
Abstract
This article focuses on the end-stage of diabetic foot disease: Diabetic foot sepsis. The aetio-pathogenesis and clinical diagnosis of diabetic foot disease is discussed. The article explores the management of limb- and non-limb-threatening diabetic foot infections, and in particular, the importance of utilising the diabetic foot clinic and the specialist multi-disciplinary team to prevent high-risk patients from further foot deterioration. The importance of preventing the development of diabetic foot disease through screening and primary and secondary prevention strategies is also discussed.
The GP curriculum and the diabetic foot
From the GP curriculum there are four main areas that list the learning objectives that are relevant for GPs treating patients with diabetic foot sepsis: Recognise the signs of illnesses and conditions that require urgent intervention Promote health through a health promotion or disease prevention programme Understand the role of good diabetes management in prevention and/or postponement of associated morbidity and mortality Understand the need for early recognition and monitoring of complications in diabetes mellitus Communicate with patients clearly and effectively about the risk of complications from diabetes mellitus Advise patients appropriately regarding lifestyle interventions for obesity, diabetes mellitus, and hyperlipidaemia. Co-ordinate care with other primary care and secondary care professionals with diabetes as a focus Understand the systems of care for metabolic conditions including the roles of primary and secondary care, shared-care arrangements, multi-disciplinary teams and patient involvement
Diabetes is an enormous worldwide problem, affecting hundreds of millions of people across the globe. According to the National Institute of Health and Care Excellence (NICE), in 2013 over 3 200 000 adults in the UK were diagnosed with diabetes, with about 90% having type-2 diabetes. Diabetic care is estimated to account for at least 5% of UK healthcare expenditure, and up to 10% of NHS expenditure. The estimated cost of diabetic foot ulceration and related amputations in 2010–11 was £985 600 282, and this is predicted to increase to £2 104 864 723 by 2035–36, which is staggering (Hex, Bartlett, Wright, Taylor, & Varley, 2012).
Diabetic foot ulceration affects around 15% of patients (Singh, Pai, & Yuhhui, 2013). The underlying cause for this problem is either neuropathy or ischaemia; with patients being at an increased risk of severe limb-threatening infections and amputation. Diabetic foot disease is a leading cause of hospitalisation in diabetic patients, a major cause of morbidity and mortality, and a significant financial burden on the NHS.
A study by Qari and Akbar (2000) from Saudi Arabia (where diabetes is very common) looked specifically at patients admitted to hospital with diabetic foot infections. They found that the most common precipitating factors were peripheral neuropathy, peripheral vascular disease, smoking, and poor glycaemic control. Among this patient group there was also a significant level of other complications of diabetes: retinopathy in 47%, chronic renal failure in 32%, and 50% had ischaemic heart disease. The mean duration of diabetes was 17 years. Infected foot ulcers were the most common type of presentation, 65% of patients required formal surgical debridement, and 23.5% required major amputation. These figures are startling, but do emphasise the point that diabetes is a major disease burden, and that diabetic foot sepsis really does represent the tip of the iceberg of what is a major public health problem.
Aetio-pathogenesis
Sensory neuropathy is the cause of more than 60% of diabetic foot ulcers (Singh et al., 2013). Raised blood glucose levels lead to increased enzyme production, such as aldose reductase and sorbitol dehydrogenase. These enzymes convert glucose into sorbitol and fructose, and as these sugar products accumulate the synthesis of nerve cell myoinositol is decreased, which affects nerve conduction. Furthermore, hyperglycaemia-induced microangiopathy leads to metabolic, immunologic and ischemic injury of autonomic, motor and sensory nerves.
Sensory nerve injury leads to insensate limbs that are prone to injuries and repetitive minor trauma that is easily overlooked. Damage to the nerve innervations of the small muscles of the foot can gradually lead to an alteration of the anatomical framework of the foot and formation of deformities. These deformities, in turn, create abnormal bony prominences and pressure points that predispose to callus formation that leads to skin breakdown and ulceration. This effect on the autonomic nervous system leads to dryness and fissuring of the skin, making it weak and prone to ulceration and infection. Hence, the risk of developing foot ulcers is increased by seven-fold in diabetic patients with neuropathy.
The other major contributing factor to diabetic foot disease is ischaemia (Hobizal & Wukich, 2012). Macrovascular disease typically manifests as a diffuse multi-segmental atherosclerotic disease affecting the infra-popliteal vessels. Microvascular changes lead to capillary basement membrane thickening, altered nutrient exchange, tissue hypoxia, and microcirculation ischemia. Such changes lead to progressive ischaemia, claudication, rest/night pain, and ultimately, tissue loss/ulceration and gangrene.
Many patients with diabetic foot disease have a combination of neuropathy and ischaemia. This combination can create a vicious circle, whereby patients are prone to foot ulceration and infection, and the poor blood supply makes wounds far more difficult to heal. Particularly, in the case of diabetic foot sepsis, a compromised blood supply significantly reduces both natural healing and also the actual delivery of antibiotics to the infected site. This makes a purely conservative management of diabetic foot sepsis usually ineffective, and explains why most patients require radical debridement or amputation, and/or major revascularisation procedures.
Diagnosis
The cornerstone of good management for diabetic foot disease is a thorough clinical history and examination. The symptoms of neuropathy that patients may describe include:
Tingling in the feet Sharp stabbing pains Numbness, Weakness
Classic ischaemic symptoms include:
Rest pain in the dorsum of the foot Pain at night that prevents sleep, with the patient having to hang the limb out of bed Tissue loss/ulceration (critical limb ischaemia) Calf discomfort on walking (claudication)
The history should also explore the duration of diabetes, previous ulcers/gangrene and amputations and current diabetic treatment, previous glycosylated haemoglobin (HbA1c) levels, and also any other complications of diabetes (such as retinopathy, nephropathy, or ischaemic heart disease). It is also important to look for adherence to chronic disease monitoring and whether individualised management plans have been produced for the patient. This assessment will give the GP an indication of the global severity of the diabetes, and thus the risk of foot disease.
Examination of the foot should begin with a detailed inspection. Specifically, look for abnormalities such as dry fissured skin, hair loss, bony deformities, areas of callus, nail defects, ulceration, discolouration/gangrene, and signs of infection such as erythema, swelling and/or purulent discharge. Figure 1 shows a neglected diabetic foot with obvious gangrene and necrosis.
A case of severe diabetic foot disease with gangrene, tissue necrosis and deep-seated infection.
Look between the toes, on the plantar aspect of the foot and around the heel (i.e. raise the foot off the couch to see underneath). Palpation should incorporate checking the temperature of the foot, capillary refill time, pulse status, areas that are tender/painful, and feeling for any areas of fluctuance or bogginess that suggest an underlying abscess and spreading infection.
Neurological testing should include checking for areas of sensory loss with a monofilament, vibratory sensation, and deep tendon reflexes. When examining an ulcer, a sterile stainless steel probe is recommended for assessing its depth and to see if there are any sinus tracts present. If bone is exposed at the base of an ulcer, there is likely to be underlying osteomyelitis. The location, size, shape, depth, base and margins of the ulcer should be described accurately. Taking a picture to attach to the patient’s notes can be helpful for future comparison.
Charcot’s arthropathy is another differential for a hot, swollen, and painful foot, which although not the focus of this article, should also be borne in mind. This is generally caused by repetitive trauma superimposed on a severely neuropathic foot (Frykberg et al., 2000). Autonomic neuropathy leads to an increased blood flow to the extremity, resulting in osteopenia and increased bone weakness. A vicious cycle ensues whereby the patient continues to walk on the injured foot, allowing repetitive damage to occur. Clinical diagnosis is based on profound unilateral foot swelling, increased skin temperature, erythema, joint effusion, and bone resorption in an insensate foot (particularly in the presence of intact skin). NICE (2015a) recommends that patients with suspected acute Charcot arthropathy should be referred to the diabetic foot clinic to be seen within one working day.
It is also important to assess the patient globally for symptoms and signs of systemic upset. Patients might describe sweats and rigors, reduced appetite and nausea. Clinical assessment might show pyrexia, tachycardia, hypotension and elevated blood sugars. A patient with neuropathy, and who also has a possible foot infection and describes acute pain in their foot, should be taken seriously. This suggests there is possibly a significant underlying infective process over and above the background neuropathy.
Management of diabetic foot sepsis
The signs that suggest severe diabetic foot sepsis include:
Over 2 cm of cellulitis (and/or spreading cellulitis) Foot oedema and swelling, bogginess and fluctuance (suggesting an abscess) Purulent discharge and wound odour A deep ulcer with exposed muscle/tendon/bone Ischaemic foot changes/gangrene Signs of systemic toxicity
These patients are at very high risk of limb loss and they need to be recognised and referred to hospital immediately (NICE, 2015a). Figure 2 shows a severe limb-threatening diabetic foot infection.
Elderly diabetic female with a history of plantar callus presenting with (A) ulceration beneath the fourth metatarsal head and (B) the fourth left toe, with poor glycaemic control. A severe foot infection was apparent and (C) radiographs showed erosive disorganization of the fourth metatarsophalangeal joint. The patient developed a foot infection secondary to the plantar callus that progressed to osteomyelitis of the fourth toe and fourth metatarsal. (D) She was treated with parenteral antibiotics and ray resection. Reprinted from The Journal of Foot and Ankle Surgery, 45(5 Suppl), Frykberg RG, Zgonis T, Armstrong DG, et al., Diabetic Foot Disorders: A Clinical Practice Guideline (2006 Revision), S1-66, 2006, with permission from Elsevier.
On admission to hospital, the patient should be managed according to the Sepsis 6 pathway (Dellinger et al., 2013). This pathway was developed by the Surviving Sepsis Campaign; it was designed to improve outcomes in patients with severe sepsis/septic shock. The pathway includes: high flow oxygen, blood cultures, checking the blood lactate level, intravenous antibiotics, intravenous fluids, catheterisation and fluid balance. All these should be performed within the first hour of recognition of severe sepsis. A full set of bloods should be taken including: full blood count, urea and electrolytes, liver function tests, C-reactive protein and/or erythrocyte sedimentation rate, coagulation screen, group and save, blood glucose and HbA1c levels.
A foot X-ray should be taken to look for signs of osteomyelitis and subcutaneous gas. If foot X-rays are inconclusive then a magnetic resonance image of the foot may be required to confirm deep infection. Very sick patients with severe sepsis, organ failure and septic shock will require intensive care input. Depending on the severity of the infection, the patient may require immediate incision and drainage/surgical debridement, and/or amputation.
Patients with diabetic foot sepsis have often had diabetes for many years, and usually have other co-morbidities secondary to their diabetes. Therefore, during their stay in hospital such patients should be seen by other members of the multi-disciplinary team as required: diabetologists, vascular surgeons, podiatrists, occupational therapists, physiotherapists, dieticians, orthopaedic surgeons, nephrologists, cardiologists and specialist wound care nurses.
If there is clinical evidence of underlying arterial disease (i.e. gangrene, absent pulses, rest pain) then the patient should be reviewed by a vascular surgeon. A more thorough assessment of the patient’s vasculature can then be carried out. Ankle-brachial pressure index values are important, but are often elevated in people with diabetes, as a result of calcification of the arteries. In secondary care, toe pressures and transcutaneous oxygen levels can be particularly helpful. Other diagnostic tools available include arterial duplex, computed tomography angiography, magnetic resonance angiography, and conventional angiography. Such investigations will help identify underlying arterial disease and will guide treatment options (bypass surgery, endarterectomy, or endovascular procedures).
Diabetic foot clinic
Diabetic foot problems are easy to underestimate. A patient with even “minor” diabetic foot disease is at high risk of progressive and severe deterioration over a short time period (see Fig. 3).
Schematic highlighting the possible rapid progression from ‘mild’ diabetic foot disease to severe limb and life-threatening diabetic foot sepsis.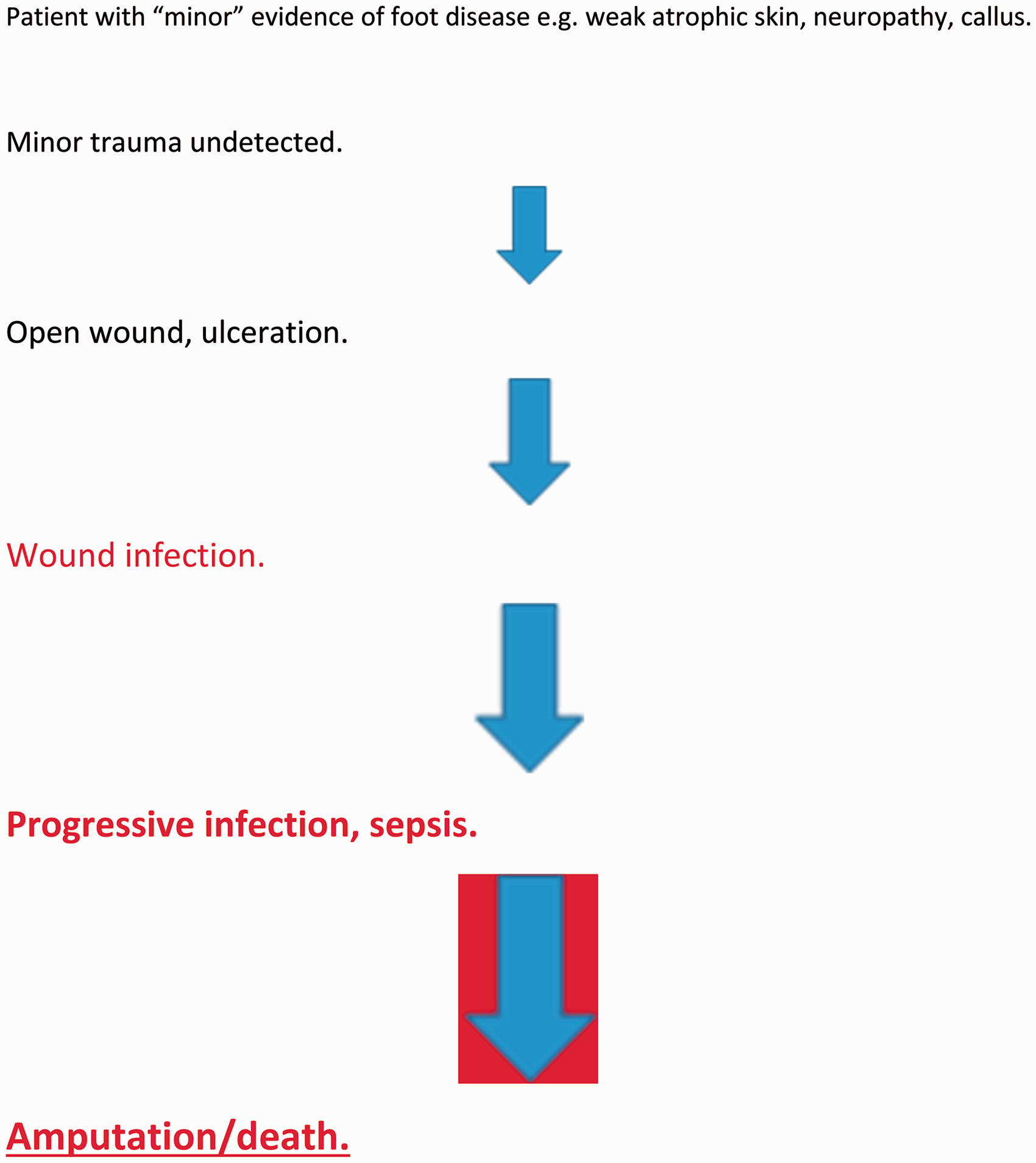
To prevent deterioration in diabetic foot disease, it is vital to ensure good glycaemic control, adequate perfusion of tissues, local wound care and regular debridement, off-loading of the foot, control of infection by appropriate antibiotics and management of co-morbidities. Patient education and support is also required. Individual practices have different pathways for reviews of diabetic patients. At the very least, the monitoring of foot care, perfusion and sensation should be undertaken during diabetic chronic disease management clinics by the practice nurse and reinforced by the GP at every opportunity.
Those patients who have developed diabetic foot disease benefit from being seen in a dedicated diabetic foot clinic. The chief aim of the multi-disciplinary diabetic foot clinic is to manage high-risk patients in the community and prevent further foot deterioration.
It is important not to wait until patients have advanced diabetic foot disease/ulceration or gross deformity before referring them to the foot clinic. Patients at low risk are those with no risk factors except callus alone, with those at moderate risk including those with deformity, neuropathy and non-critical limb ischaemia (NICE, 2015a). Patients at high risk are those: with previous ulceration or amputation, on renal replacement therapy/dialysis, with neuropathy and non-critical limb ischaemia together, neuropathy in combination with callus and/or deformity, or non-critical limb ischaemia in combination with callus and/or deformity.
Low-risk patients should continue to have annual foot assessments, with the importance of foot care being strongly emphasised to them. Patients at moderate-to-high risk should be referred to the foot clinic with moderate-risk patients being seen within 6–8 weeks and high-risk patients within 2–4 weeks. The role of the practice nurse and GP therefore is to identify patients with established diabetic foot disease, and those who are moderate-to-high risk for deterioration, and refer them to the foot clinic (see Fig. 4).
The diabetic foot clinic and appropriate referrals.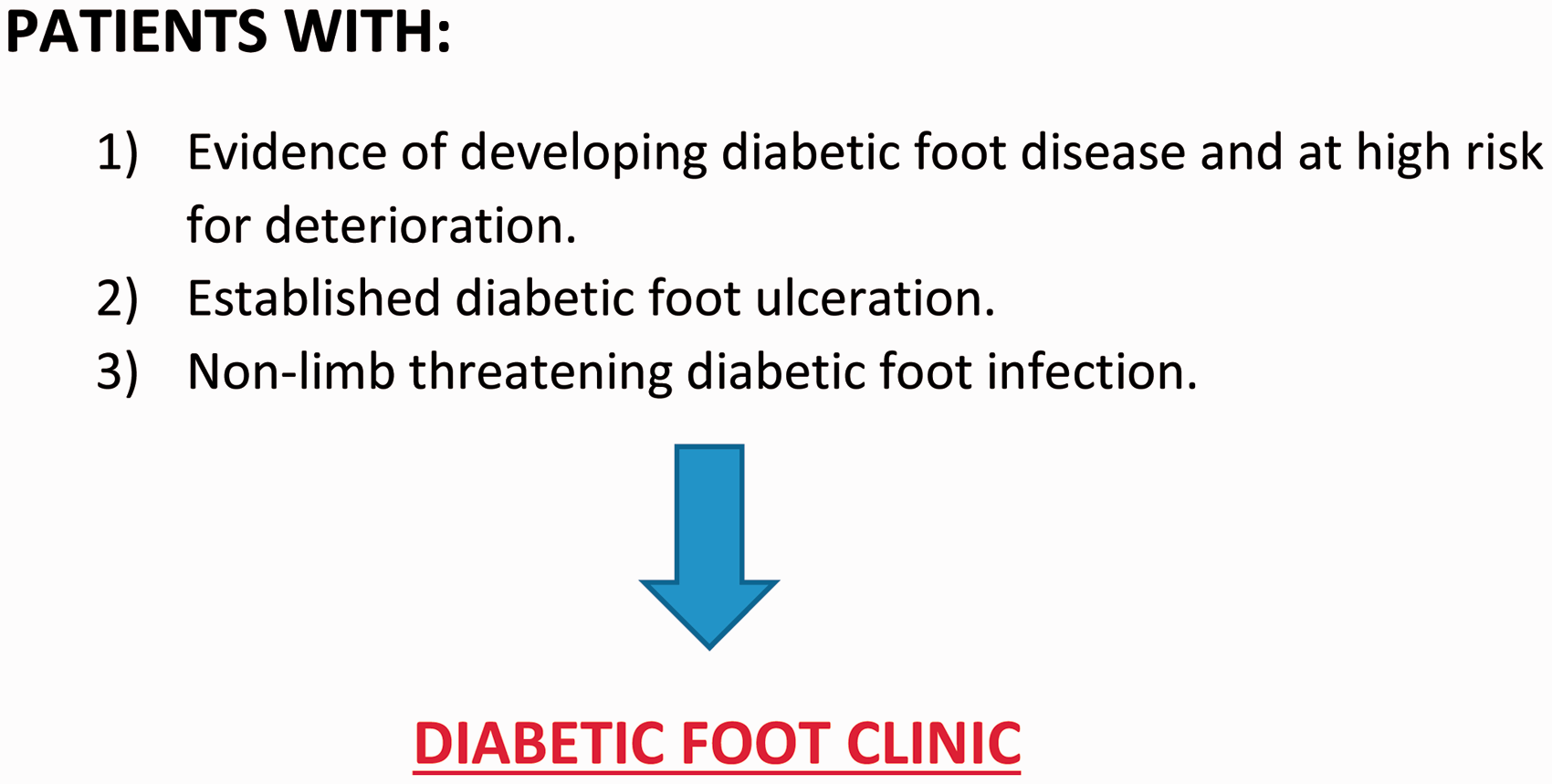
Non-limb-threatening diabetic foot infection
Not all diabetic foot infections require hospital admission; many can be referred to the diabetic foot clinic to be seen urgently within one working day (NICE, 2015a). As highlighted in Fig. 5, patients with mild superficial infection and no evidence of systemic toxicity can often be managed in the community. However, take care to ensure that the patient does not have any signs of underlying severe infection. It is not uncommon for diabetic patients to show only subtle signs of infection, despite a major underlying and ‘hidden’ disease process. For example, there may be only a small area of superficial cellulitis in a well-appearing patient, but a much deeper and tracking abscess in the plantar aspect of the foot, which can be missed if the underside of the foot is not examined.
Non-limb-threatening diabetic foot infection criteria and management.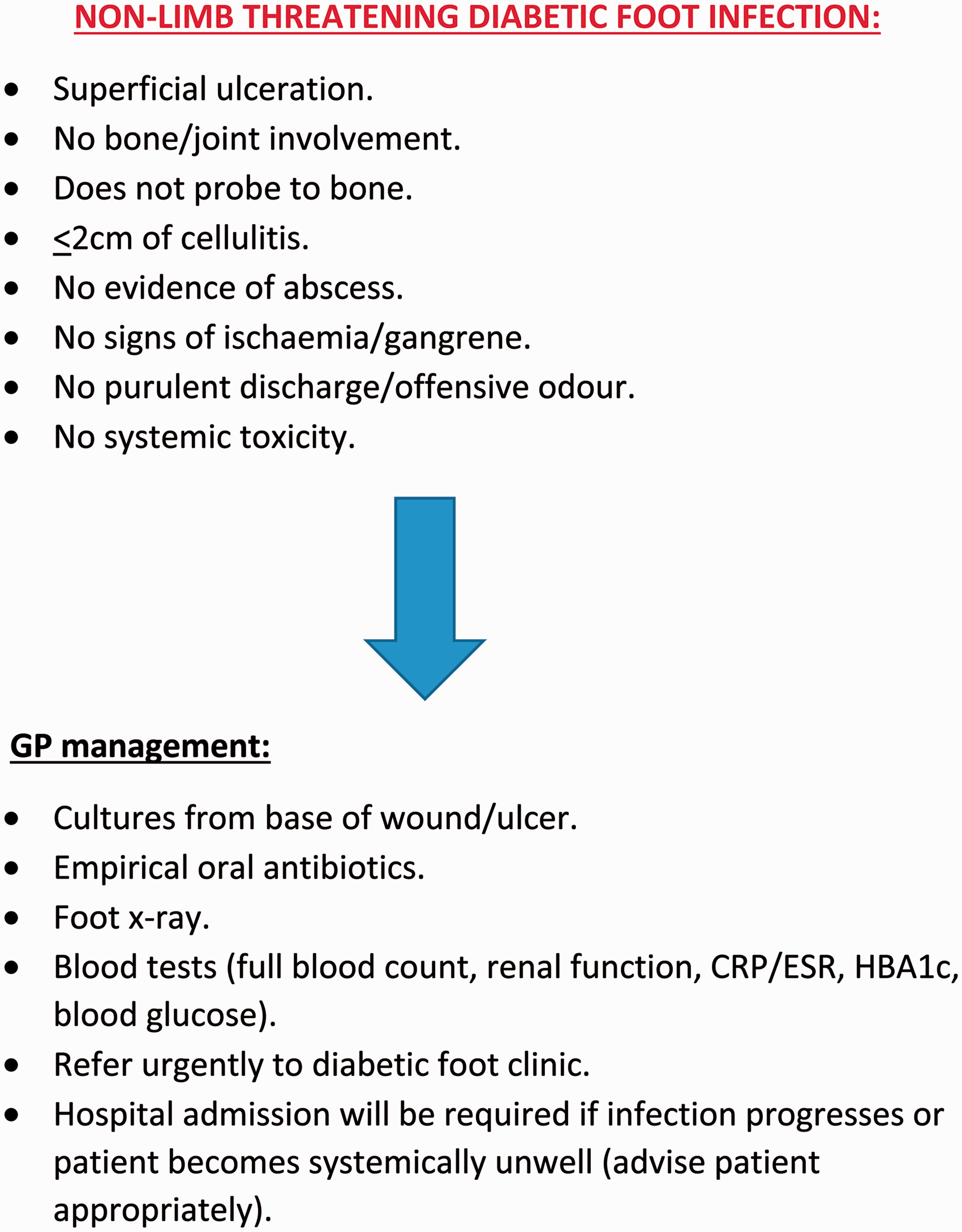
Appropriate investigations that can be arranged by the GP include a set of bloods, a deep wound swab and a foot X-ray. Empirical antibiotics should be commenced (based on local sensitivities as reflected in local prescribing guidelines) and the patient should be referred urgently to the diabetic foot clinic. However, the patient should be specifically warned that if the infection progresses and he/she should become systemically unwell, then hospital admission is indicated. Also, if attendance at the diabetic foot clinic is going to be delayed, then the GP should arrange for a follow-up appointment in 24–72 hours. If at any point the GP suspects the presence of a limb-threatening diabetic foot infection, then urgent hospital admission is required.
Preventing diabetic foot disease
The multi-disciplinary team/diabetic foot clinic is not focused primarily on preventing diabetic foot disease, but rather on treating it after it has already developed. This of course is vitally important, and in many cases appropriate treatment halts further deterioration and ulcers/wounds are healed. The same is true of patients admitted to hospital with more severe forms of diabetic foot disease. However, it is far better to prevent diabetic foot disease developing in the first place, as opposed to treating it after the fact. Indeed the primary and secondary prevention of diabetic foot disease is where the GP’s input is most required. It is the collective and enthusiastic commitment (on a national scale) by GPs to address the underlying risk factors for diabetic foot disease that is highly likely to significantly reduce its incidence.
The thrust of the GP’s efforts should be to promote healthy lifestyles among their patients in the community. In essence this means encouraging: good dietary habits, avoidance of excess fatty/sugary foods, exercise and weight loss. Such an approach is geared primarily towards the prevention/treatment of type-2 diabetes, but it is also vitally important in type-1 diabetes. In the context of vascular disease (with its potential contribution to diabetic foot disease) smoking cessation should also be promoted.
With regards to the management of patients with established diabetes mellitus, GPs should refer to recent NICE guidelines (NICE, 2015b, 2015c). Although the details of this guidance will not be discussed here, there are some important points to mention. In particular, the recommendation of individualised care plans for patients. For example, when providing dietary/lifestyle advice, this should be given in a way that is considerate of the patient’s needs, culture and beliefs, and is sensitive to their willingness to change and the effects on their quality of life. Patient education programmes should also be available that meet the patient’s linguistic, cognitive and literacy needs. It is also of paramount importance that GPs communicate clearly and effectively to patients about the risks of complications of diabetes. In the context of this paper, the risks of foot disease should be explained, with emphasis on the importance of maintaining good glycaemic control and promoting foot care/regular self-examination. Such an integrated approach is more likely to achieve patient concordance with treatment, sustained optimisation of glycaemic control, and thus a decreased likelihood of diabetic foot complications developing.
Conclusions
Diabetes is a massive problem and a cause of major morbidity and mortality worldwide. Diabetic foot problems are a major burden on both patients and the NHS. Diabetic foot sepsis represents the end-stage of diabetic foot disease, and such patients are at very high risk of amputation and/or death. Of course, it is vital that such patients are rapidly diagnosed by GPs and referred to hospital. However, it is far better to identify these patients early and refer them to the diabetic foot clinic to prevent the advancement to limb- and life-threatening diabetic foot sepsis. Even more important is the primary and secondary prevention of diabetic foot disease, particularly in the context of type-2 diabetes, which is the major cause of adult diabetes in the UK. Such prevention strategies should focus on lifestyle changes, dietary improvements, exercise, and weight loss. For patients with established diabetes, the above measures equally apply, in addition to the importance of optimising glycaemic control and appropriate foot care.
Key points
Diabetic foot infections should be taken very seriously as they can progress rapidly, leading to amputation and death Patients with diabetic foot ulceration and non-limb-threatening diabetic foot infections should be referred urgently to the diabetic foot clinic Patients with developing diabetic foot disease who are at risk of deterioration should also be referred to the foot clinic GPs should aim to prevent diabetic foot disease through screening, risk factor reduction, and optimisation of glycaemic control Foot care and regular self-examination should be encouraged in diabetic patients