
Abstract
In 1817, James Parkinson described a ‘shaking palsy’ that subsequently took his name. Parkinson’s disease is a chronic, progressive neurological condition that has a profound impact on a sufferer’s quality of life. It is common condition that will affect around 1 in 40 of us in our lifetimes. Early diagnosis results in treatment to reduce symptoms and preserve quality of life, but also enables planning for the future. Most patients with Parkinson’s disease will initially present to their GP. This article explains why diagnosis can be difficult and provides a guide to possible features that might trigger referral for specialist diagnosis.
The GP curriculum and Parkinson’s disease
Know the indications for referral to a neurologist for chronic conditions that require on-going specialist management and conditions that require early treatment to avoid permanent deficit Communicate prognosis, including any uncertainties, truthfully and sensitively to patients with disabling neurological conditions such as Parkinson’s disease (PD) Understand the principles of treatment for common conditions that are managed largely in primary care including PD
What is Parkinson’s disease?
Epidemiology
Parkinson's disease (PD) is the second-most-common neurodegenerative disease (Parkinson’s UK, 2009). It affects all ethnic groups with prevalence and incidence both being age-related (Fig. 1). The overall prevalence in the general population is estimated at 274 per 100 000 (Parkinson’s UK, 2009) with an annual incidence of 13 per 100 000 (Von Campenhausen et al., 2005). There is a 1.3-times greater risk of PD in men compared with women (Parkinson’s UK, 2009). The mean age of presentation is 65 years, with 2% of the population aged 80 and over having PD, but it is important to remember that 1 in every 20 newly diagnosed patients (about 10 000 per year in the UK) is under the age of 40 (Parkinson’s UK, 2007).
Increasing prevalence of PD by age.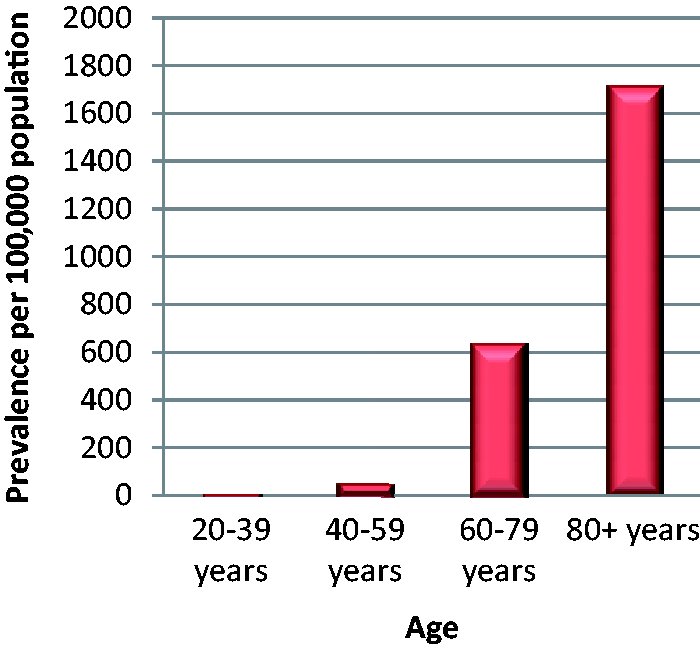
Pathology
The pathological basis for the symptoms of PD is the loss of dopaminergic cells in the substantia nigra. This leads to a reduction of the thalamic stimulation of the motor cortex and the motor effects of PD. The depletion of other neurotransmitters may play a part in the development of other non-motor symptoms (NMS), such as depression.
Cause
The cause of PD remains uncertain, but it is likely to be due to a combination of genetic risk factors and environmental agents. Up to one in five patients with a new diagnosis of PD have a family history in a first- degree relative (DiFonzo et al., 2005); a family history is more likely with early-onset PD. Although up to 14 genes have been implicated, mutations in five causative genes may account for around 2–3% of all cases of PD with clinical features similar to the classic disease (Klein and Lohmann-Hedrich, 2007). Perhaps the best known of these is the Parkin mutation that is inherited in an autosomal recessive pattern and associated with PD under the age of 46 years (Scottish Intercollegiate Guidelines Network (SIGN), 2010).
Symptoms have also been associated with exposure to certain chemicals, and particularly pesticides (European Food Safety Agency, 2013). This suggests that exposure to an environmental, or even endogenous toxin, may also play a role in the development of PD.
Costs
PD is a progressive and disabling neurological disease. In addition to the costs to the individual in terms of reduced mobility and independence, in most patients there are costs of on-going drug treatment and social support within the home. Furthermore, PD is a frequent cause of falls, fractures and hospital admission; the prevalence of PD in residential and nursing homes is 10%. As such, PD is a costly disease, especially in the later stages. The annual estimated costs of PD vary widely according to the model used for their calculation. However, in 2010 it was estimated that the annual cost in the UK of just health and social care for patients with PD was €2 361 000 (Fineberg et al., 2013). Another study done in 2007 estimated the costs to be £13 804 per person per year (McCrone, Allcock, and Burn, 2007).
Diagnosis
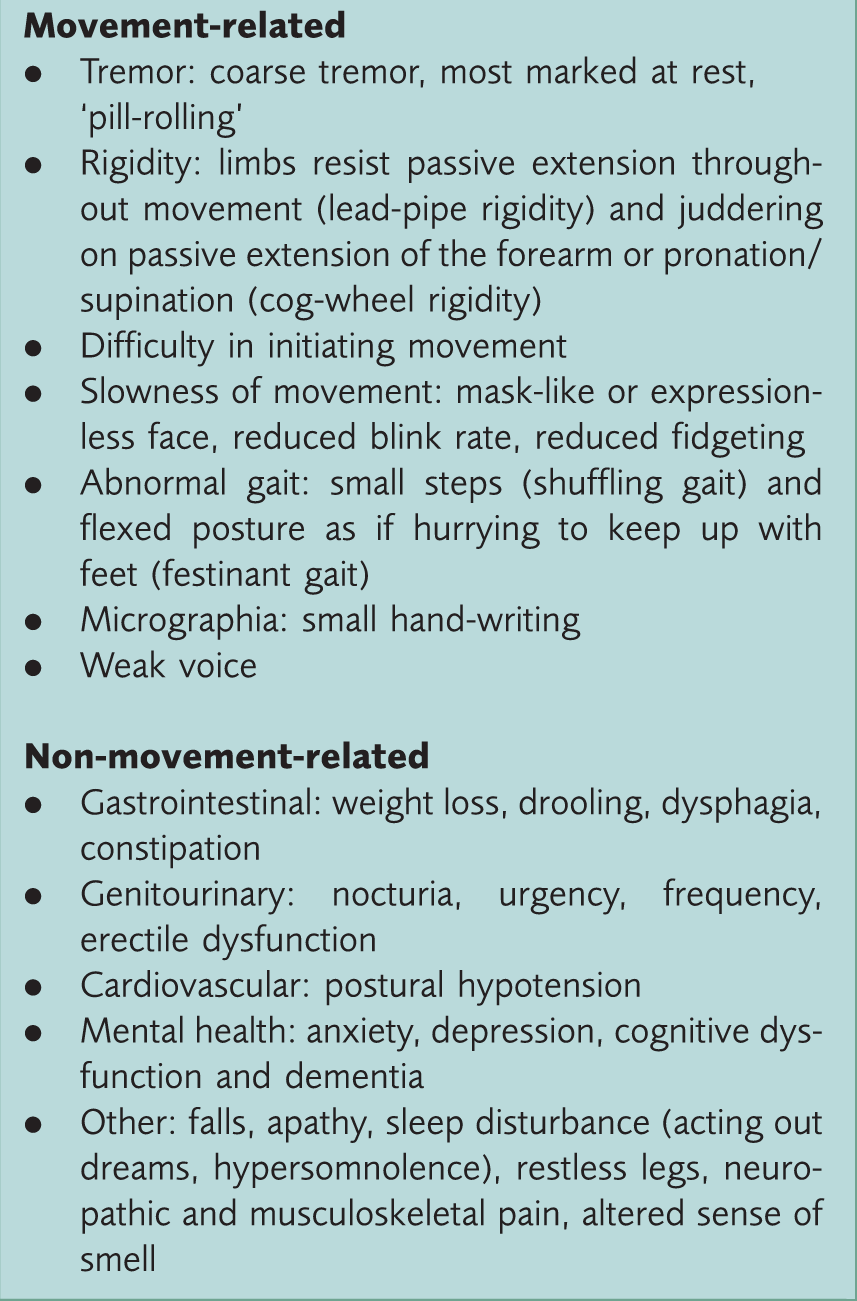
Summary of symptoms and signs of PD.
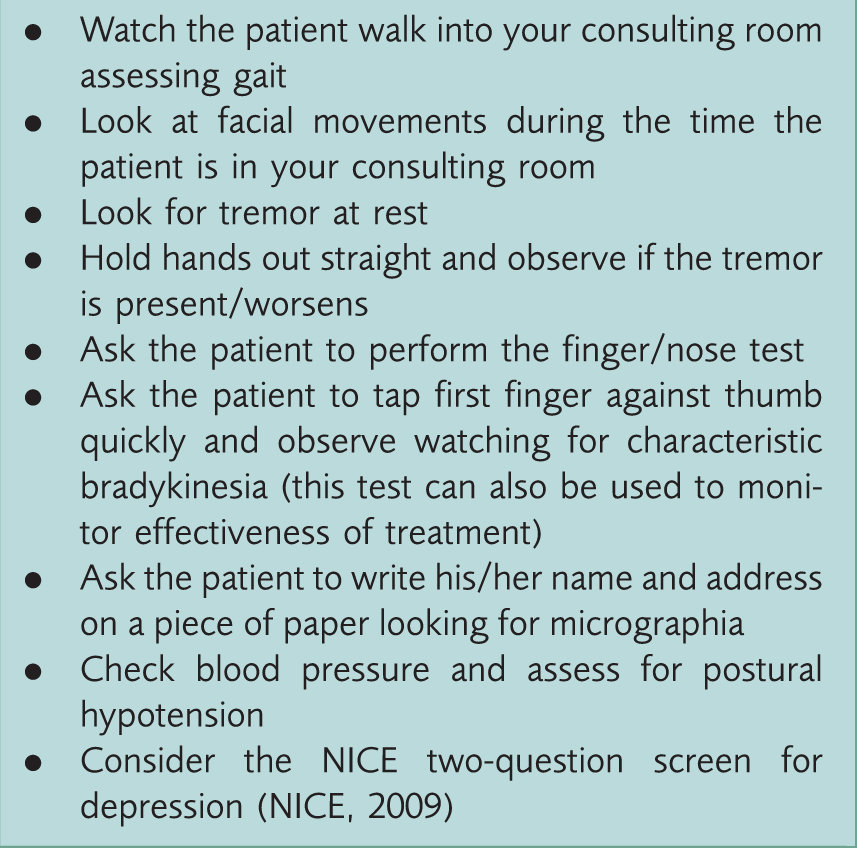
Rapid examination for PD for use in a 10-minute consultation.
A definite diagnosis of PD is difficult. Diagnostic error is common with an error rate of up to 50% in community-based studies (Meara, Bhowmick, & Hobson, 1999). A GP with an average list size of about 1500 will see only one new case of PD every 3.3 years, which makes it difficult to develop and maintain expertise (SIGN, 2010). Therefore, although a diagnosis of PD may be strongly suspected in primary care, unless very frail, patients should always be referred to a specialist for confirmation of diagnosis
In secondary care, PD is diagnosed following a detailed clinical examination. The use of standard diagnostic criteria, such as the UK Parkinson’s Disease Society Brain Bank and Gelb criteria, have been shown to increase diagnostic accuracy (NICE, 2006; SIGN, 2010). This article highlights the possible ways that patients with undiagnosed PD may present to primary care to enable prompt referral if a diagnosis of PD is suspected.
Motor features of PD
PD is a movement disorder and has the classic symptoms and signs of:
Tremor Bradykinesia (slow movements) Hypokinesia (poverty of movement), and Rigidity
Tremor
Typically, patients with PD have a unilateral resting tremor, and this may be the presenting complaint. However, PD can cause bilateral tremors even on first presentation and the tremor may fluctuate, meaning that it is more obvious at some times than others. Alternatively, the tremor may be noticed by the GP incidentally when the patient is consulting for another reason. The patient may already be concerned about an underlying diagnosis of PD as this is perhaps the best known feature of the disease, but this fear may not be disclosed immediately.
The tremor of PD occurs at rest, is briefly suppressed by motion and re-emerges on maintaining a posture, for example, holding a cup of tea. The tremor is a rhythmic, repetitive movement, with a rate of two to five movements per second in the thumb and index finger (‘pill-rolling’) or at the wrist. The legs may also shake in the same way when inadequately supported. The tremor is worse when the patient is tired, under stress or when attention is drawn to the tremor.
Bradykinesia
Patients with PD become slower in all movements (bradykinesia) and movements may be restricted in range. Gait is particularly affected and patients are described as having:
A ‘shuffling gait’ characterised by short steps, with the feet barely leaving the ground, producing an audible shuffling noise. Small obstacles tend to cause the patient to trip Turning ‘en bloc’, keeping the neck and trunk rigid, and requiring multiple small steps to accomplish a turn Gait freezing characterised by an inability to move the feet, which may worsen in tight, cluttered spaces or when attempting to initiate gait A stooped, flexed posture as if the person is hurrying to keep up with his or her feet or ‘festinant gait’
If a patient is taking longer than you might expect to get to your consulting room, take a look to see how that person is walking. If a patient is very slow to initiate movement and shuffles towards your consulting room door, at times feeling it hard to initiate or carry out movements, this is suggestive of possible PD.
Hypokinesia
Hypokinesia (poverty of movement) manifests as loss of facial expression, loss of arm swing and difficulty with movement. This may affect one side of the body before the other. On the affected side, the arm stops swinging when walking and the leg feels heavy. The voice tends to lose its natural inflexions and eventually becomes very weak.
The natural mobility of the patient’s face reduces so that the face becomes less communicative and eventually a ‘masked’ or expressionless appearance develops. Although mental alertness is unaffected for many years, this can give the impression that the patient cannot understand, is disinterested in the world around, or depressed (but remember that up to 40% of patients with PD do have depression).
Rigidity
Gradually the characteristic Parkinsonian rigidity sets in, usually on one side; however, both sides become affected as the condition progresses. Hand-writing becomes smaller (‘micrographia’). Muscle tone is increased with the classic ‘lead pipe’ or ‘cog-wheel’ rigidity. The tendon reflexes are usually normal or even a little brisk and the planter reflexes are flexor.
Non-motor symptoms
Parkinson’s UK has produced a ‘Non-motor symptoms questionnaire’ with 30 yes/no questions relating to the month prior to the consultation. This can be given to patients to aid recognition of NMS when a diagnosis of PD is suspected.
Sensory disturbances
A disturbed sense of smell affects up to 90% of patients with PD and may be of use as a pre-clinical marker (Parkinson’s UK, 2007). Pain is also a common symptom, affecting up to 50% of PD patients (Parkinson’s UK, 2007). Pain may be neuropathic in nature, with paraesthesia, burning dysthaesia, coldness, numbness, or deep aching, and may be related to motor fluctuations. Musculoskeletal pain may also result from rigidity and hypokinesia.
Psychiatric symptoms
Anxiety is common and may be pre-clinical indicator of PD. It takes the form of generalised anxiety, often with panic attacks, and also obsessive–compulsive behaviours such as compulsive eating and punding (repetitive performance of meaningless tasks) (Parkinson’s UK, 2007).
Depression is also common, affecting up to 40% of patients with PD (and also 40% of their carers) (Van der Hoek et al., 2011). It may present with feelings of guilt, helplessness, remorse or sadness but often goes undetected. Always consider screening patients with suspected Parkinson’s disease for depression (Box 2).
Apathy is also a common symptom among patients with PD and seems to be independent of depression or fatigue. It does not respond to treatment of the underlying PD.
Dementia eventually affects 40% of patients with PD (Parkinson’s UK, 2007). The proportion of patients with dementia increases with time post diagnosis, with up to 80% affected 20 years after intial diagnosis. It is progressive and characterised by cognitive impairment, impairment of visuo-spatial abilities, impaired concentration, excessive sleepiness, visual hallucinations and delusions.
Sleep disturbances
Most people with PD have problems with sleep. The causes are multifactorial, but degeneration of the sleep regulation centres in the brain has been implicated. Specific sleep problems that are more common among patients with PD include:
Hypersomnolence: Excessive daytime sleepiness and dozing affects up to 50% of patients with PD (Parkinson’s UK, 2007) Restless legs syndrome Rapid eye movement (REM) sleep behaviour disorder: This involves the loss of the normal skeletal muscle atonia during REM sleep, resulting in physical acting out of dreams. This often precedes the development of motor symptoms in patients with PD
Weight loss and dysphagia
Unintended weight loss is common in individuals with PD. Moderate or severe dyskinesia can be the cause, however, if the patient presents with significant weight loss, other medical causes, such as malignancy, endocrine causes or poor diet, should be considered.
Swallowing difficulties usually relate to disease severity and may affect all phases of the swallow process. There is a risk of aspiration pneumonia, malnutrition and dehydration if swallowing difficulties are severe.
Autonomic disturbance
Autonomic dysfunction (dysautonomia) is common in PD, due to the effects of the disease on the autonomic nervous system. It can manifest in many different ways.
In the genitourinary system, autonomic dysfunction may lead to urinary symptoms in 40% of patients with PD. These include nocturia, urgency (including urge incontinence) and/or frequency. Sexual dysfunction is also common resulting in erectile dysfunction in men, or difficulty with arousal, orgasms, dyspareunia or vaginismus in women.
In the gastrointestinal system, autonomic dysfunction often results in constipation, which affects around half of all patients with PD. Sialorrhoea (excessive saliva or drooling) can occur in 70–80% of people with PD (Parkinson’s UK, 2007). In addition to social embarrassment and soiling of clothing, sialorrhoea may also be associated with perioral infection.
Postural or orthostatic hypotension affects 50% of patients with PD (Parkinson’s UK, 2007). It is defined as a fall in systolic blood pressure of over 20-mm mercury on standing. Patients who are experiencing orthostatic hypotension may complain of dizziness, visual disturbances, falling or fainting.
Falls
Due to a combination of abnormal gait and postural hypotension, frequent falls are common in patients with PD. It is important to take a detailed history about the exact events surrounding any fall: was this a simple trip or something else? There are is a helpful InnovAiT article on falls in the elderly (Lawrence, 2008) that provides more information on this topic.
Differential diagnosis
Differential diagnosis of PD.
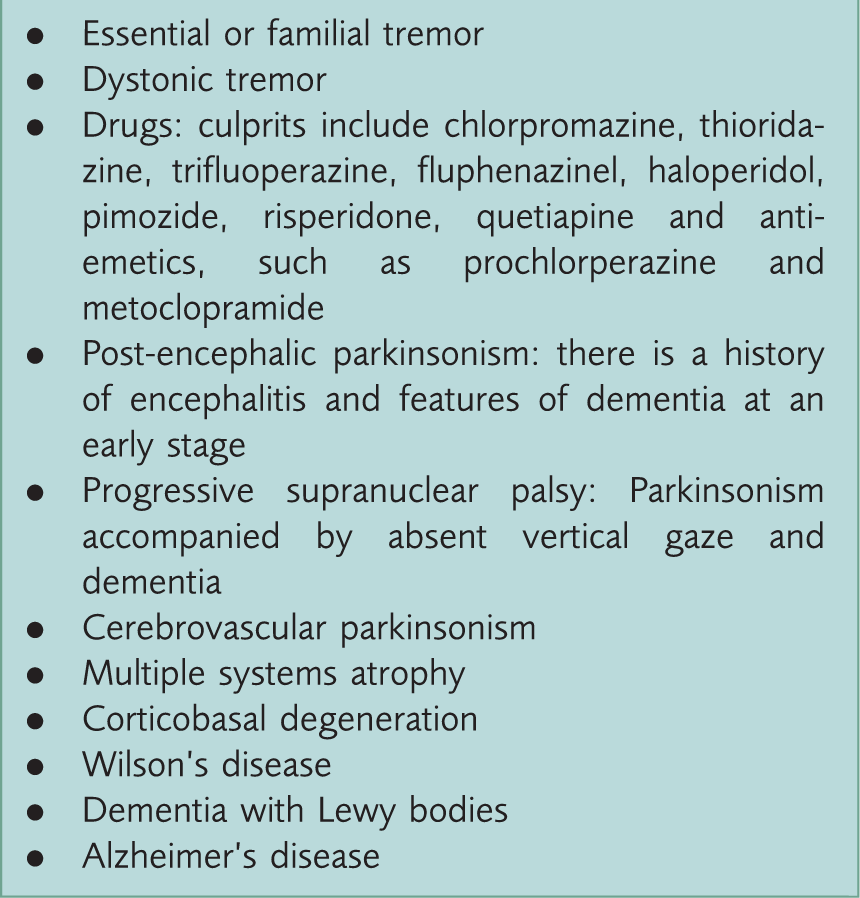
Another common cause of Parkinsonian symptoms is neuroleptic drug treatment. Withdrawal of the drug is likely to result in resolution of symptoms.
It is also common, as the illness evolves, for the diagnosis to change. Some patients have a delayed diagnosis of PD as they do not present with typical symptoms early in the course of their disease. This is especially true if tremor is not an early symptom. Other patients with a diagnosis of PD later develop atypical features and the diagnosis is revised to another.
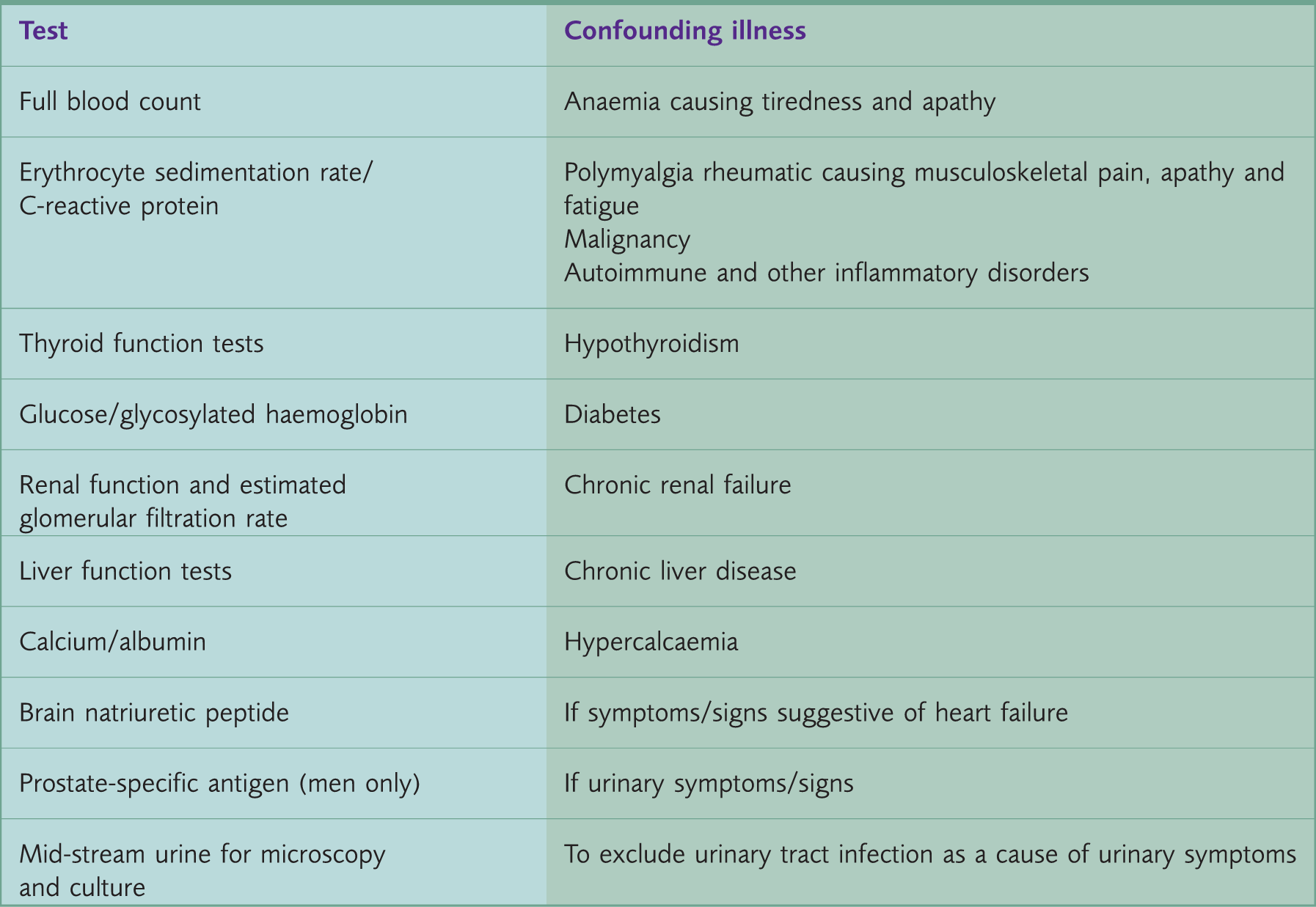
The role of investigations
Investigations that can be performed to exclude a confounding illness.
Communication
PD can be a devastating condition affecting every aspect of the patient’s life. The manner in which the diagnosis is communicated to patients and carers is very important and has been shown to have a significant effect on quality of life many years later. Patients and their families may already suspect a diagnosis of PD, particularly if another family member or close family contact already has PD.
In all cases, it is important to explore patients’ and carers’ views about what may be wrong and to address any worries or fears they may have (SIGN, 2010). If on clinical assessment you feel that there are features suggesting a diagnosis of PD, it is important to explain that diagnosis is complicated, and that specialist referral is needed to evaluate the situation further and confirm or refute the diagnosis. If further information or support is needed, Parkinson’s UK has a useful website (www.parkinsons.org.uk) with information for patients and also runs a helpline (telephone: 0808 800 0303).
Key points
PD is a common neurodegenerative disease that is more common with age, and has profound effects on an individual’s lifestyle and independence Early diagnosis enables drug treatment to preserve quality of life and allows planning for the future, however, presenting features can be very variable and subtle; having a high level of awareness is key Patients may present with motor symptoms (tremor, bradykinesia, hypokinesia and rigidity) and/or NMSs (autonomic dysfunction, depression, anxiety, weight loss, dysphagia, and/or falls), or signs may be noticed incidentally when the GP is seeing the patient about another problem All patients with a suspected diagnosis of PD should be referred to an appropriate specialist for confirmation of diagnosis When communicating with patients and families about a suspected diagnosis of PD, it is important to stress that diagnosis is difficult and should be made by a specialist and to address patients’ and carers’ worries and fears