
Abstract
Colonic diverticula constitute the most common endoscopic anomaly in the Western world. They are responsible for a spectrum of disease. Most presentations associated with colonic diverticula can safely be managed in primary care. The distinction between those patients who are suitable for primary care management and those who require secondary care referral can be difficult to formulate. This article aims to provide a framework, informed by current guidelines, for the management of diverticular disease in primary care, and the identification of patients likely to benefit from referral to secondary care. An overview of the secondary care management of diverticular disease is also provided.
The GP curriculum and diverticular disease
Recognition and immediate management of acute diverticulitis
The assessment of abdominal pain to enable a diagnosis of diverticular disease Understanding the important dietary factors to consider in diverticular disease and offer appropriate dietary advice The epidemiology of digestive problems as they present in primary care, and their often complex aetiology The understanding of secondary care management of diverticular disease
Definitions
A diverticulum is an abnormal blind-ending protrusion of the wall of a hollow viscus. It is termed either a true or false diverticulum, depending on whether it involves all the layers of the viscus or only some of the layers, respectively. Colonic diverticula are false diverticula that are formed by protrusion of only the mucosal and submucosal layers at weak points in the circular muscle of the intestinal wall close to perforating blood vessels (see Fig. 1).
The anatomy of a diverticulum. The association with perforating blood vessels is highlighted in this figure.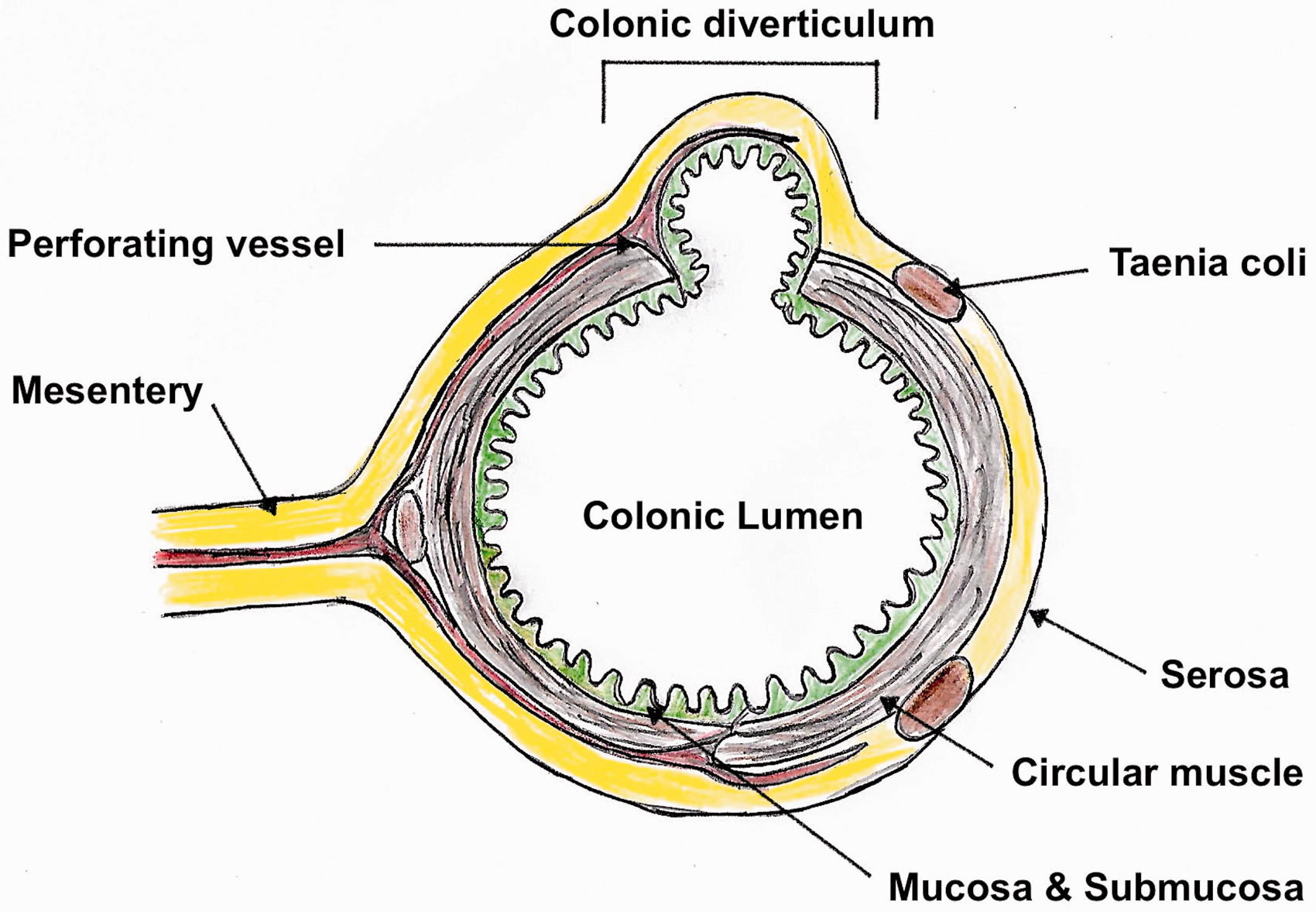
‘Diverticulosis’ describes the presence of diverticula within the colon, but not whether they are clinically significant. A complex interaction between changes in the structure of the colonic wall, alterations in colonic motility, and a range of environmental factors, such as low-fibre diet, are responsible for diverticular disease (Spiller, 2015; Tursi, 2016).
The term ‘diverticular disease’ is reserved for clinically significant colonic diverticula: it includes diverticular haemorrhage, which results from erosion of the arterial wall of perforating blood vessels, and diverticulitis. Diverticulitis is the macroscopic inflammation of diverticula that arises from the interplay between environmental factors, genetics, variations in microbial gut flora, and variations in colonic motility (Tursi, 2016).
‘Uncomplicated diverticulitis’ describes localised inflammation alone, whereas ‘complicated diverticulitis’ refers to situations where inflamed diverticula have progressed to frank peritonitis, intra-abdominal abscess or fistula formation (see Fig. 2). Patients with diverticular disease who smoke and take non-steroidal anti-inflammatory drugs (NSAIDs) are at greater risk of complicated diverticulitis (Hobson and Roberts, 2004). Similarly, immunosuppressed patients have a greater risk of complex disease.
Diverticulitis may be complicated by perforation, fistula formation and abscess formation. Bowel obstruction and haemorrhage (not shown) may also complicate diverticulitis.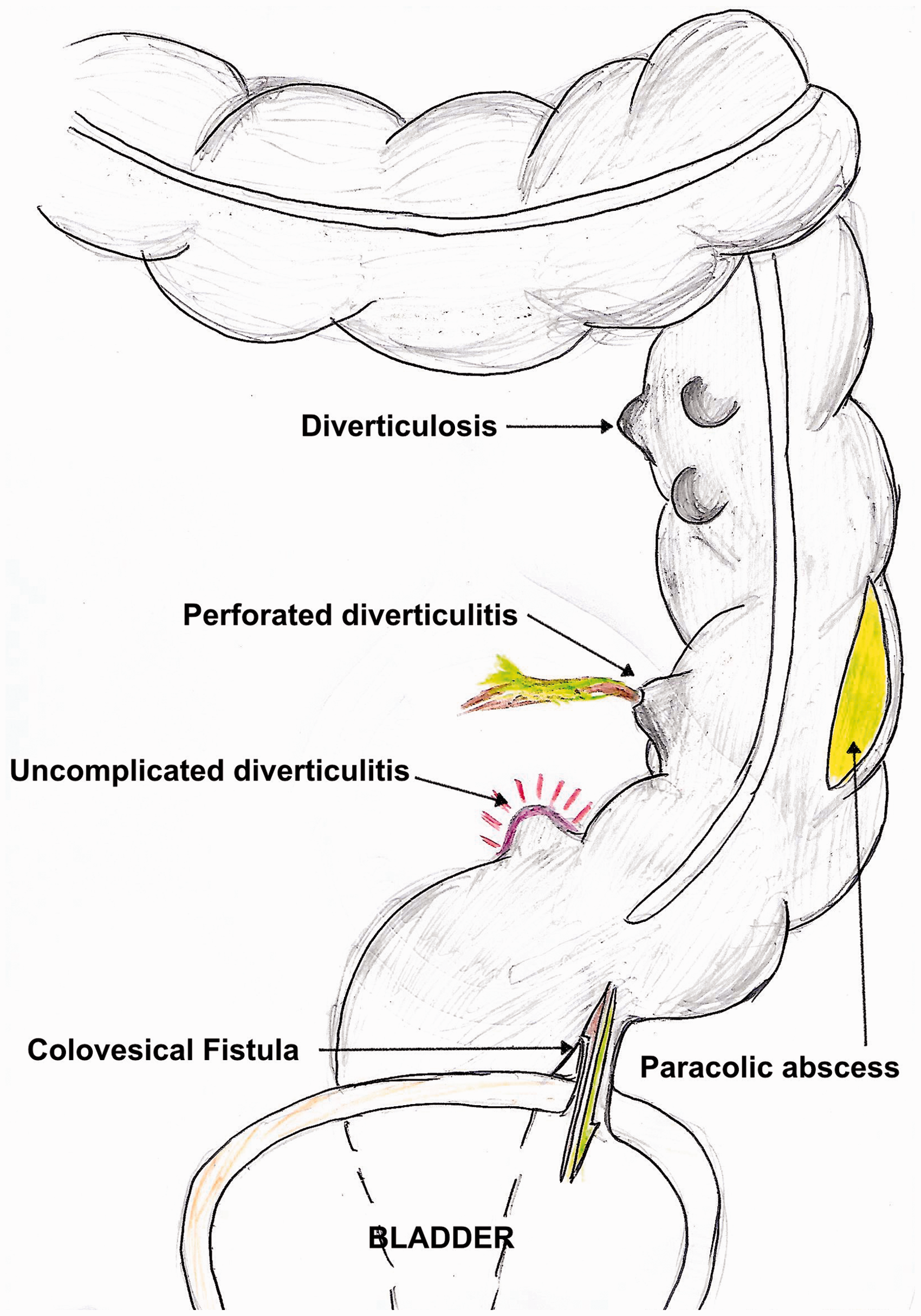
‘Symptomatic uncomplicated diverticular disease (SUDD)’ describes symptomatic diverticulosis in the absence of macroscopic diverticulitis or colitis. The mechanisms that underlie SUDD are currently not well understood. Alterations in gut motility, alterations in the expression of neurotransmitters in the colonic myenteric plexus, and low-grade inflammation may be involved in the pathogenesis of SUDD (Elisei and Tursi, 2016). It is likely that multiple factors interact to cause symptoms in affected patients. Psychological factors have also been shown to play a role in the experience of symptoms (Humes, Simpson, Neal, Scholefield, and Spiller, 2008).
Epidemiology
The development of diverticulosis is particularly common in industrialised nations, it is predominantly a disease associated with increasing age. Post-mortem studies show that diverticula are present in only 5% of patients before the age of 50 years, and in around 50% of patients over the age of 50 years (Hughes, 1969).
Diverticulosis appears to affect the left colon more frequently in Western populations. In Asian populations, right-sided diverticulosis is more common. The exact mechanisms for this are unclear.
There has been a change in the distribution of diverticulosis between the sexes. Initially there was a male preponderance, but in more recent studies there is an equal distribution in male and female patients (Tursi, 2016).
Progression from diverticulosis to diverticular disease occurs in around 20% of patients (Elisei and Tursi, 2016). Most patients with symptomatic disease appear to suffer from SUDD. Based on a large American study, only about 4% of patients with diverticulosis appear to suffer from diverticulitis (Shahedi et al., 2013), and diverticular haemorrhage occurs in 5–15% of patients (Sugihara et al., 2016).
Clinical presentation
Diverticulosis
Most patients with diverticulosis remain asymptomatic. They may only be discovered during the investigation of other conditions, such as an incidental radiological or endoscopic finding.
SUDD
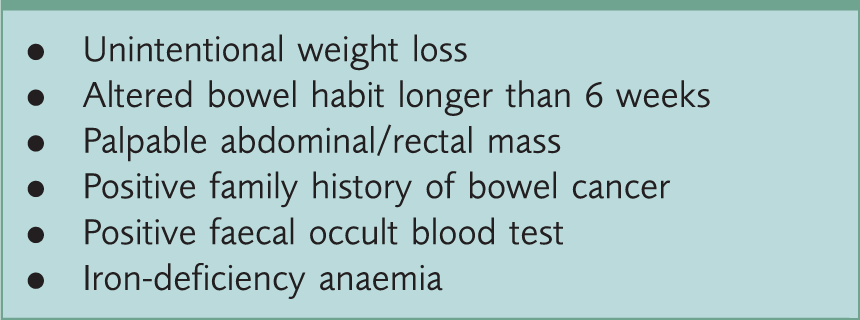
Red flag features.
Clinical features of the systemic inflammatory response syndrome (SIRS) include tachycardia, tachypnoea and pyrexia greater than 38℃. These symptoms are not consistent with a diagnosis of SUDD. Similarly, features of peritonism with, for example, abdominal guarding, suggest an alternative diagnosis. In SUDD the inflammatory markers, such as C-reactive protein (CRP) and white cell count, will be within normal limits.
There are no clear guidelines on the distinction between IBS and SUDD. Indeed, some authors suggest that diagnosis is often based on the discretion (or bias) of the clinician (Wensaas and Hungin, 2016). There is, however, some evidence that faecal calprotectin levels might be elevated in SUDD, thus differentiating SUDD from IBS (Tursi, 2016). However, there is no current guidance on faecal calprotectin levels in the diagnosis of SUDD.
Diverticular bleeding
Diverticula are a common cause of massive gastrointestinal haemorrhage. If identified in primary care, these patients will require resuscitation and emergency hospital admission. Less-severe rectal bleeding can occur in diverticulosis, and is often the only symptom. In the absence of any obvious ano-rectal pathology, and in the presence of red flag symptoms, most patients will require further investigation in accordance with both the British Society of Gastroenterology commissioning guidelines (British Society of Gastroenterology, 2009) and the more recent guidelines for suspected cancer by the National Institute for Health and Care Excellence (National Institute for Health and Care Excellence (NICE), 2015).
Acute diverticulitis
Clinical features tend to mirror the severity of the disease process. Uncomplicated acute diverticulitis is characterised by left-sided lower abdominal pain that responds to oral analgesia. The patient may also complain of nausea, altered bowel habit, and fever.
In uncomplicated acute diverticulitis, abdominal examination will reveal marked tenderness in the left lower quadrant. This is often associated with features of localised peritonism, such as guarding. Features of overt SIRS, such as tachycardia and tachypnoea, should be absent.
Features in the clinical history that indicate a greater risk of progression to severe disease include the presence of significant comorbid disease, physical frailty and the presence of immunosuppression. Patients who are unable to tolerate oral fluids, and patients with any adverse social circumstances, are not ideal candidates for primary care management.
A history of urinary frequency or dysuria can point to disease complicated by pelvic abscesses or colovesical fistulae. In addition, the distressing symptoms of pneumaturia or faecuria are also associated with the presence of a fistula between the colonic wall and the bladder.
In more advanced disease, features of SIRS with more severe abdominal signs will be evident. The absence of bowel sounds on auscultation together with generalised tenderness and guarding indicate generalised peritonitis.
Management in primary care
Diverticulosis
Asymptomatic patients may be found to have diverticulosis as an incidental finding on investigation for another problem. Such patients will benefit from lifestyle advice and explanation of the investigation findings. The Royal College of Surgeons of England (RCSEng) and NICE both recommend that patients with diverticulosis maintain a high fibre intake (18 to 30 g per day) and also an adequate fluid intake (NICE, 2013; RCSEng, 2014). There is no recommendation for further follow-up in this cohort of patients.
Current guidance does not recommend other lifestyle or dietary changes, but there is evidence that smoking, alcohol intake, obesity, and use of NSAIDs are important factors in disease progression. It may be helpful to address these factors when consulting with patients who have asymptomatic diverticulosis. Eating nuts and popcorn is no longer considered likely to precipitate diverticulitis (Tursi, 2016).
Some patients may be concerned that diverticulosis is associated with colorectal cancer; however, such an association does not appear to exist (Regula, 2009). However, it is important to be alert to red flag symptoms (see Box 1) as the two conditions can co-exist.
SUDD
Patients with the confirmed presence of diverticula who present with symptomatic disease should also be advised to maintain a high fibre intake. If dietary modification alone does not improve symptoms, then supplementation with bulking laxatives (e.g. ispaghula or methyl-cellulose) is recommended.
Analgesia should be limited to paracetamol, given the potential of NSAIDs to increase the risk of diverticular complications, and of opiate drugs to alter gut motility. Referral to secondary care should be considered for patients when paracetamol does not control pain, when quality of life is impaired or when there is diagnostic uncertainty. Surgery is unlikely to be indicated for patients with SUDD and gastroenterology referral is likely to be more appropriate.
NICE guidelines do not support the use of antispasmodics in the primary management of SUDD (NICE, 2013). However, the crossover between SUDD and IBS is acknowledged, and if after a month symptoms persist, then a trial of IBS treatment may be initiated.
The role of psychological factors in SUDD is less clear than for IBS. There are currently no trials on the use of antidepressants or psychological interventions in the treatment of SUDD.
Recent studies have suggested a role for antibiotics (rifaximin), mesalazine and probiotics in the control of SUDD symptoms (Elisei and Tursi, 2016). However, this approach is not recommended within current guidance on the management of SUDD.
Acute diverticulitis
Uncomplicated acute diverticulitis can be managed in primary care, but this depends on the differentiation of complicated from uncomplicated diverticulitis and recognition of those patients at risk of developing severe disease (Fig. 3). Patients with no co-morbid disease, who can safely maintain oral hydration and are not immunosuppressed, may be suitable for management in primary care. Urgent admission is required for patients with signs of sepsis or complicated diverticulitis.
A flowchart proposed for the management in the community of uncomplicated acute diverticulitis.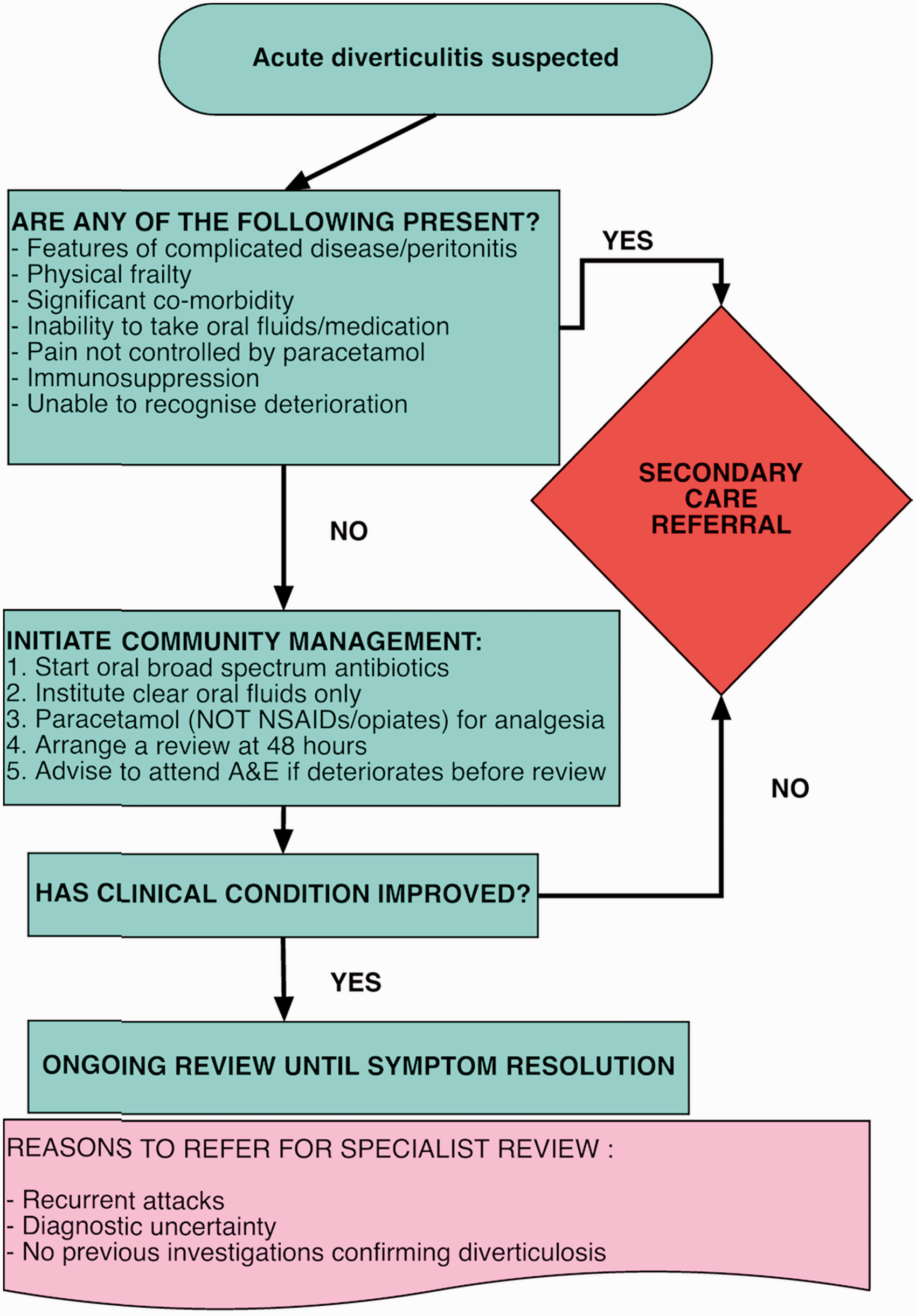
The evidence supporting a role for antibiotics in the management of uncomplicated acute diverticulitis is surprisingly limited. One Swedish multicentre randomised trial (Chabok, Påhlman, Hjern, Haapaniemi, & Smedh, 2012) showed no significant differences in both length of hospital stay and complication rates between patients treated with antibiotics and those treated without antibiotics. These findings have been supported by another more recent multicentre trial in the Netherlands (Daniels et al., 2017). It is not yet clear how these results would translate into primary care management.
Despite this emerging evidence, NICE (NICE, 2013) continues to advocate a 7-day course of broad-spectrum antibiotics to cover anaerobes and gram-negative bacilli (e.g. Co-amoxiclav or if penicillin allergic ciprofloxacin and metronidazole). This guidance is echoed by the RCSEng guidance (RCSEng, 2014).
Analgesia is limited to paracetamol, and patients are encouraged to take clear fluids only for the first 48 hours to ‘rest’ the bowel. Patients can then take solid foods if symptoms improve.
Review of progress after 48 hours is necessary. If the patient has failed to respond or deteriorates before review, then emergency surgical admission is required.
Current guidelines recommend that patients responding to community therapy with a proven diagnosis of colonic diverticula can be managed in the community and do not require referral to secondary care. However, if symptoms are recurrent, in patients without a proven diagnosis of diverticula or when there is diagnostic uncertainty, outpatient surgical referral and further investigation is strongly recommended (RCSEng, 2014).
Management of acute diverticulitis in secondary care
An outline of the management of acute diverticulitis in secondary care can be helpful when informing patients who are being admitted and to inform subsequent management after discharge from hospital. Detailed guidelines on secondary care management are published by the Association of Coloproctology of Great Britain and Ireland (Fozard, Armitage, Schofield, and Jones, 2011).
Initial resuscitation
Patients presenting as an emergency in secondary care are assessed and resuscitated based on the ABCDE algorithm. Intravenous fluids and analgesia are likely to be required. SIRS or sepsis will require treatment with broad-spectrum intravenous antibiotics.
Investigations
Secondary care investigations may reveal a leucocytosis and an elevated CRP. Renal function may be abnormal, particularly with severe dehydration. Arterial blood gas analysis is important in sick patients, and a serum amylase is checked to exclude a diagnosis of pancreatitis.
In secondary care, early radiological diagnosis is important (Fozard et al., 2011; RCSEng, 2014). Plain erect chest radiographs may show evidence of pneumoperitoneum in patients with an unconfined perforation. Abdominal radiographs help exclude diagnoses such as sigmoid volvulus, and can in some cases also provide evidence of pneumoperitoneum.
Contrast-enhanced computed tomography (CT) provides the best diagnostic evidence of acute diverticulitis and diverticular complications. In the past, patients with signs of frank peritonitis proceeded directly to theatre after only basic bedside investigations, but it is now unusual for patients to avoid CT.
Medical management
Patients without overt signs of peritonism generally respond to treatment with bowel rest and intravenous antibiotics. Solid food is reintroduced normally after 48 hours if the clinical condition is improving. Progress is assessed clinically and with reference to serum inflammatory markers.
Radiological management
Around 15% of patients with acute diverticulitis develop intra-abdominal abscesses. Isolated abscesses of less than 5 cm diameter tend to respond to antibiotic therapy alone. Larger abscesses or multiple abscesses, however, require drainage. The advent of interventional radiology has permitted many patients to undergo percutaneous drainage. Although not without risk, this reduces exposure of the patient to the risks of general anaesthesia and open surgery.
Typically, if an abscess is amenable to percutaneous drainage, the drain will remain in situ until there is minimal drainage. If the patient’s clinical condition improves, the patient can often be discharged without further intervention. Some patients may be discharged and followed up with a drain in situ. Occasionally such patients will be encountered in primary care.
Emergency surgical management
Patients who have developed diverticular abscesses that are not amenable to percutaneous drainage, and patients with frank peritonitis, will require operative management. In centres where a 24-hour interventional radiology service is unavailable, and when patient transfer to such a centre is not possible, surgical intervention may also be required.
Traditionally, the operation of choice for peritonitis secondary to diverticulitis was a midline laparotomy, excision of the diseased segment of sigmoid colon, and the formation of a colostomy with the proximal portion of viable bowel (Hartmann’s operation - see Fig. 4). Indeed, in unstable or frail patients this can be a life-saving operation. The possibility of stoma reversal is considered during outpatient follow-up by the surgical team and the patient.
The classic Hartmann’s operation involves excision of the diseased sigmoid and the fashioning of an end colostomy. The rectal stump is over-sewn and left in-situ.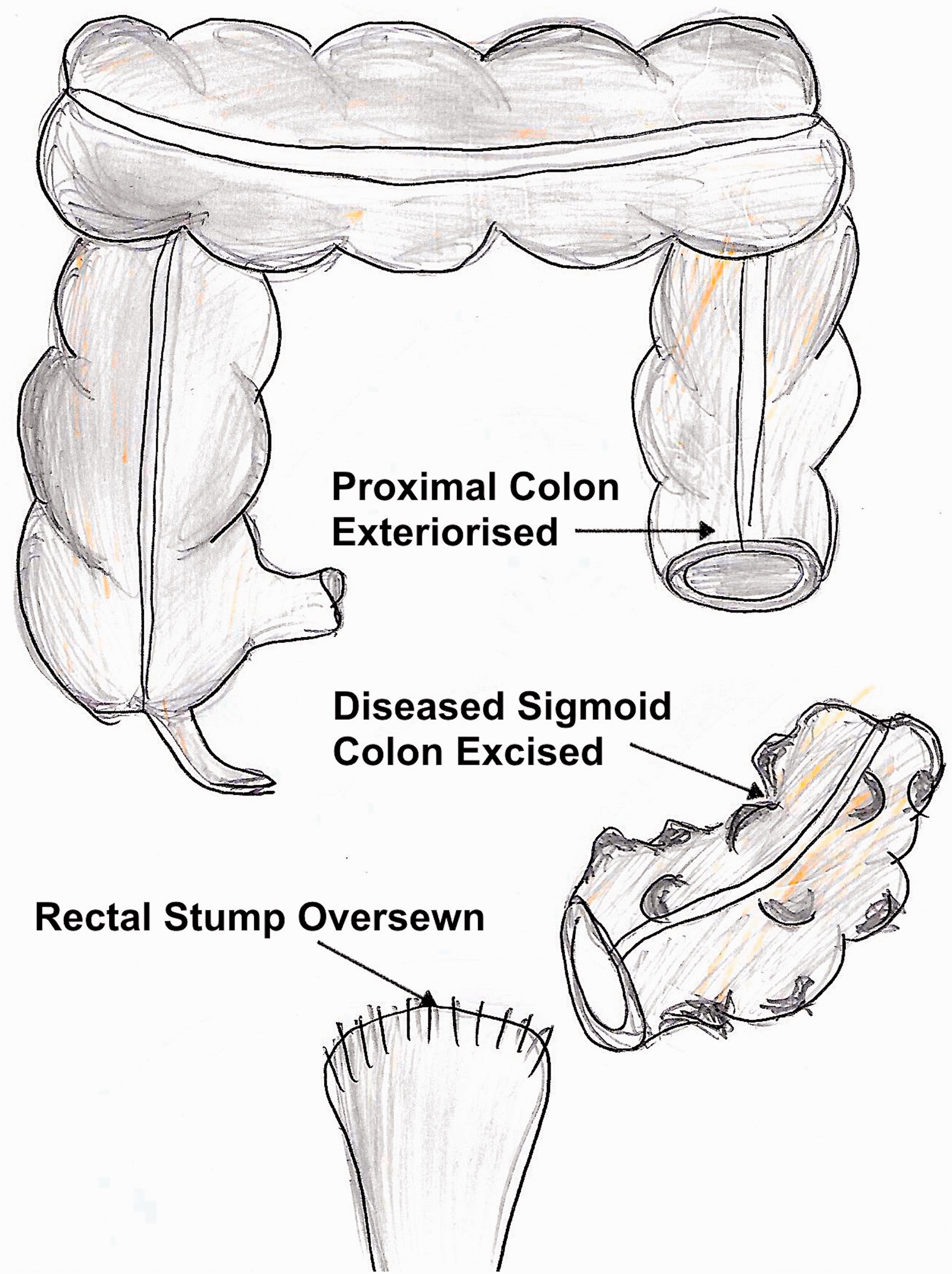
A wider variety of emergency surgery is now performed, including resection of the diseased segment together with a primary anastomosis, laparoscopic washout of the abscess cavity and laparoscopic resection of the diseased sigmoid colon. The choice of operation will depend on patient factors and the available surgical expertise (RCSEng, 2014).
Elective surgical management
Patients who develop fistulous tracts secondary to diverticular disease may be considered for elective surgery unless they are very high risk. Those who experience recurrent attacks of diverticulitis may be considered for elective surgery to remove the diseased colonic segment. The evidence for benefit is inconclusive (Fozard et al., 2011).
Key points
Diverticulosis and diverticular disease are common in Western populations Dietary advice and lifestyle modification are the mainstay of treatment for uncomplicated diverticular disease Uncomplicated acute diverticulitis can be safely managed in the community in selected cases Patients with no red flag features, but with persistent symptoms and diagnostic uncertainty, should be referred for specialist assessment and further investigation Urgent admission is required for patients with signs of sepsis or complicated diverticulitis