
Abstract
Globalisation has led to increased international travel for work, leisure, and to visit friends and relatives in a country of origin; this has led to greater exposure to tropical infectious agents. Many serious tropical infections encountered in primary care in the UK present as fever in a returning traveller. GPs must recognise potentially serious causes of fever in this population to ensure patients receive timely treatment. This article aims to provide a suitable framework for safe assessment, investigation and management of a patient with fever following international travel.
Clinical case scenario
Aliyah, a 20-year-old student comes to see you at your afternoon surgery. She has been feeling generally unwell and tired. She has been feverish for a day and complains of abdominal pain and nausea. She returned to the UK a week ago following a trip to Tanzania to visit family and attend her cousins wedding in a village close to Dar es Salaam. Aliyah has lived in the UK all her life and occasionally visits her relatives in Tanzania. She has not previously attended for travel vaccinations or chemoprophylaxis as she has been to Tanzania many times without problems. She worries that she may have eaten something that has made her sick. Neither of her parents who travelled with her have symptoms.
Introduction
UK citizens took 71 700 000 trips abroad in 2018 (UNWTO Madrid, 2018), many of which were to low- and middle-income countries (LMICs). Data from GeoSentinel – the largest surveillance system for travel-related illness, showed that the majority of acute and potentially life-threatening tropical infections presented as febrile illness (Jensenius et al., 2013). However, this data represents only the minority of patients who presented to specialist travel clinics after travel to LMICs. Many more patients with mild or self-limiting illness are likely to have presented to primary care. With 2 billion people estimated to travel internationally by 2030, mostly from LMICs (UNWTO Madrid, 2018), it is increasingly likely that GPs in the UK will encounter patients with tropical infections in their practice. Therefore, a working knowledge of the global distribution and features of important tropical diseases is essential.
What causes fever in returning travellers?
Fever is a common physiological response to infection, however, non-infectious causes such as drugs, autoimmune disease and malignancy must be considered. Infectious causes are the most common in returned travellers. These can be both endemic to the UK and imported infections. Malaria was diagnosed in 21% of febrile patients presenting to Geo Sentinel travel clinics, followed by enteric fever, dengue and rickettsial infection. Respiratory, gastrointestinal and genitourinary infections represented a third of confirmed diagnoses. However, 21% of patients remained undiagnosed, likely due to self-limiting illness or because relevant tests were not performed on presentation (Wilson et al., 2007). While formulating differential diagnoses, in addition to these diseases it is important to keep in mind rare, but serious, infections such as viral haemorrhagic fevers. Consideration of pandemic infections and the new and specific guidance that may apply in such circumstances is beyond the scope of this article.
Travel history
Given the risk associated with missing an imported infection, a travel history should routinely be elicited in patients presenting with fever. It is easily achieved within a 10-minute consultation and is invaluable in identifying patients requiring referral and in formulating a differential diagnosis. Location of travel, timing and exposure to specific risk factors are most important in a travel history.
Where?
Consider the geographic distribution of endemic diseases or current outbreaks. Falciparum malaria is common in travellers returning from sub-Saharan Africa, tick typhus in southern Africa, enteric fever in South Asia and dengue in Latin America and South East Asia. Patients may be aware of outbreaks in their region of travel. Alternatively, current information on outbreaks can be found on the World Health Organisation (WHO) outbreak news website.
When?
Diseases such as rickettsial and Arbovirus infections have a short incubation period and present within 2 weeks of travel (Rickettsiae are a diverse group of bacteria transmitted to humans by bites from fleas, lice, ticks or mites). Endemicity of certain infectious agents can vary by season.
Plasmodium
Falciparum has an incubation period of 7 days to 3 months. However, Plasmodium Vivax has a longer incubation period and can present months after travel.
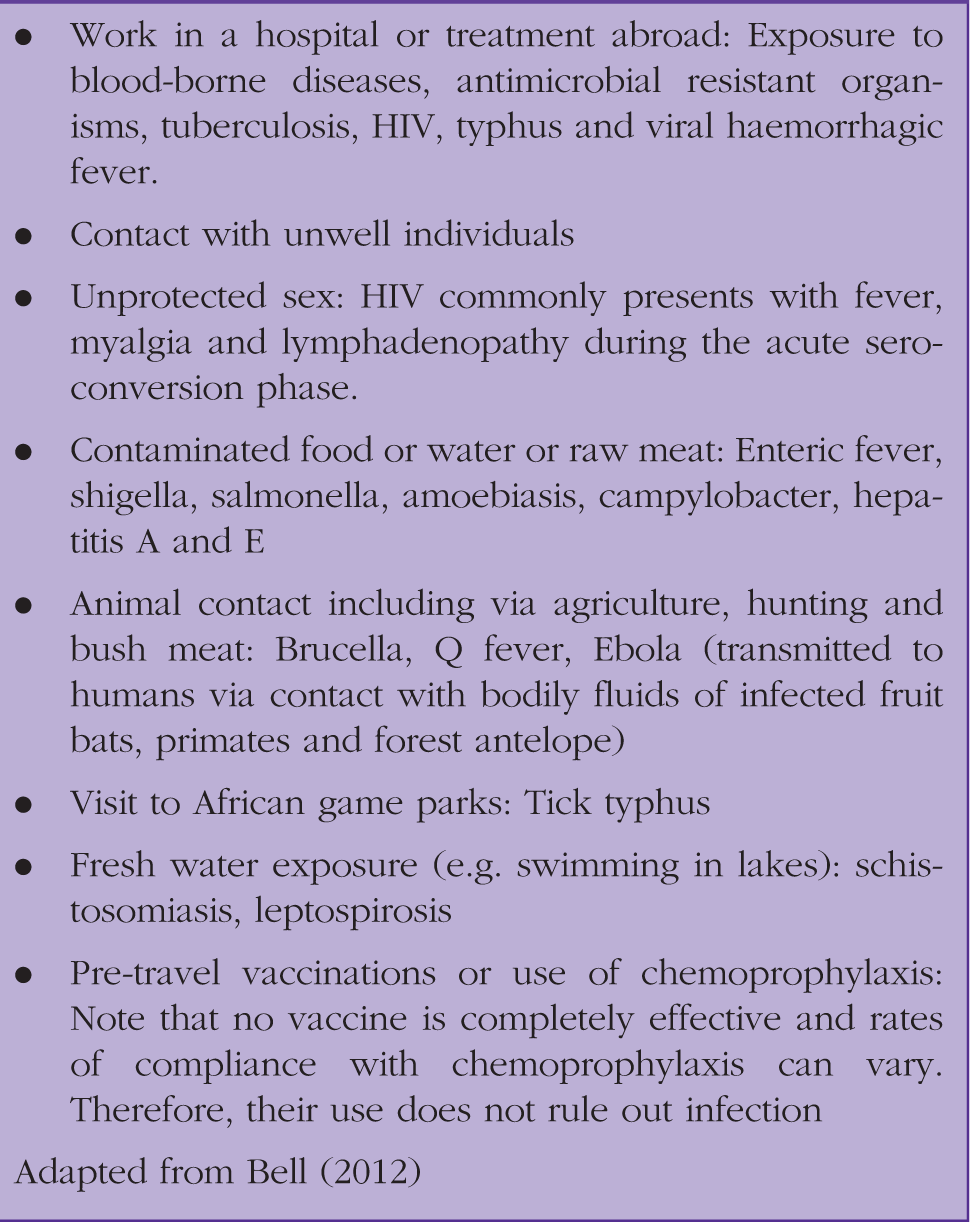
Exposure to specific risk factors
Specific risk factors.
Specific diseases
Malaria
Malaria is a protozoal disease transmitted by the Anopholes mosquito, endemic across tropical regions. It represents a significant source of global morbidity and mortality, with 219 cases worldwide in 2018 (WHO, 2019a). A total of 1375 cases of imported malarial infection were reported in the UK in 2018. Most of these were acquired in West Africa. Eighty-one percent of cases were found to be caused by P. Falciparum (Public Health England, 2019a), a rapidly progressing infection which can be fatal if untreated. All forms of malaria present with similar symptoms of fever and ‘flu-like’ symptoms such as headache, fever, abdominal pain and cough. This is particularly common in children (Lalloo et al., 2016) The majority of falciparum cases present within a month of travel. However, P.Vivax which has a long incubation period, can present weeks to months after travel. It is important to have a high index of suspicion of malarial infection in febrile travellers with a history of travel to an endemic region. Urgent thick and thin blood films and specialist referral to infectious diseases or microbiology should be completed in these patients (Bell, 2012).
Most cases in the UK were among travellers who had visited friends and family abroad (Public Health England, 2019a). This group is four times more likely than tourists to contract malaria and is less likely to have taken precautions against mosquito bites, is less likely to seek health advice prior to travel and take chemoprophylaxis (Jensenius et al., 2013; Keystone, 2019). However, malaria should still be ruled out in febrile patients with a history of travel to regions where malaria is endemic despite use of chemoprophylaxis, bed nets and insect repellent, as compliance is often poor (Fhogartaigh et al., 2012).
Dengue
Dengue is a mosquito-borne viral disease endemic across tropical and subtropical regions. It is spread by the Aedes aegypti mosquito, which also transmits the yellow fever, Zika and chikungunya viruses. Most cases of dengue are asymptomatic and resolve spontaneously. Dengue fever presents as a severe flu-like illness with high fever, nausea and vomiting, myalgia and lymphadenopathy 4–10 days after being bitten. A widespread maculopapular rash may be present. Symptoms usually resolve within a week with oral rehydration and paracetamol for symptomatic relief (WHO, 2009). Severe dengue, characterised by respiratory distress, haemorrhage, plasma leakage and organ damage can be life-threatening. Warning signs of severe dengue occur within a week of first symptoms (WHO, 2019b). They are high respiratory rate, severe abdominal pain or tenderness, persistent vomiting, mucosal bleeding and accumulation of fluid (e.g. pleural effusion and ascites). Patients exhibiting theses signs should be referred immediately for inpatient care as they are at risk of developing shock and end organ damage, requiring intensive care (WHO, 2009).
Rickettsial infection
Rickettsiae are a group of intercellular bacteria that are transmitted to humans through bites, faeces or body fluid of ticks, mites, fleas and lice. Scrub typhus and African tick typhus are most likely to present in returned travelers, as the incubation period of 5–14 days often coincides with return from holiday. Infections are commonly seen in trekkers, those who have been on safari or visited rural areas. Louse-borne typhus is a potentially serious infection that can cause epidemics in refugee camps (Beeching and Gill, 2014).
Fever and a central macular rash with eschar and lymphadenopathy are common features in all forms (see Fig. 1). Scrub typhus is endemic to South East Asia, Northern Australia and Oceania (Nicholson and Paddock, 2019). It is a zoonotic infection passed from rats to humans by being bitten by an infected mite. The eschar and rash are often present at the site of the bite. Hepatosplenomegaly may also be present. Myocarditis, delirium, pneumonia and hearing loss are possible complications. African tick typhus, on the other hand, is a milder illness usually contracted while hiking or on safari in Southern or Central Africa (Beeching and Gill, 2014).
Eschar and maculopapular rash seen in typhus.
Diagnosis is usually clinical. However, polymerase chain reaction and serological tests have a high sensitivity and specificity. Oral doxycycline is the mainstay of treatment for Rickettsial infections. However, Tetracycline-resistant scrub typhus has been identified in Northern Thailand. Milder cases of African tick typhus often do not require treatment (Beeching and Gill, 2014).
Enteric fever
Enteric fever is caused by ingestion of food or water contaminated with Salmonella Typhi and Paratyphi (type A,B or C) via faecal–oral transmission. In the UK it is most commonly seen in travellers returning from South Asia (Public Health England, 2017). Typhoid presents after an incubation period of 10–20 days depending on the number of bacteria ingested. The incubation period is shorter for paratyphoid. Symptoms include fever, myalgia, malaise, nausea, anorexia, diarrhoea or constipation and occasionally a macular rash that fades on pressure. If left untreated, 15–20% of patients develop complications such as intestinal perforation or haemorrhage, encephalopathy and toxic myocarditis (National Travel Health Network and Centre, 2019a). As antibiotic resistance is common, microbiology advice should be sought in order to identify appropriate antibiotic therapy (Public Health England, 2017). A small proportion of those infected will become chronic carriers and will continue to excrete S.Typhi in their faeces for over a year. A prolonged course of antibiotics may be required to achieve clearance (Gunn et al., 2014).
Viral haemorrhagic fever
Viral haemorrhagic fevers (VHFs) are highly contagious diseases caused by a range of viruses. They are rarely seen among travellers. However, they carry a high risk of transmission leading to outbreaks and a high case mortality rate. Examples include Ebola virus disease, Lassa fever, yellow fever, Marburg, Crimean–Congo haemorrhagic fever and dengue. Causative agents occur around the world and are endemic to certain parts of Africa, Asia and South America (Public Health England, 2018).
VHFs occur in nature in some mammals and insect reservoirs. Initial transmission to humans is via contact with bodily fluids of infected animals, or by being bitten by an infected animal. Subsequent human-to-human transmission is via close contact with bodily fluids of infected individuals or sexual contact. Due to the infectivity of the causative organisms, there is a risk of large human outbreaks that can develop quickly into epidemics following international travel. Patients typically present with fever, myalgia, headache and fatigue (Public Health England, 2018). Features of severe disease include shock, haemorrhage and pulmonary oedema. A diagnosis of VHF should be considered in those returning from areas of recent or ongoing outbreak, especially those who worked in or report contact or participation with healthcare (National Travel Health Network and Centre, 2019b). Immediate advice should be sought regarding isolation and treatment of suspected cases.
Physical examination
Many of the infections above present with fever and non-specific symptoms. However, certain examination findings may raise suspicion of a specific disease. For example, the presence of a maculopapular rash in dengue, rickettsial infection, and HIV (Bell, 2012); splenomegaly in malaria and enteric fever or the presence of an eschar in rickettsial infection (Fink et al., 2018).
Investigation
Full blood count, serum inflammatory markers, blood culture and chest X-ray should be performed routinely. In patients with geographical risk of malaria, rapid diagnostic testing should be performed. Thick and thin blood films should also be performed to determine, maturity and species
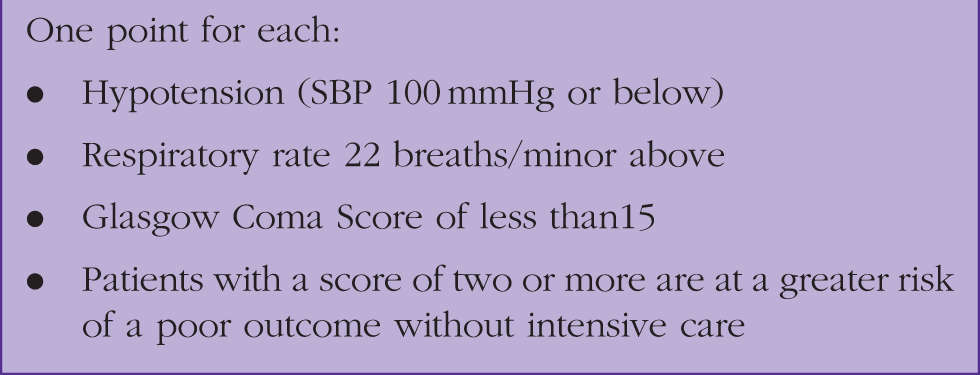
When to refer
qSOFA score.
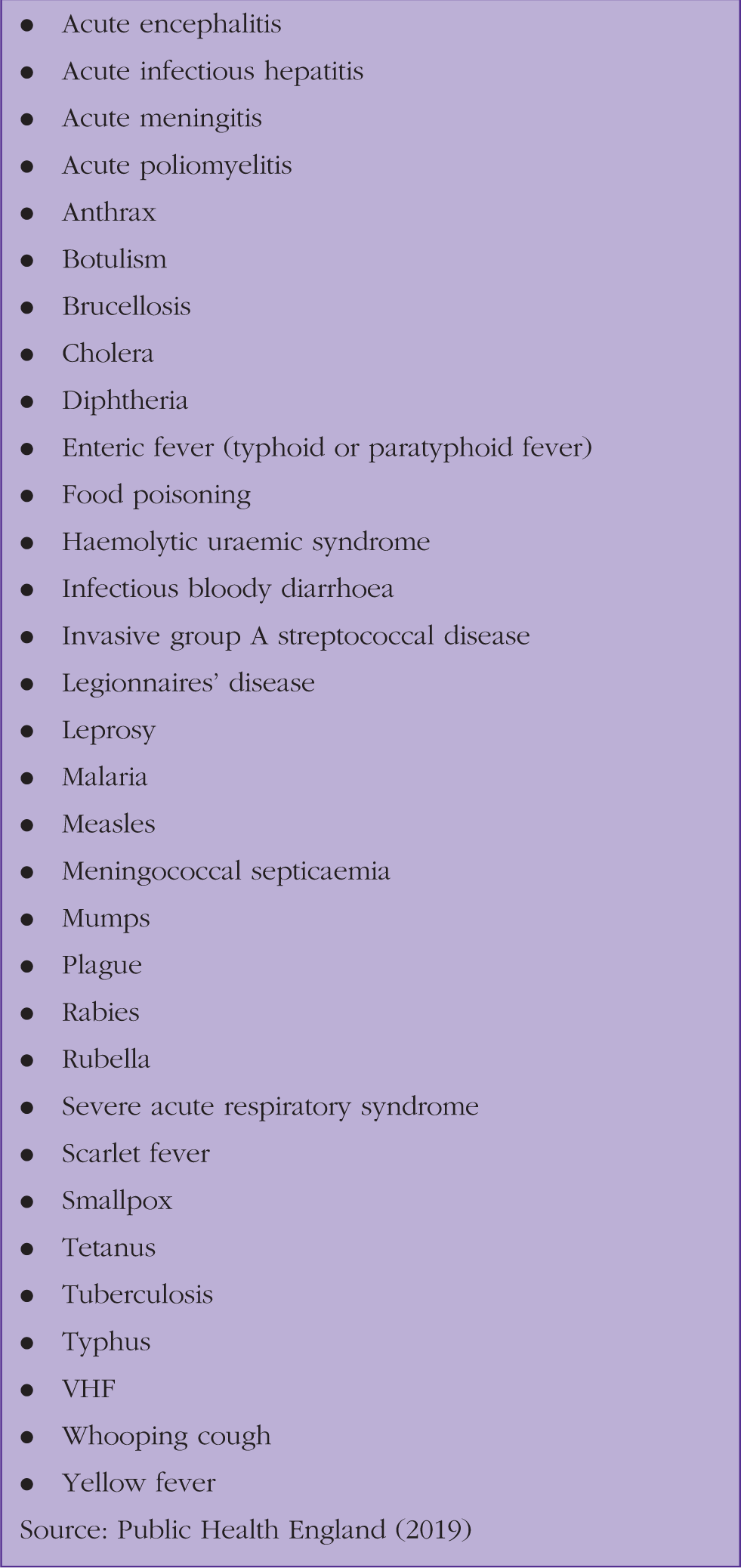
Public health: Notifiable diseases
List of notifiable diseases.
KEY POINTS
Always ask about travel history in patients presenting with fever including date of travel and destination Immediately identify life-threating illness and refer haemodynamically unstable patients to secondary care Malaria is a common, rapidly progressing cause of fever in the returning traveller and requires urgent specialist referral Use of prophylaxis and preventative measures does not guarantee protection from a disease Medical practitioners have a statutory duty to report suspected cases of notifiable diseases to appropriate authorities
Editor’s note
This article was written before the current pandemic and therefore does not consider assessment of fever according to prevailing guidance on COVID-19. However, it serves to remind us that there are other important causes of fever in returning travellers and of the importance of accurate diagnosis with testing.