
Abstract
Dealing with a medical emergency in an environment with limited life-saving resources is a frightening situation. Oncology emergencies can be especially challenging and life-threatening. Although these rarely present in primary care, they require specific urgent treatment, and therefore their recognition is important. This article intends to give an insight into diagnosis and management of oncology emergencies in a primary care setting.
The GP curriculum and oncology emergencies
Describe palliative care emergencies and their appropriate management, e.g. major haemorrhage, spinal cord compression, hypercalcemia and use of emergency drugs Counsel and explain for patients, families and their carers:
^ a holistic and personalised assessment of needs ^ symptom control ^ disease progression ^ processes around death and dying ^ advance care planning ^ normal and abnormal bereavement
Recognise signs of conditions requiring urgent intervention Be aware of urgent management of such conditions Keep resuscitation skills up-to-date
What is an oncology emergency?
Classification of oncologic emergencies
Although this article focuses on urgent intervention, the ceiling of care is always dictated by the patient and/or carers. Oncology patients differ from the rest of the population, as their conditions may be terminal. Health care professionals need to discuss advance care planning with this cohort of patients to establish whether they wish for hospital emergency treatment or conservative home management. Each oncology emergency discussed in this article looks at both active and conservative management options.
Hypercalcemia
Hypercalcemia is the most common metabolic oncology emergency. It is frequently associated with tumours of the breast, lung, kidney, and oesophagus, haematological malignancies (notably multiple myeloma), and cancer of the head and neck (Cervantes & Chirivella, 2004).
The regulation of serum calcium is a complex mechanism involving parathyroid hormone (PTH), calcitonin and vitamin D that runs on a positive feedback system. In patients with cancer, a variety of mechanisms may elevate calcium levels. The tumour may release PTH-related peptides and vitamin D analogues or metastatic deposits can locally activate osteoclasts.
The presentation of hypercalcemia is diverse and depends on its severity. The diagnosis is established by measuring corrected serum calcium, which is greater than 2.65 mmol/L (uncuffed sample to avoid falsely high results). Symptoms include polyuria, polydipsia, dyspepsia, constipation, vomiting, depression or mild cognitive impairment, and muscular fatigue. Mild hypercalcaemia is an adjusted serum calcium concentration of 2.65–3.00 mmol/L, moderate 3.01–3.40 mmol/L and severe greater than 3.40 mmol/L. Severe hypercalcaemia may result in pancreatitis, cardiac arrhythmias and coma (National Institute of Clinical Excellence (NICE), 2014).
Active management
The grave prognosis of hypercalcemia necessitates prompt treatment. If the patient has severe hypercalcaemia, an urgent referral to the hospital oncology or medical team is necessary for immediate admission, intravenous (IV) fluids and bisphosphonates, e.g. pamidronate.
The frequency of monitoring of serum calcium following treatment will usually be specified by the specialist. Without treatment of the underlying cancer, hypercalcaemia usually returns 2–4 weeks after calcium-lowering treatment, and so calcium levels should be rechecked then if appropriate (NICE, 2014).
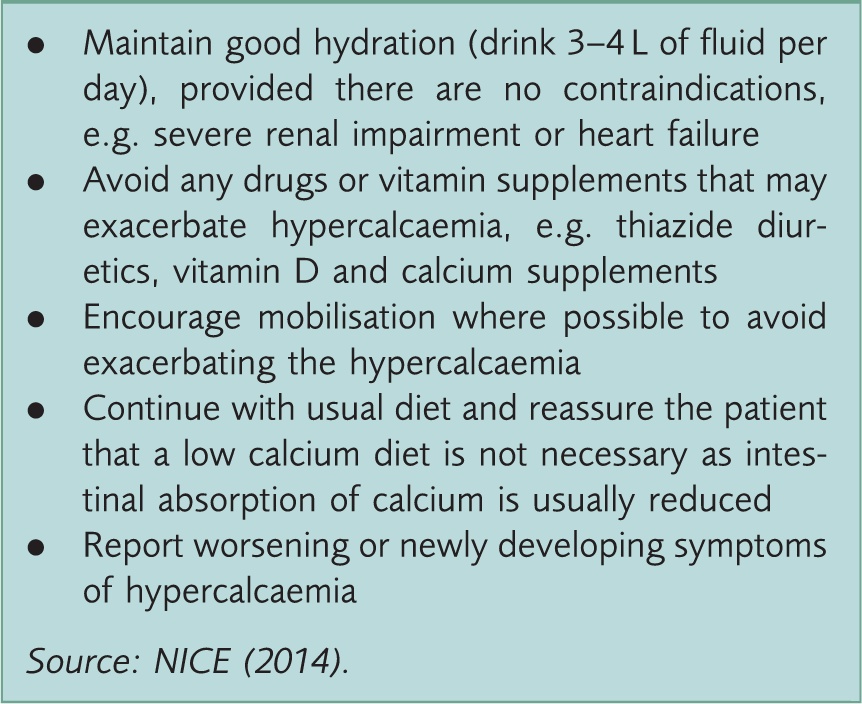
Conservative management
Advice on supportive measures for the management of hypercalcaemia.
Hyponatremia
Low serum sodium is mostly associated with the syndrome of inappropriate anti-diuretic hormone (SIADH). SIADH is most often associated with bronchogenic carcinoma (10–45% of patients with small cell lung cancer have SIADH), but also occurs in carcinoid tumours, leukaemias and lymphomas. Hyponatremia is also caused by drugs, such as thiazide diuretics, tricyclic antidepressants and selective serotonin reuptake inhibitors. It is typically defined as a serum sodium concentration lower than135 mmol/L, although local reference ranges may vary (Lewis, Hendrickson, & Moynihan, 2011).
The pathophysiology of SIADH revolves around a hormone stored in the pituitary gland (the anti-diuretic hormone (ADH)), which acts on the kidneys to regulate body water. Hyponatremia in SIADH occurs with inappropriate secretion of ADH. This results in hypo-osmolality, despite normal or increased plasma volume, which leads to impaired water excretion.
Clinical features depend on the rate and magnitude of the development of hyponatremia. Therefore, the presentation may be silent, with biochemistry results being the only indicator. A sodium level of 130–135 mmol/L (mild hyponatraemia) is usually asymptomatic. Generalised muscular weakness may be seen at serum sodium levels of 125–129 mmol/L (moderate hyponatraemia). Confusion, convulsions, and even coma and death can result at levels below 120 mmol/L (severe hyponatraemia) (Castillo, Vincent, & Justice, 2012).
Active management
Hospital admission and management is necessary in cases of severe or symptomatic hyponatraemia, in order to allow for close monitoring of fluid balance and the use of demeclocycline. Rapid correction of serum sodium should be avoided, due to the risk of precipitation of central pontine myelinolysis, however, it may be necessary in severe cases.
Conservative management
Hyponatremia resolves once its cause is eliminated, which is not always possible if the cancer is unresectable or untreatable. Patients with mild asymptomatic hyponatremia can be managed in primary care. A medication review with a view to discontinuing any contributory drugs should be conducted and sodium levels repeated 2 weeks after discontinuation.
Metastatic spinal cord compression
Metastatic spinal cord compression (MSCC) is described as spinal cord or cauda equina compression that threatens or causes neurological disability. It may be caused by direct pressure, vertebral collapse or instability by metastatic spread, or direct extension of malignancy. The cancers most likely to metastasise to bone are breast, kidney, thyroid, prostate, and lung cancers. Patients with these cancers thus have a higher risk of developing compression of the spinal cord. The most common sites for compression are thoracic (70%) and cervical (20%) vertebrae (Simon, Watson, Drake, Fenton, & McLoughlin, 2008).
Patients will generally present with neurological symptoms, including radicular pain, limb weakness, walking difficulty, sensory loss, urinary retention or faecal incontinence (NICE, 2008). Anatomically, the spinal cord ends at the level of the L1 and L2 vertebrae. Compression above this level causes upper motor neurone signs, such as increased tone, hyper-reflexia, and up-going plantar reflexes; compression below this level causes lower motor neurone signs, such as reduced tone, absent or reduced reflexes, and down-going plantar reflexes.
A Scottish audit showed that there were significant delays from the time when patients first develop symptoms to when GPs and hospital doctors recognise the possibility of MSCC and make an appropriate referral (Levac et al., 2001). The median times from the onset of back pain and nerve root pain to referral were 3 months and 9 weeks, respectively. More importantly, nearly half of all patients with MSCC were unable to walk at the time of diagnosis, and of those patients a remarkable 67% did not recover function after a month. Of those who could walk unaided at the time of diagnosis, 81% were able to walk at a month. The ability to walk at diagnosis was also significantly related to overall survival. This reinforces that GPs must urgently refer (i.e. same-day admission) patients with suspected MSCC. Figure 1 illustrates thoracic MSCC.
Magnetic resonance image of MSCC.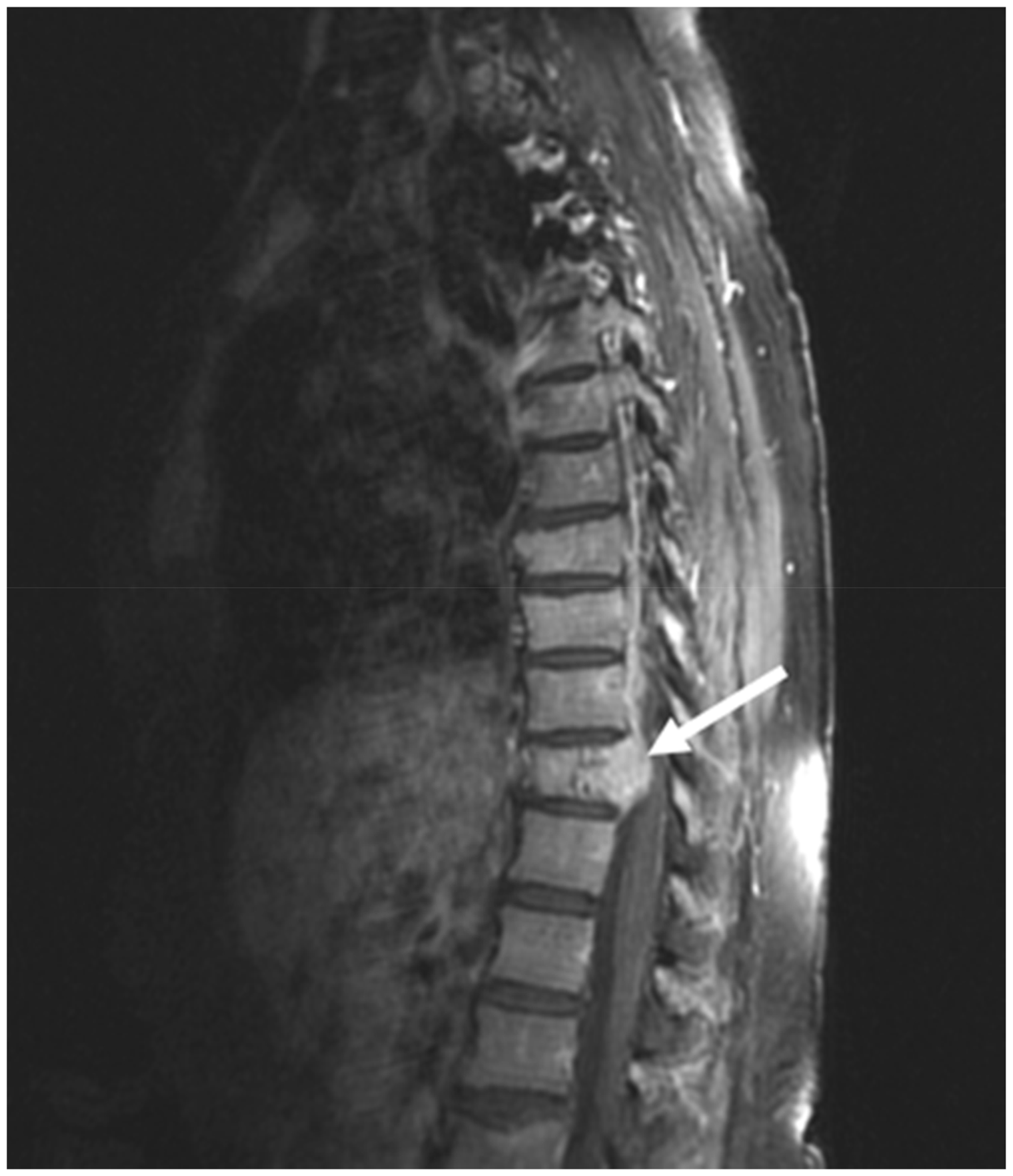
Active management
If there are features of MSCC, seek immediate specialist advice (NICE, 2008). Local referral pathways may vary, but contact points may include the local MSCC coordinator, the patient’s oncologist or palliative care consultant, or via acute hospital admission. Definitive management options for MSCC in hospital include radiotherapy and surgery. Unless contraindicated (including a significant suspicion of lymphoma), offer a loading dose of 16 mg of dexamethasone as soon as possible. Patients should be nursed flat with neutral spine alignment.
Conservative management
The appropriateness of dexamethasone can be discussed with the oncology team. After a full discussion of the risks, patients should be helped to position themselves and mobilise as symptoms permit with the aid of orthoses and/or specialist seating to stabilise the spine, if appropriate (NICE, 2008).
Malignant airway obstruction and dyspnoea
The most common causes of airway obstruction are tumours of the tongue, oropharynx, thyroid, trachea, bronchi and lungs. Up to 30% of patients with lung cancer will develop airway obstruction (Lewis et al., 2011). The obstruction may result from external pressure on the trachea or bronchi by the tumour or direct infiltration of the tumour into the above structures.
Location, magnitude and severity of the obstruction dictate the clinical manifestation. The most common presentation is dyspnoea, which is usually worse at night and on lying supine. There may also be wheeze, productive cough or stridor. These symptoms may be quite minimal until the airway becomes critically narrow, posing a life-threatening situation. Diagnosis is confirmed with chest X-ray and computed tomography (CT) scans.
Active management
Prompt recognition and treatment is vital: in an emergency, call for help, request an emergency ambulance and commence basic life support (BLS) immediately (see resuscitation skills section later).
Conservative management
For a patient who has expressed a wish to not be resuscitated, e.g. by completing ‘do not attempt cardiopulmonary resuscitation’ (DNACPR) documents, reassurance, oxygen therapy and diamorphine may help breathing and aid relaxation.
Dysphagia
Dysphagia is a debilitating, depressing, and potentially life-threatening complication, most commonly seen in patients with oesophageal or head and neck cancer (Raber-Durlacher et al., 2006). It indicates delayed passage of solids or liquids from the oral cavity to the stomach, and can be caused by direct impact of the tumour, cancer resection, chemotherapy and radiotherapy. In addition to swallowing complaints, patients may present with choking, coughing, regurgitation, poor nutrition and recurrent respiratory infection.
Oropharyngeal examination involves inspection of the oral cavity, dental status, dental prosthesis, oral dryness, as well as evaluation of the strength, motion, and symmetry of the tongue, lips, jaws, and soft palate. Assessment can be done by a simple swallow test to different consistencies to give the GP a rough objective indication of the severity of dysphagia.
Active management
Severe dysphagia or dysphagia causing breathing difficulties will require emergency hospital admission. Management options in hospital may include a formal assessment and investigations such as videofluoroscopy and barium swallow. Upper endoscopy may enable stent insertion. Surgery may be needed to relieve the obstruction.
Conservative management
Management at home may include provision of analgesia and symptomatic relief of breathlessness via oxygen and drugs, such as diamorphine. Longer-term supportive measures may include artificial feeding by a nasogastric tube or a percutaneous endoscopic gastrostomy tube. The decision for the latter would need to be made via a multidisciplinary team, including gastroenterologists, dieticians, and the speech and language therapy team.
Superior vena cava syndrome
Superior vena cava syndrome (SVCS) is caused by obstruction of the blood flow through the superior vena cava (SVC) to the right atrium. This obstruction can be due to extrinsic compression, tumour invasion, thrombosis or insufficient venous return secondary to intra-arterial or intraluminal diseases. The most common cause is superior mediastinal pressure associated with evolution and expansion of intrathoracic tumours. Of these, bronchogenic cancer most frequently causes SVCS (75% of all cases). This is followed by lymphoma (17%) and metastatic cancer (7%) (Cirino, Coelho, Rocha, & Batista, 2005).
The SVC provides venous drainage for the head, neck, upper extremities and upper thorax: it extends from the junction of the right and left innominate veins to the right atrium. Its thin-walled structure and low pressures within make it easily compressible. When the SVC is obstructed, collateral routes are provided by other venous systems, such as the azygous, internal mammary and long thoracic venous systems, which allow some venous drainage into the heart.
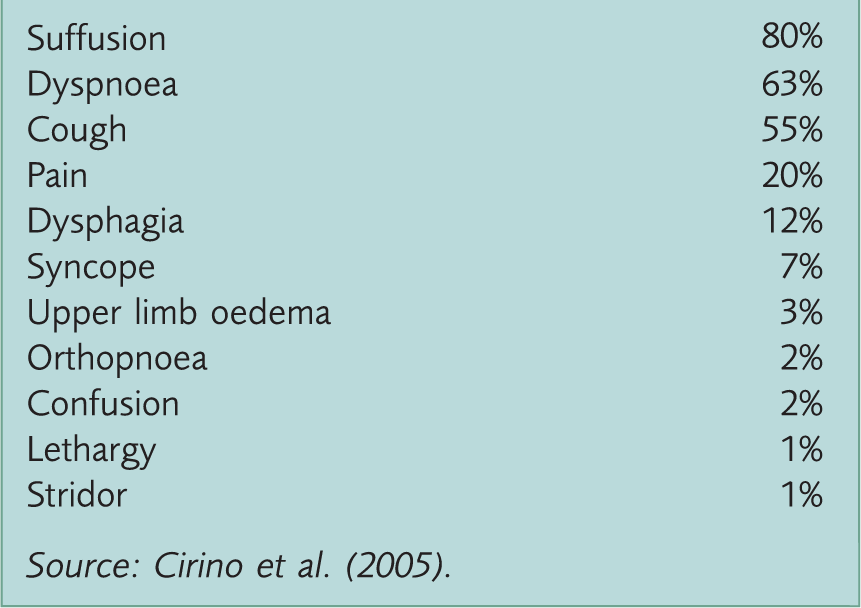
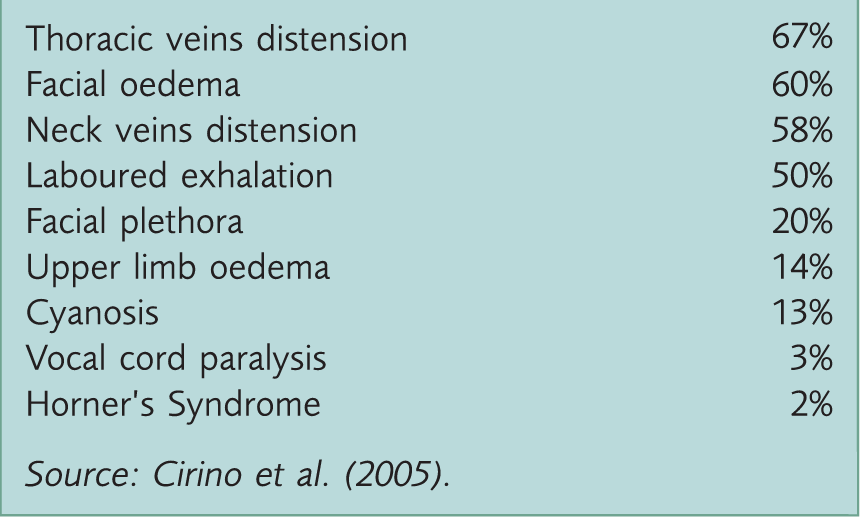
SVCS symptom frequency.
SVCS examination findings frequency.
Active management
Acute airway obstruction due to SVCS will require emergency hospital admission. Consider basic measures, such as sitting the person upright and ensuring a flow of cool air to the face. Corticosteroid use may be beneficial, e.g. prednisolone 60 mg orally, but initiation should ideally be discussed with a palliative care consultant.
Although the diagnosis may be made on clinical grounds in patients with overt signs and symptoms, further investigations maybe necessary in hospital in more subtle cases, e.g. chest X-ray, CT scan, magnetic resonance imaging and Doppler scan. Treatment measures in hospital may include thrombolysis, chemotherapy, radiotherapy and surgery.
Conservative management
Treatment measures should address possible breathlessness, pain and panic, e.g. with opioids and/ or benzodiazepines. Dexamethasone may be used, but should be discussed with a specialist.
Neutropenic sepsis
Neutropenic sepsis is a potentially fatal complication of anticancer and immunological treatment, particularly chemotherapy, with mortality rates as high as 21% (Kuderer, Dale, Crawford, Cosler, & Lyman, 2006). Neutropenic sepsis has been highlighted as an area of clinical priority in the UK, initially by a publication from the National Confidential Enquiry into Patient Outcome and Death (NCEPOD, 2008).
Although novel biological agents generally have a lower rate of neutropenia than cytotoxic chemotherapy, neutropenic sepsis is more common with chemotherapy. Cytotoxic anticancer chemotherapy is designed to kill neoplastic stem cells by causing irreparable damage to the DNA. The mechanism behind this damage varies according to the chemotherapy drug. The more rapidly dividing normal cells, such as hair follicles, mucosal linings and bone marrow cells can also be affected, causing the well-documented toxicities of alopecia, mucositis and bone marrow suppression, leading to neutropenia, anaemia and thrombocytopenia. There is a tendency for neutropenic sepsis to occur more commonly in the first two cycles of treatment, where patients may present with general symptoms of infection.
Neutropenic sepsis should be suspected in a person with known neutropenia, or any known cause for neutropenia, who is generally unwell, or has a temperature higher than 38℃, or meets the criteria of sepsis (NICE, 2015).
Active management
If neutropenic sepsis is suspected, refer the person immediately to secondary care for assessment. If critically unwell, arrange admission via an emergency ambulance. If clinically stable, follow the local protocols, which may require direct referral to the oncology centre or local medical team.
Conservative management
Unfortunately, antibiotics cannot be administered at home or outside of hospital as IV access and close monitoring of vital signs are required. On a home visit, reassurance can be given to patient and carers/ family members. They can also be advised to take 4-hourly paracetamol for pyrexia. Tepid sponging, a fan nearby and light loose clothing may also help reduce the body temperature (Dylan & Noble, 2009).
Bone fractures
Cancer and its treatment can compromise bone health, leading to pathological fractures. The skeleton is the most common metastatic site in many cancers, notably breast and prostate cancers (Lipton et al., 2009). Patients with bony metastasis are prone to having low-impact fractures and usually present with sudden, severe pain at the site of fracture. Fractures can be caused by a minor injury or fall, or even everyday activities, due to the weakness of the bone at metastatic sites. In advanced skeletal metastasis, fractures may even result without an injury as the bone crumbles. These fractures must be differentiated from vertebral fractures caused by osteoporosis. Examination shows bony tenderness, sometimes swelling and obvious deformity. The spinal cord, ribs and long bones of the arms and legs are common sites of fracture related to bone metastasis (Lipton et al., 2009).
Active management
A suspected fracture warrants urgent referral to the Accident and Emergency Department for X-ray confirmation. Hospital management may involve temporarily stabilising the joint with a cast and possible surgical correction.
Conservative management
Pain from the fracture site is addressed with adequate analgesia. Severe pain may warrant as and when required (PRN) opioids. The fracture site should be immobilised as much as possible as bone healing is a natural process. Bisphosphonates, such as alendronate or risedronate, help reduce risk of fractures and bone pain as they are powerful inhibitors of osteoclast activity. Denusomab, a human monoclonal antibody, is now increasingly being used for preventing skeletal-related events in patients with bone metastases from breast cancer and from solid tumours other than prostate. Hence, such agents can be used as supportive measures in oncology patients with bone metastasis or existing osteoporosis and osteopenia to reduce risk of fractures.
Major haemorrhage
Bleeding can occur in the form of hematemesis, melaena, haemoptysis, haematuria or directly from wounds in patients with cancer. Malignancy and its treatment may both significantly alter the haemostatic system. Some causes are thrombocytopenia, disseminated intravascular coagulation, coagulation factor abnormalities, platelet dysfunction, vascular defects and the presence of circulatory anticoagulants. Thrombocytopenia usually results from chemotherapy or marrow involvement by a tumour, but is also caused by consumptive coagulopathy, immune-mediated mechanisms, infection, or sequestration. Another major reason for a large bleed is direct erosion of the tumour into vessels, particularly with head and neck, bronchogenic and gastrointestinal cancers. Witnessing and managing major haemorrhage can be a distressful and startling experience.
Active management
Patients with a catastrophic bleed need to be admitted to hospital urgently by calling for an emergency ambulance. Commence BLS in those without prior DNACPR directives. Dark towels may be used to reduce the visual impact of the bleeding and apply direct pressure to bleeding sites.
Conservative management
Major haemorrhage may be a terminal event. A calm approach is required: offer reassurance to the patient and family, using dark towels to reduce the visual impact of the bleeding. For bleeding wounds, direct pressure and adrenaline (1 mg/ml or 1:1000) on a gauze pad can be used in an attempt to vasoconstrict the local vessels.
For smaller bleeds, consider if testing the haemoglobin level will change your management: would iron supplements or a blood transfusion be appropriate in those with a low count for symptomatic relief? Perform a medication review and consider stopping medications that may exacerbate bleeding, e.g. aspirin. The bleeding tendency can be minimised with tranexamic acid 1 g three times daily after weighing the benefits of stopping bleeding against the increased risk of stroke or myocardial infarction with tranexamic acid.
Managing common end of life symptoms
Severe pain
Severe pain in malignancy can be managed pharmacologically or non-pharmacologically. The neurophysiology of cancer pain is complex involving inflammatory, neuropathic, ischaemic and compression mechanisms at multiple sites. Knowledge of these mechanisms and the ability to decide whether a pain is nociceptive, neuropathic, visceral or a combination of all three, leads to optimal pain management. Accurate assessment and reassessment of pain is also important and should incorporate psychosocial assessment and use of quality of life measurement tools.
The World Health Organization (WHO) cancer pain ladder (Figure 2) suggests that opioids remain the mainstay of management of severe pain in cancer patients. Palliative patients are usually on regular opioids as prescribed by their specialists: GPs are often requested to prescribe as required breakthrough doses, which can be administered immediately by Macmillan or district nurses in the community. Breakthrough doses should be a sixth of the total morphine used in 24 hours. For instance, if a patient is using 30 mg of morphine sulphate in a day, the as-required dose of immediate-release morphine, e.g. morphine sulphate solution, will be 5 mg every 4 hours. The frequency may be increased to hourly administration with severe pain.
The long-term consequences of using opioids, such as tolerance, dependency, hyperalgesia and the suppression of the hypothalamic/pituitary axis should be acknowledged and discussed with the patient. In addition to that, well known side-effects, such as constipation should be accounted for when initiating opioid therapy with use of regular laxatives.
Non-steroidal anti-inflammatories, antiepileptic drugs and tricyclic antidepressants can be used as adjuvants. Non-pharmacological techniques, such as cognitive behavioural therapy (CBT), reflexology and hypnosis can give the added benefit (Delaney, 2016).
WHO cancer pain ladder.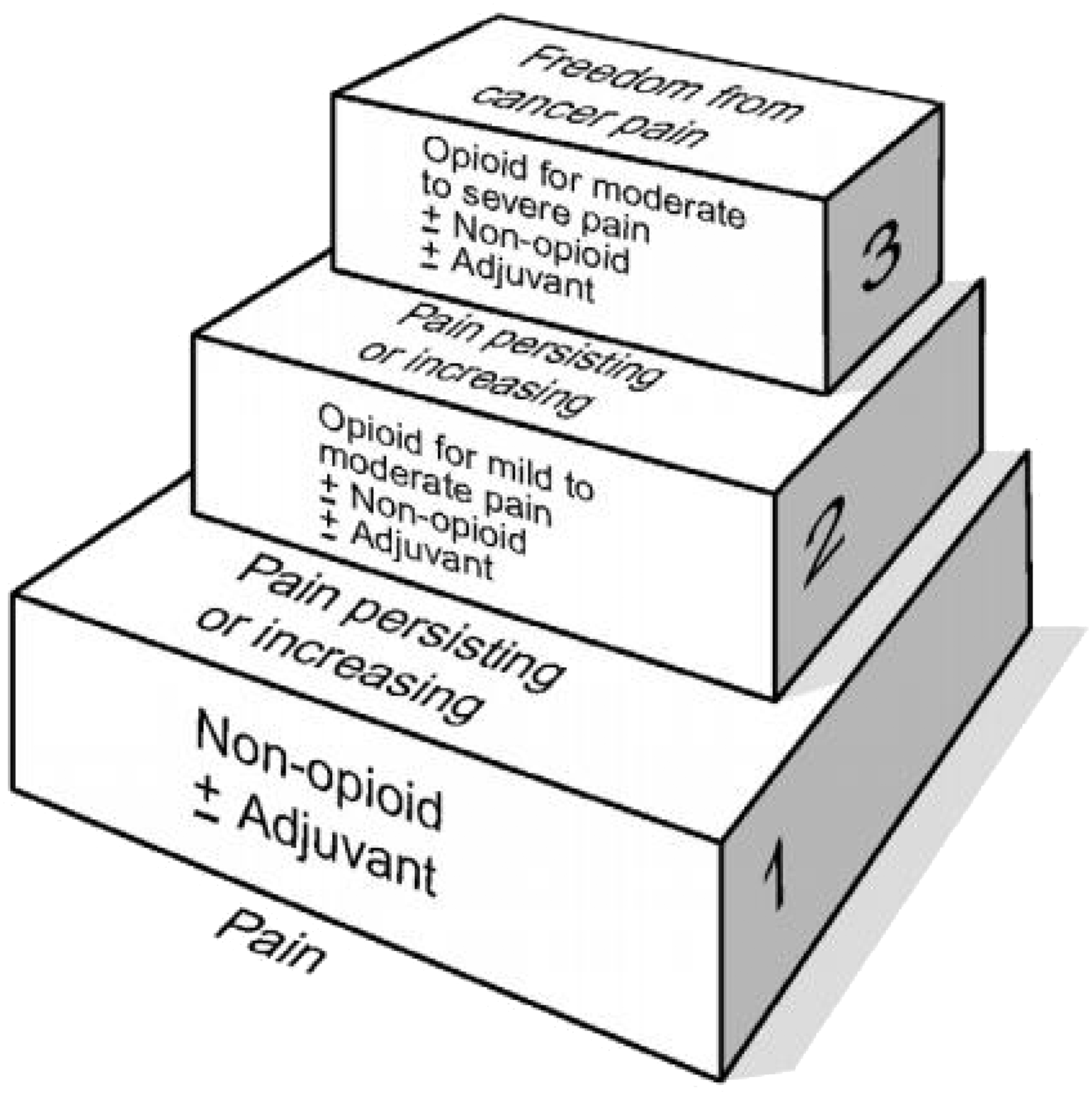
Nausea and vomiting
Simple measures, such as providing a calm environment away from where food is prepared, small palatable meals with high carbohydrate content, and cool fizzy drinks may help alleviate nausea and vomiting. Pharmacological management relies upon the cause of vomiting. For example, haloperidol is the ideal choice for nausea and vomiting caused by drugs and metabolic causes; cyclizine is more appropriate for vestibular causes and raised intracranial pressure. Gastrointestinal (GI) causes of nausea and vomiting need careful evaluation in determining the cause, as well as appropriate therapy: some medicines, like hyoscine butylbromide (Buscopan), are antimuscarinic, which can have opposing effects on the GI smooth muscle compared with prokinetics, like metoclopramide. Metoclopramide is the drug of choice in bowel obstruction and gastric stasis. Levomepromazine works on multiple receptors and so can be used as a second-line agent in almost all cases. Non-pharmacological techniques, such as acupuncture, CBT and relaxation therapies, may offer relief, particularly in those with anxiety and anticipatory nausea (NICE, 2015).
Consider causes that may warrant emergency hospital admission, e.g. complete bowel obstruction and raised intracranial pressure. Poor hydration status and suspected or confirmed metabolic abnormalities may also require hospital admission.
Anxiety and panic
Anxiety is very common during the last days of life and is affected by a combination of physiological, psychological, social and spiritual factors. It may cause panic attacks and breathlessness. Medical conditions, such as chronic obstructive pulmonary disease, pulmonary fibrosis and heart failure, may contribute to breathlessness.
Assessment focuses on exploring the underlying cause and patients’ understanding of reasons behind anxiety, panic or breathlessness, and their impact on functional abilities and quality of life. Potential reversible causes, such as pleural effusion, pulmonary embolism, infection, anaemia or bronchospasm, should be considered and treated. Non-pharmacological management includes smoking cessation, a hand-held fan and open windows to improve ventilation, relaxation and anxiety management techniques. Medical management consists of use of benzodiazepines, opioids, oxygen and inhaled nebulisers.
Anticipatory medication
Common anticipatory drugs.
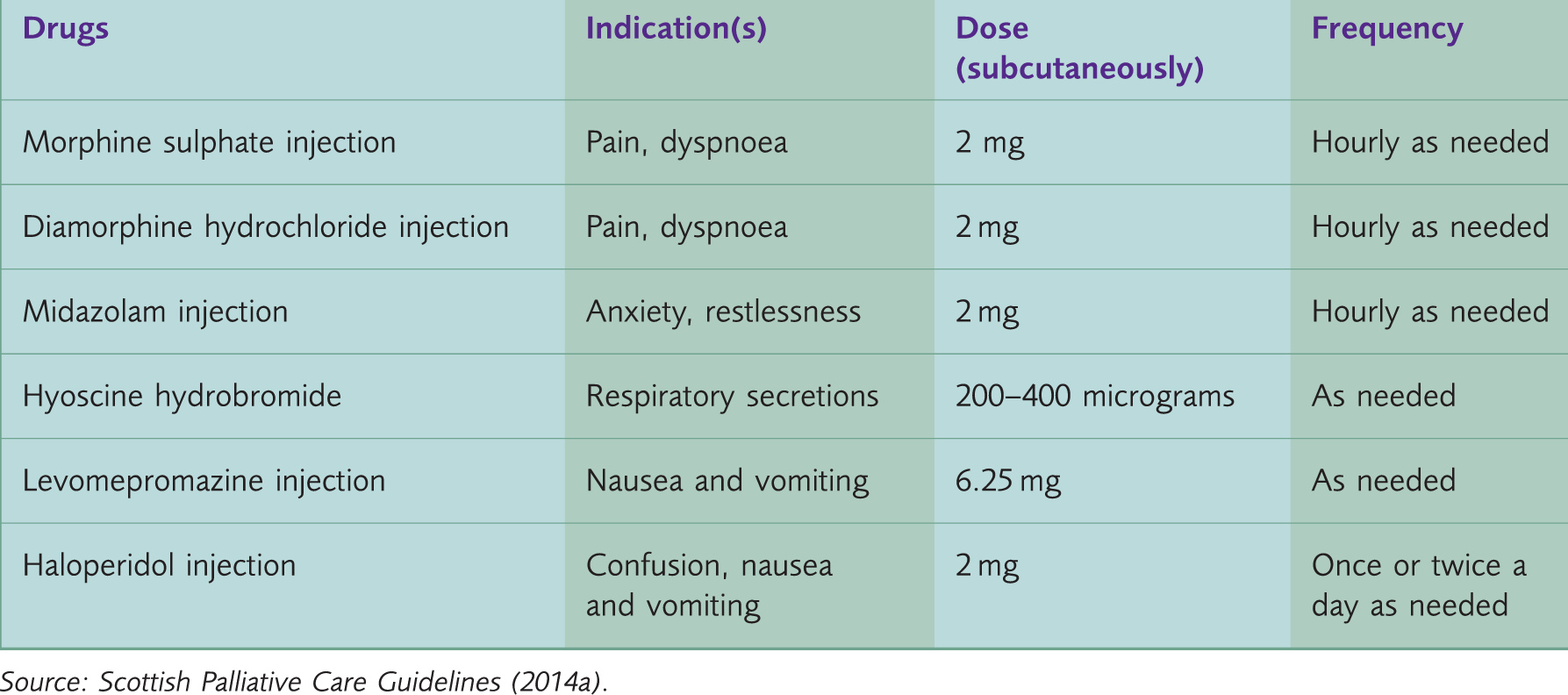
Syringe drivers are used for continuous symptom management over 24 hours in the community and the doses of these drugs prescribed for a syringe driver will be based upon the usage over the last 24 hours.
Resuscitation skills
Medical professionals must keep their resuscitation skills up-to-date as per General Medical Council (GMC) guidance. Patients with a diagnosis of cancer may have advance directives about cardiopulmonary resuscitation, but BLS must be provided in emergencies where appropriate. The Resuscitation Council UK recommends following the approach outlined in Fig. 3.
Adult BLS.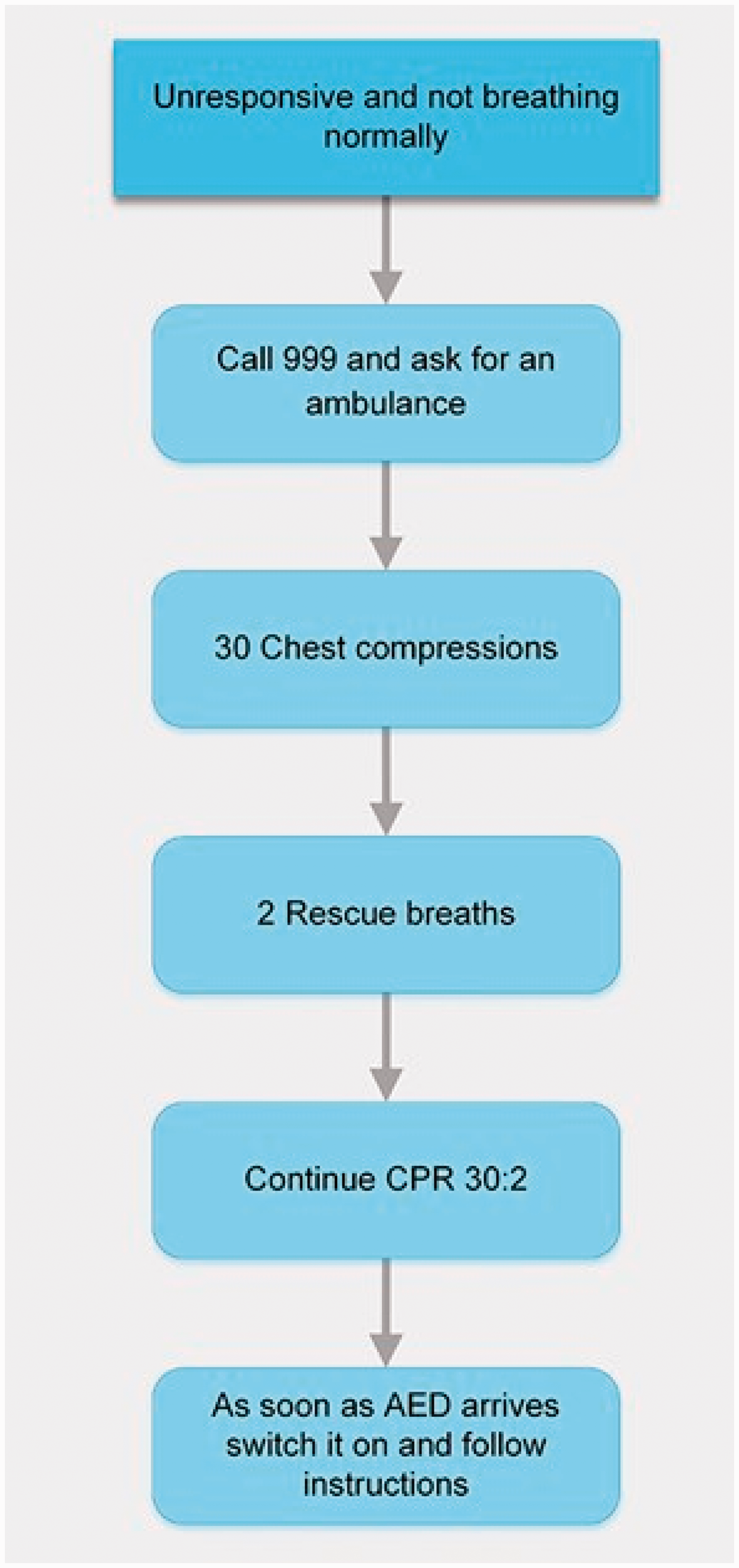
Communication during end of life care
Efficient communication is at the core of general practice, particularly during advanced care planning. Patients with cancer and their carers should have the nature and progression of their illness and prognosis of any complications and treatment thoroughly explained. Given possible long stays in hospitals for treatment such as IV fluids and poor prognosis, it is important that, where possible, patients make informed choices regarding their management. Helping patients to die with dignity and minimal distress is an essential role as a GP.
Key points
GPs should be aware of complications associated with cancer patients that may present as oncology emergencies GPs should be aware of active and conservative management options for these emergencies The level of intervention and management for any oncology emergency depends upon the patient’s advanced care planning and their wishes and goals at the end of life Efficient communication is vital to help a patient make informed decisions about urgent active management or conservative management to aid death with dignity and minimal distress