
Abstract
It is common in primary care to see people presenting with symptoms secondary to allergy, which could range from minor rashes or rhinitis to life-threatening anaphylaxis. The skin is the largest human organ, and it is involved in allergy; through both direct exposure to the allergens and manifestations of the allergic reaction. The aim of this article is to improve understanding of skin allergy and provide an outline on how to investigate and manage allergic skin conditions.
The GP curriculum and allergies and the skin
Recognise emergency skin conditions, e.g. anaphylaxis, and act appropriately Understand the different indications for patch and prick testing, and when these are appropriate Understand the effect of a patient’s environment/occupation on skin conditions
Types of hypersensitivity reactions.
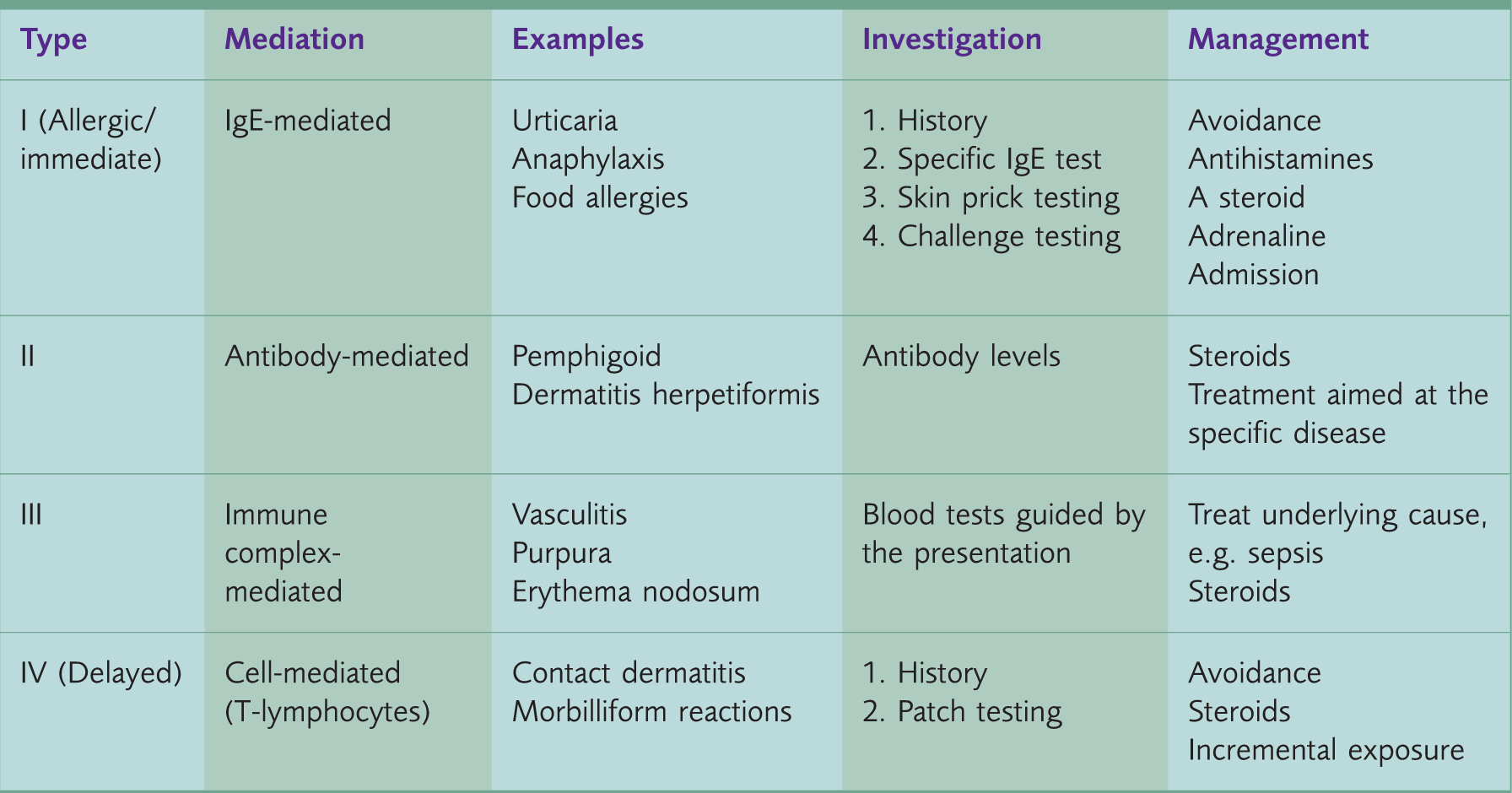
A type I hypersensitivity reaction is also known as an immediate hypersensitivity or an allergic reaction. It is mediated by immunoglobulin E (IgE), in response to exposure to allergens via inhalation, ingestion or direct skin contact. Type II and type III reactions are immune-mediated and usually have other systemic effects along with skin involvement. Type IV reactions tend to be delayed and are cell-mediated.
Allergy
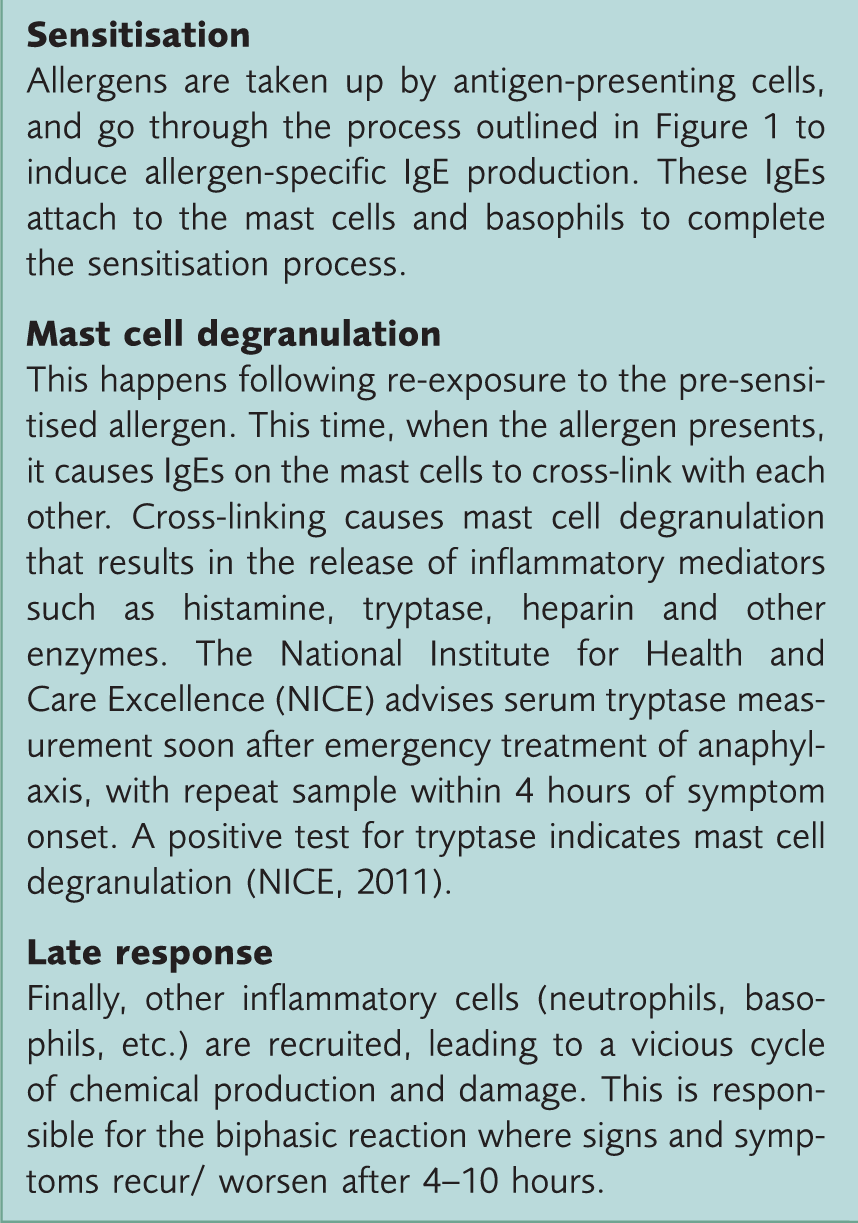
The three phases of an allergic reaction.
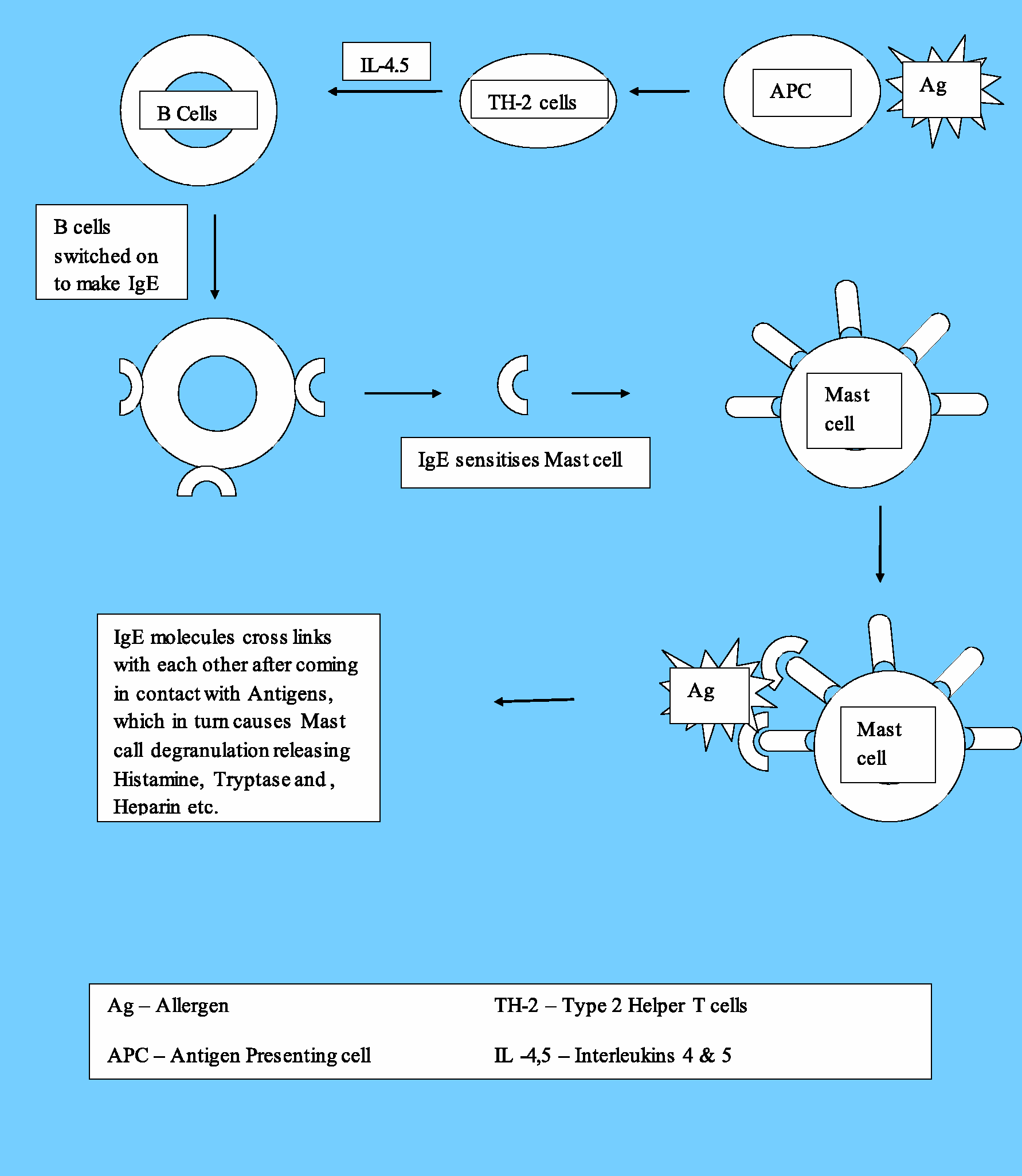
Mechanism of IgE-mediated hypersensitivity.
Assessment in primary care
History
A detailed skin history can provide enough information to enable a diagnosis and subsequent guided management. Symptoms of skin allergy can include itching, burning or soreness. It is important to note the location of the symptoms (and rash if there is one), and particularly whether the rash is symmetric and/or associated with contact of a suspected allergen. If a cause is suspected, it is useful to know the time elapsed between contact with the potential allergen and onset of symptoms. It is also important to record the duration of the rash and whether it is episodic, and to establish whether there are any relevant associated symptoms such as wheeze or breathing difficulty. An occupational history is important, particularly if a trigger related to the patient’s work is suspected.
Examination
Examination of the skin should determine whether there is any persistent rash. If there are clinical findings you should determine what level of the skin structure is affected. Scale or lichenification would suggest epidermal involvement. Weals may suggest dermal histamine infiltration.
Investigation
Most skin conditions discussed in the latter part of this article do not require tests and are a clinical diagnosis. Depending on clinical presentation, occasionally blood tests (e.g. specific Ig-E or tryptase) may be done.
Management
Patients with mild symptoms can be assessed and managed within primary care. Where there is diagnostic doubt, or potential multiple food allergies, patients should be routinely referred to a dermatologist or allergy clinic depending on local protocols. Patients with severe symptoms, particularly those suggestive of anaphylaxis, should be managed within a hospital setting. If the patient has symptoms, then immediate referral to the emergency department may be needed; if there is a history of an anaphylactic-type reaction that has now resolved, an urgent allergy clinic referral is indicated with appropriate safety netting to ensure that the patient (and/or carers) know what to do should symptoms return before the patient has been seen.
Clinical conditions
Urticaria
Urticaria is common, affecting one in six people at some point in their life and accounting for 50% of the total skin manifestations of allergic reactions. Therefore, it is important that GPs are familiar with it. Urticaria can be associated with other signs of allergy, for example, one study, which was based in an out-patients department, found one-third of cases have some degree of angio-oedema associated with urticaria (Nettis et al., 2003).
The ‘weal’ is the characteristic lesion of urticaria. Weals are raised and swollen; they are associated with profound itchiness, and each individual weal usually lasts less than 24 hours. Patients are increasingly using digital photography to record rashes that evolve and resolve before their encounter with their doctor. This can provide helpful information.
The weal, once cleared, leaves normal skin behind. Thus, any lesion lasting for longer than 24 hours, or any abnormal or flaky skin after the rash has cleared, should raise the possibility of some other diagnosis. Urticarial vasculitis and deep physical urticaria, for example, can last for more than 48 hours and are usually associated with other systemic features.
There are numerous causes of urticaria with allergy being only one of them. Causes are usually classified as follows (Grattan & Humphreys, 2007):
Ordinary urticaria: This is further divided into acute (of less than 6 weeks duration), chronic (continuously present for more than 6 weeks) and episodic urticaria Physical urticaria: Reproduced by the same stimuli, e.g. secondary to thermal or mechanical stimuli Angio-oedema without weals, e.g. drug-induced angio-oedema or C1 esterase inhibitor deficiency Contact urticaria secondary to allergens/chemicals Urticarial vasculitis Auto-inflammatory syndromes
Diagnosis of urticaria is mainly clinical. Most urticarias are mild, self-limiting and do not need to be investigated. Severe reactions involving mouth, throat or airways should be investigated. Careful history taking is most important and in some cases helps to establish the allergen. Specific IgE tests and skin prick testing can be used to confirm an allergic reaction. Tests should be guided by the history and interpreted in clinical context.
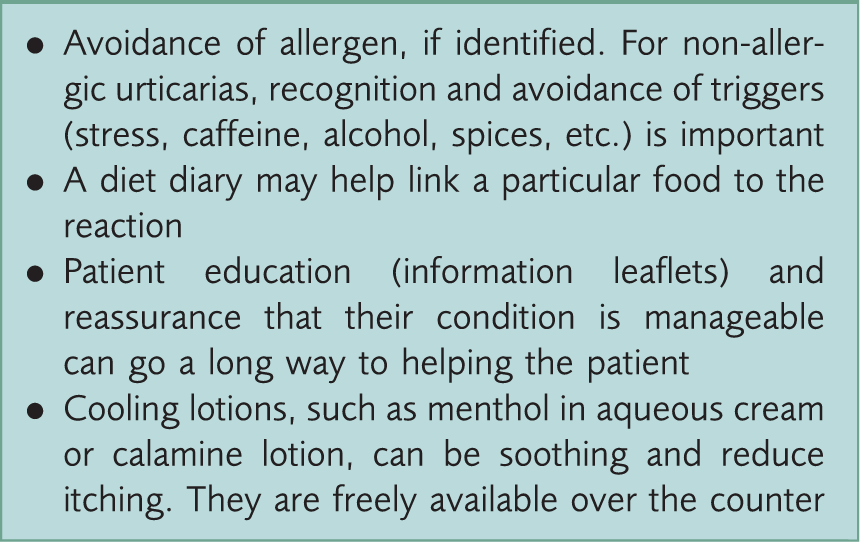
General measures for an allergy.
Medical management of urticaria.
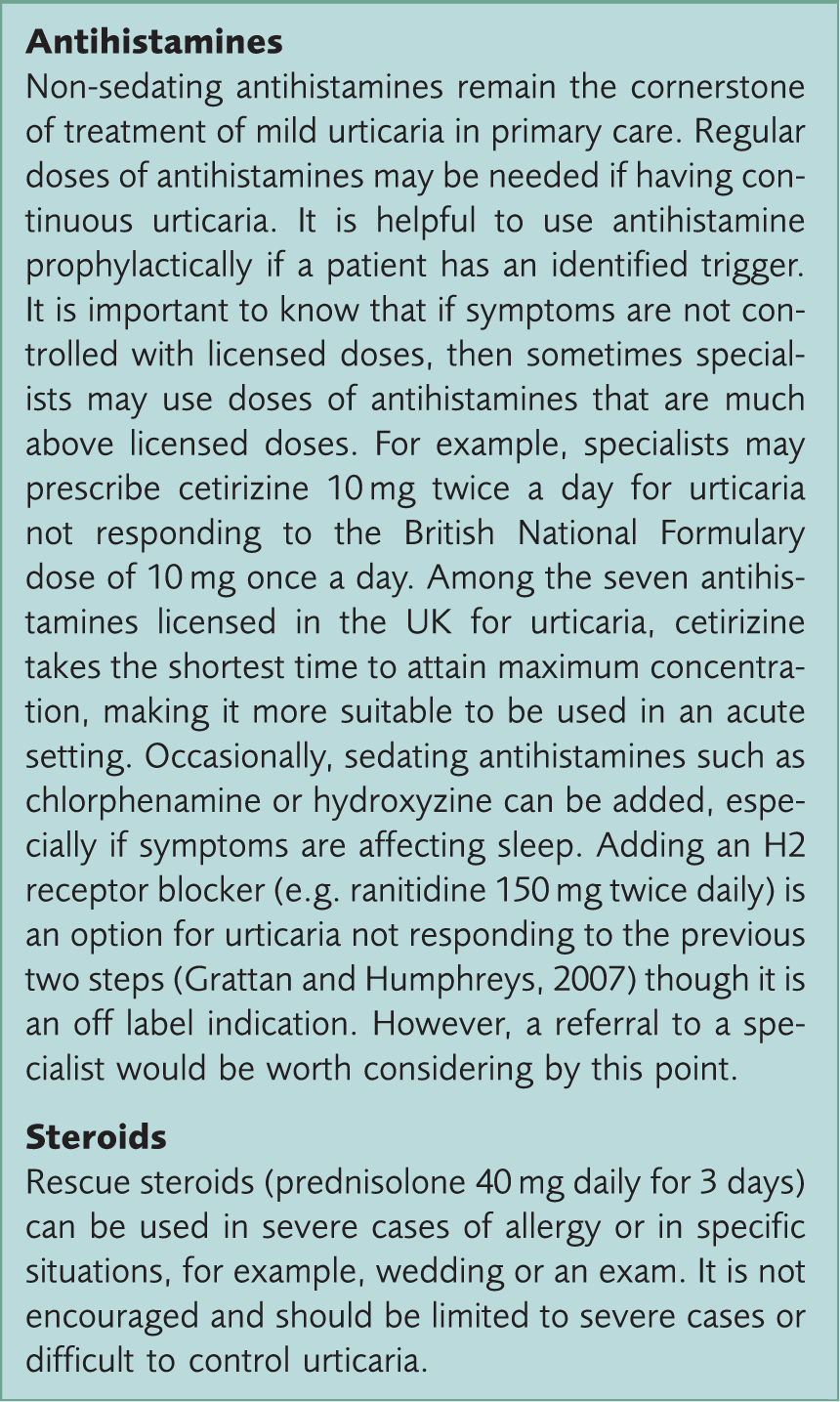
Angio-oedema
Angio-oedema is a deeper swelling that can last up to 72 hours and can affect mucosal surfaces such as lips, mouth, tongue and genitalia. Occasionally, it may affect the gastrointestinal tract (causing abdominal pain, diarrhea, and vomiting) or, the respiratory tract (causing breathlessness, wheeze, and stridor). As it involves the dermis and subcutis, the oedema can be deeper and more extensive. Angio-oedema can present with or without urticaria. In the event of airway compromise or circulatory collapse, treat it like anaphylaxis (see the next section). Otherwise, angio-oedema should be treated with anti-histamines, steroids and admission for observation (NICE, 2012).
Anaphylaxis
Management of anaphylaxis in primary care.
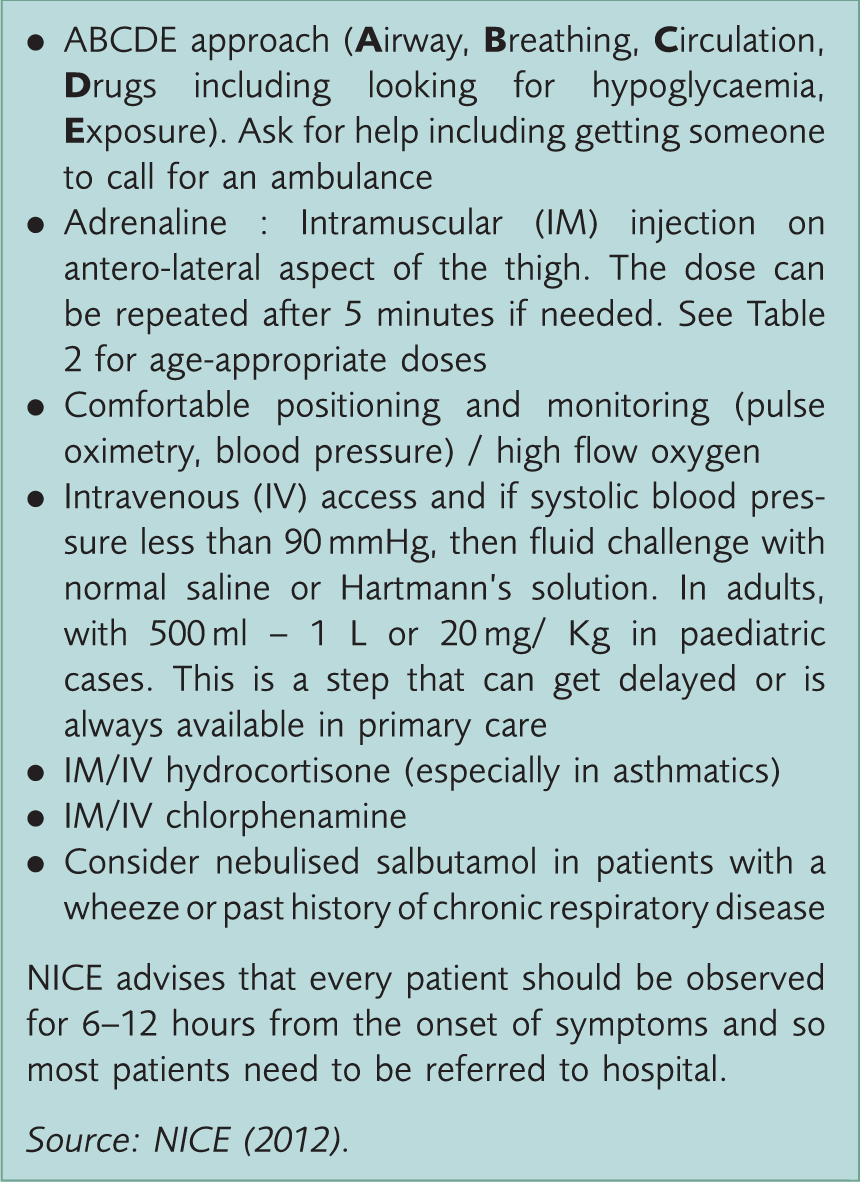
Age-appropriate doses of medicine used in anaphylaxis management.
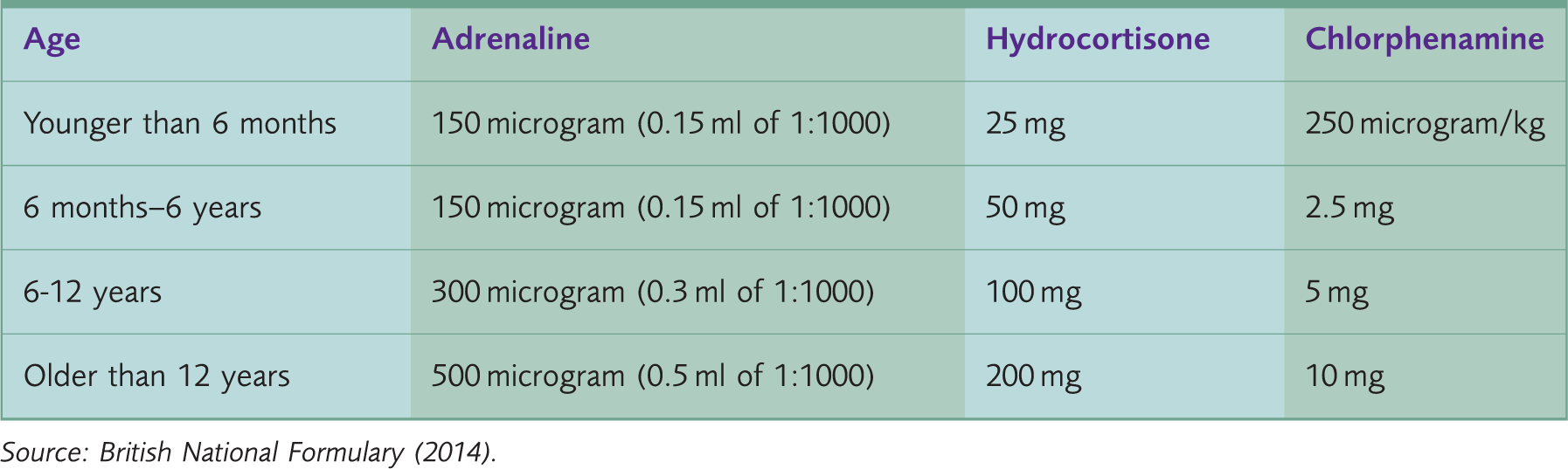
Source: British National Formulary (2014) .
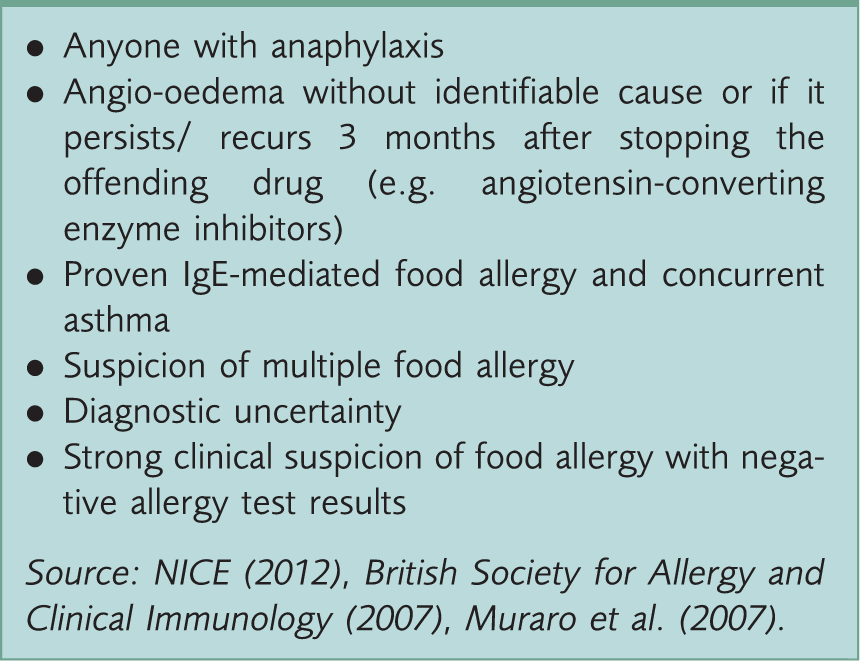
Who should be referred to an allergy clinic?
Who should be prescribed an adrenaline auto-injector device?
An adrenaline auto-injector device should be prescribed to anyone who has experienced an anaphylactic reaction on the advice of an immunologist or an allergist. A specialist may also consider prescribing for those who are at high risk of complications, for example, a child with severe food allergy and co-existent uncontrolled asthma. Patients should have enough auto-injectors to accommodate their lifestyle. In children this would include having a suitable supply of devices both at school and at home. Many patients need a repeat dose of adrenaline within 5 to 15 minutes of the initial dose or later due to delayed reaction. Therefore, it is good practice to prescribe two devices to be kept in each location that the patient usually frequents (e.g. two for home, two for work and two in the car). It is important to note that auto-injectors have a limited shelf-life and should be replaced before their expiry date regardless of whether they have been used.
Injection technique is device-specific and patient training can be undertaken in primary care, in the allergy clinic, or sometimes by school nurses. All those who are likely to be required to administer adrenaline to the patient should have training. This may involve patients, carers, other family members, school teachers and/or work colleagues as appropriate.
Mimics of allergic reactions
Morbilliform drug rash
A morbilliform rash is a measles-like rash (see Fig. 2) and it is the most common drug rash referred to secondary care. It is a type of delayed hypersensitivity reaction, mediated by type 2 T-helper cells, and is classified as a IV b hypersensitivity reaction. The rash is treated by stopping the offending drug and recording the response. Reassurance and watchful waiting is all that is usually required, however, in severe cases a 3 to 5 day course of oral steroids may be needed. Of note, giving antihistamines is not effective as mast cells (and thus histamine) are not involved in the causation of this type of rash.
Morbilliform rash.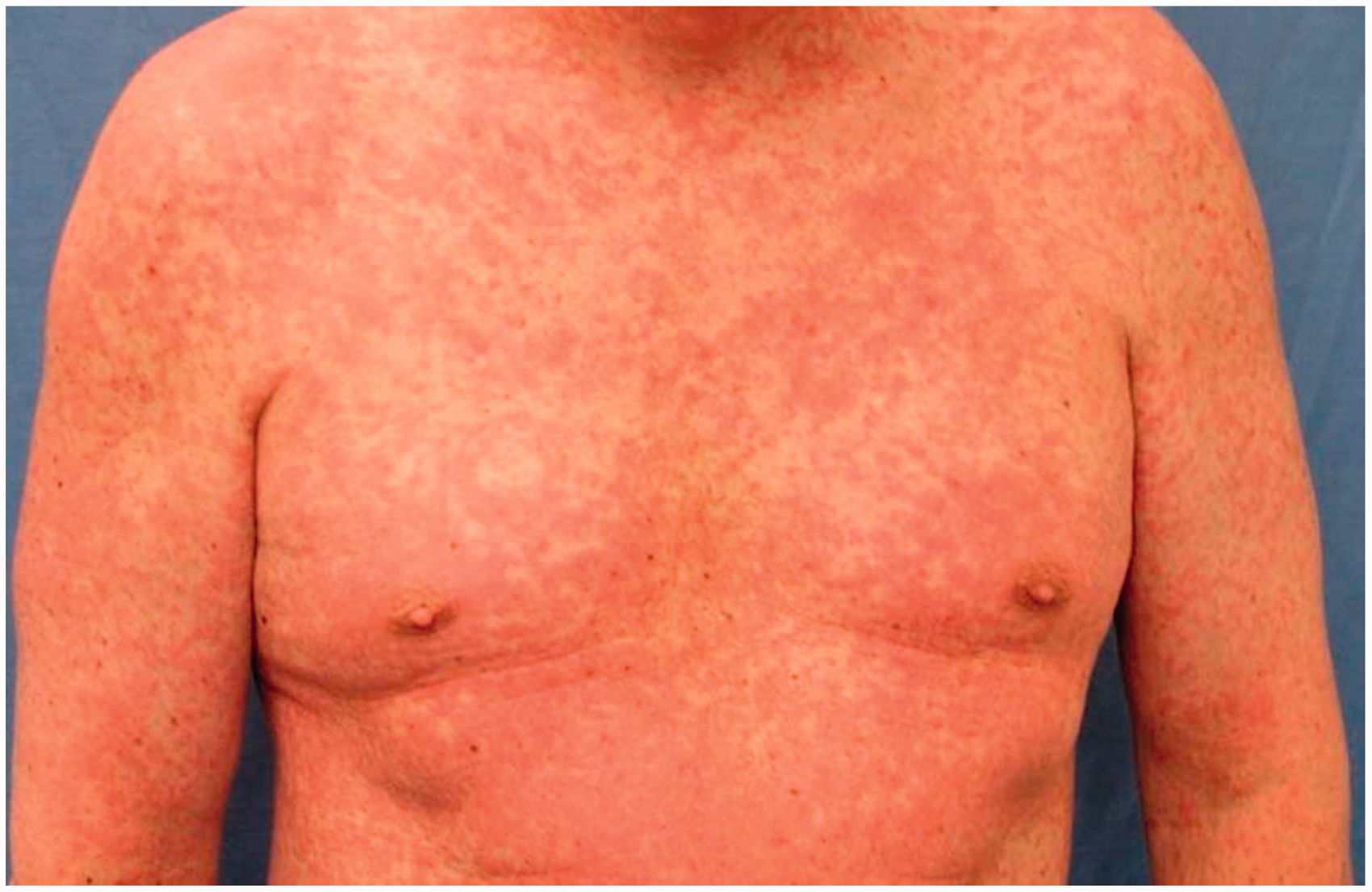
It is always important to record drug reactions on a patient’s notes to ensure that the drug is not prescribed again to the same patient. Drug reactions are classified into:
Type A reactions: These are common and relate to the pharmacology of the drug (e.g. constipation with opioids), and Type B reactions: Rare, indiosyncratic and unpredictable reactions that are often serious
Type A accounts for almost 80% of drug reactions presenting to the health professional. These can in many instances be incorrectly recorded as an allergy, but should be labelled as intolerance rather than allergies, unless they caused angio-oedema or anaphylaxis.
Pseudo-allergic reaction
Conditions that can cause direct mast cell activation (without involvement of IgE) are called ‘pseudo-allergies’. Their clinical presentation is similar to allergic reactions, as they too release the same inflammatory chemicals after mast cell degranulation. Presentation can vary from mild urticarial symptoms to anaphylaxis. Common examples are urticaria pigmentosa (cutaneous mastocytosis) and drug-induced urticaria (e.g. codeine).
The clinical significance of understanding pseudo-allergies lies in the fact that blood tests for IgE and skin prick testing will yield a negative reaction. Also, unlike allergic reactions they do not need sensitisation and can occur even after first exposure. If the reaction is severe enough to cause anaphylaxis it is termed an ‘anaphylactoid reaction’. Management depends on the clinical presentation, with cutaneous involvement responding well to antihistamines. Mast cell stabilisers, e.g. sodium chromoglycate can be helpful in cutaneous mastocytosis. Steroids are not as effective, due to the lack of Ig-E involvement in the pathogenesis. Adrenaline is the main stay of treatment of anaphylactoid reactions and they should be treated in the hospital setting.
Atopic eczema
Sometimes, a parent may bring a child to the GP with worsening eczema, wondering if it is due to an allergy. ‘Atopy’ indicates a genetic susceptibility to the development of allergic diseases (one or more of the triad of asthma, allergic rhinitis, and eczema) in response to environmental factors such as irritants or allergens.
Atopic eczema has shown to symptomatically worsen due to food allergy in 10% children, but less so in adults. Some people with atopic dermatitis have been found to have excessive levels of IgE and eosinophils. That along with a reduced barrier function of skin, which makes it easier for the allergens to penetrate skin, makes them more prone to allergy.
Investigation is usually not needed. Frequent and liberal use of emollients to restore skin barrier function is the most important part of management. Patient education regarding the condition, use of soap substitutes and at least twice daily use of a moisturising cream (cosmetically more acceptable), or ointment (greasy but more effective) helps with compliance and better management. Patient.co.uk and British Association of Dermatologists have good web-based patient information leaflets.
Allergic contact dermatitis
Differences between allergic and irritant dermatitis.
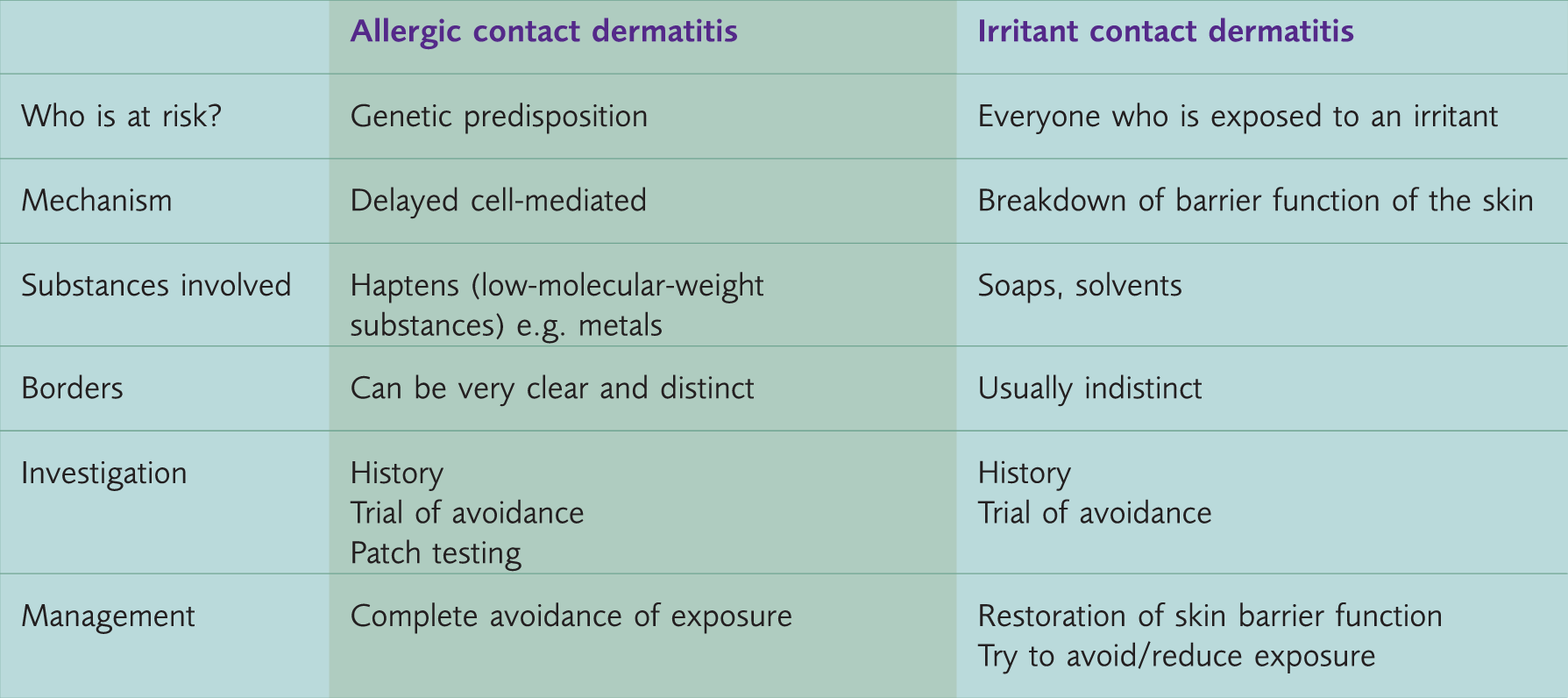
Allergic contact dermatitis is a type IV delayed hypersensitivity reaction. The allergen is taken up by the skin macrophages (Langerhans cells) and processed into smaller peptides, which in turn are presented to lymphocytes. Interleukins are released, which activate antigen-specific memory T-cells. These memory T-cells are multiplied and release cytotoxic chemicals when re-exposed to the allergens.
Contact dermatitis needs sensitisation by prior exposure before a response with dermatitis can be seen. It typically presents as redness, itching, swelling, scaling and sometimes weeping lesions.
Think of contact dermatitis in patients presenting with the following symptoms and signs (Burge and Wallis, 2012):
Hand dermatitis (though up to 70–80% of cases are caused by irritant contact dermatitis) Chronic leg ulcers not responding to usual treatment Treatment-resistant facial dermatitis Pruritis ani (especially when a few creams have already been used).
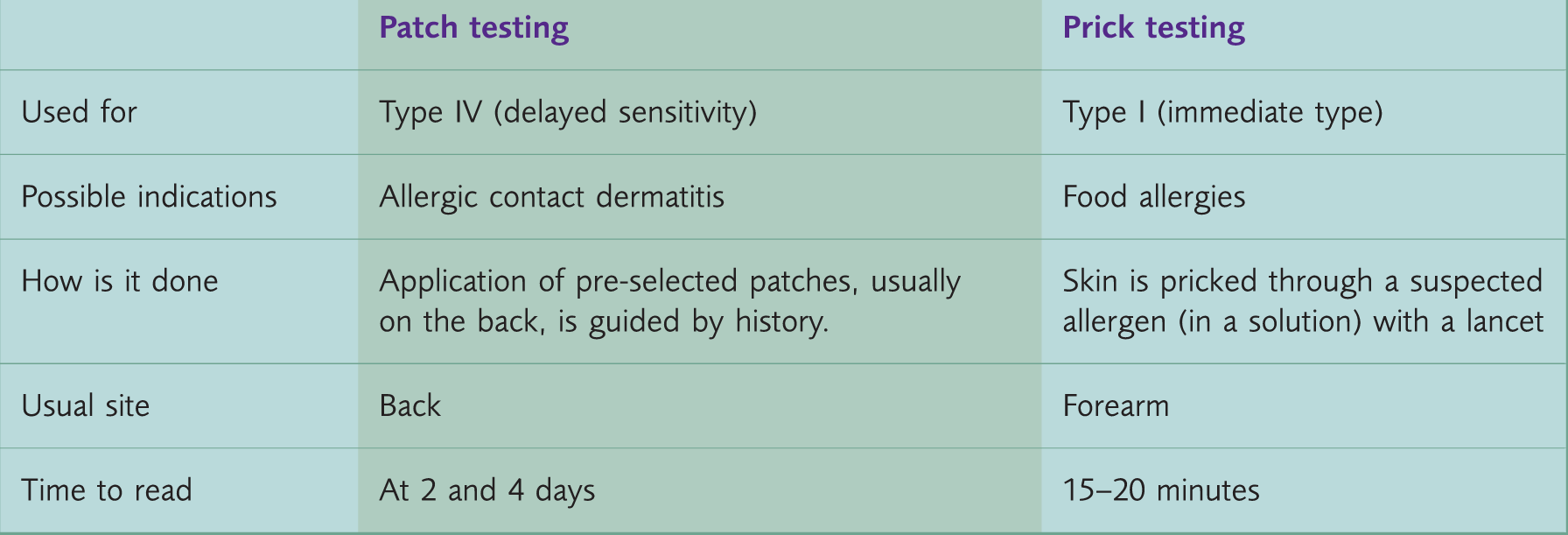
Patch and skin prick testing.
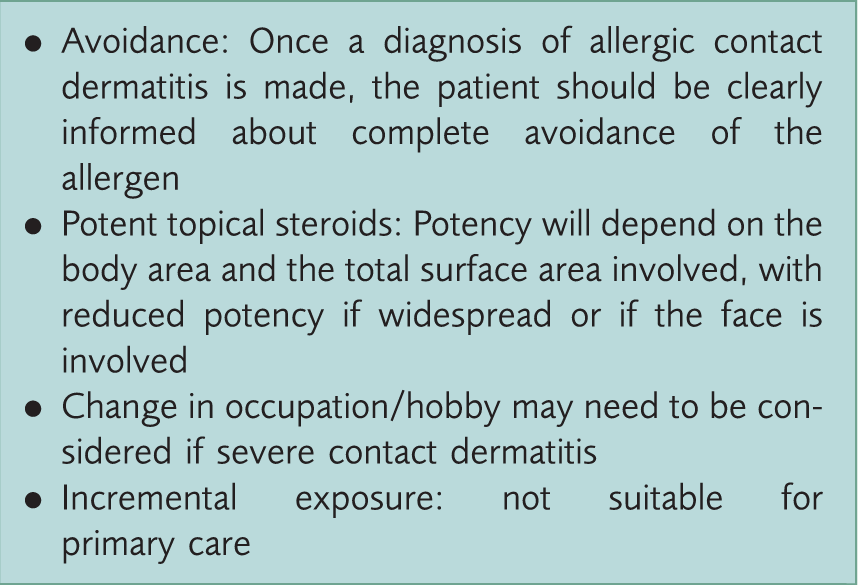
Management of allergic contact dermatitis.
Key points
Skin-related problems due to allergy are common in primary care History is the most important step in ascertaining allergy Think IgE or skin prick testing for food allergy and patch testing for contact dermatitis Avoidance of the allergen once identified is vital Reduced skin barrier function in atopic dermatitis may make people prone to allergy Be aware of anaphylaxis and its management algorithm
Footnotes
Acknowledgement
The author would like to thank Dr Joy Wright for her help with the writing of this article under the InnovAiT ‘buddy’ scheme and Dr Janis Tait and Dr Peter Kelly for proof reading this paper.