
Abstract
Exercise is beneficial to health. Exercise can be undertaken by the majority of people and completed almost anytime and anywhere. To some it may be enjoyable and rewarding, to others daunting and alien. Regardless of how physical activity is perceived, we know that despite a multitude of health benefits, we are not doing enough. This article will explore the specific health benefits of physical activity, the current national recommendations and how we might get more of our patients to exercise regularly.
The RCGP curriculum and exercise promotion
The role of the GP in the population health: promoting health and preventing disease clinical topic guide includes:
Taking part in health improvement, health protection health services, for example by promoting healthy living, delivering screening and immunisation programmes, and using resources and services appropriately Understanding the social determinants of health, from pre-birth to old age Assessing the needs of local population groups Advocating measures that promote good health in populations as well as individuals Addressing health inequalities Assessing and communicating risk Promoting health in populations; GPs will need to keep up to date with a growing number of population health issues Knowledge of the multiple determinants of health, including the socio-economic, political and cultural factors affecting lifestyle choices Knowledge of the impact on health of factors such as alcohol and substance misuse, poor diet, smoking, inadequate exercise and risky sexual behaviour (including in pregnant women, people with mental ill health, and other vulnerable groups) Using different approaches to behaviour change; understanding their relevance to health promotion and self-care Taking action to address lifestyle factors that affect health (e.g. nutrition, sleep, physical activity) and implementing behaviour change Knowledge of clinical, social, and environmental risk factors for a range of common/important conditions
The relevant emerging issues, knowledge and skills include:
Why exercise?
We are facing a global crisis of physical inactivity, with 20 000 000 adults in the UK falling into this category (British Heart Foundation, 2017). The Department of Health reports that physical activity can help prevent and manage over 20 chronic health conditions (National Institute for Health and Care Excellence (NICE) 2013). These gains can be beneficial at any age and the potential benefits are both mental and physical.
Physical activity has been strongly associated with a reduction in the incidence of non-communicable diseases. Non-communicable diseases are the world’s leading cause of death, responsible for 72% of the 54 700 000 deaths in 2016 (Astrup et al., 2019). These conditions include obesity, diabetes, coronary heart disease, cancer and chronic respiratory disease.
Obesity
Obesity rates in the UK are increasing. Since 1993, the prevalence of adult obesity has gone from 15% to 26% of the population (House of Commons, 2018). Obesity is linked to many of the conditions discussed below, such as type 2 diabetes, cardiovascular and cerebrovascular disease, musculoskeletal conditions, venous thromboembolism, abnormalities of menstruation and fertility, erectile dysfunction, respiratory problems (including sleep apnoea), stress incontinence, mood disorders and cancer. The earlier obesity starts, the earlier the onset of these conditions, hence, the concern in rising childhood obesity rates. According to the National Child Measurement Programme, 9.6% of reception-aged children are obese, and a further 13% are overweight. These figures rise to 20% and 14.3% respectively in year-6 children (House of Commons, 2018). Physical activity can help prevent all of the above by increasing the total energy expenditure, which is fundamental to weight control (World Health Organisation (WHO), 2010).
Cardiovascular disease
Most people recognise physical activity as having cardiovascular benefits, and for good reason. Regular aerobic physical activity improves the efficacy of cardiac function, increasing stroke volume and cardiac output, resulting in lower blood pressure, autonomic tone (Tiukinhoy et al., 2003) and average heart rate. There is a dose–response relationship between exercise and premature death, particularly from cardiovascular causes (Warburton et al., 2006). Interestingly, even those that are physically active, with cardiovascular risk factors, have a lower risk of premature death than inactive individuals with no cardiovascular risk factors (Wessel et al., 2004).
Regular physical activity also has beneficial effects on cholesterol levels. It improves lipoprotein profiles, through reducing triglycerides, increasing high-density lipoprotein (HDL) cholesterol levels and decreasing low-density lipoprotein (LDL) cholesterol levels (Wang and Xu, 2017). This is thought to be achieved through increased triglyceride consumption in muscle tissue, hence, increasing triglyceride hydrolysis and LDL absorption, with more cholesterol being transported to the liver via HDL.
Diabetes
Exercise has a prominent role in diabetes prevention by improving glucose homeostasis and reducing insulin resistance. This is largely due to its role in weight management and associated reduction in adipose stores. In one randomised control trial (RCT), a lifestyle intervention of moderate physical activity for least 150 minutes a week was more effective than metformin alone in reducing the incidence of diabetes (Knowler et al. 2002).
Respiratory disease
During physical activity, particularly aerobic activity, pulmonary ventilation increases with the increased tidal volume and respiratory rate required to meet oxygen demand and increases in carbon dioxide output. With regular exercise, aerobic capacity increases and there is a reduction in the risk of developing chronic lung disease, such as chronic obstructive pulmonary disease (COPD) (Hirayama et al., 2010).
Osteoporosis, osteoarthritis and falls
Physical activity has a broad range of benefits on skeletal health. Through weight-bearing exercise and particularly resistance training, bone mineral density increases, preventing osteoporosis. In a meta-analysis of RCTs, exercise-training programmes were found to prevent or reverse almost 1% of bone loss per year in the lumbar spine and femoral neck in both pre-and postmenopausal women (Wolff et al., 1999). Exercise that promotes balance, mobility and coordination, such as Yoga, is associated with a lower falls risk, probably through improvements in proprioception (Youkhana et al., 2015). Strength training through physiotherapy reduces pain and increases joint stability in osteoarthritis and other musculoskeletal disorders. These benefits reduce frailty and falls, particularly relevant in the elderly.
The inflammatory response
The inflammatory response has been linked to the aetiology of many chronic diseases and associated with increases in levels of C-reactive protein. Some RCTs have suggested that regular physical exercise may reduce the inflammatory response (Nicklas et al., 2005).
Cancer
Several studies have shown an association between regular physical activity and a reduction in the incidence of cancer, particularly of breast and colon cancer (Lee, 2003). The exact mechanism is unclear, but increasing energy expenditure may prevent tumour development through effects on sex hormone levels, immune function, insulin and insulin-like growth factors and free radical generation (Westerlind, 2003). Exercise has also been shown to improve the quality of life in patients with cancer (Galvao and Newton, 2005).
Dementia
Physical activity has been shown to be beneficial in reducing the risk of Alzheimer’s disease, all cause dementia and cognitive decline. The only exception is vascular dementia. The mechanism behind this is unclear. It has been postulated that improved cognitive function may result from the effects of exercise on cortisol and stress levels. Physical activity may also contribute to improvements in cerebrovascular integrity through improved blood flow to the brain (Chodzko-Zajko and Moore, 1994).
Mental health
Evidence of a beneficial effect from physical activity on mental health is growing. It is widely assumed that exercise can boost self-esteem, for example by improving physical skills, fitness and body image. Dishman et al. (2013) reported a 20–33% reduction in the risk of depression for active groups in prospective cohort studies. The exact form and regimen of exercise seems dependent on the individual, and is an area of growing interest that is difficult to measure in studies.
In children and adolescents, there is a correlation between exposure to green space and positive effects on mental health, including in hyperactivity and emotional disorders (Vanaken and Danckaerts, 2018).
Child development
There have been many studies on the effects of exercise on development of motor skills, social skills and cognition in children. These include assessments of language development, academic achievement and memory (Gao et al., 2018). There appear to be beneficial effects from exercise.
Cost
It is estimated that physical inactivity costs the NHS around £1 billion per year (The Kings Fund, 2014).
What are the guidelines?
Patients’ perceptions of what constitutes physical activity vary. Some will recognise gardening and housework as exercise, others only consider running and more intensive forms of exercise as having any health benefit. So what does NICE count as physical activity and how much is needed to give a health benefit?
The NICE guidelines (NICE 2013) state: Physical activity includes everyday activity such as walking and cycling to get from A to B, work-related activity, housework, DIY and gardening. It also includes recreational activities such as working out in a gym, dancing, or playing active games, as well as organised and competitive sport.
In children, the NICE guidelines define physical activity as ‘any force exerted by skeletal muscle that results in energy expenditure above resting level’ (NICE, 2009).
Put simply, if your body is in motion, you are active. However, the guidelines give more specific advice for different age groups.
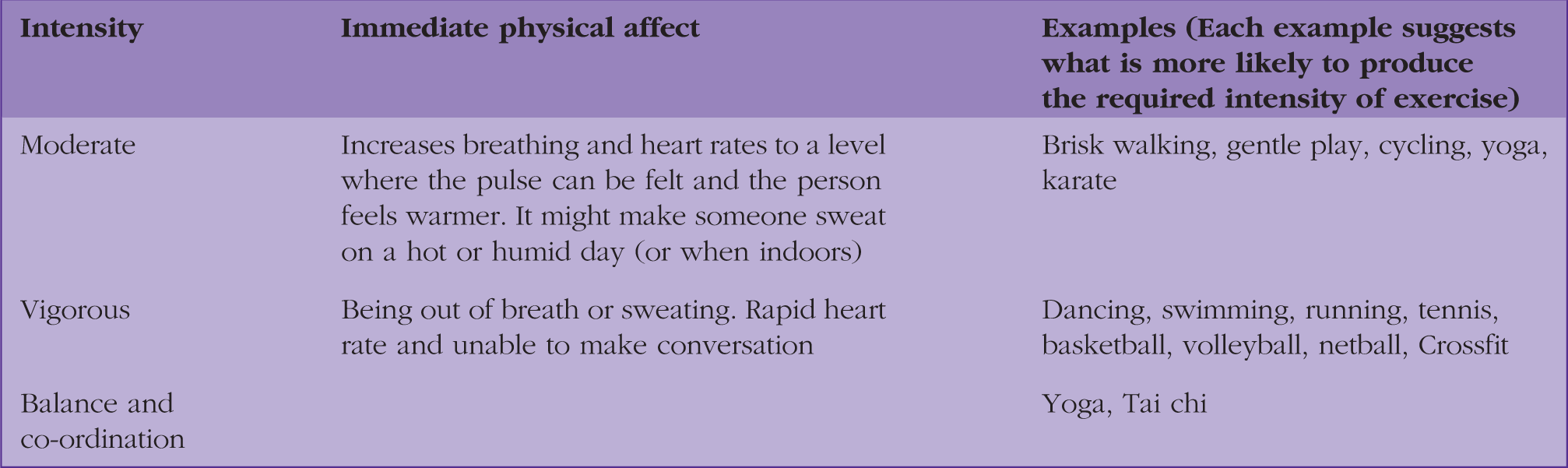
Adults
The immediate physical effects of exercise based on intensity.
Children
Children are expected to undertake moderate to vigorous-intensity exercise for 60 minutes over the course of a day (NICE, 2009). Twice a week there should also be weight-bearing exercises delivered in 10-minute bouts. This differs slightly from the WHO guidelines, where the weight-bearing target is three times a week (WHO, 2010).
In a child under-5 years in age, the general rule is that they should be as active as possible. When they can walk independently, they should be aiming to be active for 180 minutes a day in intervals throughout the day (Department of Health, 2011). This includes all forms of physical activity from light/moderate (walking/standing up) or intense (running, hopping, dancing, biking, skipping, etc.).
How can we improve access?
Exercise has to be made appealing through individual preference, socio-economic accessibility and convenience. In 2018, NICE set out guidance to address this problem by targeting public open spaces, means of travel, buildings and school playgrounds (NICE, 2018).
Pubic open space
In a plea to local authorities, owners of open space and public transport planners, NICE asked for better public access to free exercise facilities. Well-maintained and safe spaces will hopefully encourage low cost benefits to health.
Means of travel
NICE’s recommends ‘physically active travel’ that incorporates walking and/or cycling. Well-maintained cycle-ways and walkways will encourage the public to use these as their means of travel. The aim of making physical activity easy and part of everyday life should make it more sustainable in the long term.
Workplace
Another NICE initiative is engaging the workplace in physical activity, a logical way to incorporate movement into a normal day. Exercise Move Dance (EMD) UK is dedicated to the provision of workplace exercise programmes. They particularly promote group, rather than solo exercise. This is primarily to improve productivity and camaraderie in the workplace, as well as reduce sick days lost to stress or mental health issues and preventable physical ailments (EMD UK, 2016).
Playgrounds
Primary school playgrounds are designed to encourage movement. With colourful paints for hopscotch and games, children are drawn to move and play naturally, through interaction with stimulating surroundings.
There are specific government campaigns integrating research, parental/child input and the media to encourage children to meet their physical activity targets. Campaigns such as change4life to reduce obesity, aim to make exercise enjoyable and accessible.
Exercise on prescription
There are exercise referral schemes available in primary care (NICE, 2014), the exact content of which can differ between Clinical Commissioning Groups. What is universal is that sedentary or inactive individuals must not be referred if they are otherwise healthy. Examples of health conditions eligible for tailored exercise programmes include myocardial infarction, stroke, COPD, heart failure, lower back pain and chronic fatigue syndrome (NICE, 2014).
Physical activity and social media
The online ‘wellness’ industry is booming, offering everything from nutritional advice and movement inspiration to motivational captions. The accessibility of fitness advice directly from mobile devices is appealing to some and very convenient. However, the quality of advice is variable, with anecdotes and commercially sponsored sites overwhelming evidence-based information.
It is difficult to avoid incorrect advice. Clinicians can give evidence-based counter-advice. It can be helpful to know some validated or trusted social influencers to recommend to patients. Perhaps we need more NHS social influencers to help redress the balance.
Is exercise enough?
The answer to this is quite simple: No. Being physically active is one of many lifestyle factors that can be adjusted, including diet, smoking cessation, alcohol reduction, stress avoidance and improved sleep hygiene. Improving levels of physical activity can be part of several lifestyle goals to improve health and the benefits will be enhanced when improvements in lifestyle are combined.
What can we do individually?
The principles of Miller’s motivational interview involve expressing empathy, developing discrepancy, rolling with resistance and supporting self-efficacy (Rollnick et al., 2010). As either a GP or hospital doctor, time with your patients will be undoubtedly pressed. It can be challenging to personalise and develop a plan for physical activity, and sometimes this may have to be done across several appointments.
The
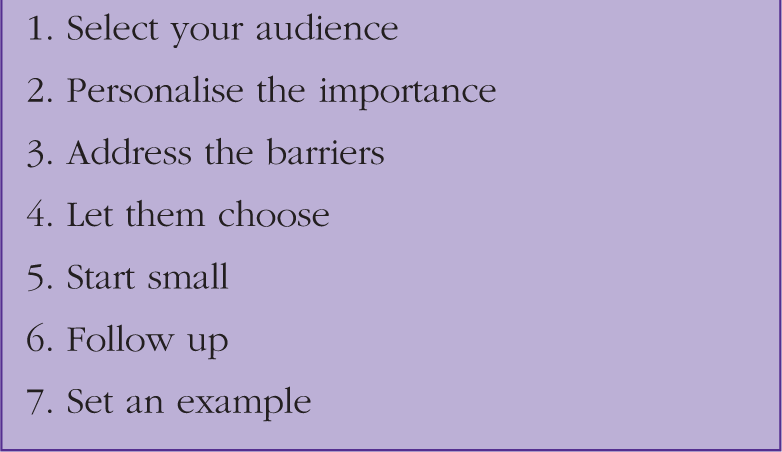
Select your audience
Suggesting changes to lifestyle requires tact and diplomacy, along with judgement, as to how open a patient is to change. There is little to be gained from ‘preaching’ to a patient. You may be adding to the general ‘nag’ of personal or societal expectation and risk harming the therapeutic relationship with the patient. Try to use open questions to introduce the issue, such as: ‘Have you thought about using exercise to help improve your health?’ Avoid sounding judgmental when discussing lifestyle, as this may lead to advice being ignored. Depending on how receptive the patient is, an exploration of ideas and beliefs about physical activity may be possible and helpful. Building trust and achieving change may require several visits depending on a variety of factors including rapport and clinical need alongside the patient’s ideas, beliefs and expectations.
Personalise the importance
This may be derived from the patient’s reason for consulting. Have they presented because of worsening symptoms from a chronic health condition, such as type 2 diabetes, hypertension, COPD or depression? If so, discussions about lifestyle might be framed around the potential benefits for the management and symptoms of co-morbidities from a particular lifestyle change. For example, lifestyle change might in some cases allow medication to be stopped or even free patients from the inconvenience of ‘medical monitoring’. If the individual’s circumstances can be used to incentivise change, then change is more likely to happen and more likely to be sustainable. Finding out what the patient’s goals are and what they want to achieve can allow lifestyle change to be linked with personal goals and ambitions, adding to the incentive for change.
Address the barriers
Addressing barriers to lifestyle/physical activity change.
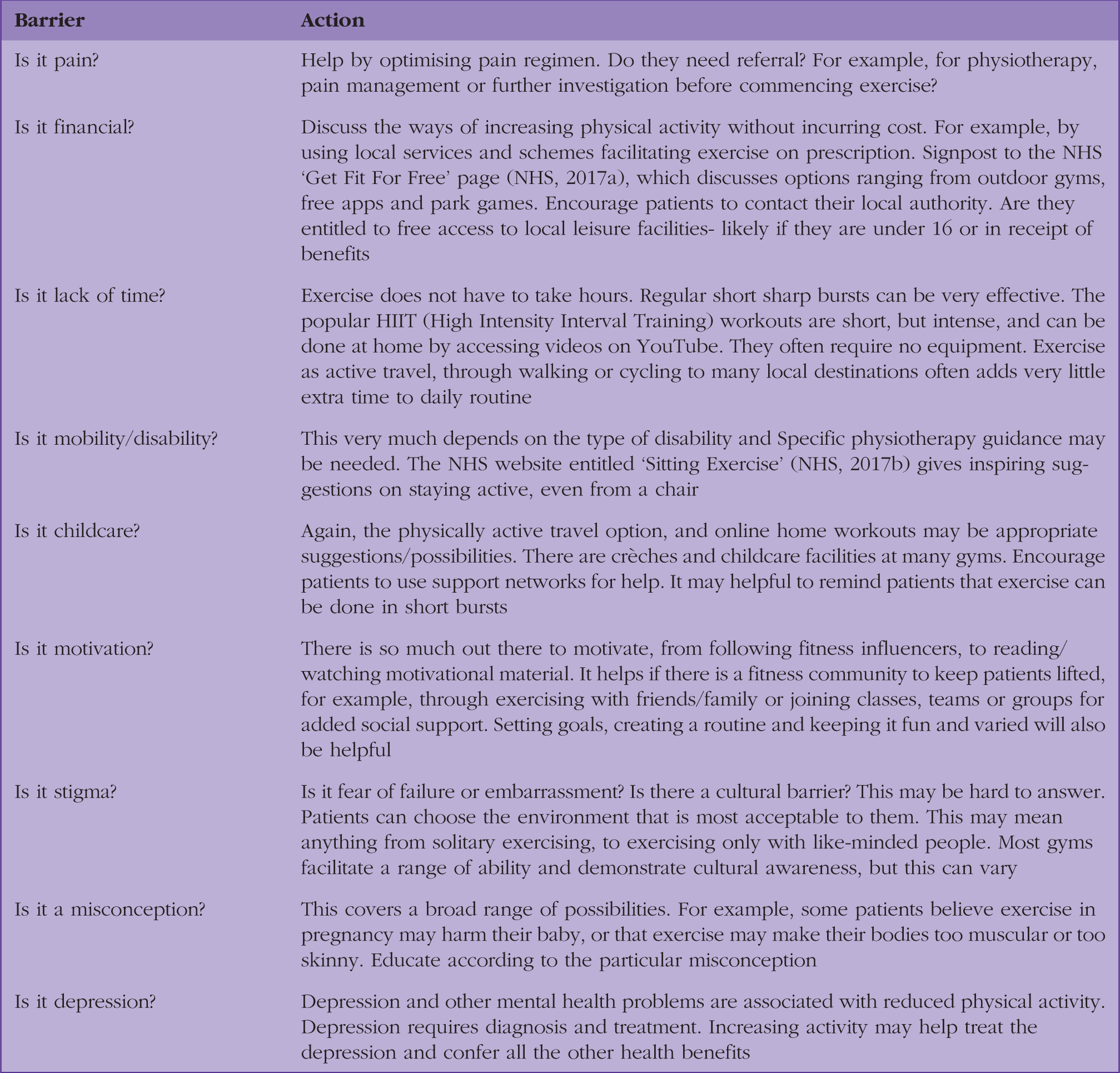
The suggestions are quite simplistic, but they illustrate the range of possible approaches needed to overcome barriers and give options and examples for patients as a starting point.
Let them choose
Your patient is an individual, so be guided by them. They may volunteer previous enjoyable pastimes or have heard of something new they want to try. You might help them reignite these old interests or nurture new pursuits. If your patient is uncertain on how to exercise, help them with suggestions appropriate to their ideas and concerns. If exercise is not a chore, it is more likely to continue and become part of a routine.
Start small
For someone who is inactive, the NICE targets for physical activity can be very intimidating. Help realign expectations around exercise. For example, discuss that walking, gardening and housework all involve exercise. If patients are starting a sporting activity, encourage them to begin with less frequent, lighter sessions and build up gradually. Encourage them to use coaches, trainers or facilitators if available, so that entry-level needs are highlighted, and intensity of exercise is appropriate. A gentle approach will hopefully encourage them to continue and to believe change is achievable. Adjust expectations. They are not expected to become an athlete; we simply want them to feel better.
Follow up
Our personal goals are more likely to be achieved if we are held accountable. The same applies to patients trying to achieve their goals. By following up patients, we can encourage or commend their achievements. Are they enjoying it or finding it too hard? Again, review and address barriers and expectations. Continue to explore and encourage the different varieties of exercise that may be possible for them. Can you measure their progress to show objective change? For example, through blood pressure readings, body mass index, or blood test results (for example, Hba1c and lipids), particularly important in cardiovascular disease and diabetes. Mental health scores may improve and are measurable through GAD7 (Generalized Anxiety Disorder) and PHQ9 (Patient Health Questionnaire) scores. Progress can be demonstrated when are no longer required. However, the change DOES NOT have to be commended by measurement alone. It can be commended simply because the patient has achieved a greater overall sense of wellbeing. Celebrate achievements with them, however small, as an important part of the motivational process. Positive results of course, are satisfying to both the clinician and patient.
Set an example
Remember to be a role model and set a personal example on the benefits and rewards from physical activity. If patients can see how exercise fits into your day, they may see how it can fit into theirs. Role models can help motivate change and this concept may help parents, carers and anyone in a position to influence, motivate and encourage others to change and improve lifestyle.
Conclusion
‘If exercise were a pill, it would one of the most cost-effective drugs ever invented’ (NHS, 2018). Remember to promote all forms of exercise at every opportunity, remembering that patients are unique and have individual needs and wishes. To move is a privilege, with so many wonderful benefits, so let us spread the message.
KEY POINTS
Physical activity targets in the UK are not being met Physical activity has many health benefits If aged 19 years or over, 150 minutes of moderate-intensity exercise per week, or 75 minutes of vigorous exercise, with two sessions of weight training weekly is recommended NICE are advocating removal of barriers and improved access to physical activity There are many opportunities to introduce the topic of physical activity and encourage patients to change lifestyle that will have beneficial outcomes A variety of motivational techniques can be used to achieve changes in lifestyle; SWEEP steps may help encourage patients to exercise