
Abstract
Thyroid swellings are relatively common; they are three times more common in females than males. The incidence of palpable nodules is approximately 5% in women and 1% in men. Thyroid cancer constitutes less than 1% of all malignancies registered in the UK, with an incidence of approximately 5 per 100 000 women and 2 per 100 000 men. However, thyroid cancer is the most common endocrine malignancy and accounts for more than 90% of cancers of the endocrine glands. Over the last decade the incidence of thyroid cancer in the UK has increased by more than two-thirds (68%).
Clinical case scenario
A 45-year-old gentleman presents to your surgery with a swelling on the front of his neck, he first noticed it 3 weeks ago and it is growing in size. The lump itself is painless. He has no other medical problems. He is anxious about what the lump is, as there is a history of cancer in his family.
Anatomy of the thyroid gland
The thyroid gland is a butterfly-shaped endocrine gland, located in the anterior neck, extending between the C5 and T1 vertebrae. It encircles the anterior and lateral aspects of the upper trachea. It has two lateral lobes that are connected anteriorly by an isthmus. Sometimes there is a superior extension near the midline known as the pyramidal lobe (Bliss et al., 2000). The trachea and oesophagus lie medial to each lobe, the carotid sheath postero-laterally, and the sternocleidomastoid and strap muscles (sternohyoid, sternothyroid, and superior belly of the omohyoid) are on the anterolateral surface. The thyroid gland is enclosed in a thin capsule, derived from pretracheal fascia. This capsule condenses near the cricoid cartilage and upper tracheal rings and forms the posterior suspensory, or Berry’s, ligament. (Fig. 1)
Anatomy of thyroid gland.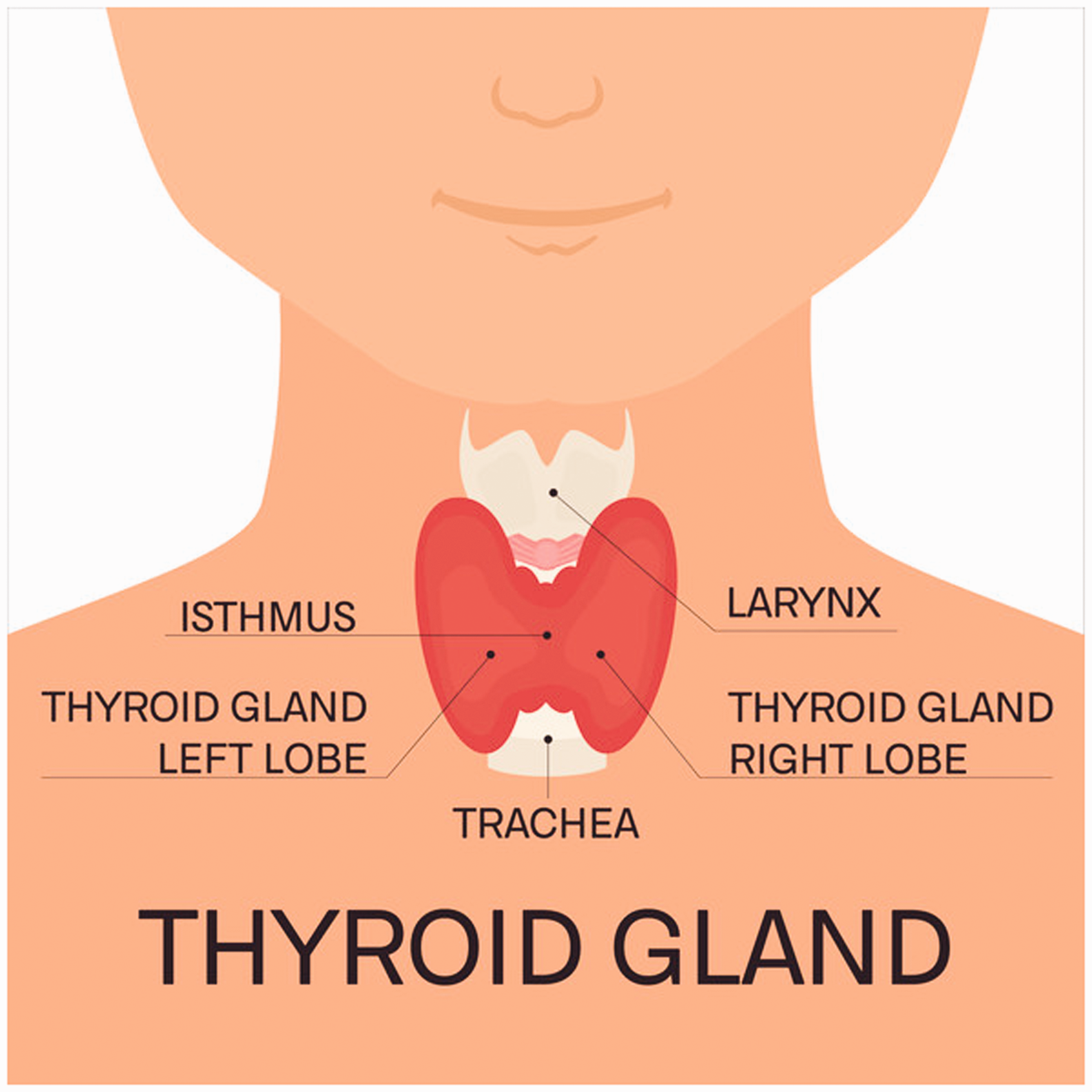
The thyroid gland is highly vascularised. The superior thyroid artery, a branch of the external carotid artery, supplies the superior and anterior portions of the gland. The inferior thyroid artery, arising from the thyrocervical trunk (a branch of the subclavian artery), supplies the posteroinferior aspect of the gland. In up to 15% of the population, there is an additional artery present, the thyroid ima artery (Chin et al., 2019), which comes from the brachiocephalic trunk of the arch of aorta, supplying the inferior surface and isthmus. The venous drainage is via the superior, middle and inferior thyroid veins, which form a venous plexus. The superior and middle veins drain into the internal jugular veins, whereas the inferior drains into the brachiocephalic vein. Lymphatic drainage of the thyroid gland is into the peri-thyroid nodes and from there into prelaryngeal, pretracheal and paratracheal nodes. Laterally the gland drains into the superior and inferior deep cervical nodes.
The thyroid gland is vital in controlling normal metabolism, growth, and many other bodily functions. The main hormones produced by the thyroid gland are thyroxine or tetraiodothyronine (T4) and triiodothyronine (T3). The thyroid gland, anterior pituitary gland, and hypothalamus form a self-regulatory circuit called the hypothalamic–pituitary–thyroid axis (Fig. 2). The hypothalamus releases thyrotropin-releasing hormone (TRH) into the hypothalamic–hypophyseal portal system to act on the anterior pituitary gland (Mallya and Ogilvy-Stuart, 2018). TRH stimulates the anterior pituitary to release thyroid-stimulating hormone (TSH). TSH is released into the blood and binds to the thyroid-releasing hormone receptor on the thyroid follicular cells. This leads thyrocytes in the thyroid follicles to synthesise a protein called thyroglobulin (TG), whilst Na+-I- symporters transport iodide (initially absorbed from the small intestine) into the thyrocytes. The enzyme thyroid peroxidase (TPO) oxidises iodide (I-) to iodine and links tyrosine residues of TG protein with iodine. TPO then combines iodinated tyrosine residues to make triiodothyronine (T3) and tetraiodothyronine (T4). These thyroid hormones are lipophilic and circulate bound to transport proteins. Only a fraction (∼0.2%) of the thyroid hormone is unbound and active – free T4 (Mughal et al., 2018).
Physiology of thyroid gland.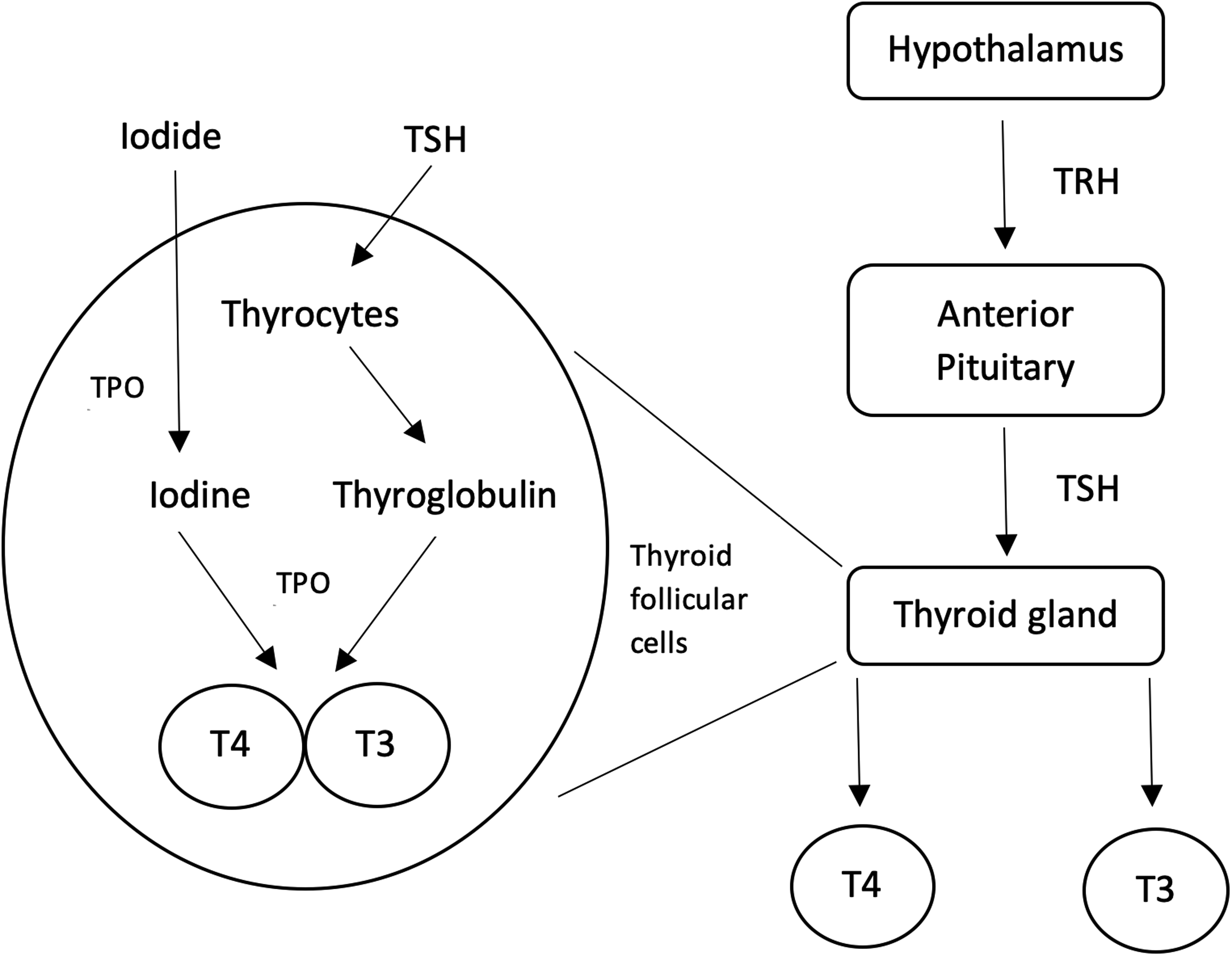
Thyroid swellings
Thyroid swellings can generally be thought of as goitres (diffuse or nodular) or nodules. The description for each follows.
Diffuse goitre
An enlarged thyroid gland is called a goitre. A physiological goitre is seen during puberty and pregnancy, due to increased metabolic demand. It is necessary to check thyroid hormones in a patient with a physiological goitre and ensure the levels are adequate.
Goitres secondary to iodine-deficiency are now typically only seen in iodine-depleted areas of the world, including the mountainous regions of Europe, the Northern Indian Subcontinent, the extensive mountain ranges of China, the Andean region in South America and the lesser ranges of Africa are all iodine deficient. The Ganges Valley in India, the Irawaddy Valley in Burma, and the Songkala valley in Northern China are also areas of endemic iodine deficiency. Iodinised salt and other forms of food supplementation are used in these regions to overcome the deficiency (Eastman et al., 2018). The recommended daily intake of iodine for an adult (140 micrograms) is generally fulfilled by a balanced diet.
Diffuse goitre is also seen in auto-immune thyroid disorders such as Graves’ disease, Hashimoto’s thyroiditis and post viral thyroiditis.
Nodular goitre
An enlarged thyroid gland with multiple nodules is called a multi-nodular goitre and commonly seen in Graves’ disease.
Solitary nodule
A solitary thyroid nodule can be benign (euthyroid or hyperthyroid) or malignant.
Euthyroid benign nodules can be:
Colloid nodule: Benign overgrowth of thyroid tissue and most common type of thyroid nodule Follicular adenoma: Benign neoplasms arising from follicular epithelium within the thyroid, they tend to be solitary homogenous nodules Simple or haemorrhagic cysts
Benign nodules that become hyperthyroid are referred to as toxic adenomas, or ‘hot nodules’. This is typically due to TSH receptor pathway mutations (Trülzsch et al., 2001). These hot nodules carry a 1% chance of malignant transformation. Multiple functional benign nodules lead to a toxic multi-nodular goitre.
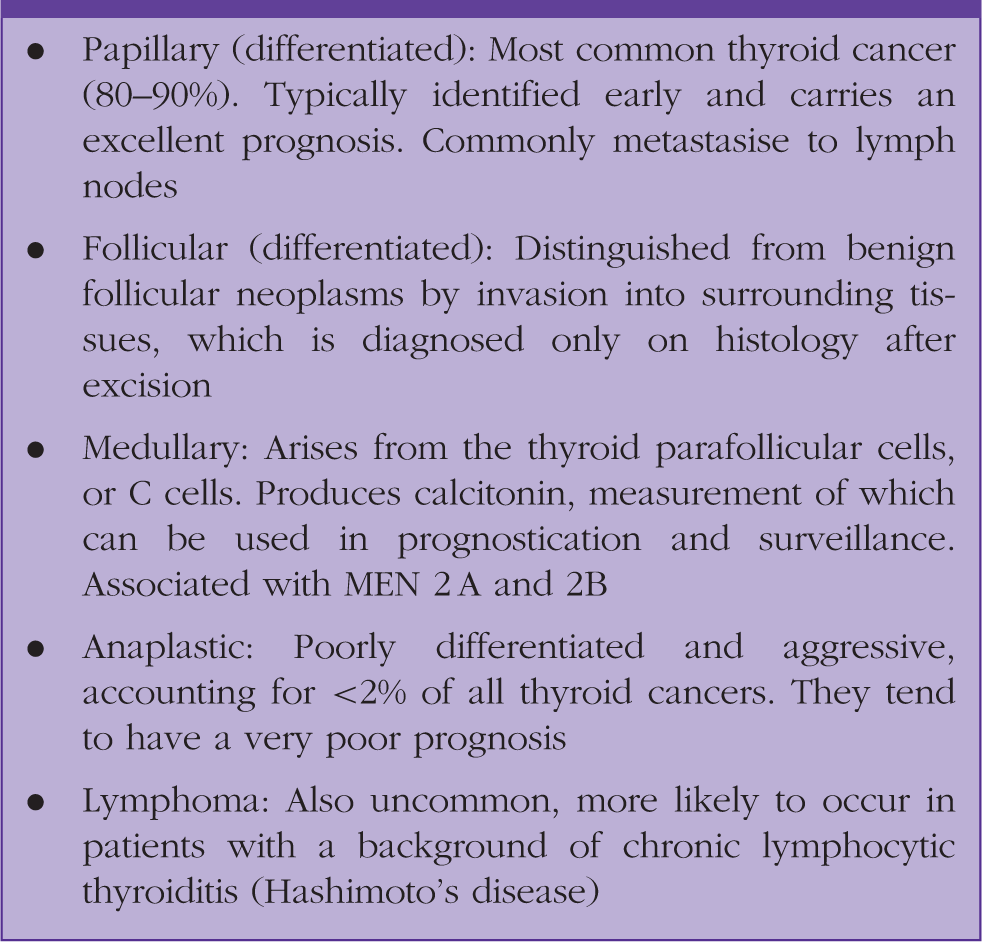
Malignant nodules.
Assessment and management of thyroid swelling
History
When a patient presents with an anterior neck swelling, thyroid gland disorders should be included in the differential diagnosis. A history detailing the onset, duration and progression of the swelling should be elicited.
A history of sudden increase in size suggests haemorrhage into the swelling or an aggressive tumour. Any change in the patient’s voice, swallowing symptoms, breathing symptoms or neck lumps should be elicited. Hoarseness is a red flag. Dysphagia or dyspnoea suggest compression of the oesophagus or trachea, respectively, by a large thyroid swelling or infiltration by cancer. The presence of cervical lymphadenopathy suggests lymphatic involvement in thyroid cancers.
Symptoms and signs of thyroid dysfunction.

A history of radiation exposure, particularly at a young age should also be elicited, as this is associated with an increased risk of thyroid cancer (Tucker et al., 1991). The patient’s history of smoking and alcohol intake should also be documented. Smoking increases the risk for thyroid cancer. Alcohol has a suppressive effect on thyroid function.
Family history may be significant, particularly where there is a history of genetic conditions. For example, medullary thyroid cancer is associated with MEN 2A and MEN 2B genes (Moo-Young et al., 2009)
Examination of thyroid swelling
Examination should focus on signs of thyroid gland dysfunction and detailed assessment of any swellings. Assess for tremor, skin and hair changes, muscle wasting, hyper dynamic circulation – tachycardia, widened pulse pressure, atrial fibrillation, increased resting heart rate, changes in reflexes and signs of thyroid eye disease (as seen in Graves’ disease). Thyroid swellings move with swallowing, as they are enclosed within the pretracheal fascia. All structures within the pretracheal fascia move with deglutition. The suspensory ligament of the thyroid gland, or Berry’s ligament, attaches to the cricoid cartilage causing the gland to move with deglutition. Neck examination should enable a clear description of the thyroid swelling detailing site, size, surface, consistency, contour, tethering, tenderness and temperature. Other important features include the relation to swallowing and the presence or absence of palpable lymph nodes.
Red flag features for malignancy on examination include (Hegedüs, 2004):
Nodule size of >4 cm Firm on palpation Fixation to surrounding tissues Cervical lymphadenopathy Vocal cord paralysis (evidence of voice changes)
Remember that thyroglossal duct cysts are a common cause of midline neck masses. They are found anywhere from the tongue base to the isthmus of the thyroid. They can be differentiated from a thyroid swelling by the fact that thyroglossal cysts move both with deglutition and tongue protrusion. There are some non-thyroidal causes of neck swelling that may be mistaken for thyroid nodules, including, for example, enlarged parathyroid glands and rarely, metastases to the thyroid gland.
Referral
Differentiating between different types of thyroid nodule is challenging in primary care. Ultimately, a thyroid swelling needs assessment in secondary care (ENT, general surgeon or endocrinologist). Referral pathways differ depending on the organisation of local services. However, any neck swelling suspicious of cancer should be referred to secondary care on the appropriate urgent suspected cancer (USC) pathway.
Referral criteria for thyroid lump.
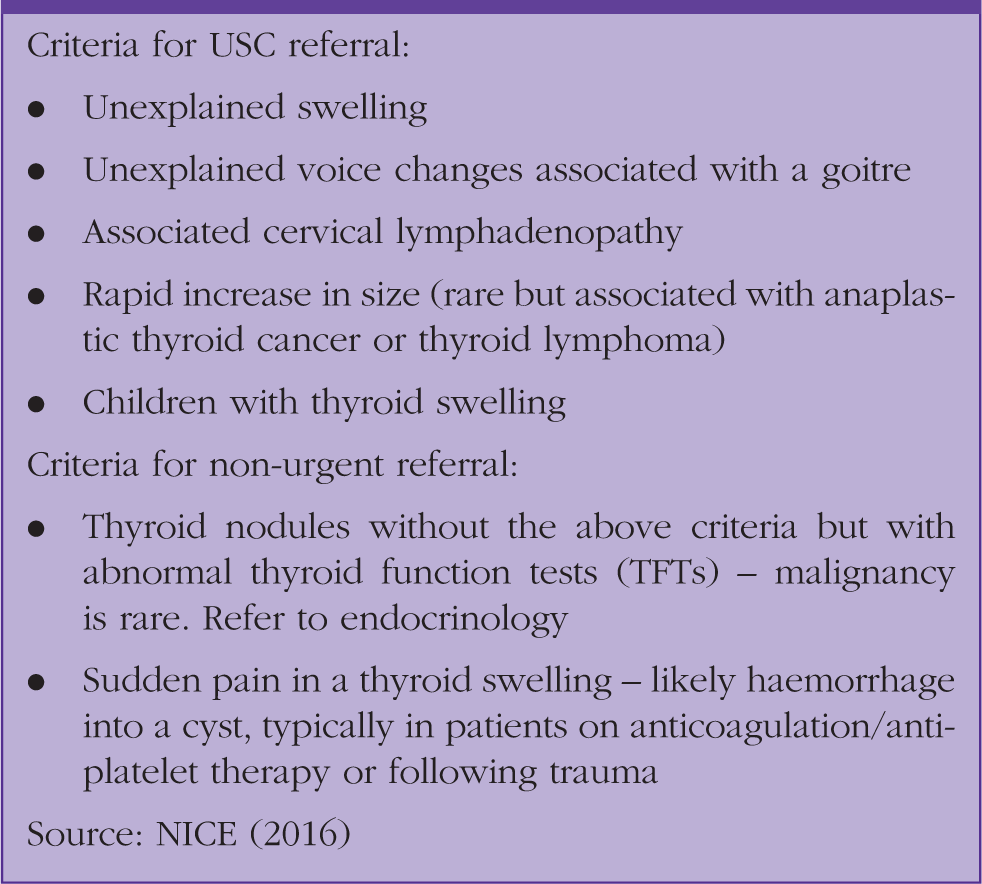
In our clinical case scenario the patient presenting to the surgery is a 45-year-old male with a family history of cancers. An unexplained, painless and progressively enlarging neck swelling needs a thorough assessment. Once confirmed on examination to be a thyroid swelling, it requires a USC referral and thyroid function tests. Further investigation in secondary care includes ultrasound and ultrasound-guided aspiration for cytology.
KEY POINTS
A normally functioning thyroid gland is essential for good health; tests of thyroid function should be initiated in primary care but should not delay referral Thyroid swellings are goitres or nodules; nodules may be singular or multiple and benign or malignant Thyroid cancer remains relatively rare, but the incidence is increasing A thyroid swelling associated with hoarseness, dysphagia, dyspnoea, increasing size or cervical lymphadenopathy needs USC referral Referral should be based on local pathways depending on the suspected pathology Thyroid function tests followed by ultrasound and possible FNAC are the appropriate initial investigations in secondary care for a thyroid swelling