
Abstract
Headaches are common in children; however, assessment can be a challenge in this age group. The description of an attack may not be clear, attacks may be infrequent and so a pattern of attacks may be difficult to ascertain, examination can be difficult, especially in a very young or uncooperative child, and presentation is often accompanied by significant parental anxiety. This article aims to provide a strategy for GPs to differentiate primary from secondary headaches and common primary headache types such as migraine and tension-type headache. It also outlines the primary care management of these conditions.
The GP curriculum and headaches in children
Be able to demonstrate how you manage primary contact with patients who have neurological symptoms, including headache, dizziness or tremor Know the epidemiology of common and important neurological conditions such as epilepsy, headache, causes of vertigo, multiple sclerosis and/or important inherited conditions Know the indications for referral for conditions that require ongoing specialist management and those that require early treatment
Appropriately treat common but important paediatric conditions encountered in primary care Be aware of the early presenting symptoms of childhood cancers
Epidemiology
The epidemiological data on childhood headaches is mostly focused on migraines and tension-type headaches. European studies have shown that the prevalence of migraine increases from childhood to adolescence and varies from 3% in the preschool population to 8–23% during the later school years (Abu-Arafeh and Russell, 1994; Sillanpaa and Anttila, 1996). Tension-type headache is the most frequent headache in children, with a prevalence range between 0.9 and 73% that increases with age.
Assessment of children with a headache
This article only intends to cover the assessment of children with a history of ongoing headaches, it does not attempt to cover the assessment of children acutely unwell with a headache. Taking a headache history, identifying triggers, uncovering red flags and carrying out a focused examination are essential.
Medical history
The clinical history is an important foundation in forming a diagnosis and differentiating primary from secondary headaches. First, it is helpful to explain to the parents and child the process of the assessment. History should be appropriate to the development of the child and leading questions should be avoided. It is also useful if the parents and patient keep a record of a typical headache attack. If needed, GPs may organise a second visit or a brief telephone discussion as a follow-up to ensure they have a complete history.
Diagnosis of a headache in the under-fours relies upon clinical judgement. Some children may not be able to remember the entire headache attack and might find it difficult to provide a precise headache description. Some symptoms such as photophobia and phonophobia can be difficult to retrieve from a child. Therefore, professionals need to make allowances for lack of detail in the history, and also potential bias in the parents’ account.
In children, a lot of information can be gained by asking about the behaviour of the child during headache attacks. For example, the impact of the headache on daily activities, improvement after having a good sleep, avoidance of bright light, looking pale and feeling unwell, crying because of pain and putting hands on head or pointing.
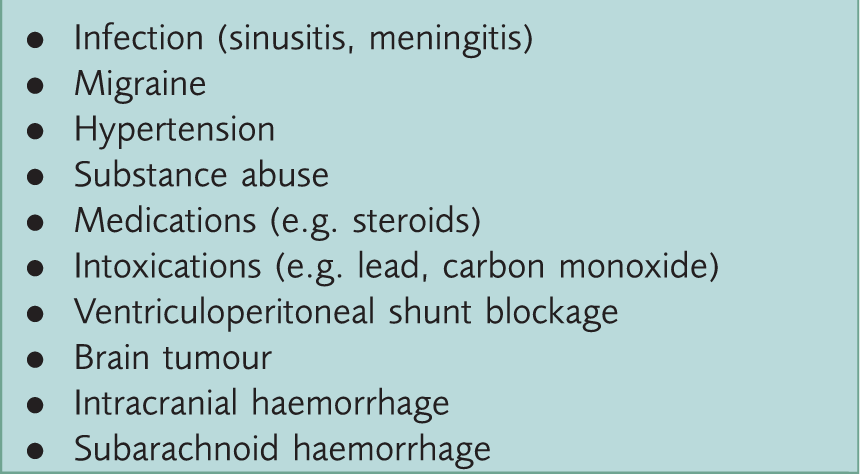
Main causes of acute headaches.
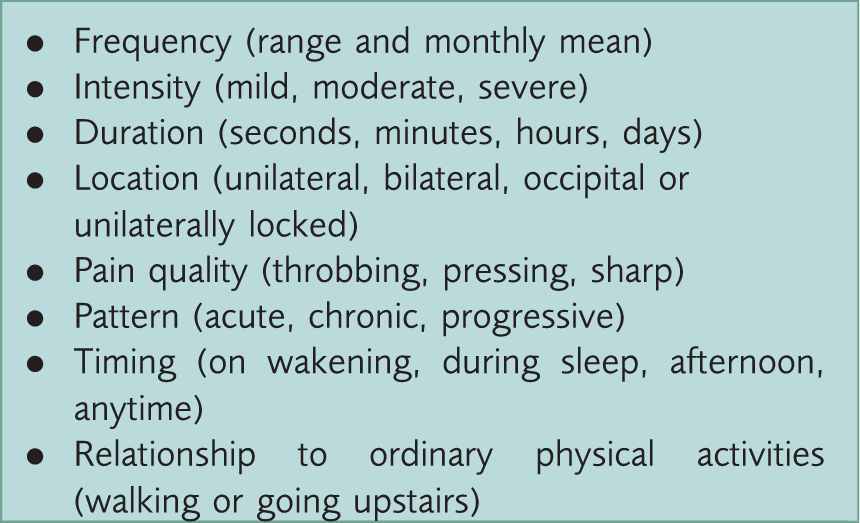
Headache characteristics.
A systemic history is as valuable as the headache history. GPs should ask specifically about evidence for increased intracranial pressure, including nocturnal vomiting, headache on wakening or headaches causing sleep interruption. A family history of headache and a history of systemic illness may also be relevant.
Specifically ask about use of medications (pain killers), as excessive use can lead to medication-overuse headache; this is mainly an issue among teenagers. Using paracetamol or ibuprofen for 15 days or more per month, for more than 3 months, should alert GPs to the likelihood of medication-overuse headaches.
It is usually helpful to briefly explore the patient’s lifestyle, with an emphasis on sleep habits, caffeine, and fizzy drink intake, street-drug use, and excessive use of computer games or television viewing. Another aspect is the impact of the headaches on quality of life, such as relationships, school performance and achievements.
Carbon monoxide poisoning is not uncommon, and should always be considered among patients with headaches. Ask about gastrointestinal symptoms, tiredness, and family history of similar complaints, improvement of headaches when the child is away from home and headache worsening during winter time. Other clues include a yellow or orange flame instead of a blue flame from the cooker or gas boiler.
The presence of allergy and use of decongestants may suggest sinusitis headaches. This condition should be considered among patients with severe headaches together with purulent nasal secretions.
General medical history should include recent head injury, as headache after brain injury is common. Child protection issues, mainly in the form of emotional abuse, have also been identified as a risk factor for chronic headaches in children.
Parental worries are critical to the assessment of the child. When parents have a lot of anxiety it can be challenging, especially when they perceive their child’s headache to be due to a serious underlying cause such as a brain tumour. Parents with a positive family history of brain tumours may present as a particular challenge for decision-making. For GPs, it is important to achieve a balance between the care plan for the child with headaches and the needs of concerned parents reaching out for help.
Red flags
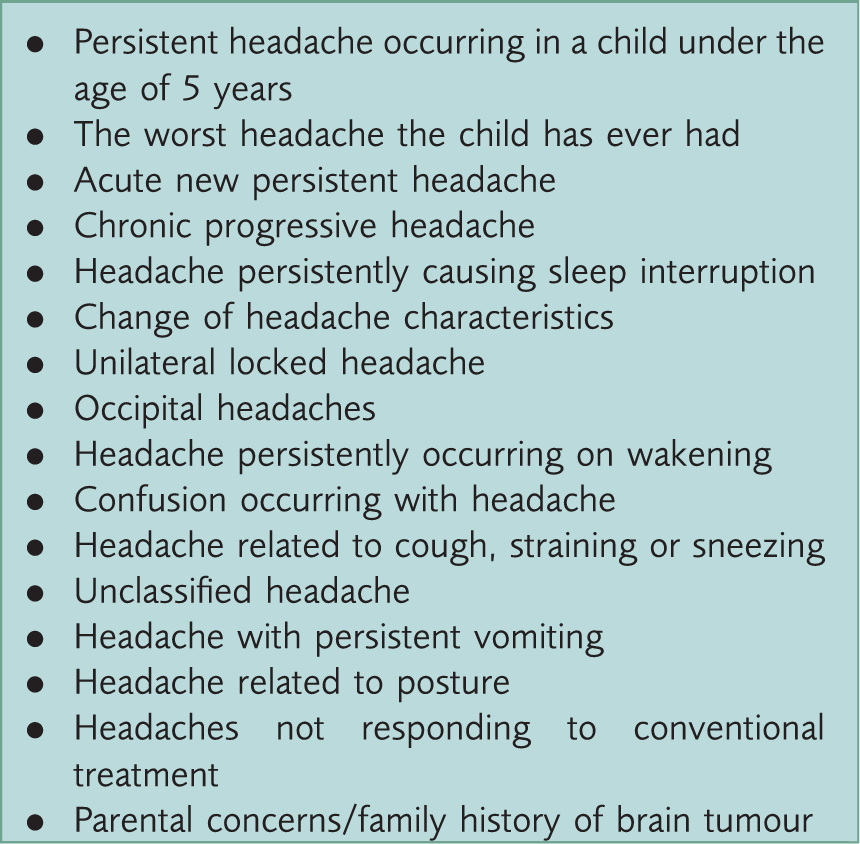
Red flags among neurologically normal children with headaches.
In assessing for red flags, determining the headache pattern is usually helpful. Chronic progressive headache or acute severe headaches are both important red flags. Characteristics that are particularly worrying include headaches that occur immediately after transferring from a recumbent position to a sitting or standing posture, which may be secondary to underlying intracranial lesions.
Patients presenting with occipital headaches require further assessment to rule out a vascular brain lesion or space-occupying lesion. Equally, patients with a change in headache characteristics (e.g. increased frequency), might have an underlying threatening aetiology.
Examination
Relevant parts of the examination.
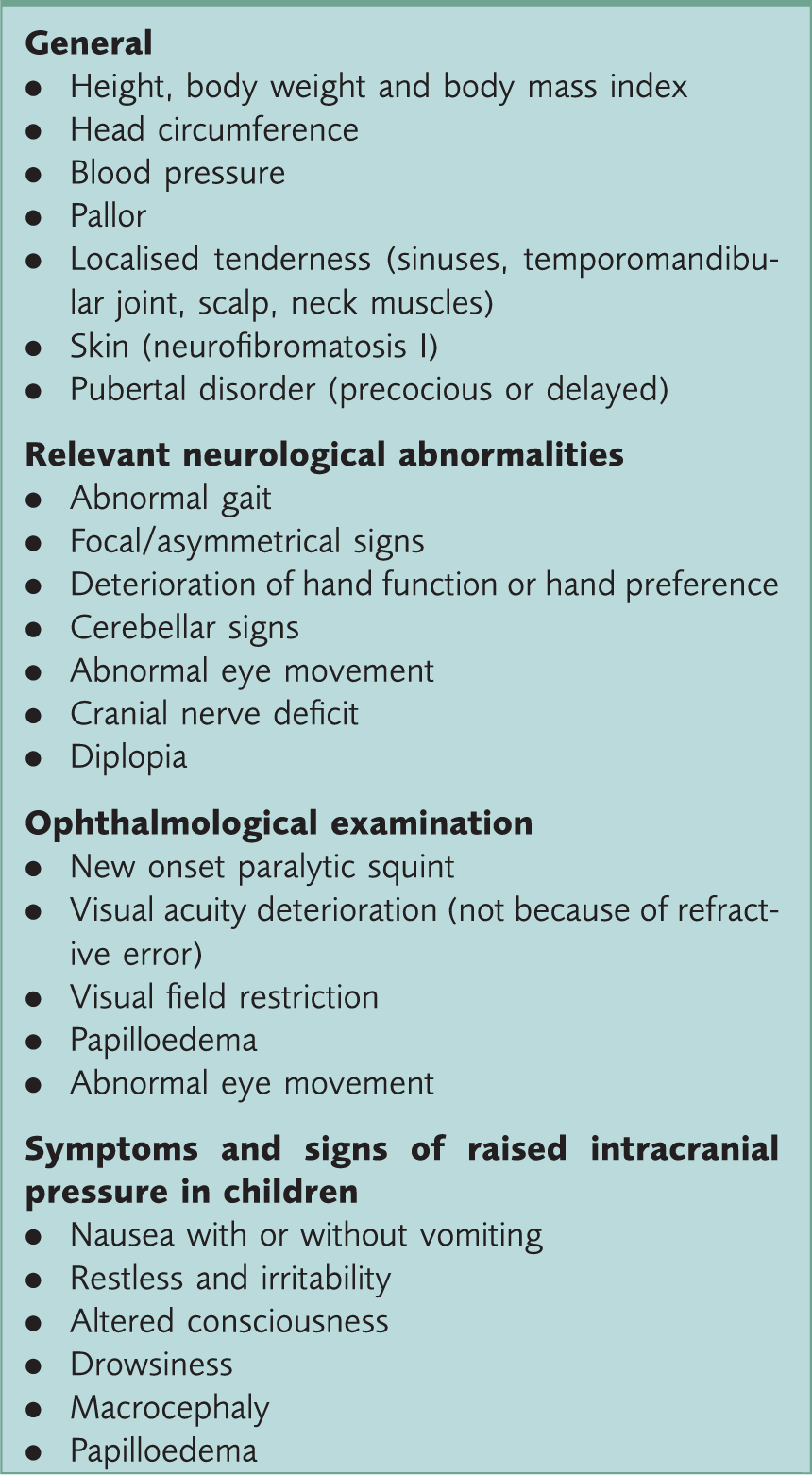
Measurement of blood pressure and looking for pallor are important parts of the general examination; anaemia and hypertension are well recognised causes to consider among patients with unspecified headache. In addition, skull auscultation (orbital and temporal areas) looking for cranial bruit might reveal intracranial arterio-venous malformation. Inspection of the skin looking for neuro-cutaneous markers is helpful as children with neurofibromatosis are at higher risk of a brain tumour. Examination must include pubertal staging and measurement of height and body weight, an unexplained short stature or weight loss may indicate an intracranial pathology. Comparison of the child’s height and weight with earlier measurement can be useful.
Investigations
The majority of children presenting to general practice with headaches require no investigations. However, abnormal neurological and/or ophthalmological examination constitutes an absolute indication for brain imaging. Brain imaging is also indicated in children with progressive chronic headaches and those with suspected secondary headaches and should be considered for healthy children with unclassified headaches and red flags (Ahmed, Martinez, Cahill, Chong, & Whitehouse, 2010).
Other investigations should be arranged on an individual basis. For example, a full blood count might be helpful for children with headaches and pallor. If indicated, diagnosis of carbon monoxide poisoning can be made by a venous blood sample for carbon monoxide haemoglobin assay.
What do GPs need to know?
Understanding commonly used terminologies, headache types and red flags is essential in the assessment of childhood headaches. It is also important to be able to distinguish between primary and secondary headaches.
Terminology
Particular terms to describe headache characteristics include frequency, duration, location and intensity. Frequency refers to the number of headache attacks per time period (usually measured in months). Headaches occurring less than once a month, or fewer than 12 attacks per year, are termed ‘infrequent’, whereas ‘frequent’ headaches imply a frequency ranging from one to 14 attacks per a month. Chronic daily headache’ requires the patient to have at least 15 headache days per a month for a period of 3 months or more.
Duration of attacks is calculated from the time of onset until full termination of an attack. If the patient falls asleep during an attack and wakes up with no headache the duration is until the time of awakening.
Unilateral headache refers to pain on either the right or left side of the head not crossing the midline. It can be temporal, frontal or occipital. Unilateral ‘locked’ headache implies headaches that are fixed and always occur at one specific site of the head.
The intensity usually refers to the scale of pain in terms of its functional consequences. Patients with mild headaches usually run normal daily life activities, whereas moderate and severe headaches inhibit and prohibit daily activity, respectively.
Migraine aura is a transient focal sensation, developing over a period of 5–15 minutes and spontaneously completely resolves within an hour. It is usually divided into visual, sensory, language and motor auras. Visual aura is the most common type. The child might find it difficult to read or write during the period of visual aura, however, normal vision should return within an hour from the time of onset. Patients may experience a blurred or absent area in the visual field or even complete blindness. Others may notice flashing lights or may see various visual patterns. Patients commonly first perceive a little flickering light in the central visual field. This tends to move to the peripheral field of vision where it becomes more noticeable and then might be followed by zigzag lines. This is often called a ‘fortification spectrum’ because the jagged edges of the visual hallucination look like a fortified town with bastions around it. Sensory aura is the second most common type of aura and presents with pins and needles or numbness that begins in the hand, moves up the arm and usually skips the shoulder and moves into the face and tongue.
Headache types
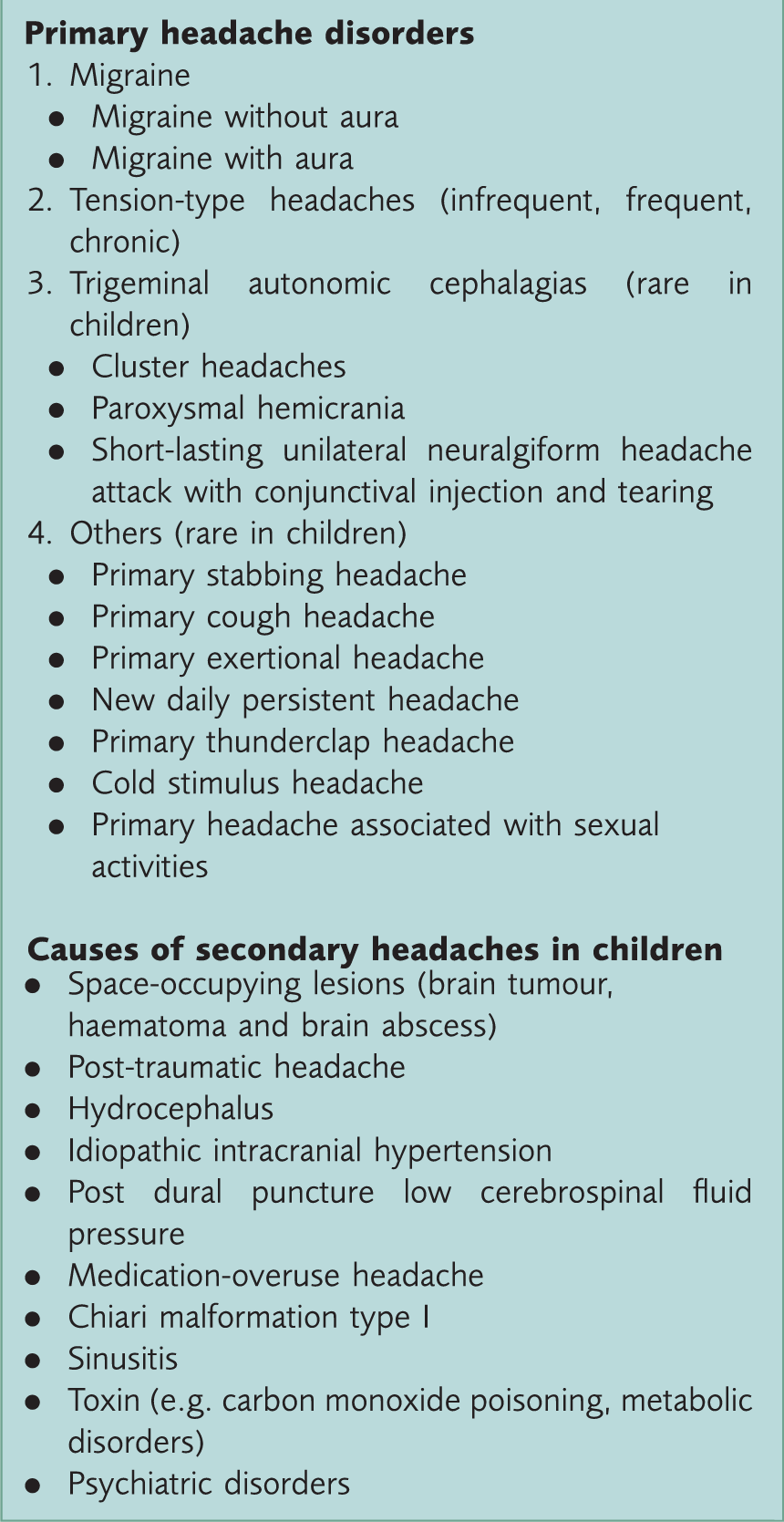
Headache disorders in childhood most relevant to GPs.
Types of migraine.
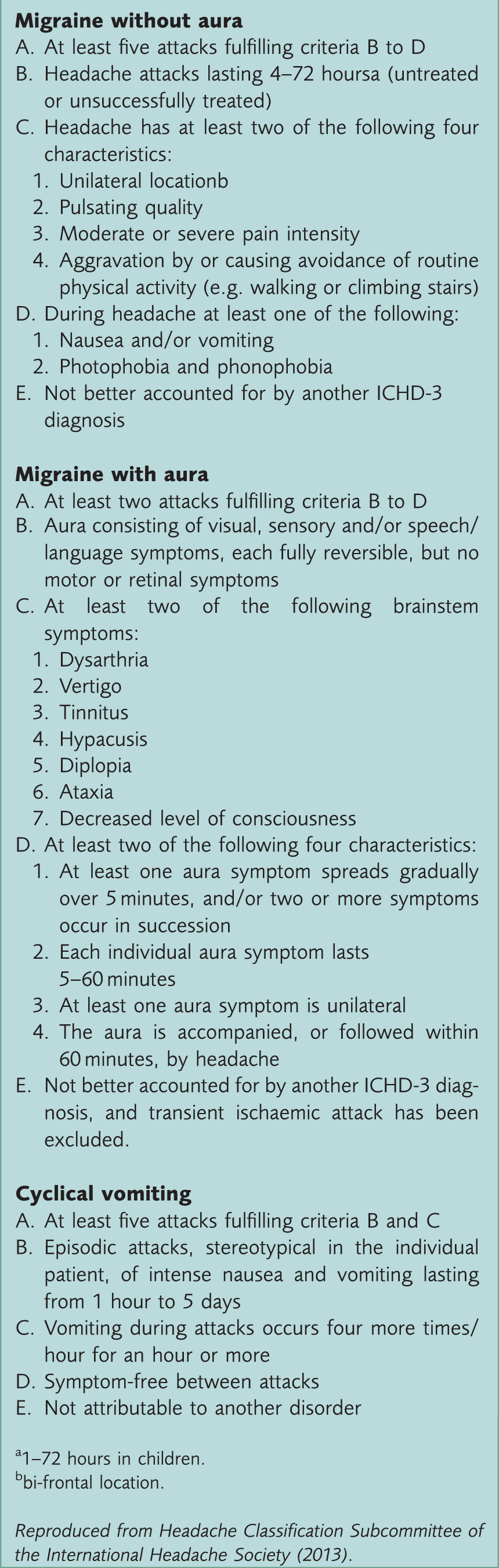
1–72 hours in children.
bi-frontal location.
Case study 1.
A 13-year-old boy presents with a 2 year history of recurrent, moderate, bi-frontal throbbing headache lasting for at least a day. His headaches are associated with vomiting, phonophobia, photophobia and visual aura. Further history reveals no red flags. Systemic and neurological examination is normal.
This boy has a good history of migraine with no red flags. Therefore, reassurance can be given that it is unlikely that there is any sinister underlying cause and treatment for migraine initiated.
Tension-type headache.
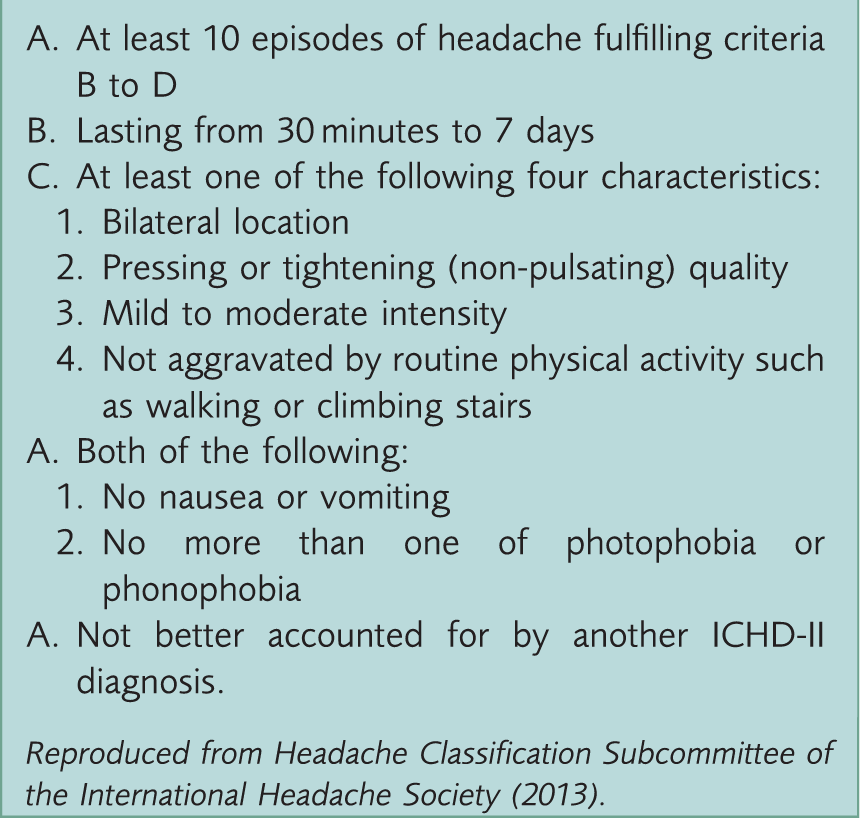
Reproduced from Headache Classification Subcommittee of the International Headache Society (2013).
Case study 2.
A 14-year-old girl presents with an 8 month history of recurrent, mild, bi-temporal headaches lasting from a few hours to a day, with an average frequency of four times a week. There are no accompanying symptoms. There are no specific triggers or other concerns. Systemic and neurological examination is normal.
In this case, a tension-type headache is the most likely diagnosis. Examination is normal and there are no red flag symptoms, so referral is probably unnecessary. It would be useful for the girl to keep a headache diary to see if her headaches are related to her environment and also to monitor her use of analgesic medication, as medication-overuse headache is a possibility.
Trigeminal autonomic cephalagia is another type of primary headache. In addition to severe unilateral headache, patients with this condition manifest associated autonomic features such as conjunctival lacrimation and / or injection, eye lid oedema, miosis, ptosis, facial sweating or nasal congestion.
Trigeminal autonomic cephalagia includes cluster headache, paroxysmal hemicranias, and short-lasting unilateral neuralgiform headache attack with conjunctival injection and tearing (SUNCT). These three conditions vary in terms of duration and frequency of headache attacks.
A cluster headache usually occurs in recurrent bouts, each lasting for a week or so and separated by remissions lasting more than 4 weeks. The bouts usually happen between once to a few times a year.
Paroxysmal hemicrania occurs with higher frequency, the attacks are shorter (2–30 minutes) and it does not present in clusters. SUNCT usually manifests with unilateral orbital, supra-orbital or temporal pulsating pain lasting 5–240 seconds with conjunctival injection and tearing. The attacks usually occur with a frequency of 3 to 200 per day. Other primary headaches (Box 7) are usually short lasting and not accompanied by autonomic features.
Treatment
The most immediate therapeutic action for primary headaches is to establish the diagnosis and to eliminate underlying triggers. Sufficient information to make a diagnosis can help GPs to arrange an appropriate care plan. Management of specific causes, such as carbon monoxide poisoning or anaemia, is usually straight forward.
Non-pharmacological measures such as distraction techniques and behavioural treatment have been proposed for the management of tension-type headaches. Additionally, simple analgesics and non-steroidal anti-inflammatory drugs can be useful; however, frequent use must be restricted in order to avoid medication-overuse headache. Aspirin is not recommended for children under the age of 16 years because of concerns regarding Reye’s syndrome.
Acute treatment of migraine attack
The family as a whole should be involved in the management of migraine in children. The avoidance of specific triggers and reassurance for parents are helpful. Additionally, sleep and/ or placing the child in a quiet dark room where he/she can rest are often an effective means to relieve the migraine attack.
Simple analgesics and triptans are the drugs of choice to treat acute attacks. The decision on which group of drugs to use depends on the response to previous treatment. Paracetamol and/ or ibuprofen are very popular to terminate an acute attack. There is no considerable difference in efficacy, tolerability or safety between these two drugs. The general principle is to start with a simple analgesic concomitant with an antiemetic. Domperidone is licensed for use in children of all ages. Migraleve, a combination of paracetamol and codeine, is popular in adults but it is not recommended for those under 10 years.
Some 5-hydroxytriptamine 1 (5HT1) receptor agonists (triptans) can be used for children who fail to respond to simple analgesics. Sumatriptan and zolmitriptan are most commonly used in migraine. Their use in children should be initiated by a paediatrician or paediatric neurologist. For patients aged 12–18 years, sumatriptan nasal spray can be used. Ergot alkaloids are not recommended for the treatment of migraine in children in primary care. In all cases, it is important to be aware that excessive use of analgesics can lead to medication-overuse headache.
Prophylactic treatment of migraine
Avoidance of triggers and provoking factors remains the foundation of migraine prevention; however, prophylactic medication may additionally be considered to minimise headache frequency and improve quality of life (e.g. school attendances). The main indications for migraine prophylaxis are:
Missing more than 3 days of school a month Having one to two migraine attacks a week No response to symptomatic treatment
Effective drugs to prevent migraine attacks.
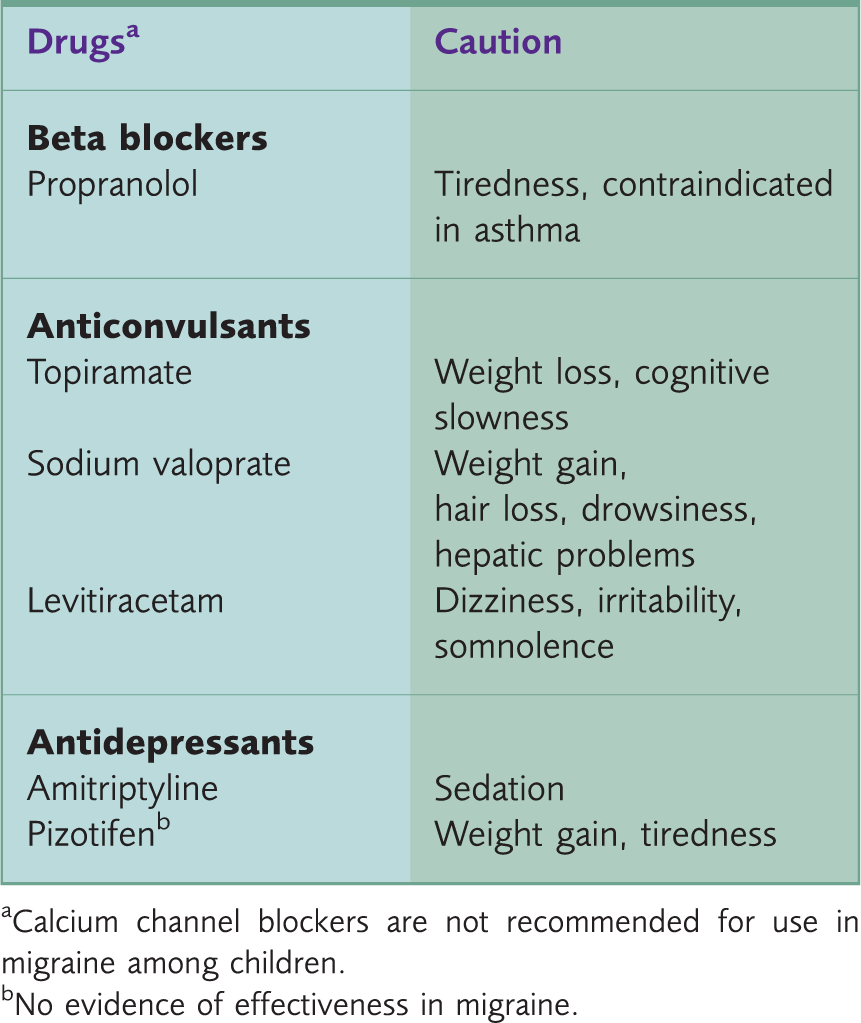
Calcium channel blockers are not recommended for use in migraine among children.
No evidence of effectiveness in migraine.
When to refer?
Children with a headache and abnormal neurological signs and/or ophthalmological findings should be urgently referred to a specialist secondary care service via the 2-week wait system. In patients with headaches of recent onset accompanied by either features suggestive of raised intracranial pressure, focal or non-focal neurological symptoms, an urgent same-day referral to the local paediatric team for urgent brain imaging should be made. Children presenting with red flags, those with suspected secondary headaches and those who are not responding to primary care treatment should also be referred. The referral guidelines for suspected brain cancer proposed in NICE (2005) also recommend the following:
Patients with a new, qualitatively different unexplained headache that becomes progressively severe: Make an urgent referral Patients with unexplained headaches of recent onset, present for at least 1 month but not accompanied by features suggestive of raised intracranial pressure: Consider discussion with a local specialist or referral (usually non-urgent).
Case study 3.
An 8-year-old girl presents with an 8 month history of recurrent, mild, bilateral, pressing headaches lasting from a few hours to a day. There are no accompanying symptoms. No specific triggers can be identified. Further questions reveal that her headaches cause sleep interruption. Systemic and neurological examination is normal.
In this case, the history suggests tension-type headache but interruption of sleep as a result of headache is a red flag symptom that might imply intracranial pathology. Consider discussion with a paediatrician/paediatric neurologist or referral.
Decisions about referral for healthy and well children with headaches can be difficult. If the parents are reassured and no follow-up is planned, employ safety netting by telling parents to seek advice if they notice their child is deteriorating. Follow-up in primary care can be also helpful as new symptoms and signs may develop with time in patients with life-threatening conditions such as a brain tumour. For healthy children with headaches that remain unclassified, arranging a second visit with the use of a headache diary in the interim may provide additional useful information.
It can be tricky to assess visual function and to be certain that fundoscopy is normal in younger children. If this is needed, a referral of these children to the local ophthalmologist or optician can be valuable. In addition, where there is diagnostic uncertainty or parental anxiety exists, referral for a specialist paediatric opinion may be warranted.
Case study 4.
A 6-year-old girl presents with an 18 month history of recurrent, severe, headaches. The headaches always occur over the left parietal site and last for hours. They used to occur once a month but a few months ago, their frequency increased to four times per week. The headaches are not associated with nausea, vomiting, phonophobia, photophobia or aura. There are no specific triggers. Systemic and neurological examination is normal.
In this case, there are concerns about increased headache frequency and unilaterally locked headache. These are both red flags which should prompt referral for specialist assessment.
Key points
Most headaches among healthy children are primary headaches with no serious underlying cause and can be managed in primary care Migraine is a headache with characteristic features and specific accompanying symptoms History taking can be difficult, as a younger child might not be able to provide clinical details, and there may be potential bias in the parents’ account due to parental anxiety History and examination should include specific reference to red flags Secondary headaches should be considered among children with abnormal neurological signs, red flags and or headaches that do not improve despite appropriate management and specialist assessment requested
Footnotes
Acknowledgement
We would like to thank Dr Lesley Ayling for her help with the writing of this article under the InnovAiT ‘buddy’ scheme.