
Abstract
Local anaesthetics are frequently used in both primary and secondary care. These agents transiently reduce the nervous conduction of nociceptive signals, reducing sensations of pain. In primary care, local anaesthetics are often used for minor surgical procedures. However, there are other uses for these agents. It is important to understand the issues encountered when using local anaesthetics in primary care. This review will cover clinical use, relevant pharmacology and adverse effects of the different local anaesthetic preparations.
Clinical case scenario
Mr Johnson attends your surgery accompanied by his daughter. He is an 85-year-old gentleman with a past medical history of atrial fibrillation, hypertension, type 2 diabetes, gastro-oesophageal reflux, depression, osteoarthritis and mild memory impairment. He also has a history of falls and has previously undergone a hip replacement following a fractured neck of his femur. He lives alone, has carers twice a day and he takes apixaban, ramipril, metformin, omeprazole, citalopram and paracetamol, as well as codeine when required.
He complains of continuous pain across the right side of his torso, worse over the preceding month. He describes having a rash in the same area, but reports that the rash improved some time ago. Examination is largely unremarkable, but he complains of intense pain on light palpation of the T5 dermatome on the right side. You diagnose post-herpetic neuralgia. You decide to prescribe a lidocaine plaster rather than oral analgesia having considered his frailty and propensity for falls. You arrange to review his symptoms in 2 to 3 weeks having given him instructions on how to apply and when to remove the plasters.
Basic science
Physiology of pain
The sensation of acute pain arises from the activation of peripheral nociceptors secondary to local inflammation or trauma. Through the activation of sodium channels, this causes depolarisation of either fast conducting, myelinated A-delta nerves (sharp pain) or slower conducting, unmyelinated C fibres (dull, visceral pain) which travels to the central nervous system whereby an unpleasant sensation is experienced (Yam et al., 2018).
Local anaesthetic mechanism of action
Local anaesthetics exert their mechanism of action by blocking sodium channels, thereby preventing the depolarisation of peripheral nerves. By preventing an influx of sodium, the resting membrane potential of the nerve axon is altered, and the propagation of an action potential is therefore inhibited.
Local anaesthetics are highly lipid soluble molecules, meaning that they readily pass through the phospholipid bilayer surrounding the nerve axon. Once inside the nerve cell, the local anaesthetic molecule becomes ionised, and therefore, is unable to pass back through the cell membrane and stays trapped within the nerve. Here, they bind to the inside of active sodium channels, preventing the return to their resting state, and hence, inhibiting the transmission of further neuronal impulses (Peck et al., 2008).
Physicochemical properties
Structurally, local anaesthetics are either esters or amides. These two molecules share two common parts. A hydrophilic, tertiary amine tail is connected by either an ester or amide link to a lipophilic aromatic ring (Becker and Reed, 2006).
A useful aide memoir to recall the members of each category is that the ester local anaesthetics do not contain the letter ‘i’ before the suffix ‘_caine’ (e.g. procaine, amethocaine and cocaine) whereas the amides do (e.g. l
The most notable differences between the two categories of local anaesthetic are in their metabolism and elimination. For the most part, esters are rapidly hydrolysed in the blood by plasma cholinesterases; this leads to the production of the metabolite para-aminobenzoate (PABA), which is often the responsible compound in patients allergic to local anaesthetics. Amides, on the other hand, are metabolised hepatically, and so are less likely to cause an allergic reaction (Peck et al., 2008).
The ratio of un-ionised to ionised local anaesthetic molecules accounts for the varying speed of onset and potency seen between different local anaesthetic preparations. Given that the ratio of ionisation of a molecule is dependent on the pH of the surrounding environment, in the acidic environment of infected tissue, there are fewer un-ionised local anaesthetic molecules available to cross into the nerve cell, and therefore, action potentials may still be generated. It is for this reason that local anaesthetics are often less effective if used in an attempt to anaesthetise infected tissue, e.g. an abscess (Peck et al., 2008).
As with many other medications, the lipid solubility of a local anaesthetic preparation is partially responsible for its potency. Highly lipid soluble local anaesthetics freely diffuse through the neuronal cell membrane, and so relatively smaller doses are needed to achieve a comparable pharmacological effect (Peck et al., 2008)
Pharmacological properties of commonly used local anaesthetics.
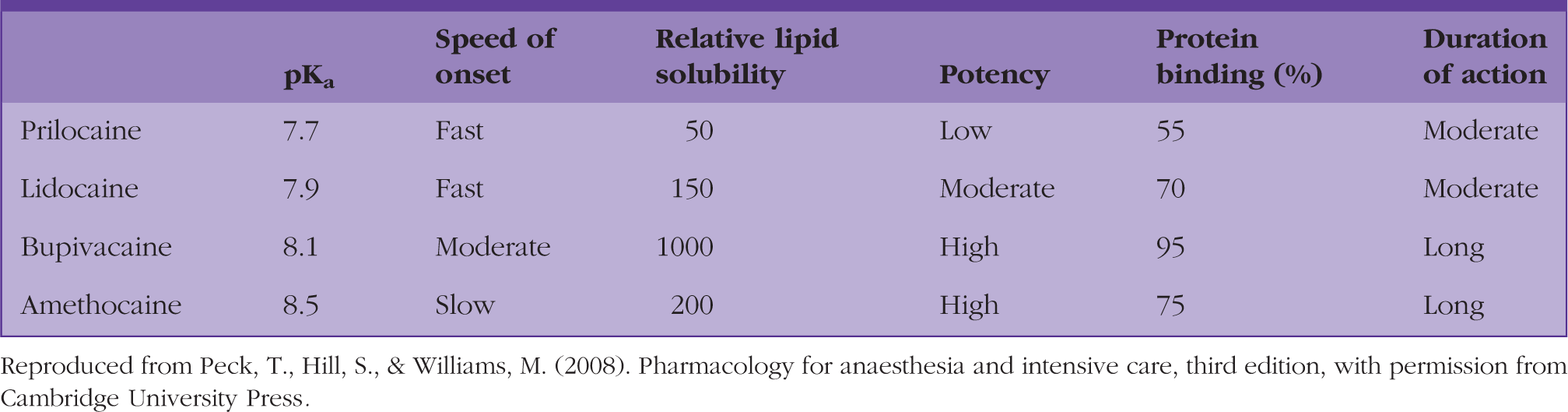
Reproduced from Peck, T., Hill, S., & Williams, M. (2008). Pharmacology for anaesthesia and intensive care, third edition, with permission from Cambridge University Press.
Clinical application
Solution for injection
Doses of commonly used local anaesthetics.
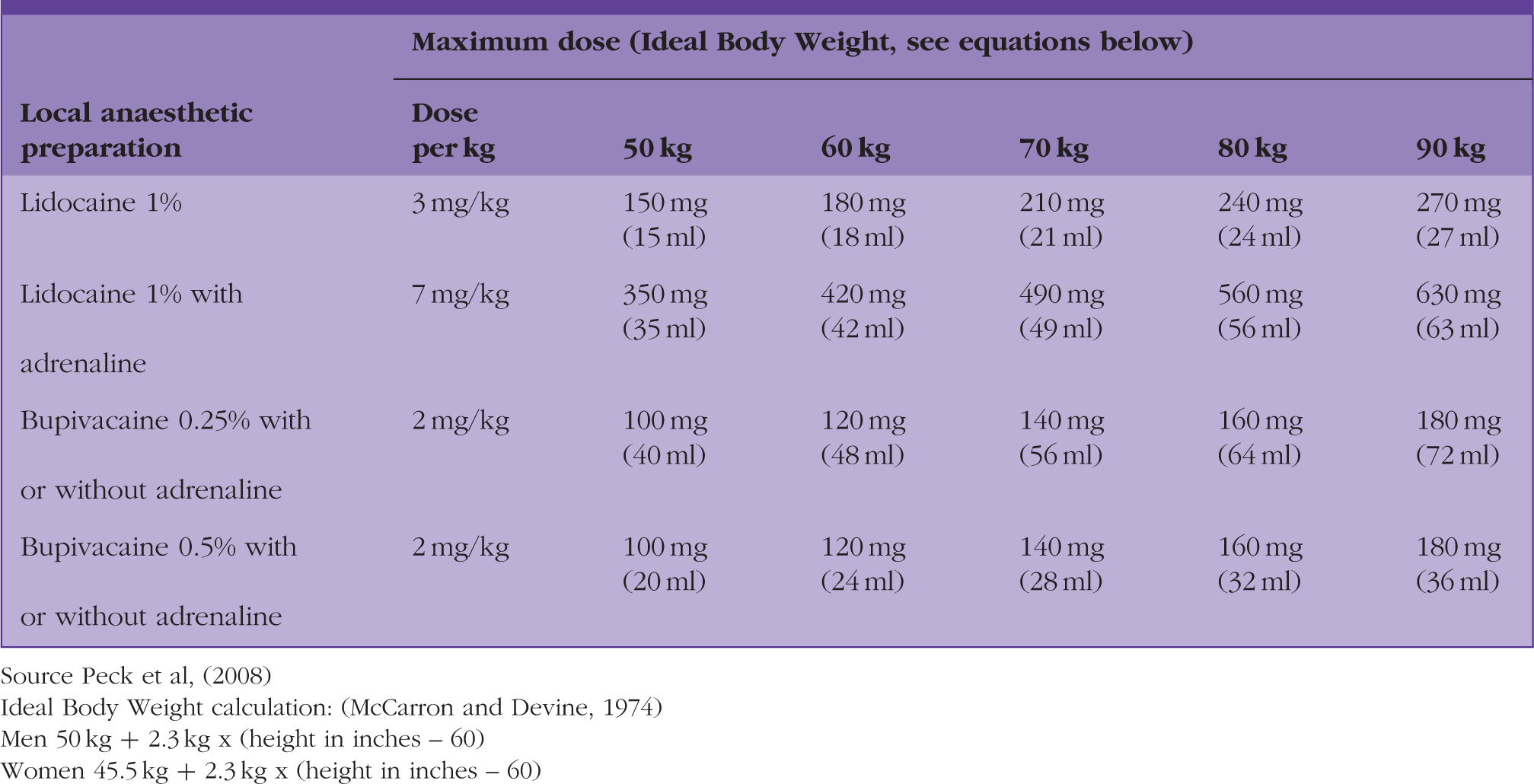
Source Peck et al, (2008)
Ideal body weight calculation: (McCarron and Devine, 1974)
Men 50 kg + 2.3 kg x (height in inches – 60)
Women 45.5 kg + 2.3 kg x (height in inches – 60)
If using adrenaline-containing preparations, it is important to acknowledge the potential drawbacks of this approach. Traditional teaching has suggested that the use of an adrenaline-containing local anaesthetic mixture is contraindicated in any area of the body in which blood supply may be compromised if local vasoconstriction occurs, for example, the digits, ears, nose or penis. However, it has been suggested that the use of an adrenaline-containing local anaesthetic preparation in finger and hand surgery is safe and is not associated with the previously feared theoretical risks (Chowdhry et al., 2010).
Inadvertent intravascular injection of local anaesthetic is possible when attempting to anaesthetise subcutaneous tissue, however, the adoption of correct surgical technique should reduce the likelihood of this event occurring. If an adrenaline-containing local anaesthetic mixture is injected intravascularly in this circumstance, the recipient may become flushed and hypertensive or complain of palpitations. This should alert the clinician to stop injecting the solution and reposition the needle tip before continuing infiltration.
It is also important to understand the potentially confusing nomenclature when it comes to choosing the correct concentration of both local anaesthetics and adrenaline. Local anaesthetics are commonly referred to with regards to a percentage concentration. Using the example of lidocaine, 1 ml of 1% lidocaine contains 10 mg of local anaesthetic whereas 1ml of 2% lidocaine contains 20 mg of local anaesthetic. Importantly, adrenaline concentration is named differently, whereby 1 mL of 1:1000 adrenaline contains 1 mg of adrenaline. The amount of adrenaline added to a local anaesthetic mixture will vary depending on intended use and clinician preference; however, a commonly used preparation in primary care includes adrenaline at a concentration 1:200 000.
The initial subcutaneous injection of local anaesthetics is painful, and is often the most unpleasant part of minor procedures (Zilinsky et al., 2005). It is possible to anaesthetise an area inflicting minimal pain; however, this requires the user to establish an effective technique. Prior preparation of the local anaesthetic by warming the solution to body temperature or by the addition of bicarbonate (in order to better match the pH of the solution to the pH of the skin) can reduce pain on injection, however, the amount of bicarbonate needed in order to ‘neutralise’ the local anaesthetic in the volumes that are often used in primary care is extremely small, and may potentially lead to complications of inaccurate drug dilution, and so is perhaps best avoided. A simpler approach to minimising pain on injection of local anaesthetic may be to use a smaller gauge needle (27G or 30G) and not repeatedly using the same needle, as this leads to a gradual blunting. Although the use of these smaller needles may be effective in minimising pain, with a reduction in gauge often comes a reduction in needle length, therefore increasing the number of dermal punctures required to anaesthetise a larger area. When choosing the most appropriate needle for local anaesthetic infiltration, it may be best to first consider the size and shape of the area to be anaesthetised, and selecting a needle that best compromises gauge with the number of fresh skin punctures that will be required.
Simple distraction techniques (both conversational and tactile) as well as ‘looking away’ have also been shown to reduce perceived pain on injection. Paying careful attention to the manipulation of one’s needle is also important in reducing injection-associated pain. By injecting into the subdermal layer (rather than intradermal), at a 90° angle to the skin and using an ‘inject, stop and go’ technique all help to reduce local anaesthetic-related pain. By ensuring the bleb of local anaesthetic is at least 10 mm in front of the needle tip at all times helps ensure that further advancements of the needle are only ever into already anaesthetised tissue (Strazar et al., 2013).
Topical
Local anaesthetics are also available in topical preparations. These preparations have the advantage of being very easy to apply and are often utilised in the anxious or non-compliant adult or child. There are a number of local anaesthetic creams available; however, a eutectic mixture of local anaesthetic (EMLA) and Ametop are two that are commonly used. EMLA cream is a mixture of lidocaine and prilocaine. Combining these two local anaesthetics allows the otherwise crystalline solid compounds to form an oil mixture, due to a reduction in boiling point (Peck et al., 2008). Application of the cream followed by a clear dressing 60 minutes prior will provide satisfactory analgesia for minor interventions lasting less than 2 hours, such as venesection or cannulation (Emla, 2019). The cream should not be applied to mucus membranes (due to increased systemic absorption) and should be used in caution in those with known methaemoglobinaemia or in those taking predisposing medications. Ametop is a topical preparation of tetracaine and may be used similarly to EMLA, however, has a quicker onset (30 minutes) and longer action (3 to 4 hours), however, it may cause some local skin irritation and erythema due to vasodilatation (Peck et al., 2008).
Other uses of local anaesthetics
As well as being used in minor surgery and in aiding venepuncture and cannulation, local anaesthetics may have a number of other uses in primary care. These include in the treatment of post-herpetic neuralgia, aphthous ulcers or haemorrhoids.
The National Institute for Health and Care Excellence (NICE) suggests that along with simple analgesia and neuropathic analgesics (e.g. amitriptyline), post-herpetic neuralgia may be treated using lidocaine plasters if the pain is mild, if there are concerns regarding central nervous system side effects of oral medications or as an adjunct to oral medications if pain is severe. Each plaster contains 5% lidocaine and should be worn for a maximum of 12 hours, followed by a 12-hour break in order to help prevent skin irritation. These plasters may be cut to fit the area of pain, or two to three plasters may be combined in order to achieve a wider area of anaesthesia. It is suggested that this treatment is reviewed at regular intervals (every 2 to 4 weeks) and that if no benefit is perceived, treatment should be discontinued (NICE, 2017a).
Disorders of the gastrointestinal tract may also be treated with local anaesthetic preparations. Lidocaine-containing sprays or ointments can be utilised in the symptomatic treatment of aphthous ulcers and should be applied sparingly as required (NICE, 2017b).
Analgesia for painful haemorrhoids may be achieved with topical local anaesthetics, however, caution is advised due to the potential of sensitisation of the anal skin, and such should only be used for a few days at a time. Lidocaine-containing preparations are preferred, as these preparations are generally very well tolerated, however, local skin reactions can occur, and include burning, itching or irritation (NICE, 2016).
Many of these creams, sprays, gels and ointments are available to purchase without prescriptions over the counter (including those used in the management of minor ailments such as sore throat and haemorrhoids), and so patients may be encouraged to seek advice from a pharmacist in these circumstances.
Side effects and toxicity
Below the suggested maximum weight-based dose, local anaesthetics are very well tolerated and adverse reactions are rare. As previously discussed, allergy is possible and is usually due to the production of PABA, a metabolite of the ester local anaesthetics (Peck et al., 2008). Local anaesthetics are a recognised cause of acquired methaemoglobinaemia, whereby iron within haemoglobin molecules is fixed in the ferric (Fe3+) form and so is unable to effectively bind oxygen, leading to cyanosis (Barash et al., 2015).
Although this complication is rare, and is more often associated with procedures involving the use of local anaesthetic on mucus membranes (e.g. for bronchoscopy or gastrointestinal endoscopy), it has also been described following locally injected anaesthetics. Patients who are at highest risk of the development of methaemoglobinaemia include those with comorbidities that already impair oxygen transport (such as chronic obstructive pulmonary disease and anaemia) or in those with significant liver disease (Barashet al., 2015). Other side effects are more related to particular preparations rather than systemic effects (e.g. pain on injection or skin irritation in response to topical formulations).
In the event of local anaesthetic overdose, or significant inadvertent intravascular injection, severe toxicity can occur. Signs and symptoms of local anaesthetic toxicity can generally be classified into either neurological in origin (agitation, altered mental status, perioral tingling and loss of consciousness, with or without seizure activity) or cardiovascular (bradycardia, conduction blocks, asystole and ventricular tachyarrhythmias). It is, however, worth considering that many of the described neurological side effects may be observed in an extremely anxious or significantly needle phobic patient and so local anaesthetic toxicity may be considered a differential diagnosis in these circumstances.
Should cardiac arrest occur, basic life support should be initiated immediately as per resuscitation council guidelines and urgent transfer to a clinical area with appropriate equipment and personnel should be arranged. Further treatment in the event of severe local anaesthetic toxicity includes infusion of an intravenous lipid emulsion (e.g. Intralipid) and ongoing supportive care (Association of Anaesthetists, 2010).
KEY POINTS
Local anaesthetics are safe medications when used correctly and have multiple uses in primary care There are a wide range of local anaesthetic options for subcutaneous injection, with varying pharmacological properties, therefore it is important to select the most appropriate local anaesthetic for the clinical indication There are multiple indications for topical anaesthetic preparations, including for the treatment of post-herpetic neuralgia, haemorrhoids and aphthous ulcers Care must be taken to ensure the maximum dose of local anaesthetic is not exceeded Local anaesthetics are generally well tolerated and side effects are rare, however, there is potential for toxicity
ORCID iD
Gareth Allen https://orcid.org/0000-0002-2286-4403