been associated with prematurity, perinatal morbidity, genetic disorders, family history of squint, female sex, astigmatism and detrimental prenatal environmental influences such as maternal substance abuse and smoking (American Academy of Ophthalmology Pediatric Ophthalmology/Strabismus Panel, 2012). As is the case for esotropia, it can be divided into infantile and acquired categories, depending on the age of presentation. Acquired exotropias are mainly of the intermittent type and the deviation becomes manifest at times of fatigue, visual inattention or illness.
Exotropia.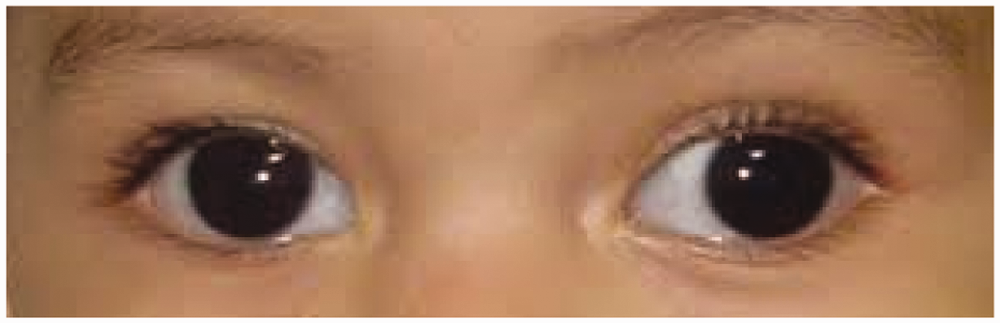
Paralytic squint
Paralytic squints occur when there is impaired motion of one or more of the extra-ocular muscles. This can cause esotropia, exotropia and vertical deviation, depending on the muscle or muscles that are involved. In all cases and characteristically, the angle of the squint is affected by the direction of gaze, which will be greatest in the field of action of the affected muscle. This type of squint is termed an incomitant squint. This is opposed to non-paralytic squints, which are comitant, and hence the size of the angle of deviation does not change with the direction of gaze.
Paralytic squints are normally acquired, and hence, more common, in adulthood than in childhood. They tend to give rise to symptoms of diplopia, as well as a compensatory head tilt to counteract the inability to move the eye in a particular direction.
Childhood squint
Presentation in primary care
GPs should be able to detect a squint, as well as pick-up features that suggest a more sinister cause and therefore require urgent referral. An otherwise healthy child with a squint might not always complain of symptoms and usually only presents to the GP if parents or carers notice the abnormality, or note that their child has an asymmetric or absent red reflex in photographs.
Begin your assessment by taking a thorough history. Questions to consider when screening a child with a squint include asking about the onset of eye deviation and whether this was present in early infancy. Ask whether the squint is constant or intermittent and whether evoked by certain positions of gaze only. It is also important to exclude any associated symptoms of headache or double vision. Any family history of squint or amblyopia is relevant, as well as any history of head injury, or prenatal maternal history of severe infection or medication and toxin exposure.
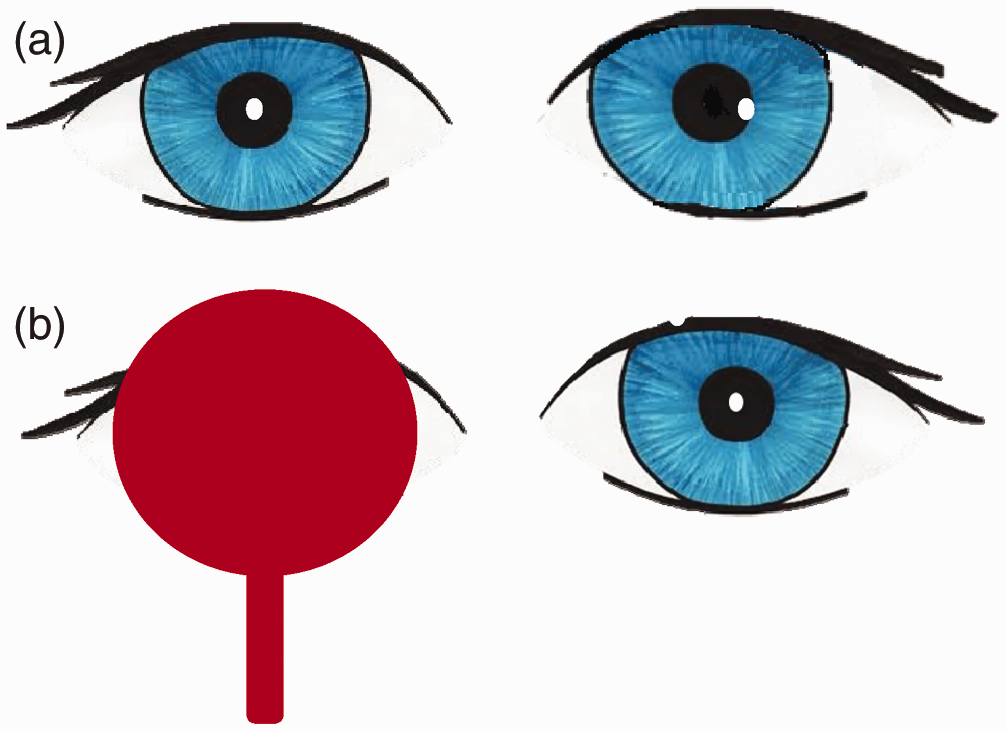
The patient should then be examined, beginning with a general examination to check for any extra-ocular neurological symptoms and signs. When examining the eyes, perform a gross anatomical inspection looking for any nerve palsies, afferent pupillary defects and abnormal red reflexes. The latter is assessed using the Bruckner method, which involves shining the light of an ophthalmoscope from approximately a 30 cm distance onto the pupil; if positive a red reflection of light is seen bouncing off the retina. It is used to screen for posterior segment eye abnormalities or visual axis opacities. Dark spots in the red reflex, a blunted or absent red reflex or the presence of a white reflex (retinal reflection) are all indications for referral to an ophthalmologist. The corneal light reflex should be assessed using the Hirschberg method that is explained in Fig. 3. Finally, the child should undergo cover testing, which is explained in Fig. 4.
Assessing for light reflex. Hirschberg method of assessing for light reflex: this involves asking the child to fixate on a pen torch held at a distance and assessing the reflection of the light on the cornea in relation to the pupil. (a): Normal corneal light reflex. (b): Corneal light reflex in exotropia. (c): Corneal light reflex in esotropia. Cover test to detect squint. In the cover test, the patient is asked to fixate on an object at a particular distance. One eye is first covered and the other eye is observed for any movement. If there is temporal movement of the uncovered eye (as shown in B) then there is an esotropia. If there is nasal movement then there is an exotropia.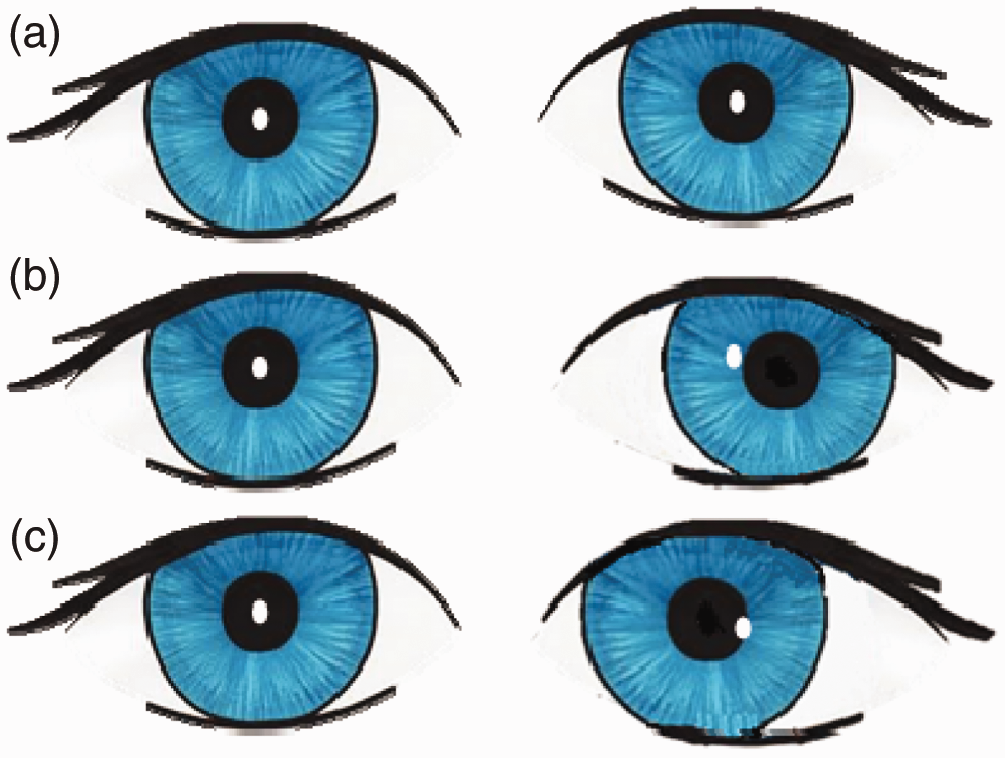
Referral of children with non-paralytic squint
GPs have the responsibility of deciding which children with squint need referral. When making this decision in young children it helps to remember that in humans the visual system is not fully developed at birth. Before the age of 6 weeks co-ordination of eye movements is poor, and intermittent neonatal ocular misalignments are a common finding. By 2–3 months infants should be capable of following objects in the horizontal and vertical planes while maintaining binocular visual alignment. Therefore, GPs can reassure parents that the child will start to grow out of these misalignments by 2 months of age and any apparent squint should have resolved completely by 4 months. Any misalignment that begins to worsen by 2 months of age or is still present after 4 months requires referral.
Childhood squint is associated with a number of prenatal and perinatal factors, including:
Low birth weight (less than 1250 g), especially if associated with retinopathy of prematurity or hydrocephalus Congenital ocular abnormality Tumours of the eye or brain Perinatal head injury, such as subdural, subarachnoid or intra-ventricular haemorrhage due to birth trauma Congenital infections (e.g. rubella, and cytomegalovirus) and neonatal infective mastitis Prenatal exposure to drugs and toxins, including alcohol, narcotics, and recreational drugs such as cocaine and heroin
The prevalence is also increased in families with a positive family history and in children with neuro-developmental disorders such as Down’s syndrome and cerebral palsy. Many children in these groups will already have been referred for specialist screening, but as squint is more prevalent in these populations GPs should refer those who have not already had specialist screening to an ophthalmologist for an assessment to exclude squint.
In addition to this, the American Preferred Practice Guidelines on Esotropia and Exotropia (American Academy of Ophthalmology Pediatric Ophthalmology/Strabismus Panel, 2012) recommend the following indications for referral:
Constant esotropia at any age Intermittent esodeviations that persist at 4 months of age Positive light reflex or cover test that reveals deviation Asymmetry of appearance on red reflex testing Incomitant deviations Parental concern about ocular alignment
Alarm features that should prompt urgent referral.

Treatment of squint in children
With early detection the prognosis of squint is excellent, thus it is extremely important to know when to refer a child to an ophthalmologist. If squint is accurately diagnosed and correctly treated before the age of 6 years the outlook is positive. Unfortunately, once a child reaches the threshold of 8 to 10 years, treatment of squint has been found to be poor and permanent visual problems can result. Squint is treated with a multidisciplinary approach.
The first step in the management of many cases of squint involves correcting any refractive error with prescription glasses. Children’s glasses should always be made of plastic, if possible, to reduce the risk of injury. Following refractive correction it is customary to allow for refractive adaption to occur, as visual acuity can improve with glasses alone.
When there is both strabismus and amblyopia, treatment must also involve stimulating the amblyopic eye by using occlusion therapy. This involves using an adhesive patch to cover the ‘good’ eye, thereby encouraging the development of the visual pathway of the weaker or ‘bad’ eye. This is carried out for a period of time each day. It is especially indicated if the visual pathway of the bad eye has been retarded by a squint or refractory error. However, this can only be done for a limited period. Most ophthalmologists feel that after the age of 7 years occlusion therapy is unlikely to be helpful. In the meantime, the underlying problem must be corrected.
Orthoptics (vision therapy) entails the use of active exercises with the aim of improving fixation ability, oculomotor control, and sensory and motor fusion. Vision therapy is successful in the treatment of many forms of strabismus.
Surgery should only be considered once the conservative techniques have been tried and, following best correction, the angle of strabismic deviation remains too large for binocular comfort and is not cosmetically acceptable. With regards to infantile esotropia, surgical alignment improves the odds of a child developing normal visual function, especially when carried out at an earlier age - although the ideal age for surgery still remains controversial (Simonsz, Kolling, & Unnebrink, 2005). There are essentially three options available to the surgeon to effect the action of the extra-ocular muscles. These are: weakening, strengthening or transposition procedures. Weakening procedures are achieved either by a recession, where the surgeon dis-inserts a muscle or tendon from the globe and reattaches it posterior to its original insertion; or via a Z tenotomy, where the surgeon lengthens the muscle or tendon via two incisions partially across the tendon or muscle. Strengthening procedures involve shortening of the muscle via resection or making a pleat or fold in the muscle, thereby shortening the muscle and hence strengthening it. Lastly, the technique of transposition involves reinserting the insertion of the muscle to a new position on the globe and hence altering its field of action.
An alternative to conventional surgery is the use of botulinum toxin type A. This chemical agent works by inhibiting the transmission of a nerve impulse at the neuro-muscular junction, therefore paralysing the muscle. This results in a compensatory contracture of the antagonistic muscle with the desired consequence of better visual alignment. This method of treatment has so far only been successful in the treatment of certain groups of squint patients such as children who have already undergone surgery for acquired esotropia and require a secondary procedure (Tejedor & Rodriguez, 1998).
Squint in adults
Causes of cranial nerve palsy.
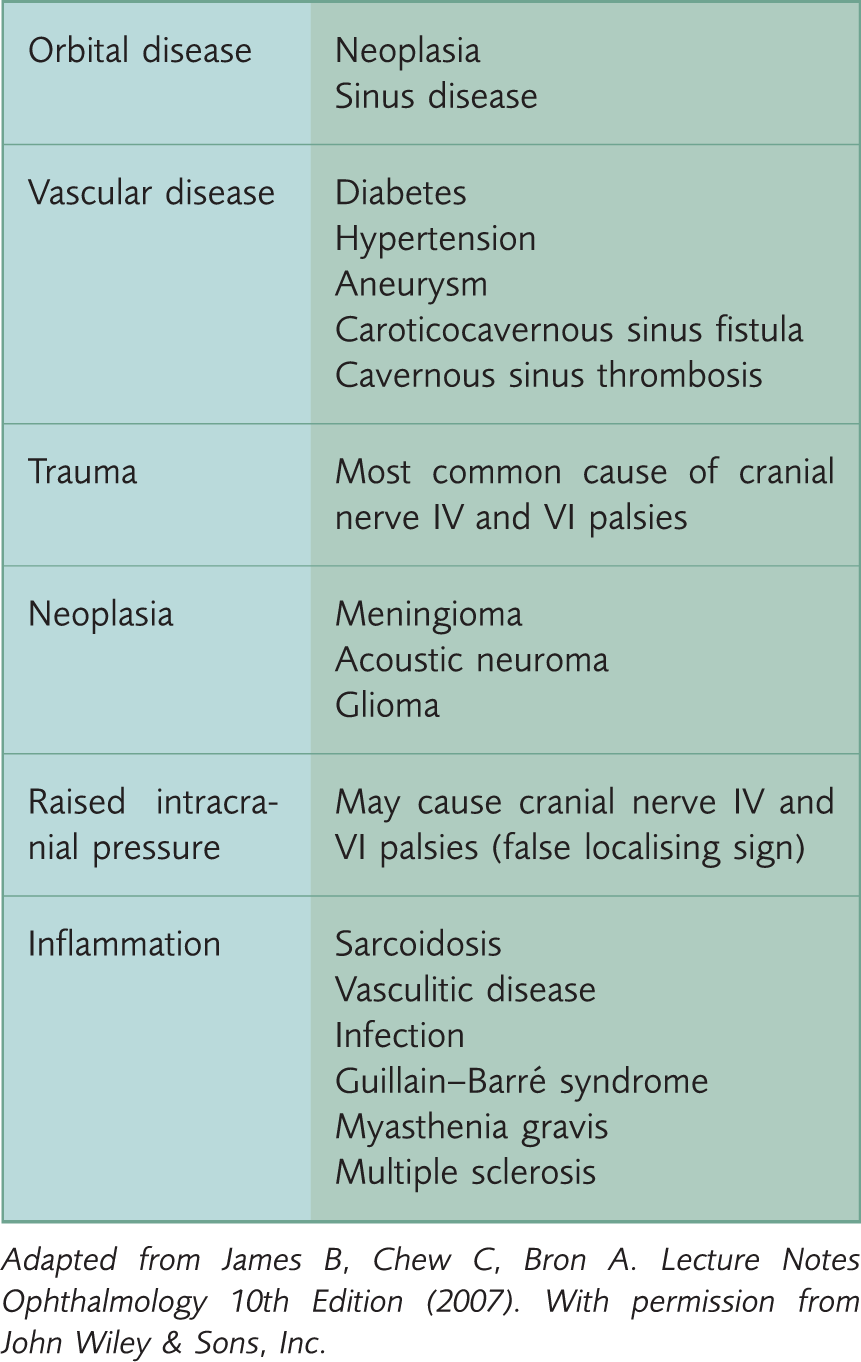
Adapted from James B, Chew C, Bron A. Lecture Notes Ophthalmology 10th Edition (2007). With permission from John Wiley & Sons, Inc.
Paralytic squints can also be due to restrictive causes, muscular diseases, or as a consequence of impaired extra-ocular muscular movement due to physical obstruction in the context of a ‘blow out’ fracture of the orbit. The neuromuscular conditions that typically cause a paralytic squint are multiple sclerosis, myasthenia gravis and botulism. Restrictive strabismus may also be observed in thyroid eye disease, where an inflammatory infiltration of the extra-ocular muscles results in swelling and impaired movement.
Squint in adulthood could also be the result of untreated childhood squint, or a recurrence of the former. This presentation is not normally accompanied by diplopia, as the image from the squinting eye will be suppressed.
GPs managing an adult who presents with a squint should check the patient’s personal ocular history, specifically whether this is a new or old occurrence. If the history points to a recent onset, it is important to consider the possibility of intracranial pathology, such as a tumour or cerebrovascular accident. A relevant history and examination should be performed, including a careful assessment of the cranial nerves, and an urgent referral to secondary care made if a neurological insult is suspected. However, if the ‘new’ squint does not exhibit any worrying features of this kind then the patient can be referred to an optometrist for sight testing and assessment of the squint. If the optometrist is unable to effectively manage the patient he or she will refer the patient back to the GP for an onward referral to the hospital ophthalmic specialist. The mainstay of hospital treatment in this situation is surgical correction of the squint; it is important that the patient is aware of this and would be willing to undergo surgery.
Many patients are under the misconception that no treatment is available for adults with strabismus, that surgical correction is not effective in improving binocular function and, if done, is simply for cosmetic reasons. Moreover, it seems that a number of optometrists, GPs and even ophthalmologists are equally misinformed (Kushner, 2001). This can lead to delay in obtaining potentially beneficial treatment. Strabismus not only impacts on a patient’s functional status but also affects his or her psychological state of mind and social interactions. In fact, in one study, 60% of adult patients with strabismus were willing to trade part of their life expectancy in exchange for getting rid of the condition and its associated effects (Beauchamp, Felius, Stager, & Beauchamp, 2005).
A recent American Academy of Ophthalmologists report states that surgery is safe and effective in improving ocular alignment for adults with strabismus. It also states that in many cases visual function is also improved. This is a result of elimination of diplopia, expansion of visual fields and, in certain cases, development of binocular fusion (Mills, Coats, Donahue, & Wheeler, 2004).
Conclusions
The importance of detecting and managing squint at an early stage cannot be underestimated. It is especially important in children, who generally will not complain of symptoms. If squint is not picked up and corrected in a child this may result in irreversible defective visual development in the impaired eye. This will also have lifelong consequences on the child’s psychological and social quality of life. Finally, squint may be the presenting feature of a more serious underlying pathology, both in children and in adults. Any healthcare professional involved in the management of squint should always be on the look out for any associated features that suggest an underlying sinister pathology.
Key points
Squint is a common childhood condition that, if not corrected, can result in irreversible damage to a child’s visual system Having a squint has a negative impact on one’s psychological and social well-being and functioning In many cases the management of squint simply involves correcting refractive error with glasses GPs should be able to perform a basic ocular examination, including testing for the red reflex, corneal light reflex and cover testing in order to detect squint Squint may be the presenting feature of serious underlying pathology and, if alarm features are present, an urgent referral is essential
Footnotes
Acknowledgement
We would like to thank Dr Lara Batchat for her help with the writing of this article under the InnovAiT ‘buddy’ scheme.