
Abstract
A feeling of blocked ears is a common presentation in general practice. Often this is caused by excess wax in the auditory canal, with subsequent ear irrigations for wax accounting for around 2 000 000 visits to primary care in England and Wales each year. There are many other causes of a blocked ear sensation, including important ones that should not be missed. GPs should therefore have knowledge of the causes and treatment, and appreciate when ear, nose and throat referral may be required. This article addresses the clinical assessment and management of the most common and serious pathologies.
The GP curriculum and blocked ears
Manage primary contact with patients who have a common/important ENT, oral or facial problem Understand how to recognise rarer but potentially serious conditions Carry out appropriate examination including more detailed tests where indicated, e.g. audiological tests Appreciate that pathology in other systems may lead to ENT-related symptoms Understand when urgent (or semi-urgent) referral to secondary care may be indicated Empower patients to adopt self-management strategies where possible Know the community services that may be available, e.g. for audiological assessment
History
Causes of a blocked ear sensation.
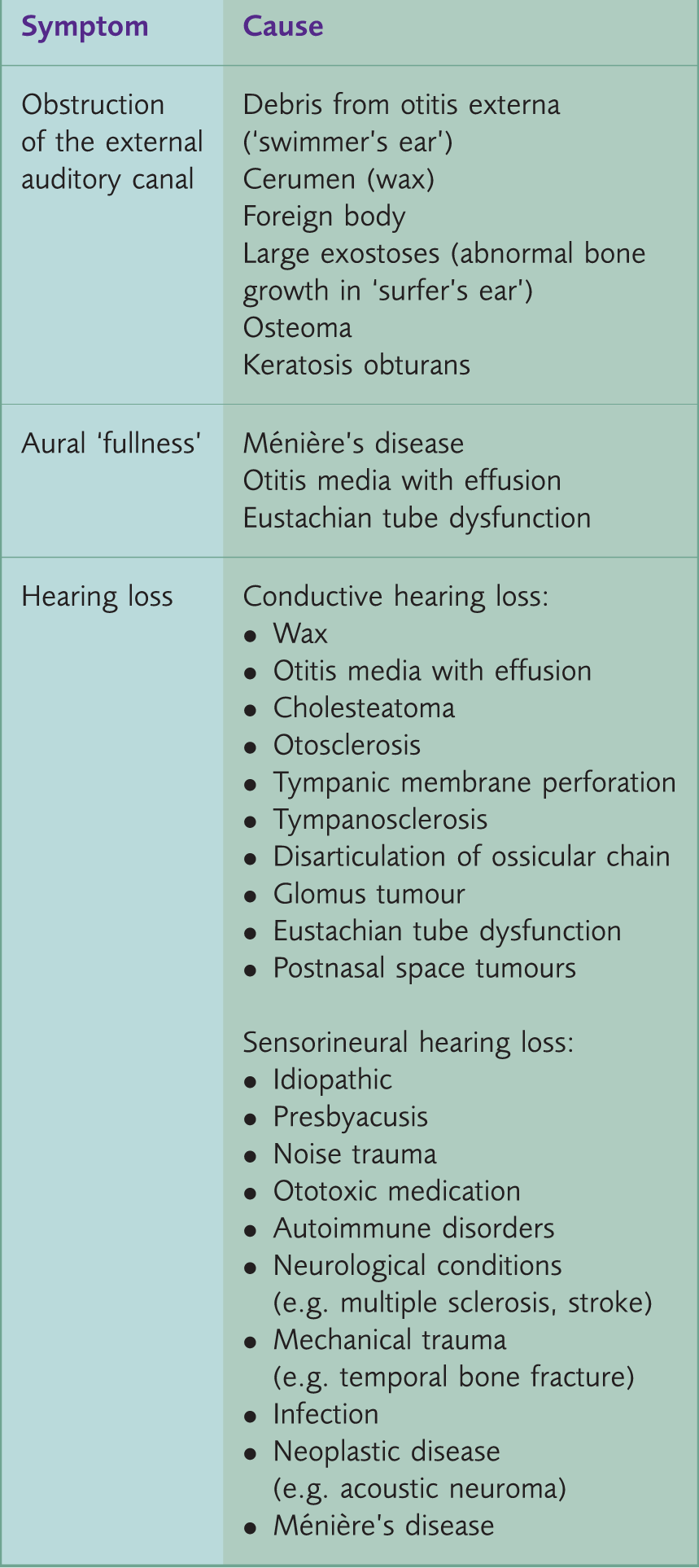
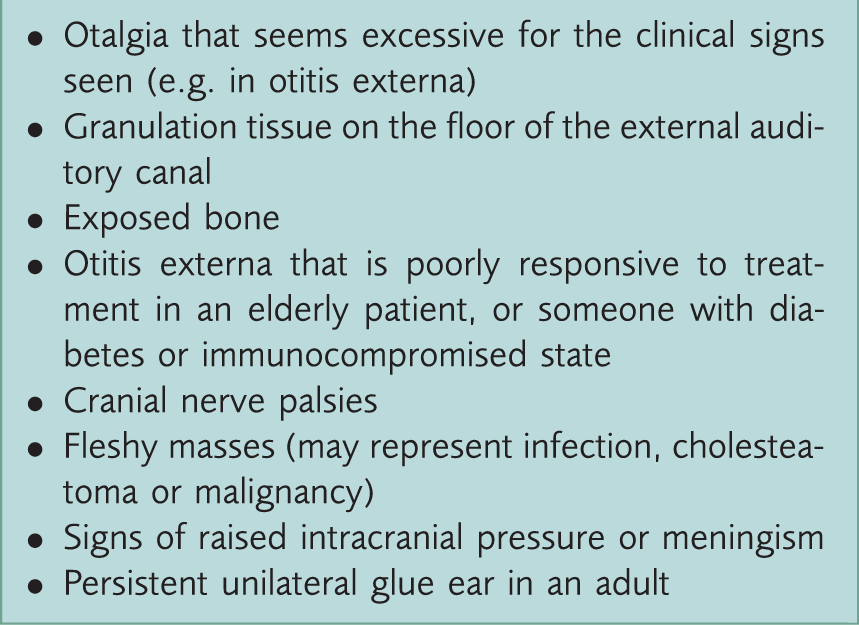
Red flag symptoms and signs.
The key symptoms to ask about are pain in the ear (otalgia), discharge (otorrhoea), vertigo, hearing loss and tinnitus. The history should determine the severity of symptoms, whether they fluctuate, the period over which they developed, and whether one or both ears are affected. In patients complaining of dizziness assess whether this represents vertigo (an illusion of movement or a spinning sensation) rather than pre-syncope, disequilibrium (imbalance), or light-headedness. Try to establish the degree to which the patient’s quality of life is affected by his or her symptoms.
A targeted assessment of risk factors may include enquiries about age, past medical history (diabetes or immunosuppression, previous ear problems or surgery), use of ototoxic medication (such as aminoglycosides, loop diuretics, non-steroidal anti-inflammatory drugs, platinum-based chemotherapy), noise exposure, and family history of hearing loss.
Special considerations in children
Birth history may be relevant, and should establish the presence of risk factors for hearing impairment, such as prematurity, intensive care admission, and neonatal or maternal infections (particularly cytomegalovirus). The Newborn Hearing Screening Programme is offered shortly after birth and aims to identify moderate, severe and profound hearing impairment. The results of this screening may be relevant in your assessment. Speech delay, educational and behavioural problems can be associated with hearing impairment. Parental and/or teacher observation and assessment may highlight problems. Parental smoking is a modifiable risk factor for glue ear and is important to ask about. Intracranial infection may complicate acute otitis media, particularly in children, so the history should look for suggestive symptoms, such as headache, drowsiness or confusion.
Examination
Examination consists in inspection of the ears and a general assessment of hearing. It may also include tuning fork testing, and an assessment of facial nerve function.
Ear examination
Examination should start with the unaffected ear with inspection of the pinna and mastoid for scars, congenital lesions and signs of infection. Then view the auditory canal and tympanic membrane using an otoscope and an appropriately sized speculum. Young children may need to be seated on a parent’s lap with their hands and head held securely to avoid injury. It is safest to hold the otoscope like a pen, as this allows the examiner to adopt a stable position bracing against the patient’s head. Gently angling the otoscope allows all portions of the tympanic membrane to be visualised. Assessment of tympanic membrane mobility, e.g. during the Valsalva manoeuvre, gives an indication of Eustachian tube patency.
Assessment of hearing
Formal audiometry is preferred, although initial hearing tests can be performed in the surgery. The examiner may use whispered voice, rubbed fingers, or a ticking watch, while masking the opposite ear (e.g. by rubbing on the tragus).
Tuning fork testing
Tuning fork tests help differentiate sensorineural and conductive causes of hearing loss. Figure 1 illustrates how to interpret these tests. For Weber’s test a 512 Hz vibrating tuning fork is placed firmly in the midline of the vertex of the skull and the patient is asked in which ear is the sound loudest. A normal test is heard equally on both sides. Sound lateralising to one side suggests an ipsilateral conductive hearing loss or a contralateral sensorineural hearing loss. Rinne’s test uses a 512 Hz vibrating tuning fork that is placed in front of the auditory canal and against the mastoid bone (firm application and counter-pressure increase accuracy). The patient is asked which is loudest. A positive and normal Rinne’s test occurs if sound is heard loudest over the ear canal (air conduction is greater than bone conduction). If the sound is loudest over the mastoid process this indicates a negative Rinne’s test, which suggests conductive hearing loss.
Rinne’s test and Weber’s test.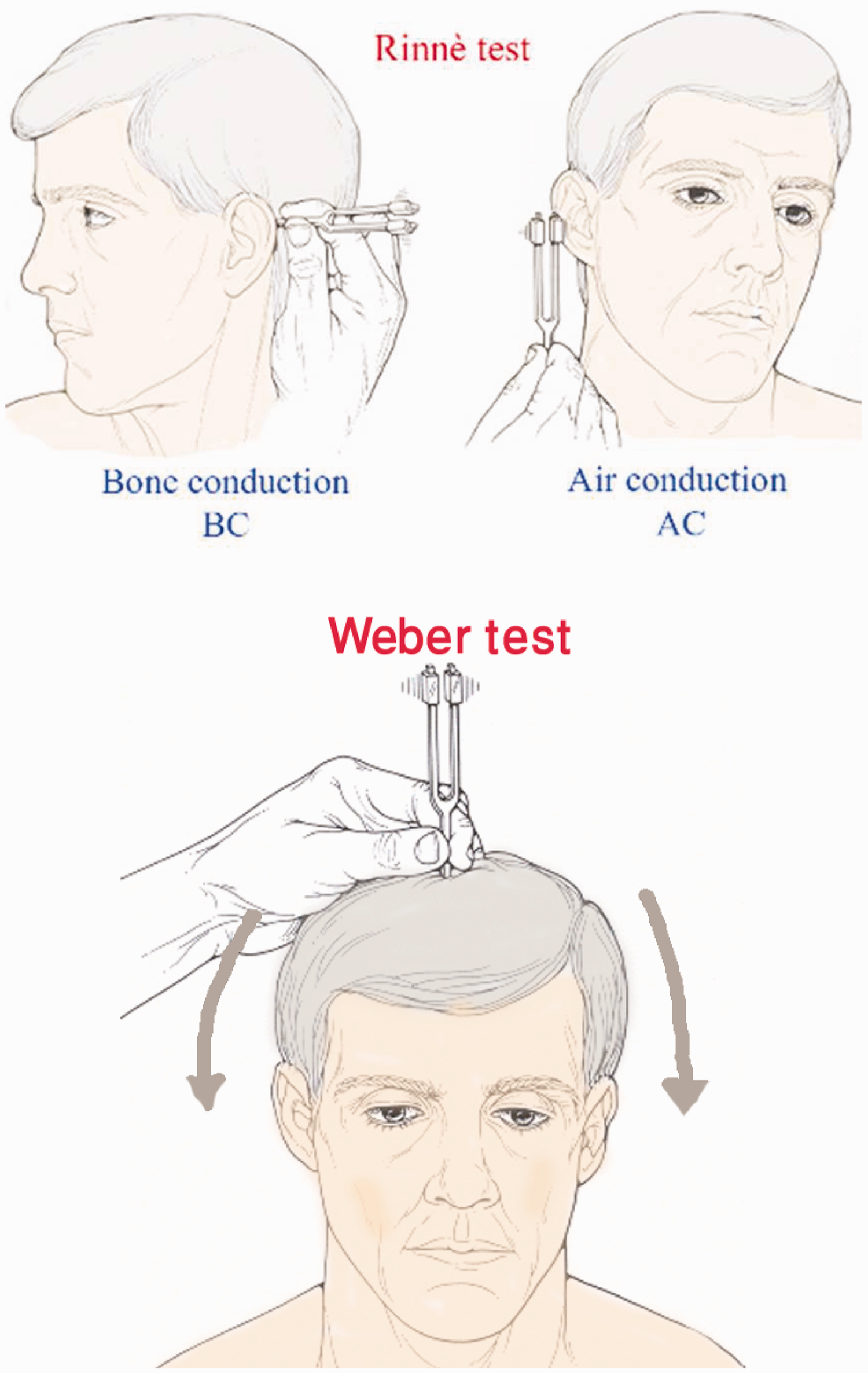
Assessing facial nerve function
An assessment of the seventh cranial nerve is important. The facial nerve’s intracranial course is in close association with the middle and inner ear. Therefore, facial nerve injury may result from diseases of the ear, such as otitis media and cholesteatoma. Acoustic neuromas may compress the facial nerve in the cerebellopontine angle. Ramsay–Hunt syndrome results when herpes zoster is reactivated in the geniculate ganglion of the facial nerve. These conditions cause a lower motor neuron lesion, with paralysis of the forehead muscles. This should be distinguished from an upper motor neuron lesion, which partially spares the forehead, and suggests an alternative cause, such as a stroke.
Investigation in primary care
Tympanometry may be available in some practices, and can be useful in aiding the diagnosis of secretory otitis media. However, the majority of investigations will require referral to secondary care. This includes pure tone audiometry, which may be accessed via audiology or via the ENT department depending on local referral pathways.
Management
Earwax
Earwax consists of a combination of dead flattened skin cells, cerumen (a wax-like substance produced by ceruminous glands), sebum and foreign substances such as cosmetics and dirt (Clinical Knowledge Summary, 2012a). Its function is to aid migration of keratin out of the ear canal and to protect the ear canal from infection. It may be wet (this can be hard or soft) or dry (most common in Asian populations), and there is variation in the amount of wax between individuals.
Wax may become impacted, which can cause a blocked ear sensation, discomfort, tinnitus, itching, vertigo or cough. Patients who produce hard wax, have narrow or hairy ear canals, or dermatological conditions affecting the ear canal are more prone to developing problems with earwax. Learning disability, advancing age and hearing aid use are also associated with an increased incidence of wax impaction, as is the use of cotton buds for cleaning the ears. (Clinical Knowledge Summary, 2012a)
Indications for removing earwax include troublesome symptoms, or a need to view the tympanic membrane for diagnostic purposes (Clinical Knowledge Summary, 2012a). There is limited good quality evidence on the best way of removing earwax in primary care. (Loveman et al., 2011) However, ear drops are often used first line and may be all that is required. Sodium bicarbonate, sodium chloride, olive oil or almond oil can be used for 3 to 5 days to soften and help remove wax. In practice, drops are often used for several weeks, and regular use may be indicated for recurrent wax.
Contraindications, cautions and warnings for ear irrigation.
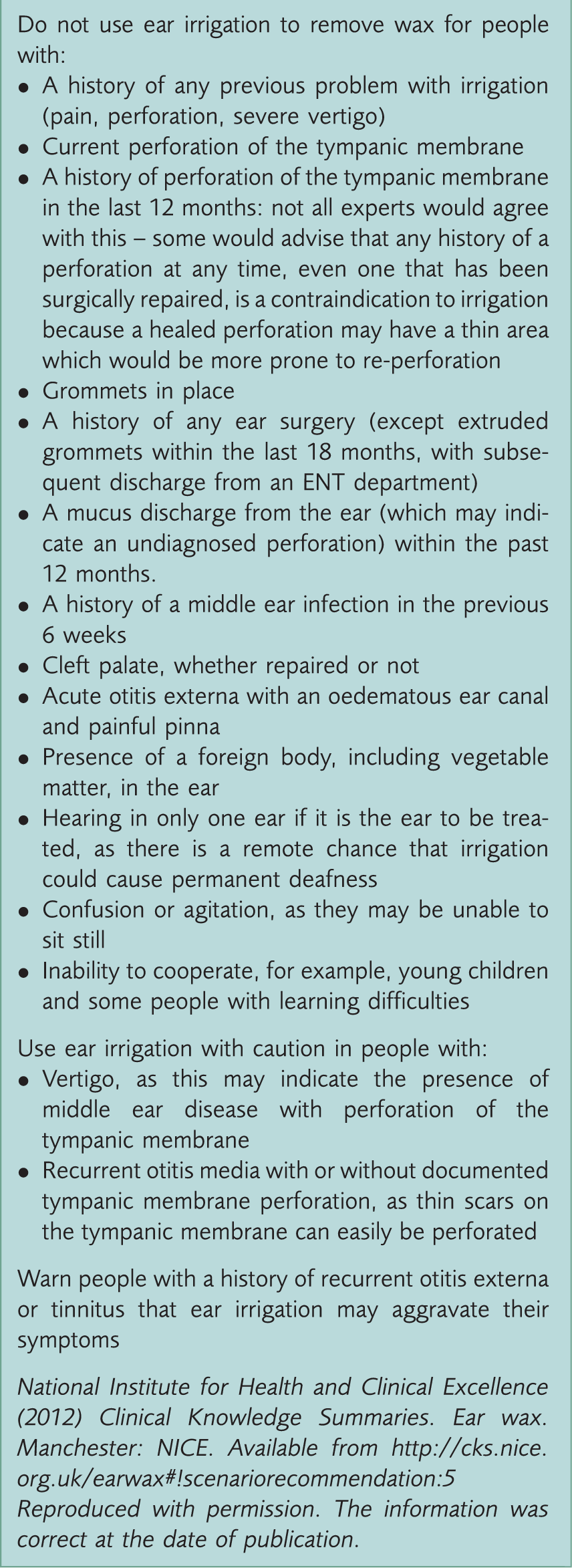
The most common problems associated with syringing are failure of wax removal, otitis externa, perforation of the tympanic membrane and trauma to the external auditory canal. Severe pain, deafness or vertigo during or following irrigation, or tympanic membrane perforation during irrigation, require an urgent ENT opinion.
Otitis externa
Otitis externa is inflammation of the external ear canal. It can be localised (as a furuncle) or diffuse, with widespread inflammation of the skin and subdermis. It is defined as acute if it has lasted less than 3 weeks and chronic if it has lasted more than 3 weeks (Clinical Knowledge Summary, 2012b). Swimming, particularly in polluted water or in humid conditions, predisposes to infection. Irritants (such as topical medications), hearing aids, and trauma (e.g. through cotton bud use or syringing), also increase the risk. Chronic skin conditions, such as dermatitis, psoriasis or eczema, are additional risk factors.
Folliculitis causes pain that is disproportionate to the size of the lesion. It is usually self-limiting and can be treated with analgesia and application of a warm compress. Oral antibiotics are only required for severe infection; for instance, if cellulitis spreads beyond the ear canal, the patient is systemically unwell, or if they are immunocompromised (Clinical Knowledge Summary, 2012b). A small pustule near the end of the ear canal may be drained by incision with a surgical needle.
Diffuse otitis externa presents with itch, discharge, hearing loss and pain brought on/exacerbated by moving the affected ear, though pain is less severe in chronic cases. Most are caused by Pseudomonas aeruginosa and investigation is rarely required, however, an ear swab may be sent for microscopy if there is no response to treatment. For mild cases with no deafness or discharge, topical acetic acid may be sufficient. More severe cases require a topical antibiotic combined with a corticosteroid. Aminoglycosides should be avoided in primary care if there is a tympanic membrane perforation, but may be used under specialist instruction (ENTUK, 2007). If there is significant debris or wax obstructing the canal the patient may require referral to ENT for microsuctioning, or wick insertion if there is extensive swelling of the auditory canal. Patients should be advised to keep the ears dry, control coexistent chronic skin conditions and avoid trauma and cotton buds to the ear canal. Fungal infection, usually caused by Aspergillus or Candida spp., may follow prolonged courses of topical antibiotics (of 3 weeks or more) and is treated with topical clotrimazole.
Necrotizing (or malignant) otitis externa is an extension of infection into the surrounding temporal bones. It is a rare but serious condition that usually arises in elderly people with diabetes. It should be suspected in this group if there is otalgia that is excessive for the signs of otitis externa. Facial nerve palsy and other cranial nerve defects may develop and strongly suggest the diagnosis. A suspicious finding is granulation tissue on the floor of the external canal, or exposed bone in the ear canal. Investigations are performed in secondary care and include inflammatory markers, radiological imaging, and sometimes biopsy and culture. Treatment is usually with intravenous antibiotics administered for several weeks.
Acute otitis media
Acute otitis media (AOM) is characterised by the presence of middle ear pus and mucosal inflammation. Infection may cause obstruction of the Eustachian tube resulting in fluid retention. It is a common problem in general practice, and is seen particularly in younger children. Passive smoking, nursery attendance, use of formula milk, Down’s syndrome, craniofacial syndromes (e.g. cleft palate), and being male are predisposing factors (Clinical Knowledge Summary, 2009a). The condition presents with earache (younger children may pull or rub their ear), fever and other non-specific symptoms including irritability, poor feeding, restlessness, cough or coryza. The tympanic membrane is red, yellow, or cloudy, and may be bulging. There may be otorrhoea if the eardrum has ruptured.
Pain and fever can be managed with paracetamol or ibuprofen. Most children do not need antibiotics, as symptoms will resolve spontaneously. However, a 5-day course of amoxicillin (erythromycin in penicillin allergy) should be given to patients who are systemically unwell or whose symptoms have lasted for 4 or more days (Clinical Knowledge Summary, 2009a). Patients at risk of complications, such as those with significant comorbidities, immunosuppression or previous cochlear implant, should also be given a prescription. Antibiotics can be considered depending on severity if there is otorrhoea, or for children under 2 years old with bilateral infection (Venekamp, Sanders, Glasziou, Del Mar, & Rovers, 2013).
Guidelines suggest that children under 3 months old with a fever of 38 ℃, and children under 6 months with a temperature of 39 ℃ and over, should be admitted to hospital (NICE, 2013). Children with suspected complications of AOM, such as mastoiditis, facial paralysis or meningitis, also require immediate referral.
Otitis media with effusion
Otitis media with effusion (OME/’glue ear’) is defined as the chronic (over 3 months) accumulation of mucous in the middle ear due to mucosal inflammation (Browning, 2008). It may occur following a middle ear infection, or be secondary to Eustachian tube dysfunction. It is the most common cause of hearing impairment in childhood with around 80% of children affected at some time before the age of 10 years (Clinical Knowledge Summary, 2011). Incidence peaks between 2 and 5 years, particularly during winter months. Risk factors include having older siblings, attending day care and parental smoking. Children with cleft palate or Down’s syndrome are at increased risk and should be regularly assessed for OME (NICE, 2008). Otoscopy may show loss of the light reflex, retraction or opacification of the ear drum, and a fluid level or bubbles. The tympanic membrane may appear straw-coloured, as shown in Fig. 2.
Otitis media with effusion.
Bilateral and persistent symptoms may lead to educational, language and behavioural problems. As most cases are self-limiting, a period of watchful waiting for 6–12 weeks to see if symptoms resolve before considering referral is appropriate (Clinical Knowledge Summary, 2011). Autoinflation devices available over the counter (Otovent device, Ear Popper) may improve effusions in some cases and are safe to try in older children (Williamson, 2011). If signs and symptoms persist the child should be referred for audiometry and tympanometry. Hearing aids are offered if there is persistent bilateral OME where surgery is contraindicated, and may be the most appropriate management option for children with Down’s syndrome or cleft palate. (NICE, 2008). Surgical management usually takes the form of myringotomy and insertion of ventilation tubes (grommets), with or without adenoidectomy (Haggard et al., 2012).
Chronic otitis media
Chronic otitis media (COM) causes inflammation of the middle ear and mastoid cavity, leading to recurrent ear discharge through a tympanic perforation. It is a painless condition, assumed to be a complication of AOM. The prevalence is less than 1% in the UK but it is common in parts of the world with overcrowding, malnutrition and limited healthcare (World Health Organisation (WHO), 2004) Symptoms supporting a diagnosis of COM are otorrhoea for more than 2 weeks without pain and fever. There may be hearing loss and usually a history of AOM, ear trauma, previous glue ear or grommet insertion. Examination is painless and shows evidence of tympanic membrane perforation.
Management involves topical antibiotics, regular microsuctioning, and topical steroids to control granuloma formation. Systemic therapy is occasionally required if there is no response to topical treatments.
Treatment in primary care is limited as there are not many GPs with the required skills and equipment to carry out aural cleaning. It is more appropriate to simply advise patients to keep the ears dry while awaiting ENT referral. Many topical antibiotics initiated by specialists are used off-licence or not recommended with tympanic perforation (Clinical Knowledge Summary, 2009b). Surgical intervention may involve myringoplasty or tympanoplasty, and patients with hearing loss persisting after resolution of COM require follow-up by audiology. Hospital admission is required for patients with signs of infection beyond the ear (postauricular swelling or tenderness, headache, facial paralysis or vertigo).
Cholesteatoma
Cholesteatoma results from keratin build-up within the middle ear. This may become infected and erode through neighbouring structures, e.g. the ossicular chain. Patients typically present with scanty, foul-smelling otorrhoea and hearing loss. More rarely they present with facial nerve palsies, vertigo or nystagmus. On examination there may be dried discharge or granulation in the external auditory canal and crusting or a polyp over the attic of the tympanic membrane. Figure 3 shows an otoscopic view of a cholesteatoma in the posterosuperior part of the pars tensa. In a patient thought to have otitis externa that is not resolving, cholesteatoma should be considered as an alternative diagnosis. The management is surgical, and aims to remove the offending tissue. Suspected cholesteatoma requires urgent referral to ENT.
Cholesteatoma.
Eustachian tube dysfunction in adults
Eustachian tube dysfunction causes conductive hearing loss with a feeling of fullness in the ear. The person may hear clicking noises on swallowing or yawning. This is usually a self-limiting problem that lasts a week or so and commonly occurs after an upper respiratory tract infection. Conservative treatment may involve the use of autoinflation devices or the Valsalva manoeuvre. Intranasal decongestants, steroids and antihistamines are frequently tried, particularly if rhinosinusitis is suspected as the precipitating factor, but there is no proven benefit (Gluth et al., 2011). Decongestant use should be limited to 7 days to reduce the risk of rhinitis medicamentosa (rebound nasal congestion). Persistent symptoms require referral to ENT to rule out a nasopharyngeal tumour, particularly if symptoms are unilateral or if there is associated nasal obstruction or epistaxis. The incidence of this malignancy is particularly high in people of Southeast Asian origin. Surgical management, once malignancy has been ruled out, may involve grommet insertion.
Ménière’s disease
Ménière’s disease is a rare idiopathic progressive disorder of the inner ear that is due to endolymphatic hydrops. It is characterised by recurrent episodes of vertigo, hearing loss, tinnitus and aural pressure sensation. The first episode usually occurs between the ages of 30 and 60 years and is most commonly unilateral, but around half progress to bilateral involvement, usually over several years. Diagnosis should be in secondary care, and requires at least two spontaneous episodes lasting 20 minutes or more with tinnitus or aural fullness, and sensorineural hearing loss confirmed by audiometry (Clinical Knowledge Summary, 2012c).
Prochlorperazine, cinnarazine, cyclizine or promethazine can be used to alleviate symptoms during an acute attack but should be discontinued as soon as possible (within a week) to promote central compensation. Patients should be encouraged to move around, although they must consider the safety of activities, such as operating heavy machinery, swimming or driving. Drivers should be advised to inform the Driver and Vehicle Licensing Agency (DVLA). People without warning symptoms generally have their licence revoked until their symptoms are under control. (DVLA, 2014).
Choice of treatment is dependent on the patient’s residual hearing, whether both ears are affected, and whether vertigo is the predominant symptom. Supportive care options include hearing aids, sound therapy or distraction techniques, and vestibular rehabilitation exercises. Prophylactic treatment with betahistine may be tried where necessary. Diuretics, local steroid injection, local gentamicin treatment or pulse pressure treatment are additional management options. Surgical interventions include grommet insertion, endolymphatic sac decompression, vestibular nerve section and labyrinthectomy.
Otosclerosis
Otosclerosis is a hereditary condition that is usually transmitted in an autosomal dominant fashion. However, the penetrance is so variable that a genetic association is not always obvious. It leads to abnormal remodelling around the otic capsule, which can result in fixation of the stapes leading to conductive hearing loss. This usually begins on one side but progresses to involve both ears in around 80% of cases (Hueb, Goycoolea, Paparella, & Oliveira, 1991). There may be associated tinnitus. Presentation is typically between teenage years and middle age, and is more common in women. Previous infection with measles and possibly the drinking of non-fluoridated water are predisposing factors. Around 0.3% of the population is diagnosed with otosclerosis, but histological evidence of the condition is present in a much higher proportion (Declau et al., 2007). Otoscopy is usually normal but the ear drum may have a ‘flamingo pink blush’ due to the underlying otospongiosis of the basal turn of the cochlea (Schwartz sign). Medical management is with fluoride therapy, and the use of hearing aids (Warner, Burgess, Patel, Martinez-Devesa, & Corbridge, 2009). Stapedotomy is an alternative or can be used in addition to hearing aids.
Sudden sensorineural hearing loss
Sudden sensorineural hearing loss occurs as a rapid loss of hearing that is usually unilateral and develops over a period of less than 72 hours. Most cases are idiopathic, and typically occur in middle age. Prognosis depends on the severity of hearing loss with around half of people recovering some or all of their hearing within 2 weeks. It is a medical emergency that should be distinguished from conductive hearing loss using tuning fork testing. The diagnosis is confirmed on the basis of pure tone audiometry. The evidence for corticosteroid therapy is unclear but treatment with prednisolone 1 mg/kg/day (up to a maximum daily dose of 60 mg) is generally recommended (Crane, Camilon, Nguyen, & Meyer, 2014; Wei, Stathopolous, & O’Leary, 2013). If the diagnosis is suspected the GP should start steroid treatment (within 2 days of onset), while the patient is awaiting ENT review. Intratympanic steroids may be offered in secondary care if there is failure of initial management (Conlin & Parnes, 2007).
Key points
A sensation of blocked ears is common and is usually caused by earwax Most causes of a blocked ear sensation can be managed in primary care GPs should be aware of the indications, contraindications and complications of ear irrigation GPs should recognise red flag symptoms and signs that may suggest cholesteatoma, malignancy, necrotizing otitis externa or intracranial complications of otitis media GPs should be aware of sensorineural hearing loss as a cause of a blocked ears sensation, and manage this as an emergency