
Abstract
The majority of the UK population becomes sexually active in their teenage years. At that point, many present anxiously to their GP for advice, contraception or with an unplanned pregnancy. This article considers our legal and ethical responsibilities, special considerations in history taking, a young person’s health concerns and the declining, but still significant, incidence of teenage unplanned pregnancy.
The GP curriculum and contraception for teenagers
Describe the legislation relevant to women’s health (e.g. abortion, contraception for minors) Appreciate the definition of sexual health as being about the ‘enjoyment of the sexual activity you want without causing yourself or anyone else suffering or physical or mental harm’. It is also about contraception and avoiding infection Know when urgent intervention is needed in sexual health and, if necessary, refer appropriately, e.g. in the provision of emergency contraception
Legal and ethical considerations
The age of consent to sexual activity in the UK is 16 years; however, around one-third of teenagers will already then be sexually active. Although unlawful, mutually agreed sexual activity between persons of similar age will not typically result in prosecution, unless there is evidence of abuse or exploitation. In England, Wales, and Northern Ireland, those under 13 years in age are considered unable to consent to sexual intercourse. In Scotland, sexual activity with a person under 13 years of age is regarded as ‘rape of a young child’ (Faculty of Sexual and Reproductive Healthcare (FSRH), 2010a).
Confidentiality
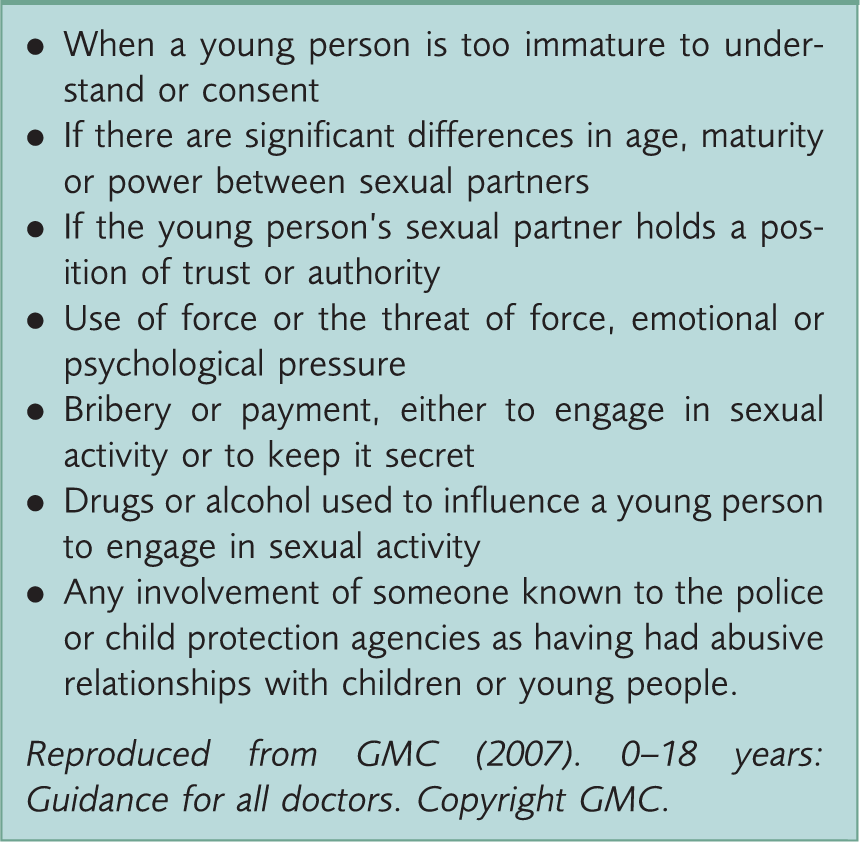
Examples and indicators of an abusive or harmful sexual activity.
Consent
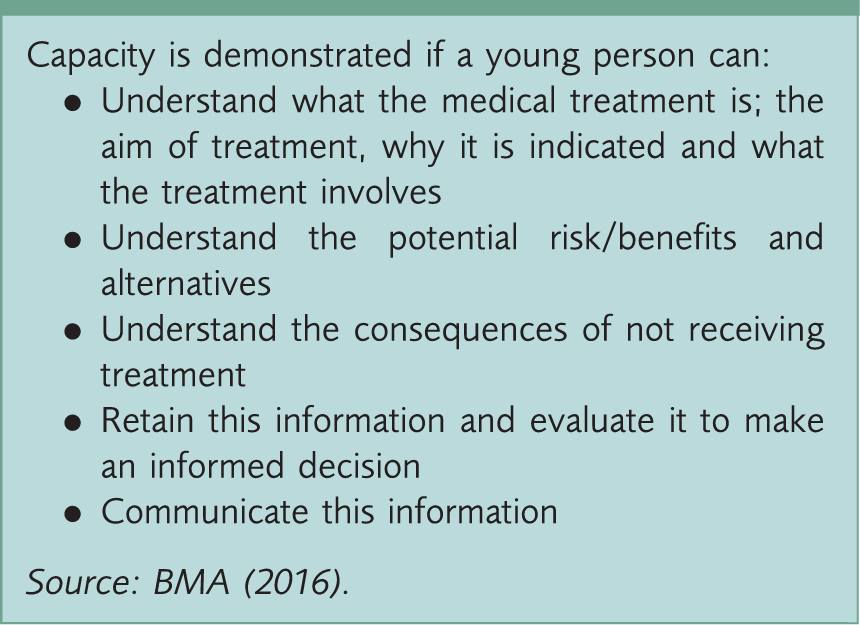
Capacity.
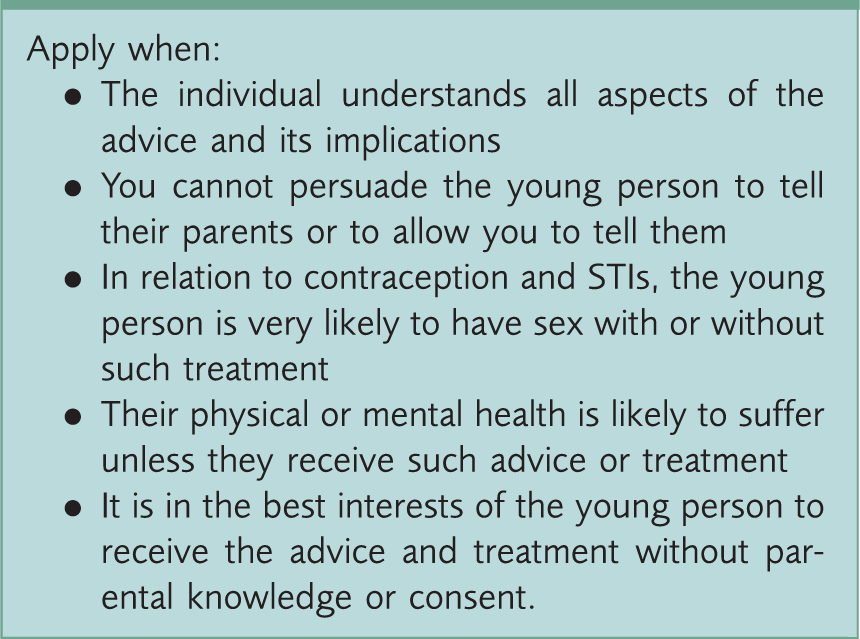
Fraser guidelines.
In Scotland, the Fraser guidelines and ‘Gillick competence’ are often discussed; however, they have no authority in Scottish Law. Scottish legislation states the only criterion for consent is that the child understands the nature and consequence of treatment (BMA, 2016).
If you have concerns regarding a young person, advice should be sought from colleagues, local child protection leads and your medical defence organisation. It is good clinical practice to tell the young person that you are going to share information with another agency.
Availability
Contraception is available from a range of sources: specialist family planning clinics, GPs, specialist outreach clinics at young people’s centres (varies with geographic location). We should ensure services are convenient and accessible to young people in terms of timing and location (as they may wish to come alone after school). Approachable, friendly, non-judgemental staff are the key to providing effective contraception services. This positive approach to sexual health from health professionals improves patient self-esteem, motivation and achievement.
History taking
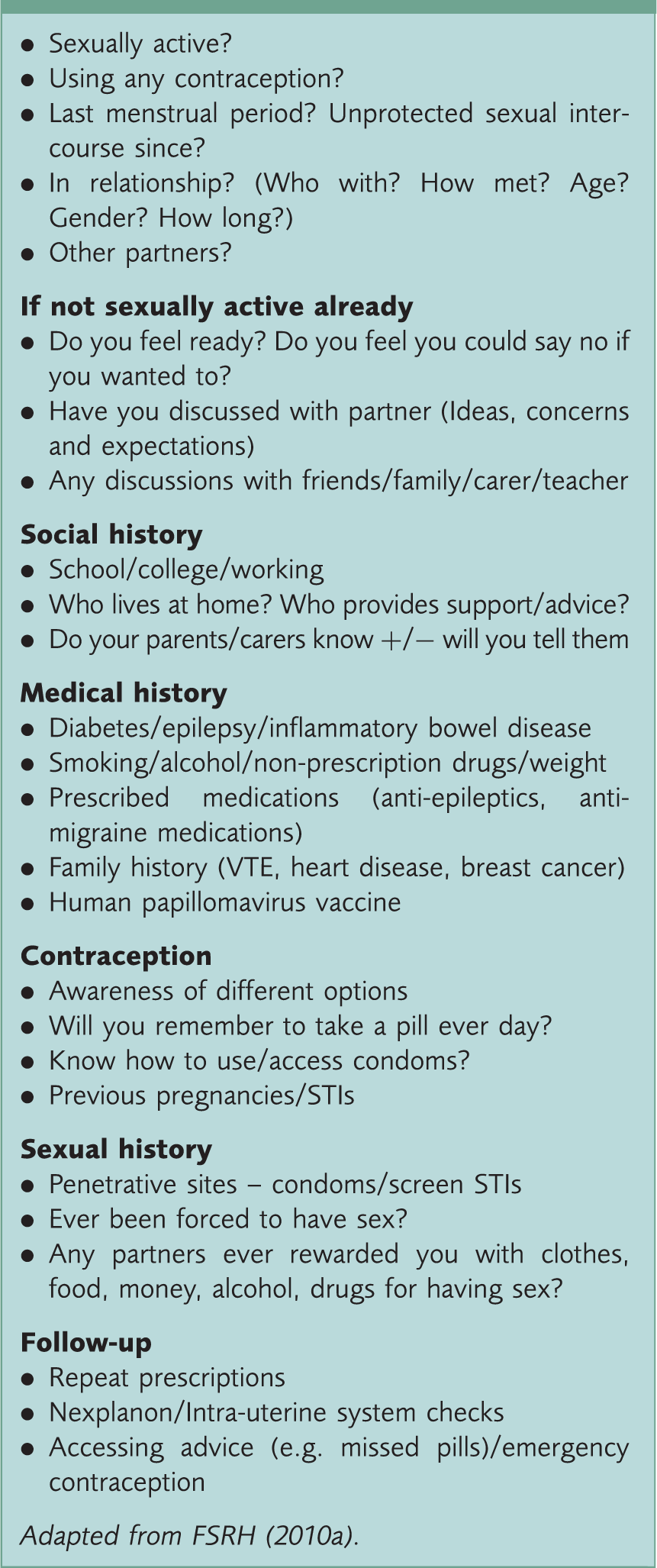
History taking.
Contraceptive choices
In 2008–09, 43% of sexually active women aged between 16 and 19 years were not using any contraception. Of those that were, the most common choices were contraceptive pill (54%) and condoms (65%) (respondents were allowed more than one response) (Office for National Statistics, 2009).
Prior to menarche, condoms are the recommended contraceptive choice. Progestogen-only emergency contraception can be prescribed pre menarche if required (FSRH, 2010a). After menarche, young women can choose their preferred method of contraception provided there are no medical contraindications (United Kingdom Medical Eligibility Criteria (UKMEC), 2016).
Patients present with wide variation in contraceptive knowledge and preferences. Time should be spent establishing baseline information without presuming young people are aware of all contraception choices. Factors influencing contraceptive choices include effectiveness, anecdotal advice, safety, side-effect profile, discreetness, self-control, understanding of method, accessibility, ease of compliance. We should be mindful that our own assumptions on contraception or the views of practitioners providing specific services (such as implant or coil fitting) do not impede the consultation. For example, some practitioners prefer not to fit intrauterine devices in nulliparous women but there is no contraindication. Each individual woman should be given the full choice of contraceptive options unimpeded by false assumptions about what patients may or may not want.
Long-acting reversible contraception (LARC) options are less user-dependent and have lower failure rates. As such, these should be discussed and highlighted with young people. For example, with typical use oral contraceptives are associated with a 9% failure rate and condoms with an 18% failure rate compared with 0.05% for a progestogen-only implant (UKMEC, 2016). Real-size demonstration models of implants and coils may be useful to some patients during the consultation. Some patients may wish to take time to consider their options. These patients should be offered patient information leaflets or advised about online resources such as the Family Planning Association (www.fpa.org.uk/) or Brook (www.brook.org.uk/your-life/category/contraception). Patients may have individual preferences shaped by access to information. A review appointment to review choices, perhaps with partner or parent/carer may be appropriate. Where there are concerns that a patient may not re-present, consider ‘quick starting’ as discussed later in this article.
Young people’s health concerns and risks
Increasing use of social media by young people may bring heightened exposure to claims of side effects and risks associated with contraception use. We will discuss common health anxieties and current evidence to help us educate patients and facilitate decision-making.
Thrombosis
Recent publicity has again highlighted the venous thromboembolism (VTE) risk with combined hormonal contraception (CHC). Young people should be aware that there is a slightly increased risk, although absolute risk remains very small (5-12 per 10 000 women years). An individual may already be at an increased VTE risk, due to immobility, obesity, pre-existing medical conditions or family history and therefore CHC may be contraindicated. Specific guidelines are available in UKMEC (FSRH, 2010a; UKMEC, 2016)).
Weight gain
Patients can be reassured that some weight gain during reproductive years is normal, and is associated with eating and lifestyle changes. There is no clear evidence that CHC use promotes weight gain. Depot medroxyprogesterone acetate (DMPA) may be associated with a 2–3 kg weight gain over a 1-year period; the effect is greatest in those with a body mass index greater than 30 kg/m2 pre-treatment. Other progestogen-only methods are not associated with weight gain (FRSH, 2010a).
Acne
Acne is common in the teenage population. CHC may improve acne. If there is no improvement consider switching to a less androgenic progestogen or a higher oestrogenic content. Co-cyprindiol combines a higher oestrogen component with less androgenic progestogen; it is licensed for severe acne that has not responded to antibiotics, it is not licensed for contraception alone. Patients prescribed co-cyprindiol should have clear documentation of discussion of higher VTE risk and should be reviewed regularly. Studies suggest the VTE risk is 1.5 to 2 times higher with co-cyprindiol than CHCs with levonorgestrel, but similar to the risks associated with third-generation progesterones (Medicines and Healthcare products Regulatory Agency, 2013). Treatment should be discontinued 3 to 4 months after the condition has resolved. The progestogen-only implant may be associated with an improvement, worsening or onset of acne. Acne is not associated with DMPA, but there is a slight increase in acne reported with the use of an intra-uterine system (IUS) (FSRH, 2010a).
Mood changes
Mood changes are subjective and individual. There is no evidence that hormonal contraception causes depression, however, in clinical practice, mood changes are associated with discontinuation of the CHC and progesterone-only pill (POP) (FSRH, 2010a).
Fertility
Only DMPA is associated with a delay in return of fertility for up to 1 year after discontinuation of DMPA. There is no delay in return of fertility with CHC, POP, progestogen-only implant and IUS methods (FSRH, 2010a).
Altered bleeding patterns
Pre-treatment counselling should involve discussion of menstrual changes. This can reduce patient distress and reduce subsequent consultations rates. Altered bleeding is common with progestogen-only methods and should be highlighted. CHC is beneficial in treating dysmenorrhoea and allows some control of bleeding by omitting the pill-free period. Altered bleeding on CHC may be more clinically significant, as it may be associated with missed pills, STIs and malabsorption (FRSH, 2010a). Guidance on unscheduled bleeding in women using hormonal contraception is available from FRSH (Royal College Obstetrics Gynaecology (RCOG), 2009).
Bone density
A Cochrane review concluded that CHC did not affect bone mineral density (BMD), but that DMPA may reduce BMD. This is of greatest concern in women under 18 years of age who may not have reached peak bone mineral mass. The small loss in BMD is usually recovered after discontinuation. The FRSH concludes that the DMPA may be considered for use by patients under the age of 18 years after all other options have been discussed or trialled and found to be unsuitable or unacceptable (FSRH, 2010a).
Cancer
CHC is not associated with an overall increased cancer risk. There may be a very small increased risk in cervical cancer with prolonged CHC use and a small increased risk of breast cancer, but the risk of breast cancer reduces after stopping treatment. The risk of ovarian and endometrial cancer is slightly reduced (FSRH, 2010a).
Follow-up
When initiating contraception, a 3-month review appointment should be offered. This gives an opportunity to address side effects, questions they have been too embarrassed to discuss and health promotion. Review may also improve compliance and reduce contraceptive failure rate. This is also an opportunity to discuss condoms and STI risk/screening.
Quick starting
Young people may be offered ‘quick starting’, which involves starting the oral contraceptive immediately instead of waiting until the start of their next menstrual period. This may be continued indefinitely or used as a bridging method until a LARC appointment can be scheduled. It may be used after emergency contraception. Patients should be counselled to use barrier methods until their contraceptive becomes active. Further detailed clinical information about quick starting and other contraceptive types is available from FRSH (FSRH, 2010b).
Emergency contraception
In 2008–09 17% of women aged between 16 and 19 years had used emergency contraception at least once in the preceding year (Office for National Statistics, 2009). Unfortunately, more recent figures are unavailable due a change in the way the information is recorded (general practice data is not included).
Emergency contraception.
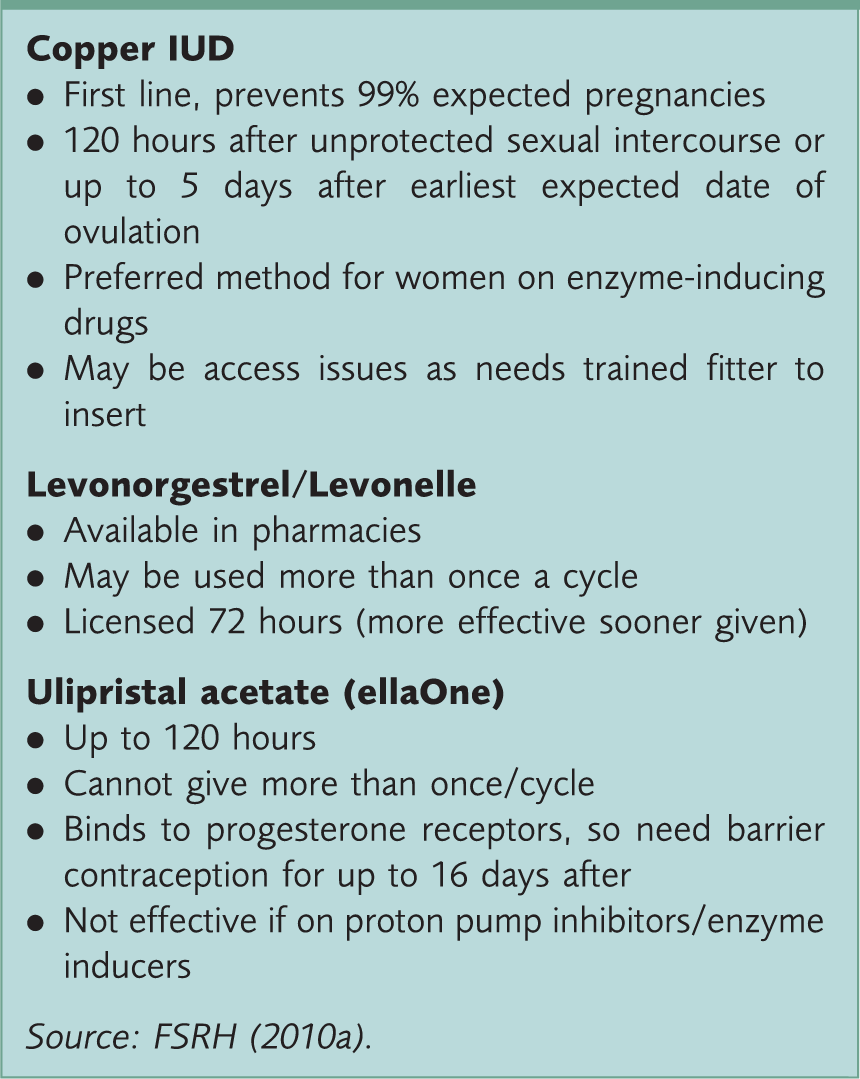
Any women presenting after an episode of unprotected sexual intercourse should be advised to have STI tests at 2 and 12 weeks. Opportunistic discussion of condom use/accessibility and contraception can help prevent further presentations. Condoms can be offered during the consultation.
Teenage pregnancy
Enhanced sexual health education and improved access to services promoted by the Government’s Teenage Pregnancy Strategy are thought to have contributed to the reduction in teenage pregnancy rates. Societal changes with increased educational and working aspirations of young women and the stigma associated with teenage pregnancy have also provoked change. In England and Wales, in 1998 the conception rate in under 18 year olds was 46.6 per 1000, whereas in 2015, the estimated number of conceptions to women aged between15 and 17 years was 21 per 1000 women, a reduction of 55% (Office for National Statistics, 2017). The number of teenage mothers in education, employment or training has risen from 22% to 33% (Department of Health, 2010).
In Scotland, teenage pregnancy rates continue to reduce; from 7.8 per 1000 in 2007 to 4.2 in 2014 for under 16 year olds and from 41.9 per 1000 in 2007 to 22.1 in 2014 for under 18 year olds. Termination rates in the under-16-year age group remain higher than the delivery rate (Information Services Divisions, 2016). These figures remain higher than most of Western Europe.
Risk factors for teenage pregnancy.
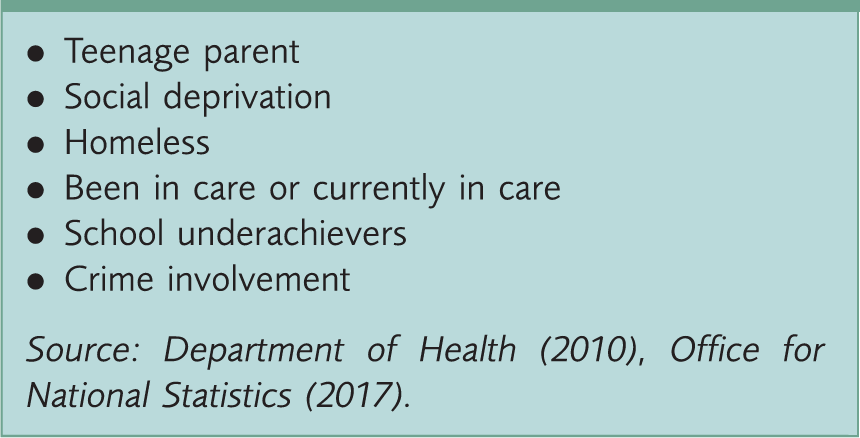
When a young person presents pregnant, a discussion of ideas, concerns and expectations, partner involvement, parent/carer involvement and their options is important. Although there are significant adverse events associated with teenage pregnancies (Table 1) avoid promoting the feeling that this is ‘the worst thing ever’; it does not have to to mean ‘game over’ for their own life and aspirations. This can be achieved with supportive, non-judgemental communication and understanding of the patient’s perspective.
Adverse effects of teenage pregnancy.

Source: Department of Health (2010), Office National Statistics (2015).
Key points
Presenting to the GP can be a daunting experience for any young person wanting to discuss contraception and requires the GP to have particular awareness, knowledge and skills Contraceptive options for young people post menarche are the same as for all women, but careful attention is needed when gathering information and giving advice Special vigilance is required to identify young people in need of advice on sexual health and contraception Routine consultations about contraception provide an opportunity to promote a healthy sex life and to discuss STIs and the risks of teenage pregnancy It is important not to assume prior knowledge of contraceptives when giving advice and to confirm knowledge and understanding Young people may have particular worries about the specific side effects and risks of contraception that need to be explored and addressed