
Abstract
Peptic ulcer disease (PUD) is defined as a disruption in the innermost lining of the gastrointestinal tract, due to the secretion of gastric acid or pepsin. The disruption is in the gastric epithelial layer, specifically the muscularis mucosae. PUD normally affects the stomach along with the first and second parts of the duodenum, although it is not limited to these areas. Typically, gastric ulcers induce upper abdominal pain within 30 minutes of eating, whereas duodenal ulcers cause discomfort much later. Endoscopic and histological investigations are the key to early identification and treatment of patients with PUD, with testing for Helicobacter pylori necessary in those patients suspected of having PUD. In this article we will be looking at the aetiology, pathophysiology and management of PUD.
Clinical case scenario
A 45-year-old gentleman, presents with epigastric pain. He has been complaining of indigestion for 4 months, with pain occurring several hours after eating. He describes the pain as being burning, sharp and intermittent, however, on this occasion his pain is more severe. He denies any weight loss, dysphagia or vomiting, but yesterday passed melena. He normally drinks coffee in the morning with a cigarette, having up to five cups of coffee a day. He drinks six units of alcohol a day in various combinations of wine and beer. He works as a lawyer, and yesterday attended a work party, consuming more alcohol than normal with a spicy curry for dinner. On examination, the patient has epigastric tenderness along with an incidental soft reducible epigastric hernia. The patient is concerned that his long-standing hernia is the source of his pain and wants to be referred to the surgeons for repair of the hernia.
Aetiology
Causes of peptic ulcer disease.
Helicobacter pylori
H. pylori is a gram negative spiral-shaped bacillus found within gastric epithelial cells. Approximately 50% of the worldwide population carries H. pylori, with a higher incidence in developing countries. It accounts for approximately 90% of duodenal ulcers and between 70 and 90% of gastric ulcers (Talia et al., 2020). There is a higher prevalence in lower socioeconomic groups, with transmission by the faecal–oral route and disease being acquired in childhood. H. pylori adheres to and irritates gastric mucosa as a result of a variety of factors. The resulting effect is hypochlorhydria or achlorhydria, causing ulceration. Virulence factors are factors that allow micro-organisms to survive and promote disease. In the case of H. pylori there are three main factors:
Urease: H. pylori produces urease, an enzyme responsible for the breakdown of urea into carbon dioxide and ammonia. The ammonia produced by H. pylori allows it to survive by neutralising gastric acid Toxins: Cytotoxin-associated gene A (CagA) is a highly antigenic protein secreted by approximately 60% of H. pylori strains and is responsible for inflammatory responses and a role in carcinogenesis. Vacuolating toxin A (VacA) is is a protein secreted by H.Pylori and enhances colosization by the bacteria Flagella: Allow H. pylori to migrate to gastric epithelium
Individuals with H. pylori tend to have elevated serum gastrin levels, with raised gastric acid secretion compared with controls. As a result, evidence of gastritis is present in most individuals with the infection. Chronic infection and gastritis can result in more sinister manifestations, in the form of atrophy, metaplastic or neoplastic changes.
Non-steroidal anti-inflammatory drugs
Risk factors for NSAID-associated peptic ulcer disease.
Medications
It is not only use of NSAIDs that causes PUD. Other medications can also have a causative role. These include the use of corticosteroids, bisphosphonates, potassium chloride, fluorouracil, aspirin, anticoagulants and higher doses of NSAIDs.
Smoking and alcohol are significant risk factors in duodenal ulcers, although the association is not completely clear. Both inflame the gastric mucosa and result in raised gastric acidity levels.
Epidemiology
Worldwide, the lifetime risk of developing PUD is between 5 and 10% (Talia et al., 2020). This incidence has decreased over recent years with improvements in hygiene and sanitation, along with improved treatment and a more considered approach to the administration of NSAIDs and protective measures to reduce the well-documented side effects. Gastric ulcers are less common than duodenal ulcers, with the former being four times as common. Duodenal ulcers are more common in males, compared with females.
Clinical features
Upper abdominal pain is the main symptom of PUD. Patients often describe the pain as ‘burning’ or ‘gnawing’ in nature. The history of PUD is very important in helping to determine the type of ulcer. Signs vary according to the position of the ulcer, along with the duration of symptoms. The time to onset of symptoms in relation to mealtimes can discriminate between gastric and duodenal ulcers. Duodenal ulcers typically induce pain and discomfort 2–3 hours after meals or nocturnally, with symptoms resolving with food. Pain may be colicky in nature, with patients often being symptom-free for several weeks. In contrast, gastric ulcers are also associated with mealtimes, but pain tends to occur sooner after meals, and symptoms are often exacerbated by eating.
Red flag signs and symptoms.
Differential diagnosis for symptoms of dyspepsia.
Investigation
Dyspepsia, as defined by the National Institute for Health and Care Excellence (NICE), is a range of symptoms arising from the upper GI tract. The British Society of Gastroenterology defines dyspepsia as a group of symptoms that alert doctors to consider the diseases of the upper GI tract. Dyspepsia itself is not a diagnosis, it is a symptom.
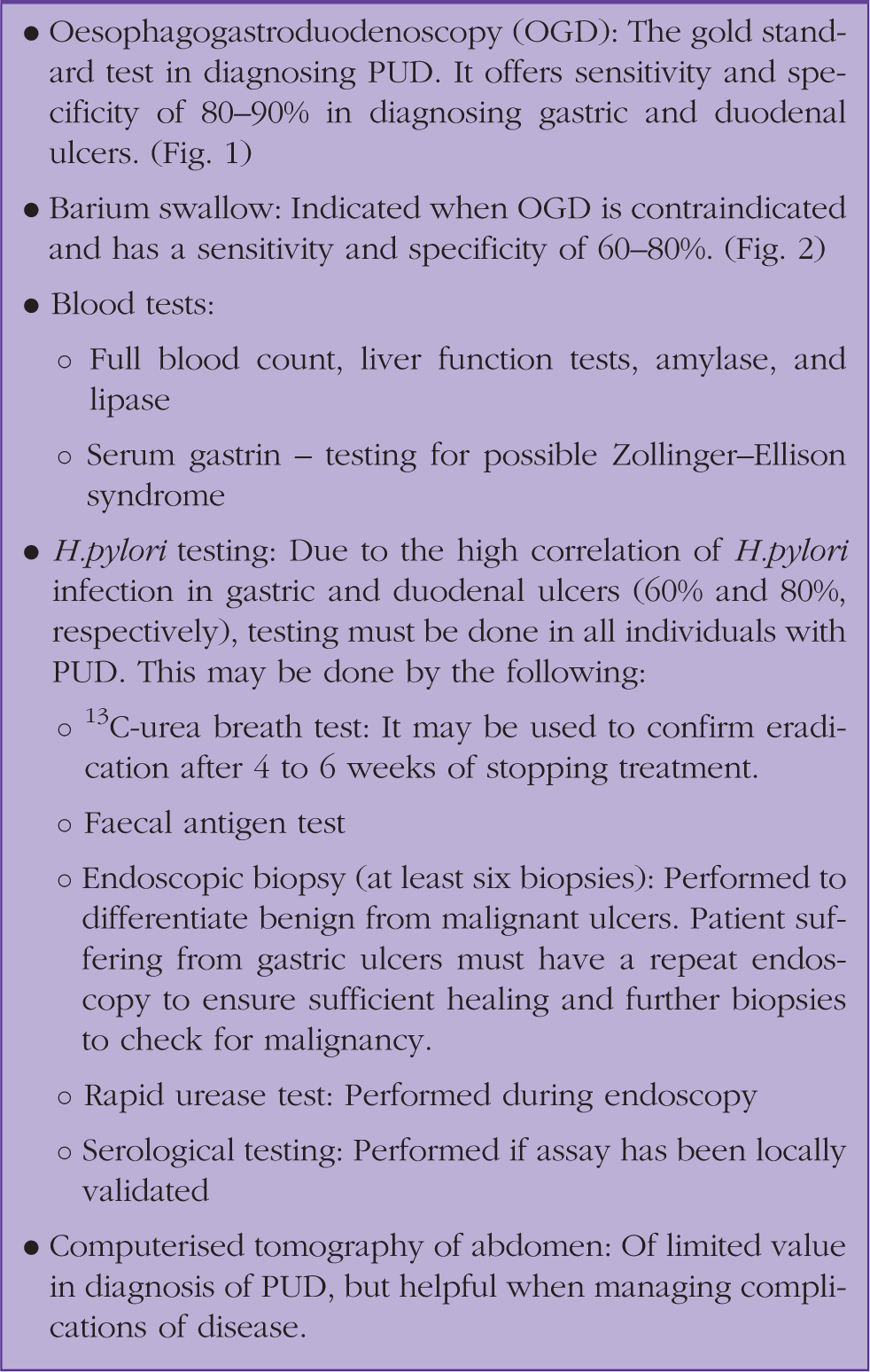
Investigations.
Treatment
The management of PUD has changed considerably over the course of the 20th century. It was initially treated with bed rest and antacids before the introduction of H2 receptor antagonists and PPIs, culminating in H. pylori eradication therapy. Antacids have been used in symptom control of patients with dyspepsia. Although relatively safe, aluminium-containing antacids have constipating side effects, magnesium-containing antacids may cause diarrhoea and both can exacerbate underlying renal failure.
The mainstay of medical treatment for PUD is anti-secretory drugs. These can be in the form of H2 receptor antagonists, which work by decreasing histamine-stimulated acid secretion, basal acid secretion, and meal-induced acid production. However, PPIs have largely replaced H2 receptor antagonists, due to their increased efficacy and more potent inhibition of acid secretion. Their mode of action is through inhibiting H+/K+-ATPase of the gastric parietal cells. They are activated by acid, and therefore, work more efficiently when proton pumps are activated, hence, the recommendation that PPIs are taken just prior to breakfast. These drugs are well tolerated with limited side effects, but can induce headaches and diarrhoea. Due to the reduced acid secretion, PPIs provide symptom relief and promote ulcer healing. It is important that calcium levels are checked in patients on PPIs, and if appropriate, calcium supplements prescribed. Long-term use of PPIs can increase the risk of osteoporosis, and resulting fragility fractures.
In individuals found to have H. pylori infection regardless of the use of NSAIDs, it is appropriate that they are treated with a full course of eradication therapy.
This includes a week of full dose PPI (e.g. Omeprazole or lansoprazole), metronidazole 400 mg twice daily(BD) and clarithromycin 250 mg BD or full dose PPI, amoxicillin 1 g BD and clarithromycin 500 mg BD. Studies have shown that the use of PPIs alone is less successful in treating PUD, when compared with eradication of H. pylori alone. Without the use of H. pylori eradication, ulcers recur in up to 95% of individuals, whereas with treatment the recurrence rate decreases to approximately 10%. To be confident of complete eradication it may be necessary to repeat H. pylori testing. This is normally done in the form of a 13C-urea breath test, as it is non-invasive. Serological tests may be used, but it has been shown that these remain positive for more than a year after successful H. pylori eradication (Cutler and Prasad, 1996).
Peptic ulcers associated with NSAIDs
When identified as being the cause of PUD, NSAIDs should be stopped. Where NSAIDs cannot be discontinued, ranitidine is identified as being inferior to omeprazole in clinical trials (63% versus 80% healing at 8 weeks). Omeprazole 20 mg is the recommended dose (not 40 mg). NICE guidelines advise an 8-week course of PPI or H2-receptor antagonist for treatment of NSAID-associated PUD (NICE 2014a).
Since the use of NSAIDs is so prevalent, both as a prescription drug and over the counter, clinicians must consider giving primary ulcer prophylaxis. This was previously treated using misoprostol 800 mcg once daily, which has been shown to decrease the incidence of PUD and its associated complications. Misoprostol does tend to cause GI side effects and NICE recommends PPIs as first line prophylactic treatment. Those with previous PUD complications, on aspirin or glucocorticoids, or with multiple additional risk factors should avoid NSAIDs altogether.
Refractory ulcers
A refractory ulcer is one greater than 5 mm in diameter that does not respond to treatment despite 2–3 months of PPI administration. When patients are not responding to medical treatment consider ongoing H. pylori infection, issues with compliance, lifestyle changes (e.g. smoking cessation) or an alternative diagnosis.
Alternative diagnoses to consider include:
Hypersecretory conditions Infection (e.g. Cytomegalovirus, tuberculosis) Infiltration (e.g. Sarcoidosis, Wegener’s) Cocaine use Crohn’s disease Neoplasm
If the ulcer continues not to heal after giving consideration to other diagnoses, then surgical intervention should be considered, including vagotomy or partial gastrectomy.
Complications
Unfortunately, PUD is associated with significant complications. These include:
Upper GI bleeding Gastric outlet obstruction Perforation Penetration Gastric cancer
Bleeding
Upper GI bleeding is a life-threatening condition, associated with a mortality of around 10%. Around half of all acute upper GI bleeds are the result of PUD. Individuals present with haematemesis, melaena and often accompanying hypovolaemic shock. In the acute setting, there frequently is not a drop in haemoglobin levels, but a significant rise in serum urea disproportionate to serum creatinine levels as a result of the gastric degradation of haemoglobin.
Upper GI bleeding resolves spontaneously in approximately 80% of cases, but it is important to identify patients with persistent bleeding, as the associated mortality is high. Patients with upper GI bleeding are managed by medical gastroenterologists usually and require urgent endoscopic intervention. Therapeutic interventions include adrenalin injection, cautery or endoscopic haemoclip application. Studies indicate that a bolus of omeprazole followed by infusion for 72 hours can decrease the rate of re-bleeding. Previous guidelines have suggested that patients suffering with acute GI bleeds should receive 1g tranexamic acid. However, the recent HALT-IT trial suggests there is no difference in outcome between patients receiving tranexamic acid and those given placebo. In some circumstances, mesenteric angiography and embolisation can be used to identify and treat bleeding points. However, in those individuals considered haemodynamically unstable, surgical intervention is required when either the source of bleeding cannot be identified or is not amenable to endoscopic intervention. This may involve ligation of the vessel if bleeding is from duodenal ulceration, or partial gastrectomy for bleeding associated with gastric ulceration.
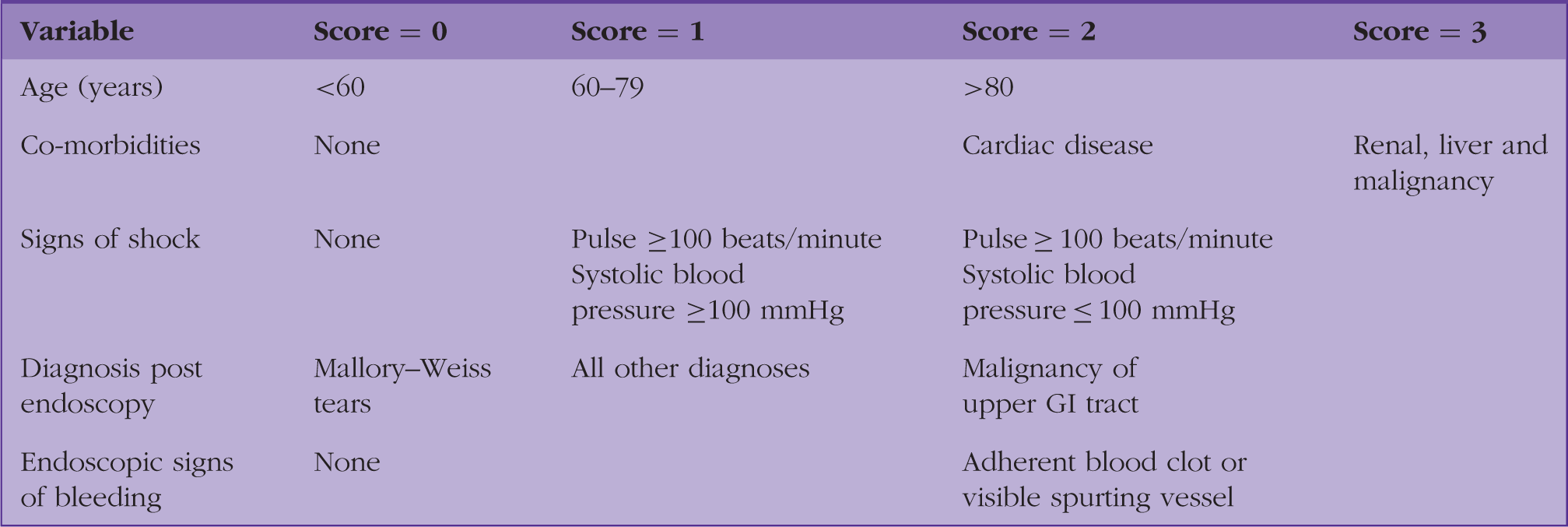
Rockall scoring system.
Perforation
Ulcers that perforate can be life-threatening. The high associated morbidity and mortality is related to the sudden presentation, with 10–15% of patients having no prior history of PUD. Patients normally present with sudden abdominal pain, which then improves over the next few hours followed by a further deterioration as the perforation develops into frank peritonitis. Individuals with such a condition need urgent surgical intervention. In some circumstances, it is possible that the perforation has sealed, due to omental migration, however, this must be confirmed by clinical assessment and further radiological imaging. Duodenal ulcers are repaired using omental patches, followed by H. pylori eradication, as this reduces the risk of recurrence. Patients generally do better following surgery for duodenal ulcers, whereas perforations from gastric ulcers are associated with much higher rates of mortality (10 to 40%). Alongside clinical findings of peritonism, imaging is highly important in diagnosing a perforation. This may be in the form of an erect chest X-ray or computerised tomography (CT) scan.
Penetration
Perforation is a sequela of ulceration that instead of resulting in perforation into the abdominal cavity results in fistula formation with nearby or adjacent structures, commonly the liver and pancreas. Often asymptomatic, diagnosis is difficult, but penetrating tracts can be identified via CT or endoscopy.
Gastric outlet obstruction
PUD may result in gastric outlet obstruction, due to oedema or scarring. Patients present with epigastric pain, early satiety, vomiting, malnutrition and bloating. Treatment includes correction of electrolyte imbalances from poor nutritional status and placement of a nasogastric tube. In patients where there is significant concern about nutritional status, an endoscopically placed naso-jejunal tube may be employed to meet nutritional demands. Often this conservative approach to management is sufficient to settle surrounding oedema. However, in some circumstances it may be necessary to dilate the stricture using endoscopic balloon dilatation. However, this approach often proves difficult, due to fibrosis, and in some circumstances surgery may be required, such as bypass procedures (gastrojejunostomy) or antrectomy.
Improving outcomes
PUD is an increasingly common disorder as our population deals with ongoing societal issues such as obesity, binge drinking and smoking. When untreated, PUD results in significant illness. Most patients present with PUD to their GP, with some occasionally attending emergency departments. The wide range of signs and symptoms, along with the vague nature of symptoms requires clinicians to be vigilant and wary of missing the diagnosis or passing off symptoms with an alternative explanation such as simple ‘bloating’ or ‘abdominal migraine’. It is important to investigate thoroughly, as a missed diagnosis has significant consequences.
Once diagnosed, the mainstay of management is education. Implementing lifestyle change, including smoking cessation, advice on alcohol through liaison services and advice on appropriate self-medication can all be important. Since a considerable number of NSAIDs can be purchased over the counter, without a prescription, it is important to involve practice pharmacists as part of the multi-disciplinary team, to rationalise and optimise patients’ medication. Dietitians may offer important advice and provide appropriate advice sheets on foods that reduce gastric acid secretion and programmes that promote weight loss. There is evidence to suggest that obesity is a factor in triggering PUD. It is only by using a primary care multi-disciplinary team approach that a significant impact will be made on the morbidity associated with PUD. In time, hopefully, such efforts will also reduce the incidence of PUD.
KEY POINTS
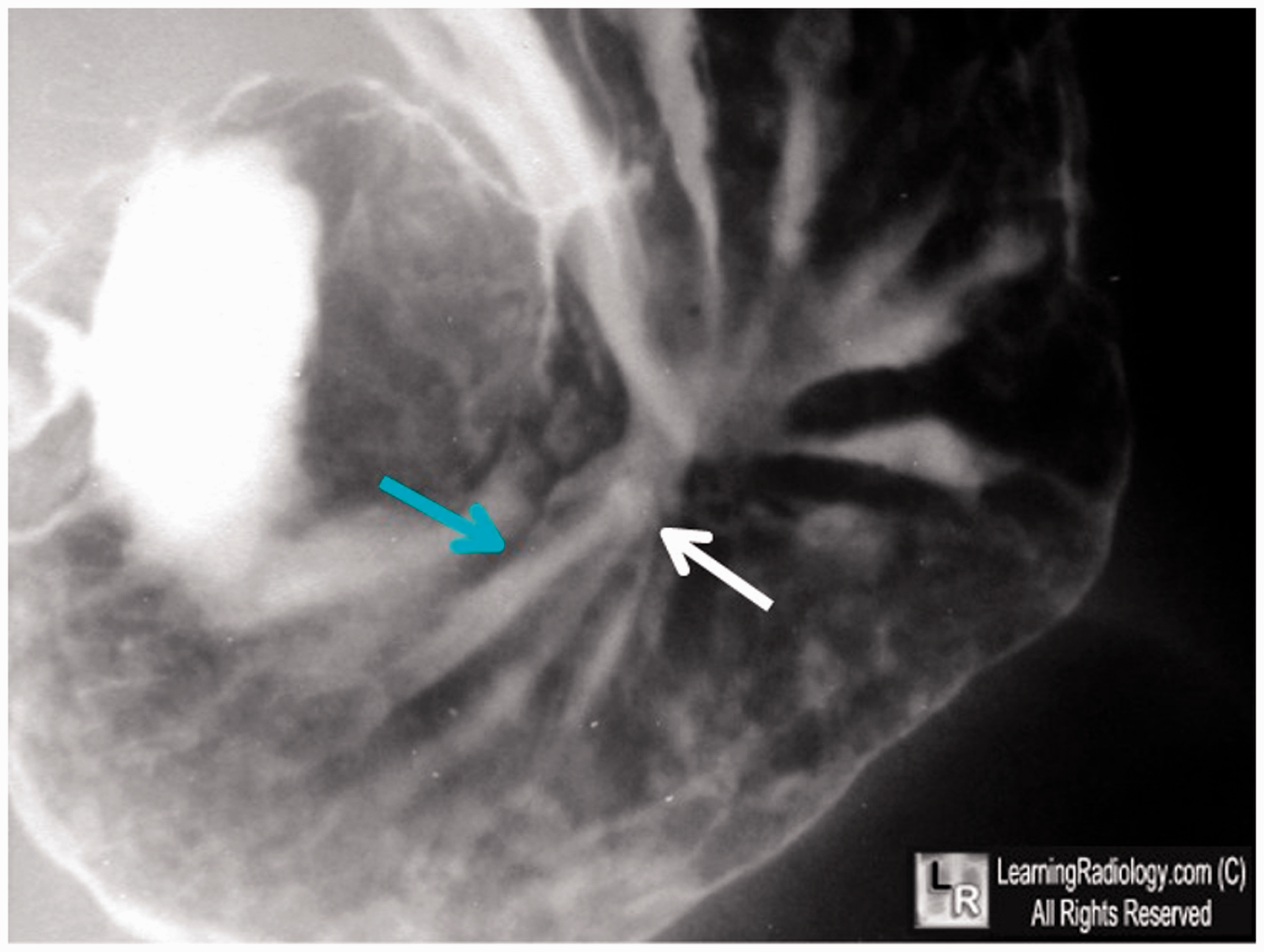
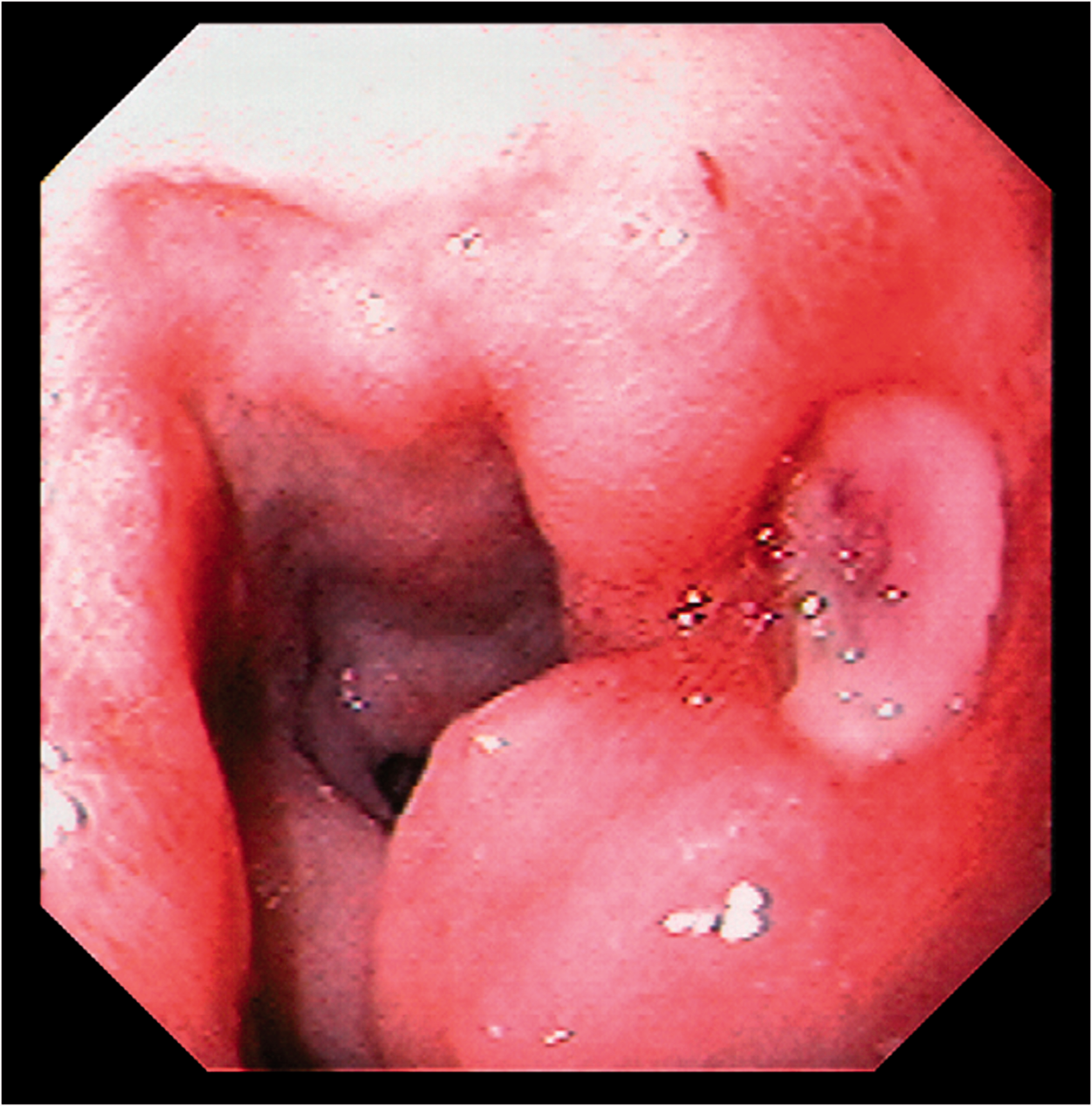
PUD is a common condition, more prevalent in lower socioeconomic groups and associated with significant mortality and morbidity H. pylori infection and overuse of NSAIDs are the most common causes of PUD; approximately 50% of the population worldwide carries H. pylori, with a higher incidence in developing countries and H. pylori accounts for approximately 90% of duodenal ulcers and between 70 and 90% of gastric ulcers Management of PUD has changed over the course of the 20th century, culminating in H. pylori eradication therapy Lifestyle changes, frugal use of NSAIDS, and use of PPIs are most important in preventative management Early diagnosis and intervention are important in preventing secondary complications Not all patients with dyspepsia require investigation, but assessment of uninvestigated dyspepsia should identify red flags and other potential diagnoses Image taken of stomach following barium swallow. The green arrow shows folds following to a central position as marked by the white arrow, which is a persistent collection of barium. The white arrow indicates the position of the ulcer. Peptic ulcer as visualised using endoscope.
ORCID iD
Mr Aran Sivakumar https://orcid.org/0000-0001-8025-4227