
Abstract
The term ‘health inequalities’ is used to describe the differences in morbidity, life expectancy and access to healthcare influenced by the social and economic conditions in which a person lives. Many of these differences are unjust and can be modifiable if given appropriate support or treatment. This article considers health inequalities in the UK, the challenges they pose and potential actions to combat them.
The GP curriculum and health inequalities
Have an understanding of the impact of poverty, ethnicity and local epidemiology on a local community’s health Be aware of inequalities in health provision
Health inequalities and health inequities
Health inequality as a subject appears within the GP curriculum and throughout the medical literature on a regular basis. As a potential source of confusion the term ‘health inequity’ may also be used and is described as (World Health Organization (WHO), 2008): Health inequities are avoidable inequalities in health between groups of people within countries and between countries. These inequities arise from inequalities within and between societies. Social and economic conditions and their effects on people’s lives determine their risk of illness and the actions taken to prevent them becoming ill or treat illness when it occurs.
This definition importantly considers that these differences in health are potentially avoidable and are therefore unjust. It also recognises that socio-economic conditions are the primary influence on generating inequalities in health in the UK.
In 2008, the WHO published a report that stated that in Glasgow’s Carlton area the average life expectancy for a man was 54 years, whereas less than 10 miles away in the town of Lenzie, the life expectancy was 82 years. This statistic generated a lot of media interest at the time, with many stating the figure did not truly represent how long a person born in this area would actually live. Critics argued that the low figure for Glasgow’s Carlton area reflected certain issues more prevalent there, specifically the high number of homeless, hostel accommodation, high unemployment levels, drug- and alcohol-related deaths as well as suicide.
Nonetheless the statistic provides a valuable starting point to consider another concept closely linked with health inequalities called the social determinants of health, often defined as (WHO, 2008): The circumstances in which people are born, grow up, live, work and age, and the systems put in place to prevent and treat illness. These circumstances are in turn shaped by a wider set of forces: economics, social policies, and politics
Another key concept worth considering in relation to health inequalities is the ‘inverse care law’. This observation, described by Dr Julian Tudor Hart, is usually quoted as Hart (1971): ‘The availability of good medical care tends to vary inversely with the need for it in the population’. Another way of stating this is that those in the greatest need for healthcare (usually the most socio-economically deprived) are most likely to be those who have less access to it. Julian Tudor Hart made this observation some 40 years ago while working as a general practitioner in rural Wales. He observed that morbidity and mortality varied with geographical and social differences within the population. Current statistics suggest this concept still proves to be true today.
These definitions highlight the complex interplay of the many factors perpetuating health inequalities.
The historical political context
The understanding of the factors causing health inequality has been developing since ancient times. There are historical sources that show that even Hippocrates had recognised that ill health was not caused by supernatural causes. He instead stressed the importance of hygiene, and treating the patient in a holistic manner, taking into account their relationships and circumstance. Since that time medical knowledge has increased steadily and by the 19th century the link between disease and external factors (such as micro-organisms) was made. Robert Koch published work in 1890 that identified bacteria such as cholera and the effects of living conditions on the spread of infection.
Health inequalities can be found, to a greater or lesser extent, in any nation around the world. The Commission on the Social Determinants of Health Final Report published by the WHO in 2008 considered health inequalities on an international level. It remains a valuable reference comparing global health inequalities and contains many useful illustrative examples.
A more recent report has shown that the UK comes top for equitable access out of 11 developed countries (Commonwealth Fund Report, 2014). To build on this, several reports have looked at the social determinants of health in the UK. The Report of the Working Group on Inequalities in Health, now more commonly known as the ‘Black Report’ (after the then President of the Royal College of Physicians Sir Douglas Black who chaired the group preparing the report) was commissioned by the then Labour government but was subsequently completed and published during a Conservative government following a general election. The report demonstrated that although health outcomes across the country were generally improving, ill-health and death rates were not distributed equally among the population. It recognised that those in more deprived areas were suffering more ill-health than those in more affluent areas and the gap between these groups was widening. The report made wide-ranging recommendations to combat health inequalities, which included addressing social factors contributing to inequality, such as housing, education and employment, as well as changes to the NHS. The report was controversial due to the proposed considerable shift in social policy. It was published with a limited amount of print copies on the August Bank Holiday in an attempt to reduce its impact (Gray, 1982).
The ‘Acheson Report’ (Independent Inquiry into Inequalities in Health Report) was published in 1998. It continued to demonstrate that differences in health were associated with socio-economic status, i.e. the wealthier had better health and longer lives compared with the poor. No attempted dampening of the results occurred following its publication and the report made some impact in guiding future strategies to tackle inequalities in health. It made recommendations, including increasing the amount of state benefits for vulnerable groups, closer links between education and health, as well as measures to reduce smoking and alcohol consumption.
Current political policy in the UK
The ‘Marmot Review’ (Fair Society, Healthy Lives) was published in February 2010 based on proposing evidenced-based strategies to combat health inequalities in England. It discussed the concept of a social gradient in health, i.e. ‘the lower a person’s social position the worse his or her health’. It stated, however, that focusing solely on the most deprived would be to the detriment of everyone else; therefore, the report suggested ‘proportionate universalism’ whereby the scale and intensity of action to reduce health inequalities is appropriate to the level of disadvantage. The basis of this report influenced the current health strategies to both measure and tackle health inequalities.
The Scottish Government’s approach to tackle health inequalities comes from the 2008 document ‘Equally Well’. This proposed targets for particular areas such as the health of children, specific health conditions (e.g. coronary heart disease and cancer), mental health, and drug- and alcohol-related problems. ‘Fit and Well: Changing Lives 2012--2022’ sets out how Northern Ireland plans to tackle health inequalities promoting priority areas such as early years intervention and supporting vulnerable people and communities. In Wales ‘Fairer Health Outcomes for All’ takes a similar approach to the above papers in its plan to tackle health inequalities.
These policy documents demonstrate the breadth of organisations and services that are responsible for addressing health inequality and who should be making changes to improve the experience of patients. Many of these factors are beyond the work of the individual GP. Primary care is nevertheless in a pivotal position to positively influence some factors in their grasp. The fact that primary care services provide universal services, which include disease prevention, means that they can reach out to vulnerable groups at risk of health inequity.
Primary care approach to addressing health inequalities.
Examples of inequalities in health
Recommended further reading.
Healthy life expectancy
The average life expectancy (LE) in the UK is 79.0 years for a man and 82.7 years for a woman (Office of National Statistics, 2013a). It is also important to consider how much of a person’s life will be spent in good health, i.e. ‘healthy life expectancy’ (HLE). Within the UK, HLE varies significantly in different areas associated with socio-economic status. In England, the highest male HLE is in Richmond upon Thames at 70.3 years and the highest female HLE is 72.1 years, which is also found in the same area. This contrasts with the lowest figures for men of 55.0 years (Manchester) and for women 54.1 years (Tower Hamlets). Although this shows the significant differences in HLE between population groups consider also that, with the current state pension age of 65 years (and due to rise in the near future), a significant proportion of people of working age in socio-economically deprived areas are likely to be experiencing chronic ill-health when they would still be expected to work (Fig. 1).
LE and HLE for males at birth by local authority area in England (2011).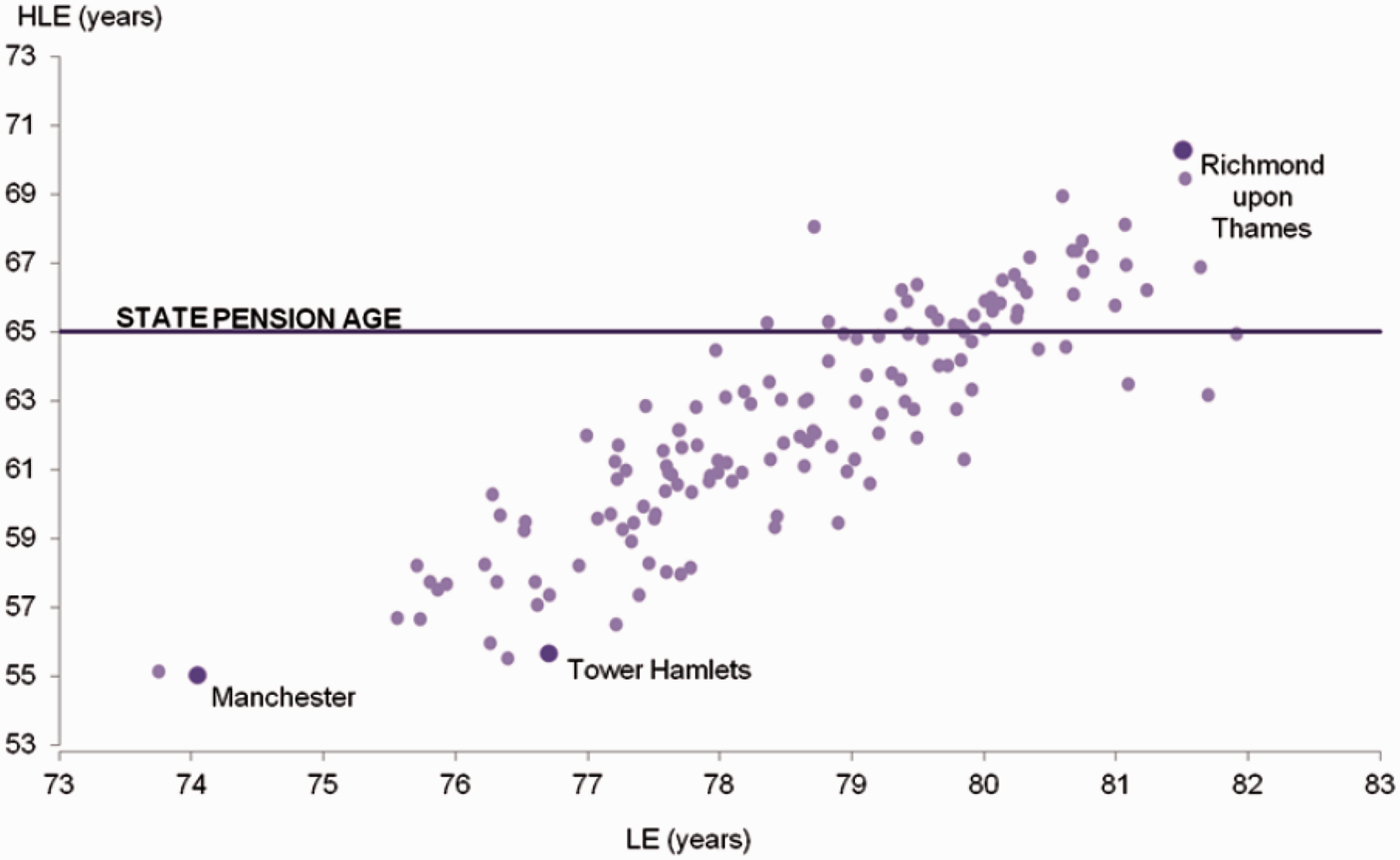
Onset of multi-morbidity
Multi-morbidity is the concept of having more than one chronic health condition, each of which is of equal significance (compared with co-morbidity whereby a primary health problem exists with other secondary health problems of lesser importance). Although it is recognised that multi-morbidity increases with increasing age, the onset of multi-morbidity in the most deprived areas occurs 10–15 years earlier than in the most affluent areas (Barnett et al., 2012) (Fig. 2). This suggests that GPs working in poorer areas are more likely to have younger patients with multiple health problems. This is likely to significantly impact on GP workload and patient complexity.
Prevalence of multi-morbidity by age and socioeconomic status (socio-economic status: 1 = most affluent and 10 = most deprived).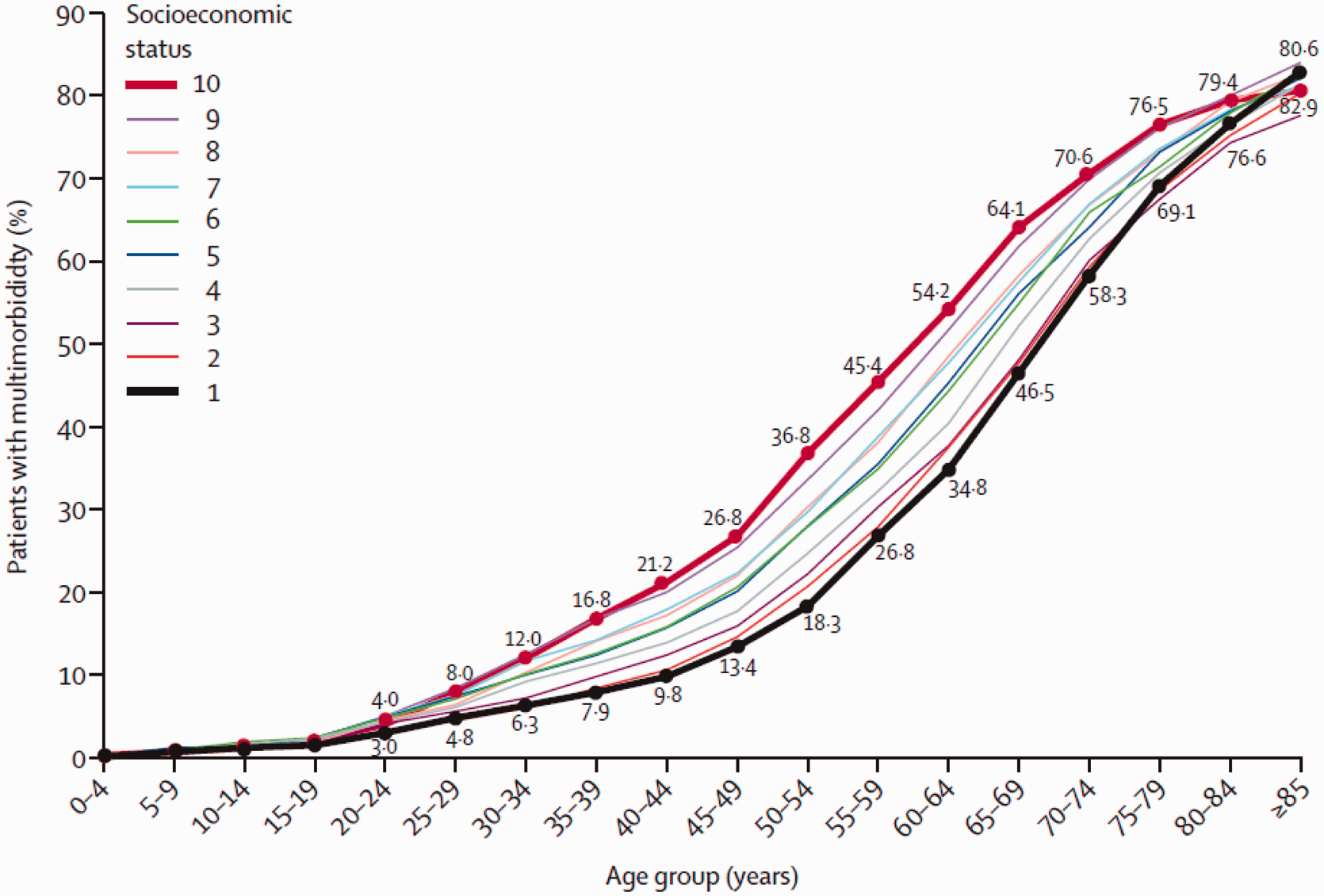
Cancer survival
It has been demonstrated that both the number of people diagnosed with cancer, as well as the likelihood of survival, are both influenced by socio-economic status. In the most deprived areas patients experience higher rates and poorer outcomes (Fig. 3). The reasons for this are complex but should be thought of in terms of the social determinants of health and the effects of the inverse care law.
Age-standardised incidence and mortality rates by deprivation quintile (2009).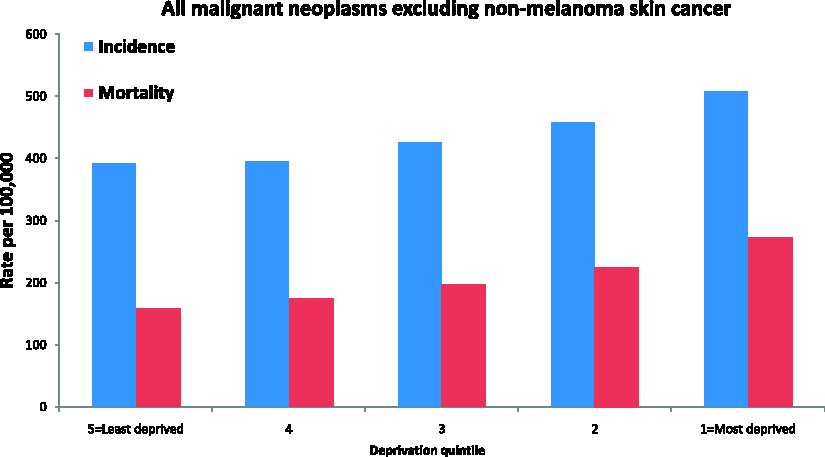
Child health
One example of the effects of deprivation on child health is seen through the association that exists between deprivation and obesity. Figures from the Health Survey for England show an association consistent throughout a child’s early schooling. Considering the numerous health problems associated with obesity in adult life; this health measure alone may indicate that more needs to be done regarding health promotion and education in schools based in more deprived areas (Fig. 4).
Prevalence of obesity in children by school year and index of multiple deprivation decile 2012/13.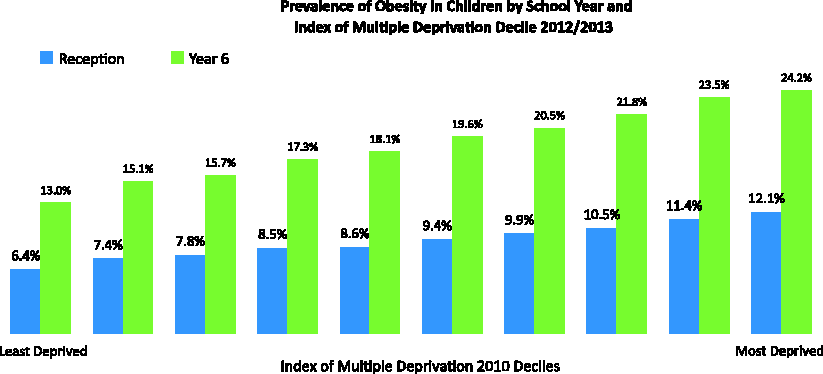
Socially excluded groups
RCGP policy work has shown that GPs as community leaders, commissioners and individual practitioners can positively influence the factors that drive inequality. It has developed a social-inclusion commissioning guide in response to a wide-ranging consultation on health inequality that focuses on the three most disadvantaged groups; the homeless, sex workers, and those from the gypsy and traveller communities.
The homeless
Case study 1.
John is a 29-year-old single, unemployed man with no fixed abode. He sometimes sleeps rough but also ‘sofa surfs’, periodically sleeping in friends’ houses. John has a past medical history of intravenous drug misuse and spent 6 years on a methadone programme. He has been free from methadone for the last 3 years and is not currently involved with addiction services. He comes to see you suffering with low mood and admits that he has started injecting heroin again; this time in his groin. He subsequently also mentions that he has noticed that his leg has become painful and swollen at the calf area. This is on the same side that he has been injecting.
The impact of homelessness on health is well recognised. LE is significantly reduced in this group as is the probability of attending the emergency department and subsequently being admitted to hospital (Crisis, 2011). This vignette raises a lot of issues to consider in a 10-minute appointment. John needs a comprehensive assessment of his mental state, his physical health, and signposting to other addiction, social and housing organisations. You should be prepared to organise your consultation to address the most acute issues first and not expect to tackle all of John’s problems completely in one consultation.
The fact that John has attended the surgery is encouraging and presents a good opportunity to help him address other health concerns. Often people who are homeless prioritise more immediate needs, such as searching for food and shelter. This, and the stigma around homelessness, can override the motivation to seek out support from mainstream general practice. There are innovative services providing outreach from hospitals and health promotion for this group, but individual practices can try and be flexible when providing appointments and support to those patients who have housing problems.
Good communication skills will help develop trust and be more likely to be successful in improving John’s health. Arrange John’s follow-up with you to assess his progress from today’s consultation. Continuity of care with one GP will mean John does not have to explain his problems from the beginning when he is next seen at the surgery. He is likely to require further review from other healthcare providers and part of your role as a GP is to help coordinate this effort. Ensure you hold accurate details of John’s address and telephone number (including mobile telephone) so that he can be contacted if required.
Good communication with other members of the primary care team is also important as they may need to be aware of John’s situation. One mechanism of doing this may be to discuss his case at a regular practice or primary healthcare team meeting. John may be a suitable patient to add to your admission avoidance case management register and have a care plan that is regularly reviewed.
Sex workers
Case study 2.
Nadia is a 32-year-old sex worker who was trafficked from Albania as a teenager. She has no family or friends nearby. She lives within a ‘parlour’ that she works from, but worries constantly about being made homeless. She finds support from a sexual health specialist nurse who runs a mobile clinic in the city centre near where she works. She receives a full sexual health screen, obtains contraception advice, and is signposted to housing services and charities that can support and rehabilitate those who have been trafficked.
The key health issues within this group include substance misuse and sexually transmitted disease. Early intervention in chaotic lives by primary care can contribute to preventing possible addiction, which can in turn lead to prostitution. From an individual practice point of view, it is important to establish positive trusting relationships with patients who are sex workers and be aware of the services available to help them. If engaging with primary care, Nadia would benefit from regular sexual health screening, contraceptive advice and signposting to organisations that can support her situation. As with homelessness there are outreach ‘one stop shop’ projects in the UK promoting services to sex workers where they work and on their terms. This case highlights the fact that one-quarter of sex workers in the UK are migrants and their potential illegal immigrant status and vulnerability for exploitation from those who have trafficked them can make them hard to reach (TAMPEP, 2009).
Gypsies and travellers
Case study 3.
Jonas is a Polish Roma immigrant and father of four children. He tries to encourage his children to regularly attend school but as he has received verbal abuse from the surrounding neighbourhood feels that he is judged by education and health services. He attends a meeting in the community centre between his community and the council leader and learns about primary care services. He was not aware this was accessible to his family. He was not aware that health prevention measures (such as immunisations) are freely available for his children.
Lack of engagement with primary health care services in gypsy or traveller communities can be due to low levels of literacy, discrimination from society and traditional health-beliefs. A myriad of health problems can affect this community, which include a higher rate of long-term conditions, and alcohol and substance misuse. This group of the population is reporting the highest level of perinatal mortality of all ethnic groups in the UK with 17.6% of mothers experiencing the death of a child compared with 0.9% of the general population (Selway, 2009). Media coverage has perpetuated this group’s mistrust in public services particularly in children’s social services. This case highlights the power of developing relationships between communities and services that can provide them with healthcare. In most cases, this group requires specialist services that include one-to-one work and outreach with a view to encouraging appropriate use of primary care services (Selway, 2009). A particular unmet need is maternal and child health; GPs should be aware of these issues if consulting with members of this community and access local specialist support.
Health inequalities: challenges and advice
Patient complexity
Those experiencing inequalities in health often have complex backgrounds and may have more than one medical problem that they wish to have treated when seen in your consulting room. To help combat complexity the use of clear record-keeping will allow you to more easily assimilate the patient’s medical record before you start your consultation. Use of problem headings and linkage of diagnosis to medications will benefit not only you but also any future medical professional wishing to read the patient file. Agreed care plans and regular review through the practice Case Management Register can be a useful tool for the most complex patients.
Multi-morbidity
Traditional medical consultations usually focus on one condition per patient per consultation. If a patient consults with a list of problems, ask which are the most important to them so that you can prioritise the consultation. You may also be aware that some symptoms the patient thinks are less important may actually indicate early signs of a more sinister disease (e.g. weight loss and change in bowel habit in a middle-aged patient) and so you can work together with your patient to decide on the problems that will take priority.
Time keeping
Ten minutes is very little time with a complex patient. Consider providing longer appointments for patients with complex needs or with a particularly tricky problem that needs to be worked though. However, even with longer appointments, you will still not be able to solve all your patient’s problems in one visit and most patients will not expect you to do so. Prioritisation of problems is important, but continuity of repeat appointments over time is also a useful tool that enables you to build rapport with your patients, and build-up a picture of their health and social care needs. This enables a more effective use of consultation time and targeting of scarce resources.
Non-attendance
Following the concept of the inverse care law, access to health services is often more challenging for those in the greatest need. Non-attendance for booked appointments should be recorded in the patient’s medical records. This allows identification of repeated non-attendance. Non-attendance both at GP surgeries and hospital outpatient appointments should be discussed with patients at the next opportunity. This may identify an appropriate reason for non-attendance (e.g. transport issues, childcare commitments) or lack of understanding for the need for follow-up. In some instances non-attendance can suggest neglect of health needs. Non-attendance of children for appointments should certainly be followed up as it may raise issues regarding child safeguarding.
Language problems
Patients who experience inequalities in health may not use English as their first language, which compounds their difficulty in accessing and understanding healthcare. Use of translation services via telephone, or booking translators to attend, can be helpful although often requires some pre-planning and sensitivity to gender and ethnicity issues as well as language issues. Use of family members is not recommended as it can be a barrier to information sharing between the patient and the doctor. Online translation services (e.g. Google Translate) appear convenient but the accuracy of the translation can be debatable.
Lack of familiarity with local services
Often GP trainees are working in areas separate from those in which they live, in particular if you work in a socially disadvantaged area. Many services are likely to exist from specialist health services, charities and religious groups to help patients with mental health, drug or addiction problems. Details of these groups are not always easy to find, so if you encounter a patient already involved with a service it can be helpful to establish what that service provides and how to access it. Within practices, it can be useful to keep a directory of useful local and national support services. Health visitors, practice carer leads and vulnerable patient leads are particularly useful sources of information about local services.
Lack of experience in health inequalities
GPs working in affluent areas may have limited experience of certain issues more frequently encountered in more deprived areas. For GP trainees working in such areas, consider the possibility of arranging a short period of time swapping with another trainee placed in a less affluent practice to gain further experience. Also consider if your GP training group could organise a teaching session on health inequalities. In some areas there may also be specific GP surgeries such as those for homeless or asylum seekers and refugees who may be willing to allow GPs short placements to gain experience in the work that they do.
Hidden health inequalities
It is easy to assume that health inequality only exists within populations deprived economically and educationally. Within every community there is a risk of fragmented access to services and therefore two patients attending with the same problem may have very different experiences. Each individual patient has a unique situation regarding employment, housing, finances, family network and/or close relationships, and caring responsibilities (including for children). All of these factors will impact on their ability to manage an illness and access healthcare. Even in affluent areas a self-employed person suffering from a sprained ankle trying to keep down two cleaning jobs will likely suffer from health inequality compared with a business man with access to private physiotherapy and with the ability to work from home.
Conclusions
Health inequality is present all around us. As a GP you are well placed to identify unmet need and be an advocate for wider social change for your patients. Despite the unique nature of each individual vulnerable group there are some common themes. These include discrimination and lack of access. Within practices and your own professional life you can try to challenge barriers and enable a positive patient experience.
Key points
Health inequalities are differences in illness, LE and access to medical care between different population groups Health inequities are inequalities in health that are potentially modifiable given the appropriate support Inequalities in health in the UK are predominantly due to differences in socio-economic status Awareness of the determinants of health inequalities can enable you to identify those who are struggling with accessing the right support from health services.