
Abstract
The Care Quality Commission (CQC) is the independent regulator of health and adult social care in England. It has a statutory duty to monitor and inspect providers of health services including General Practices. Since 1 October 2014, the CQC has rolled out its new approach to inspecting GP services. The aim of this article is to outline the CQC’s role in regulation and the rationale for and mechanism by which it carries out its regulatory activities.
The GP curriculum and the Care Quality Commission
Contextual statements in the GP curriculum list the learning outcomes that relate to quality improvement, patient safety and medical leadership skills.
Build and enhance the safety culture in your general practice setting including attending meetings Understand principles of improvement methodology to facilitate change
Gather and analyse information about organisational performance Participate in taking action to improve organisational performance Place your patients at the centre of decisions about services
Develop medical leadership skills alongside clinical and research skills to enable safer working systems
What is the Care Quality Commission?
The Care Quality Commission (CQC) is the independent regulator of health and adult social care in England. Its purpose is to ensure that health and social care services provide people with safe, effective, compassionate, high-quality care (CQC, 2014a). The Health and Social Care Act 2008 established the organisation; it is accountable to the public, Parliament and the Secretary of State (CQC, 2014b).
In the aftermath of the Francis Report, the CQC changed its approach to regulation, shifting from being regulations-focused to assessing care quality in a more holistic way. In order to do this, we now ask five key questions when assessing providers: Is the service safe? Is it effective? Is it caring? Is it responsive to peoples’ needs? And is it well-led?
As part of this cultural shift in the way we regulate, we aim to highlight areas of ‘Outstanding’ practice as well as areas where practice is ‘Inadequate’ or ‘Requires Improvement’. We want to celebrate good practice, however, there are a small number of practices that provide very poor care and this is unacceptable for the both the profession and the public. By rating health and care providers in this way, we aim to be ‘agents for improvement’ by encouraging services to improve their standards (CQC, 2014c).
How does the CQC’s work fit within the wider regulatory environment?
The CQC is one of several key regulatory bodies in the English health sector. We work closely with other organisations such as Monitor, the General Medical Council (GMC) and NHS England to ensure that services are of high quality. It is common for clinicians to question CQC’s role in primary care, given that GPs are already regulated as individuals by the GMC. However, we know from experience that there is an important role for the regulator of organisations – after all, good doctors can often work in dysfunctional organisations where patient care is adversely affected in spite of clinicians’ best efforts. The GMC, through the revalidation process, assures the profession and the public that doctors are up to date and fit to practise (GMC, 2014). The CQC needs to be assured that the doctors working in an organisation are fit for the purpose of delivering care in that organisation.
What is CQC’s role in regulating general practice?
The CQC has a statutory obligation to register and inspect all providers of healthcare in England, including general practices. We know from a range of data sources and the experiences of patients and clinical colleagues, that there is substantial variation in the quality of general practice across the country. Given this variation in quality and our legal and ethical duties to protect patients, the CQC started to inspect general practice surgeries in April 2013. These first inspections were compliance-focused and involved a single inspector assessing practices against the Regulations laid out in the Health and Social Care Act 2008 (CQC, 2010). Although these inspections were successful at identifying areas of poor compliance with the Regulations, we found that providers felt that this approach did not adequately recognise areas of excellent practice, and there was informal feedback from GPs concerned about a lack of clinical peer-review.
To address these issues, we started piloting our new inspection methodology in April 2014. This pilot phase involved 356 practices from across the country. This pilot phase ended in September 2014, and as of 1 October 2014, we have rolled out our new approach across the country. We aim to inspect all 8322 general practice surgeries in England by April 2016, including undertaking any follow-up visits or reactive inspections relating to specific concerns or whistleblowing.
CQC also inspects GP out-of-hours services, dentists, NHS 111 services, and urgent care providers. We are currently developing our approach to regulating these services and aim to have inspected all of these providers across the country by April 2016.
Methods: How does the CQC regulate general practice?
The process of regulating health and adult social care providers has four key elements:
Registration Intelligent monitoring Expert inspection, and Publication of reports including ratings (see Fig. 1). CQC’s regulatory approach.

Registration
All providers of health and social care in England must be registered with the CQC. Registration is the way providers tell CQC the following key information:
What type of provider they are – e.g. Partnership, Limited Liability Partnership, sole-trader What ‘regulated activities’ they offer (e.g. diagnostics and screening, treatment of disease, disorder or injury, surgical procedures, family planning services, maternity and midwifery services) The location of their service The name of the registered manager and nominated individual (the people who take responsibility for the regulated activities) The statement of purpose of the organisation (the organisation’s aims and vision for delivering high-quality care)
This information helps CQC know where care is provided and who is taking responsibility for doing so. It forms the basic foundation for us to focus our ‘intelligent monitoring’ and inspection upon.
Intelligent monitoring
Intelligent monitoring is the process of using data and other information to inform where CQC prioritises for inspection. For general practice we use a range of indicators including:
Quality and Outcomes Framework performance GP Patient Satisfaction Survey responses Electronic Prescribing Analysis and Costs Hospital episode statistics The Information Centre Indicator Portal (an online hub for a range of national data indicators collected by the Health and Social Care Information Centre), and NHS Comparators (an analytical service for commissioners and providers, it benchmarks and compares activity and costs on a local, regional and national level)
Based on the intelligent monitoring data, we categorise practices into six priority bands based on the risk of patients not receiving safe, effective, high-quality care – with Band 1 being the highest risk and Band 6 the lowest (CQC, 2014d).
It is important to stress that although intelligent monitoring information may raise questions about the quality and safety of care, it is not used on its own to make judgements – this information must be corroborated with findings from the inspection. The data is used for discussion with the practice during the inspection to inform the key lines of enquiry. The judgment is then made after the inspection.
Expert-led inspection
Expert-led inspections are a cornerstone to the CQC’s regulatory method. We have adopted a more peer-review approach to inspections than ever before. For the first time, GP specialist advisors accompany our Inspectors during every visit and provide clinical input and guidance for the team. The teams performing the inspection are also larger – previous inspection teams comprised solely of one (or occasionally two) inspectors. Now each team always contains an inspector and a GP specialist advisor and may also include a practice nurse, practice manager or ‘expert by experience’. These ‘experts by experience’ are members of the public who have had substantial experience of using services. They provide a unique opportunity to bring the patient perspective to the heart of the inspection process.
During the visit, our inspectors ask the five key questions mentioned earlier – are services safe, effective, caring, responsive to peoples’ needs and well-led? In order to answer these questions in a consistent way, inspectors follow a ‘key line of enquiry’ (KLOE) approach, which is published in our Provider Handbook (CQC, 2014e) and appendices (CQC, 2014f). The KLOEs provide more detailed sub-questions in a particular topic area – for example, under ‘Safe’ our first KLOE is ‘What is the track record on safety?’ and our second KLOE is ‘Are lessons learned and improvements made when things go wrong?’ We have published all these KLOEs so that providers know what to expect when the inspection team arrives and can prepare accordingly.
We also look at care through the lens of six population groups, again answering the five key questions each time. These population groups are: older people; people with long-term conditions; families, children and young people; working age people, students and those early retired; people in vulnerable circumstances and people experiencing poor mental health and dementia.
Typically a visit takes a day, although if the practice is very large or has significant problems then it may last 2 days. It starts with an opportunity for the practice team to discuss the history and context of the practice and present to the inspection team what things the practice does well, as well as describing some of the key challenges for the future. The inspection team will typically go on to talk to members of staff – doctors, nurses and administrative staff, as well as patients about their views and experience of the practice. They will ask for evidence to answer the KLOEs, which may be in the form of documents such as policies and minutes from meetings or oral statements. The day finishes with a brief period of feedback to the provider about the headline findings.
Ratings
Following the inspection, our team review the evidence collected on the day and information from the intelligent monitoring. Practices are then rated for each key question on a four-point rating scale – Outstanding, Good, Requires Improvement and Inadequate (see Fig. 2). These ratings across the five key questions and population groups are then aggregated into one overall rating for the practice.
Flow diagram illustrating how CQC decides upon ratings for services.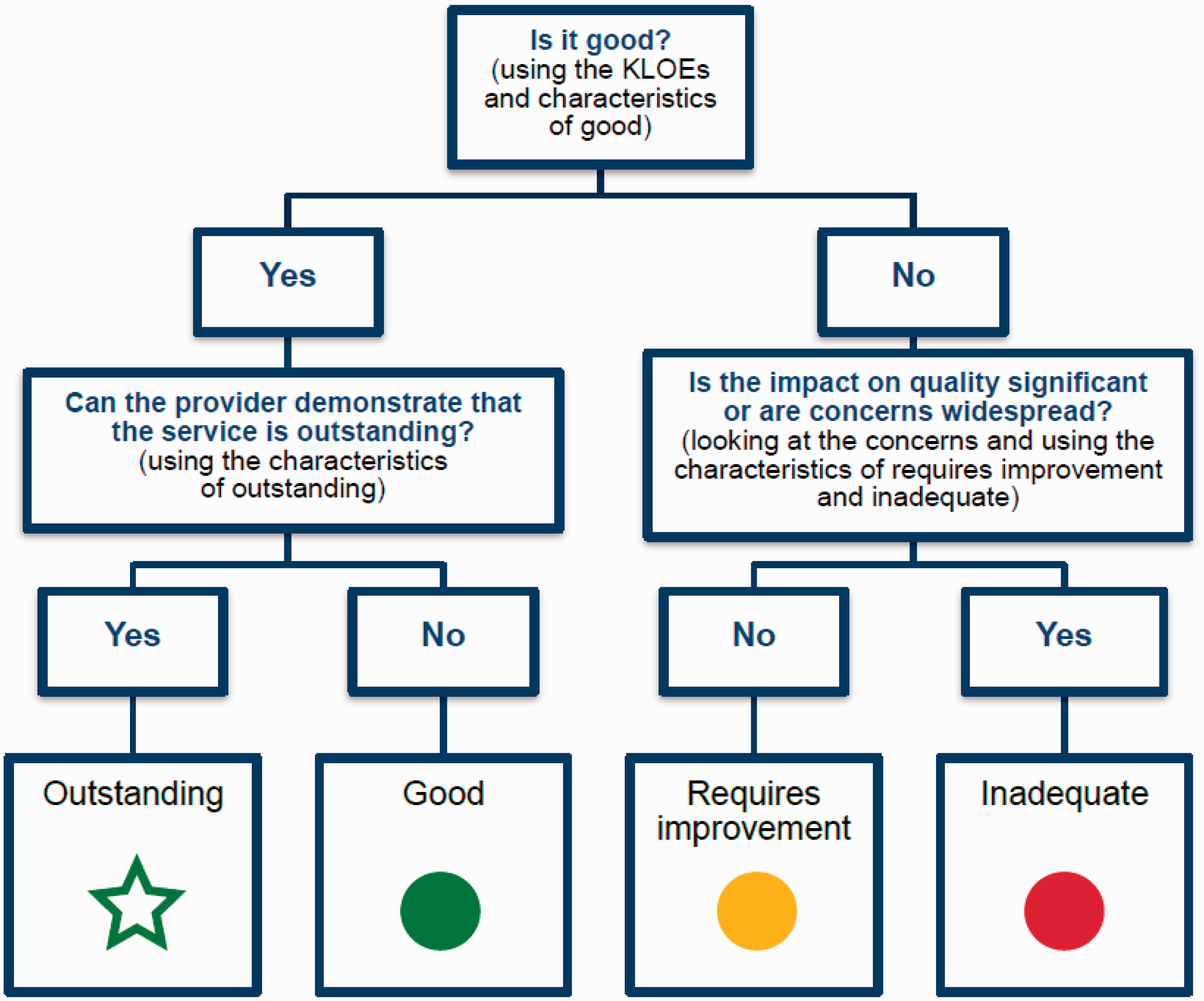
By publishing ratings we encourage practices to improve their services. It is also the mechanism by which we can highlight excellent healthcare as well as shining a spotlight on poor practice.
Quality assurance
Ensuring a robust and consistent process of inspection is paramount to regulating effectively and credibly in the eyes of the public and providers. The CQC has a substantial quality assurance process to ensure that our judgements are accurate and fair. Inspectors share their reports with colleagues for peer-review at an early stage, before being checked by an inspection manager. A regional quality panel then reviews all the reports from a particular area to ensure consistency of ratings, a further national panel then does a further check for consistency country-wide. These national panel reviews also review ‘Outstanding’ reports as well as ones that highlight ‘Inadequate’ practices that may need to be placed in ‘special measures’.
Special measures
The special measures system is used by CQC in conjunction with NHS England to issue deadlines for providers of ‘Inadequate’ care to improve or face closure. As part of the special measures programme, providers are offered additional support and resources from NHS England’s Area Team in order to help them improve. However, if after a further inspection there is no improvement in care, the CQC may deregister the practice or NHS England may revoke their contract to provide services or both (CQC, 2014g).
What have we found so far?
By early December we will have published all of our pilot phase reports and a small number from the full roll out of the new methodology. More reports are on their way, as we shall soon be publishing 50–70 reports per week.
Overall the findings have been positive. The majority of practices are offering high-quality primary care to their communities. We have identified numerous areas of outstanding practice; commonly, these are examples of effective multidisciplinary working for elderly and palliative care patients, or offering proactive services for those at risk of diabetes.
However, the variation in general practice remains significant, and the findings from our inspections support this point. Common areas for improvement are the processes of staff recruitment, safety culture and medicines management.
Conclusions
The CQC can be a powerful agent for improvement. By publishing ratings we encourage practices to improve, and by sharing examples of good practice and poor practice we help spread innovation and prevent common problems. However, we acknowledge that the inspection can be a stressful time for practices. We have produced a handbook that explains our process and the CQC website contains useful guidance, tips and information such as myth busters: www.cqc.org.uk/content/gp-and-out-hours-mythbusters-nigel-sparrow
Key points
The CQC is the independent regulator of health and adult social care services in England The purpose of the CQC is to ensure that people receive safe, effective, compassionate, high-quality care The CQC rolled out its new inspection methodology on 1 October 2014 for all general practices and out-of-hours services Regulation of general practices involves registering, using intelligent monitoring, inspecting and rating services. Inspections address five key questions: Is a service safe? Is it effective? Is it caring? Is it responsive to peoples’ needs? And is it well-led? CQC plans to inspect all general practices in England by April 2016.