
Abstract
Bell's palsy is the term given to an idiopathic lower motor neurone facial nerve paresis or paralysis. It is of rapid onset, almost always unilateral, and may be associated with facial or retro-auricular pain or otalgia. It is the most common diagnosis associated with facial nerve palsy; a GP will see a case approximately every 2 years in practice in the United Kingdom. Early diagnosis and steroid treatment increase the likelihood of full recovery, whereas ocular complications can be prevented by lubricants and lid taping. Over 70% of patients recover within a year. Options to improve facial appearance and function, in those who do not experience a complete recovery, include surgery.
Clinical case scenario
Jess, a 40-year-old café manager, attends your morning surgery. She was seen in accident and emergency (A&E) 48 hours ago with a left-sided facial weakness, which appeared over 2 days. She was given a diagnosis of Bell’s palsy, a 10-day tapering course of oral prednisolone and advised to see her GP for follow-up. Jess admits she was relieved when the A&E doctor excluded a stroke, however, she hurriedly left the department thereafter due to embarrassment over what she perceived to be time-wasting. Jess seeks further information regarding the condition, management and prognosis. She denies any additional symptoms other than irritation of the eye on the left side. How would you advise and manage this patient?
Background and epidemiology
Although anatomist Charles Bell gave his name to the condition in 1821, unilateral facial palsy has been described throughout history. ‘Palsy’ describes both paresis (incomplete weakness) and paralysis (total loss of function). Determining the incidence is challenging, as patients may not always seek medical attention and are seen in a mixture of care settings. The peak age group affected is between 15 and 45 years old. The estimated prevalence in the United Kingdom is 20 per 100 000. A GP in the UK will therefore see a case approximately every 2 years (Gilden, 2004; Holland and Weiner, 2004). There is no significant difference in incidence between ethnicities or males and females, although incidence increases in pregnant women (45 per 100 000), those with recent upper respiratory tract infections, the immunocompromised and in diabetes and hypertension (Eviston et al, 2015; Peitersen, 2002).
Anatomy
The facial nerve is composed of motor fibres (innervating the muscles of facial expression, posterior belly of digastric, stylohyoid and stapedius), parasympathetic fibres (innervating the lacrimal, submandibular and sublingual salivary glands), somatic afferents (from the external ear) and afferent taste fibres from the anterior two thirds of the tongue. The facial nerve (motor root) exits the brainstem at the lower aspect of the pons in the cerebellopontine angle and the nervus intermedius (sensory and parasympathetic secretomotor fibres) emerges between the pons and the inferior cerebellar peduncle (Ellis and Mahadevan, 2013; Sinnatamby, 2011).
Both parts of the nerve pass into the internal auditory meatus in the petrous temporal bone, travelling with the VIIIth nerve until they enter the facial canal (see Fig. 1). The genu of the facial nerve describes a sharp bend over the promontory of the middle ear where the secretomotor fibres for the lacrimal gland leave via the greater petrosal nerve, and the facial nerve travels inferiorly, in the medial wall of the middle ear cavity. Within the facial canal, the nerve to stapedius and chorda tympani are also given off before the facial nerve enters the stylomastoid foramen. The chorda tympani runs between incus and malleus in the middle ear, entering the infratemporal fossa to join the lingual nerve, carrying taste fibres from the anterior tongue and secretomotor fibres to the submandibular ganglion, supplying the submandibular and sublingual salivary glands (Ellis and Mahadevan, 2013; Sinnatamby, 2011).
Facial nerve anatomy.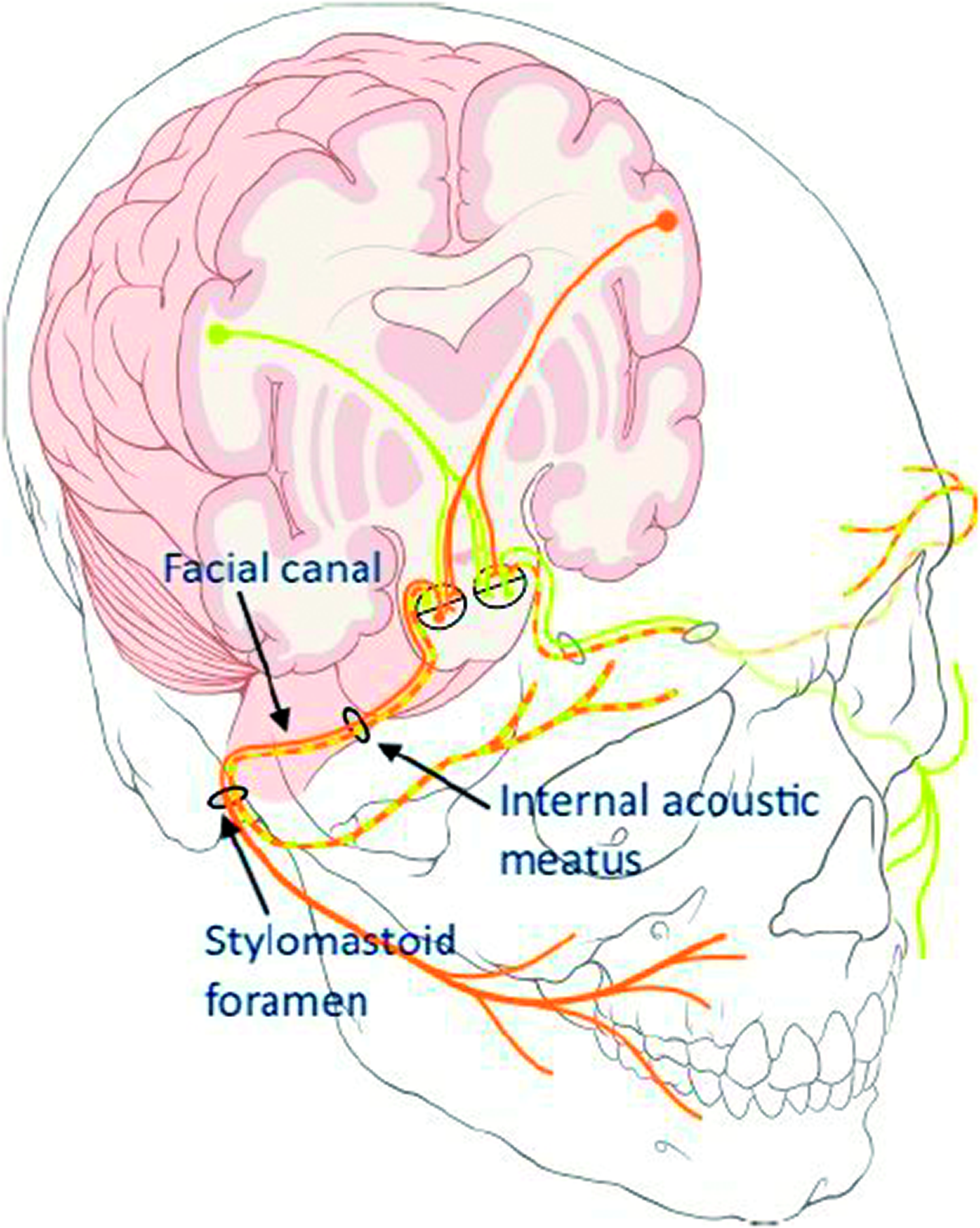
Stylohyoid and the posterior belly of digastric muscle are supplied by the nerve on its exit from the stylomastoid foramen, before it enters the parotid gland. The five (temporal, zygomatic, buccal, mandibular and cervical) divisions that arise within the parotid gland innervate the muscles of facial expression (Ellis and Mahadevan, 2013; Sinnatamby, 2011).
Aetiology
Bell’s palsy is idiopathic by definition, and is a diagnosis of exclusion, being the term used for peripheral nerve palsy without a defined cause. A clear understanding of the common and serious differentials is, therefore, required to exclude these and reach the diagnosis.
Despite its idiopathic status, several theories on the underlying aetiology of Bell’s palsy have been proposed, including viral and ischaemic options. Inflammation of the facial nerve and resultant compression in the facial canal is implicated in many of these theories and is reflected in histopathological review. Polymerase chain reaction analysis has demonstrated herpes simplex virus (HSV) type 1 DNA in endoneurial fluid from affected patients (Murakami et al., 1996). The theory that reactivation of latent herpes viruses (HSV and herpes zoster virus, HZV) underlies most cases is increasingly popular (Eviston et al., 2015; Holland and Weiner, 2004; Peitersen, 2002). Pregnancy increases the risk of Bell's palsy, and there appears to be an association with preeclampsia, suggesting that extracellular oedema may be causative in pregnant women (Katz et al., 2011).
An association between an intranasal vaccination and Bell's palsy has been previously demonstrated, potentially specific to the combination of heat labile toxin-derived molecules administered via the intranasal route (Lewis et al., 2009). The incidence of Bell’s palsy in recipients of some SARS-CoV-2 vaccines has been reported to be higher than the general population (Cirillo and Doan, 2021), although at the time of writing, the Medicines and Healthcare Products Regulatory Agency has not established a difference in rate of Bell’s Palsy between vaccinated individuals and the general population (Medicines and Healthcare Products Regulatory Agency, 2021). Given the evolving nature of this topic, up-to-date pharmacovigilance findings (such as the Yellow Card reporting system) and guidance should be consulted when offering vaccine advice to patients, including those with previous Bell’s palsy.
Diagnosis
History
Misdiagnosis is common in Bell's palsy, and GPs should be aware of important and urgent differentials for exclusion. Patients will present with an (almost always) unilateral facial weakness, developing within 3 days. This can vary from slight weakness to total paralysis of the affected muscles and may be recognisable at rest as drooping of the eyebrow/mouth and loss of the nasolabial fold (Fig. 2). The weakness may be associated with postauricular (52%), facial or ear pain or altered taste (34%), hearing (hyperacusis in up to 14%) or lacrimation (increased or decreased) on the affected side. Occasionally, weakness of orbicularis ori may result in drooling or difficulty articulating, but as with all symptoms, central causes must be excluded before Bell's palsy is considered (Mettias et al., 2019; National Institute for Health and Care Excellence (NICE), 2019; Peitersen, 2002).
Bell's palsy in a male patient, demonstrating right-sided facial weakness. Note the inability to raise the right eyebrow (LMN lesion). In UMN lesions (i.e. central cause), forehead sparing is seen.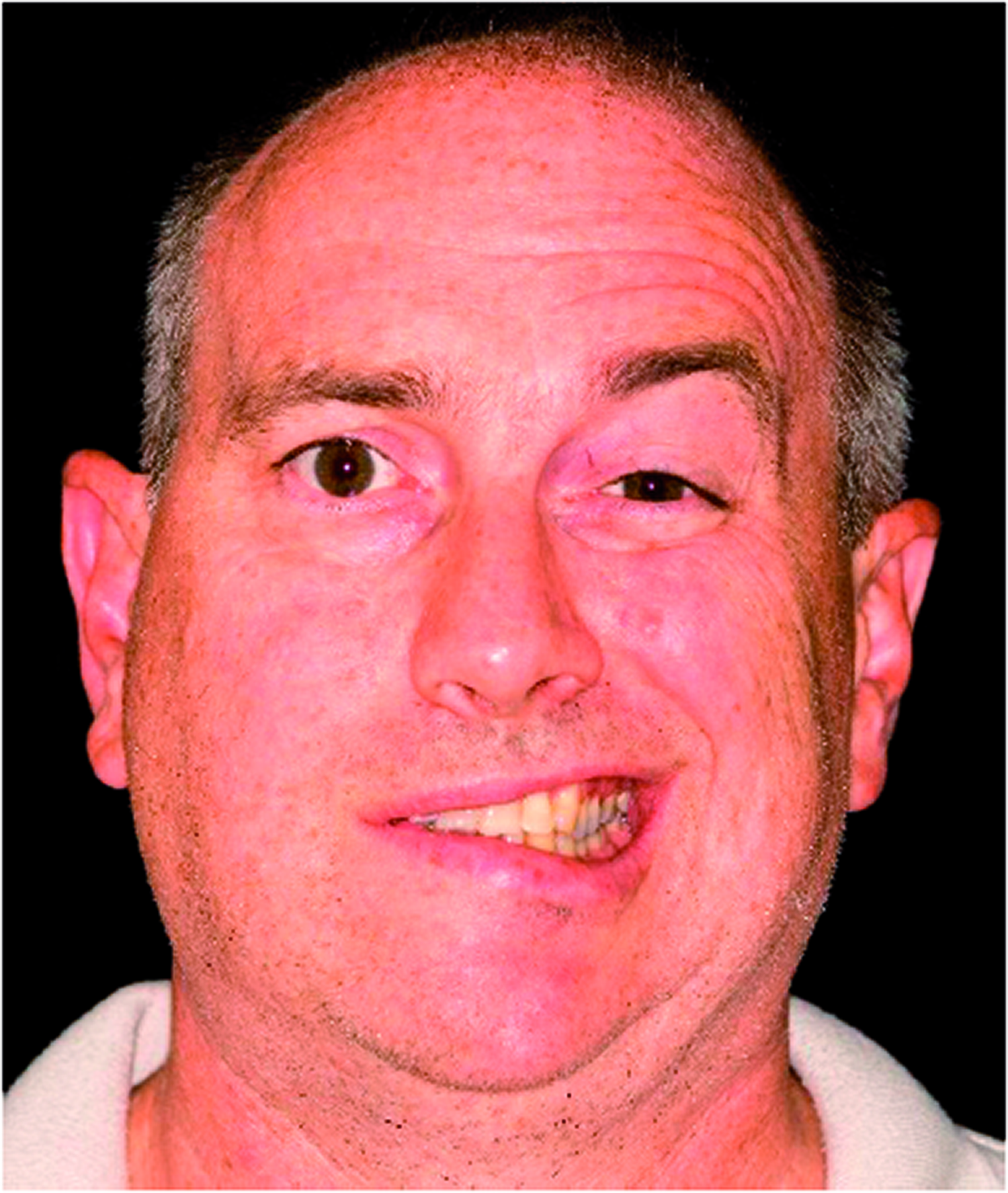
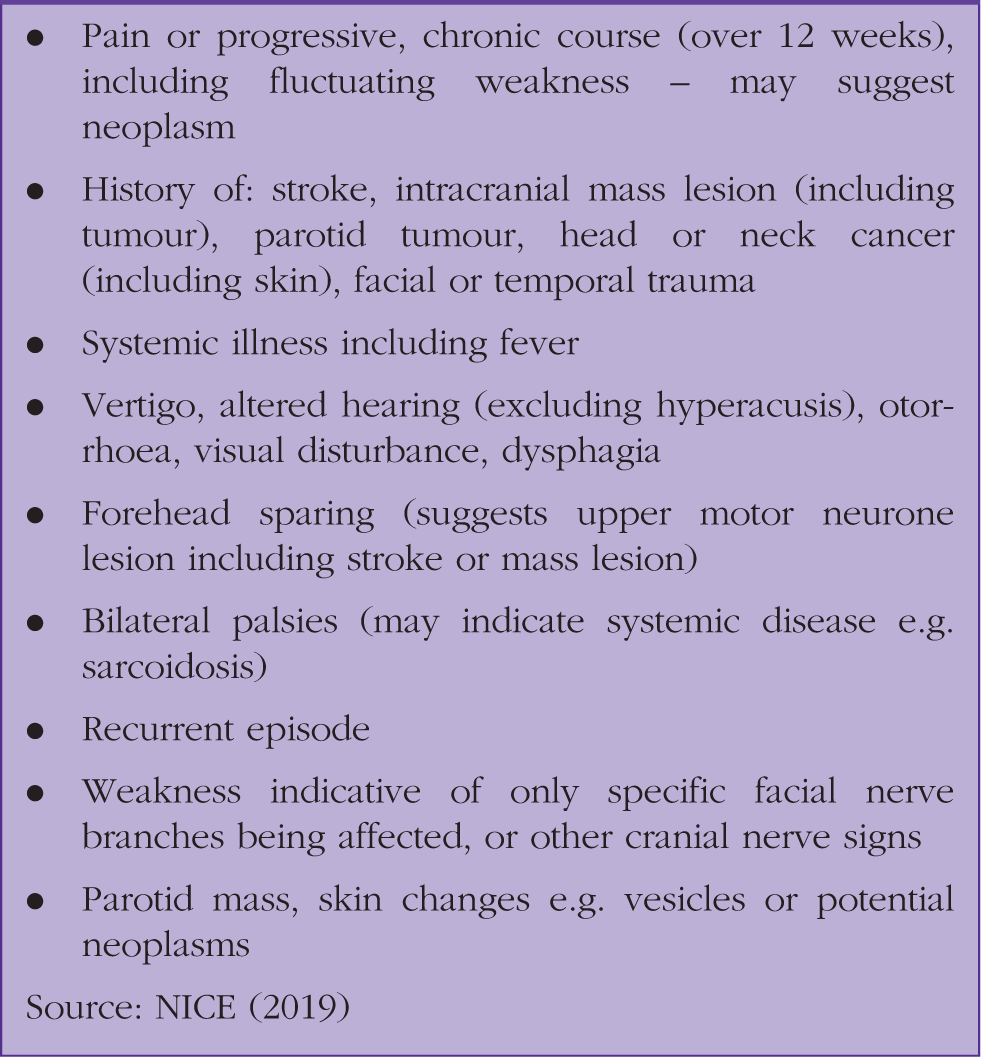
Atypical features which should prompt referral to exclude other causes.
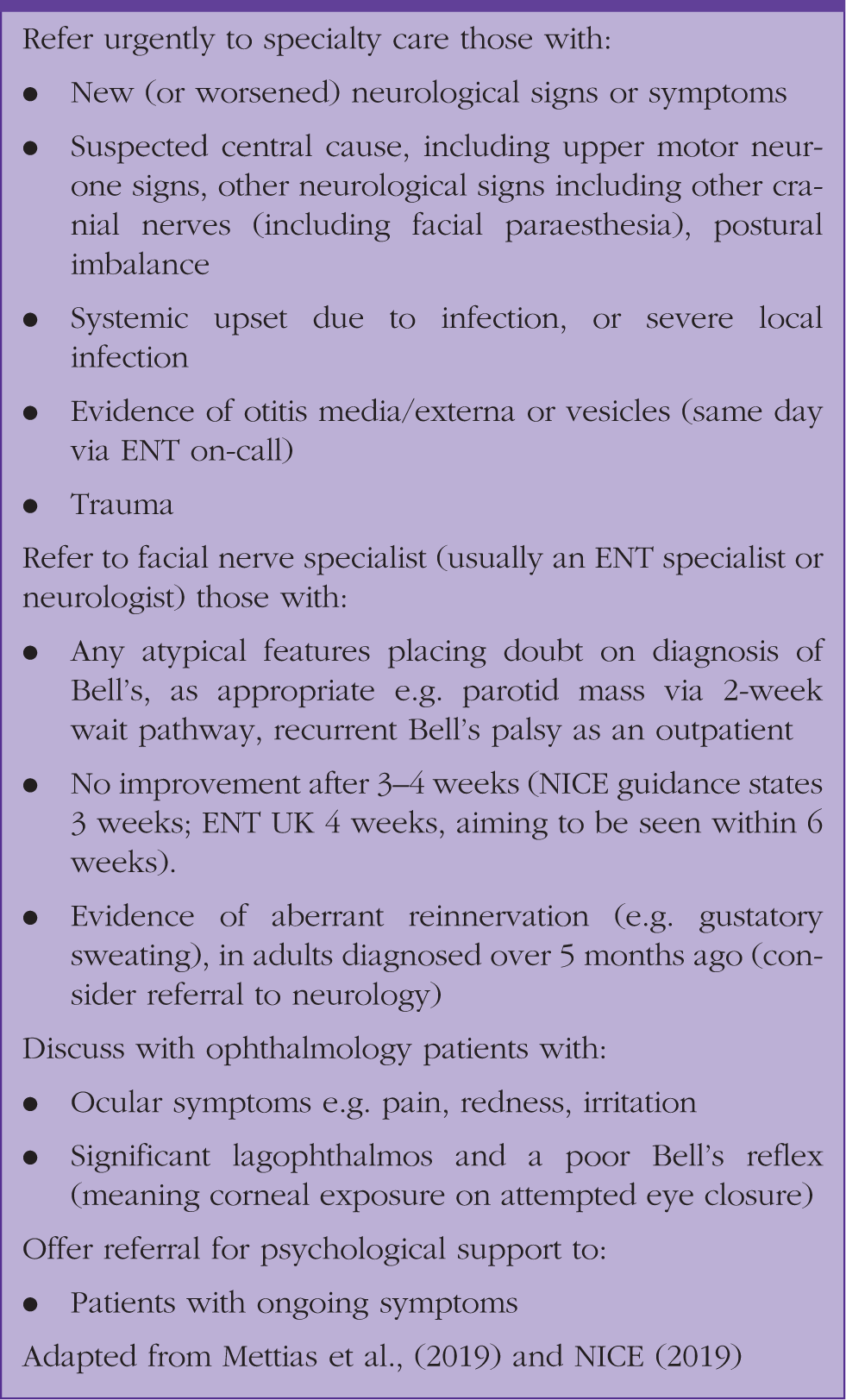
Referral to secondary care.
Examination
House– Brackmann scale of facial weakness. Many methods of measuring facial weakness have been described, but the aim is providing an objective measure which can be used by different clinicians. Of note, grade IV represents loss of eye closure.
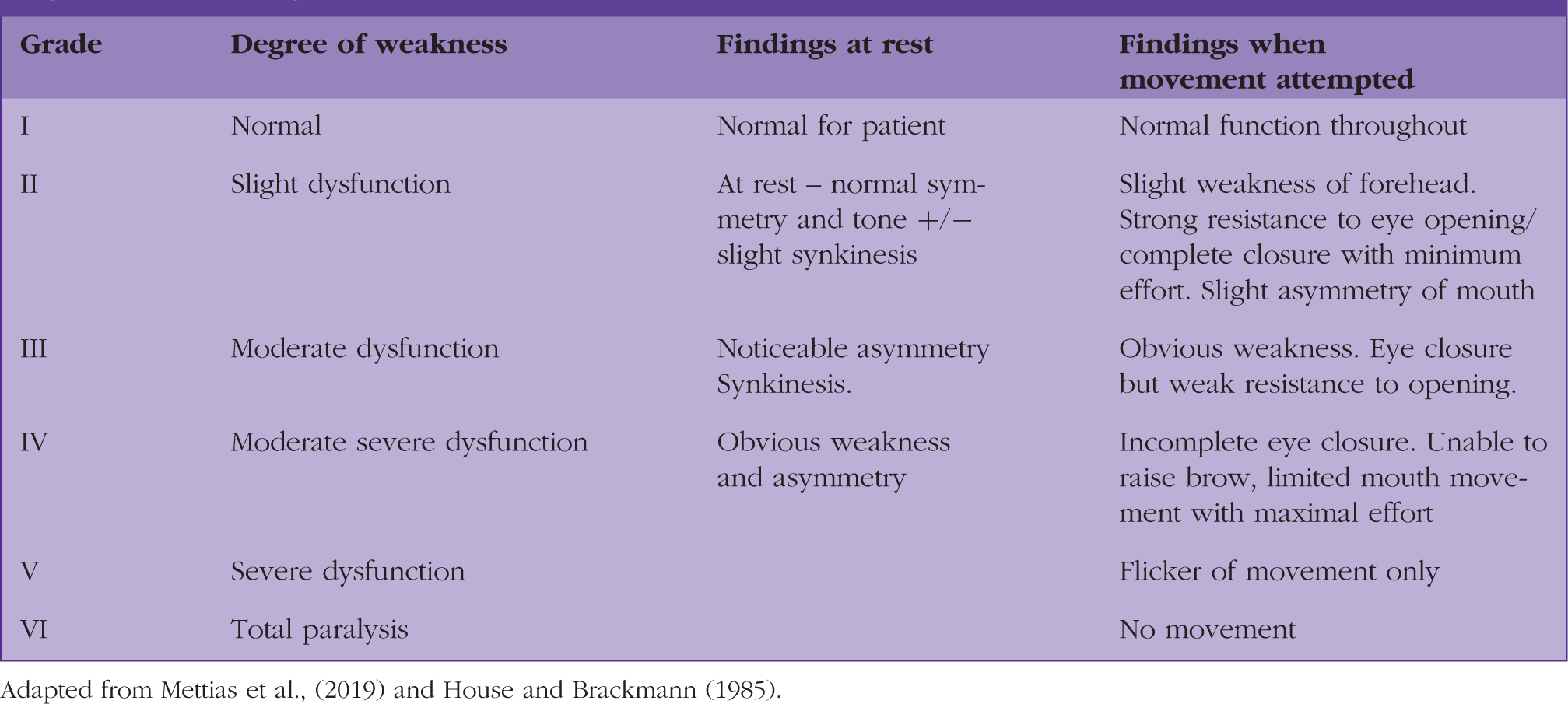
Adapted from Mettias et al., (2019) and House and Brackmann (1985).
Differential diagnoses for facial weakness.
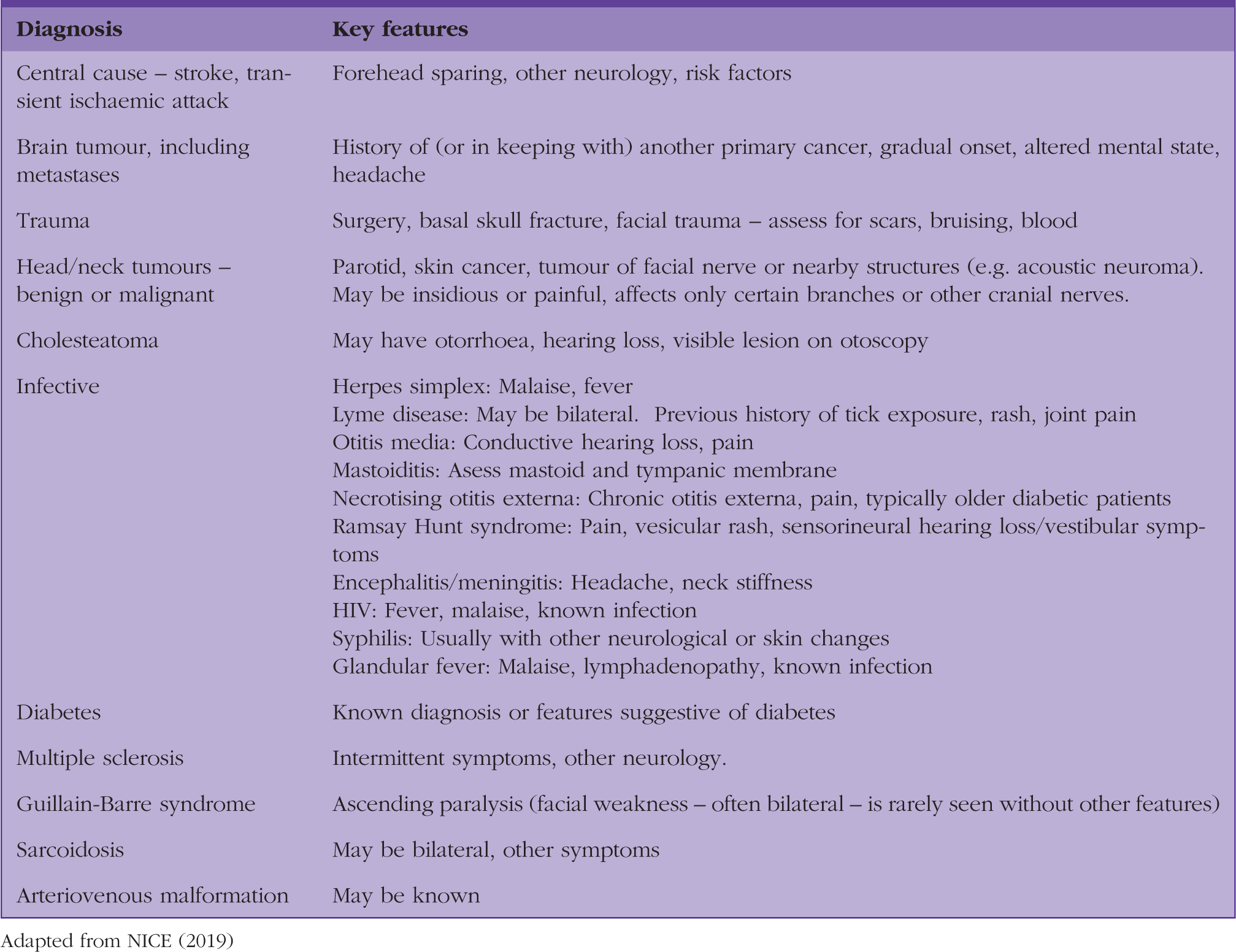
Adapted from NICE (2019)
Particular note should be made of the patient’s ability to close their eyes, including unresisted at minimal effort and against resistance. This helps to adequately assess the risk to the eye – a patient who must use conscious effort to close the eye in the absence of resistance will not achieve full eye closure when blinking or asleep. Bell’s phenomenon (the upward movement of the eye when attempting to close it, see Fig. 3) is a reflex to protect the cornea, it is found in most people (Jones, 2001). This reflex is not pathognomonic of Bell's palsy, although it may be more easily noticed when eye closure is lost. In these cases, it has a defensive role, but eye care is still required.
Bell’s phenomenon, seen on the left eye in a patient with left-sided facial weakness, demonstrating that the cornea may be exposed despite this protective reflex.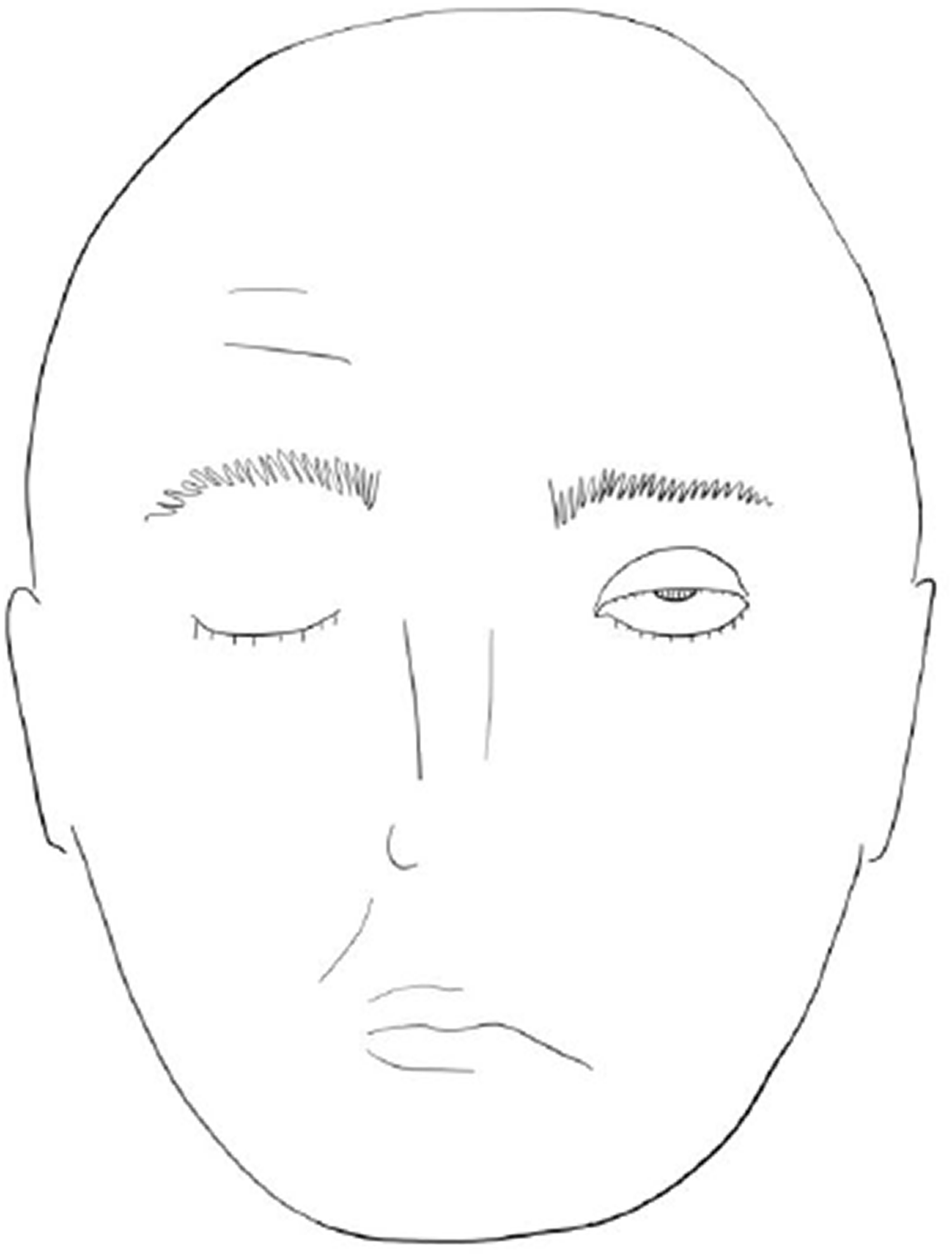
A full neurological examination to exclude a central cause must be undertaken for all cases. Once an UMN palsy, other neurological symptoms or signs, and bilateral weakness, have been excluded, examination to assess for other causes of LMN facial palsy should be undertaken. Perform an ear, nose and throat (ENT) examination, including the scalp and skin, mastoid region, parotid gland (for masses) and tympanic membranes. Visualise the attic when examining the tympanic membrane in order to help assess for cholesteatoma (see Fig. 4). A thorough examination of the oral cavity/pharyngeal mucosa, skin and external auditory canal should be undertaken to assess for scabbing or vesicles, in keeping with zoster infection. Ramsay Hunt syndrome typically presents with pain, sensorineural hearing loss and a vesicular rash on the ear or oropharynx.
Attic cholesteatoma with retraction pocket, seen as a crusty mass on otoscopy, although it may appear white or wax-like.
Atypical features, not in keeping with Bell's palsy, are found in Box 1. In a unilateral LMN weakness with no atypical features, no other neurology and no other cause found (see Table 2), a diagnosis of Bell's palsy may be made in primary care without the need for laboratory tests or diagnostic imaging (NICE, 2019).
Management
Management of Bell's palsy should take into account severity of the palsy, including eye closure, timing of presentation and the patient’s suitability for corticosteroid treatment. Clear information should be provided to patients to help them manage their symptoms.
Medication
The evidence for medical therapy in reducing permanent weakness in Bell's palsy is mixed, and guidelines vary. If the diagnosis of Bell's palsy has been made within 72 hours of symptom onset, prednisolone should be prescribed if not contraindicated (NICE, 2019). Mettias et al., (2019) extends this window to 5 days, with advice to discuss the likelihood of benefits with patients who present at 5–10 days. An example regime of prednisolone is 60 mg for 5 days, reduced by 10 mg per day, for a total course of 10 days. Consider adjunct antacid therapy if appropriate (Mettias et al., 2019; NICE, 2019).
Antiviral therapy without corticosteroids is not recommended. The addition of antiviral therapy to corticosteroid treatment remains an area of debate, although a number of guidelines recommend consideration. A 2019 Cochrane review found that combined corticosteroid and antiviral therapy was probably beneficial in reducing late sequelae (e.g. crocodile tears, motor synkinesis). Evidence of a beneficial effect on incomplete recovery is limited (Gagyor, 2019). Mettias et al., (2019) recommends combined corticosteroid and antiviral therapy in palsies of grade V and above. An example antiviral regime, to be given in addition to a corticosteroid, includes treatment for 7 days with valaciclovir 1000 mg three-times per day (Jeffrey and Khatkhate, 2007). NICE (2019) advises discussion with a specialist if this is being considered.
The scope of this article is limited to treatment of Bell’s palsy (where clinical assessment identifies no cause of facial palsy). Clinical evidence of a viral process (e.g. vesicular rash) in the presence of facial weakness excludes a diagnosis of Bell’s palsy, but should instead prompt investigation and management for the appropriate suspected condition. For instance, early aciclovir and prednisolone have been shown to improve outcomes in Ramsay Hunt syndrome (Primary Care Dermatology Society, 2021).
Eye protection
Facial nerve weakness can impact on the action of orbicularis oculi, impacting eye closure, thus leaving the cornea exposed. Prophylactic eye care can prevent potential sight-threatening infection. All patients should use eye lubricants in the form of drops administered frequently during the day (e.g. Viscotears, Celluvisc) and a thicker ointment for nocturnal use (e.g. Lacrilube) (Mettias et al., 2019). General protective measures include taping at night.
Other treatments
There is minimal guidance around the role of physical therapy in improving weakness or reducing long-term sequelae. The term ‘physical therapy’ in the context of Bell's palsy is used to describe several treatments including massage, neuromuscular exercises, electrical stimulation, thermal treatment and, in some trials, acupuncture, making trial data interpretation difficult. Trial designs have been deemed insufficient to form recommendations on whether it improves the condition. There is low quality evidence that facial exercises may be beneficial and that engagement with therapy may benefit patients psychologically (Baugh, 2013; Mettias et al., 2019; NICE, 2019).
A meta-analysis of 11 randomised control trials (RCTs) (1258 patients) concluded that more work is required to prove adequate safety and effectiveness of acupuncture, as current evidence comes from a dataset with high heterogeneity and low-quality study design (Zhang, 2019).
Referral
Patients with other neurological signs or symptoms, UMN weakness or bilateral palsies should be referred to stroke or neurology. Suspected acute stroke is an emergency. ENT referral is warranted in the case of observed palpable parotid mass, visible vesicles, otorrhoea or other evidence of otitis media/externa. Refer to an ENT outpatient clinic if the Bell's palsy is recurrent or shows no signs of recovery within a month. Ophthalmology referral is warranted urgently if ocular complications are suspected. Box 2 summarises referral timings and specialties.
Advice
Bell's palsy can be alarming for patients – in one study, half thought they were having a stroke and a quarter believed symptoms represented a brain tumour (Peitersen, 2002). Reassurance and clear advice are essential once a diagnosis has been made.
Advice on ocular and oral care
Advise the patient on proper use of eye lubricants, and to seek urgent review in the event of visual deterioration, eye pain or irritation. Atraumatic (microporous, or silicone) tape should be used at night to keep the eye closed, and it is important that the patient is shown how to do this (Fig. 5). Dusty, windy or irritant environments should be avoided (NICE, 2019).
Atraumatic tape should be applied horizontally (not vertically) covering the upper and lower lid, to prevent the eye opening (shown here on the left eye), after instilling drops.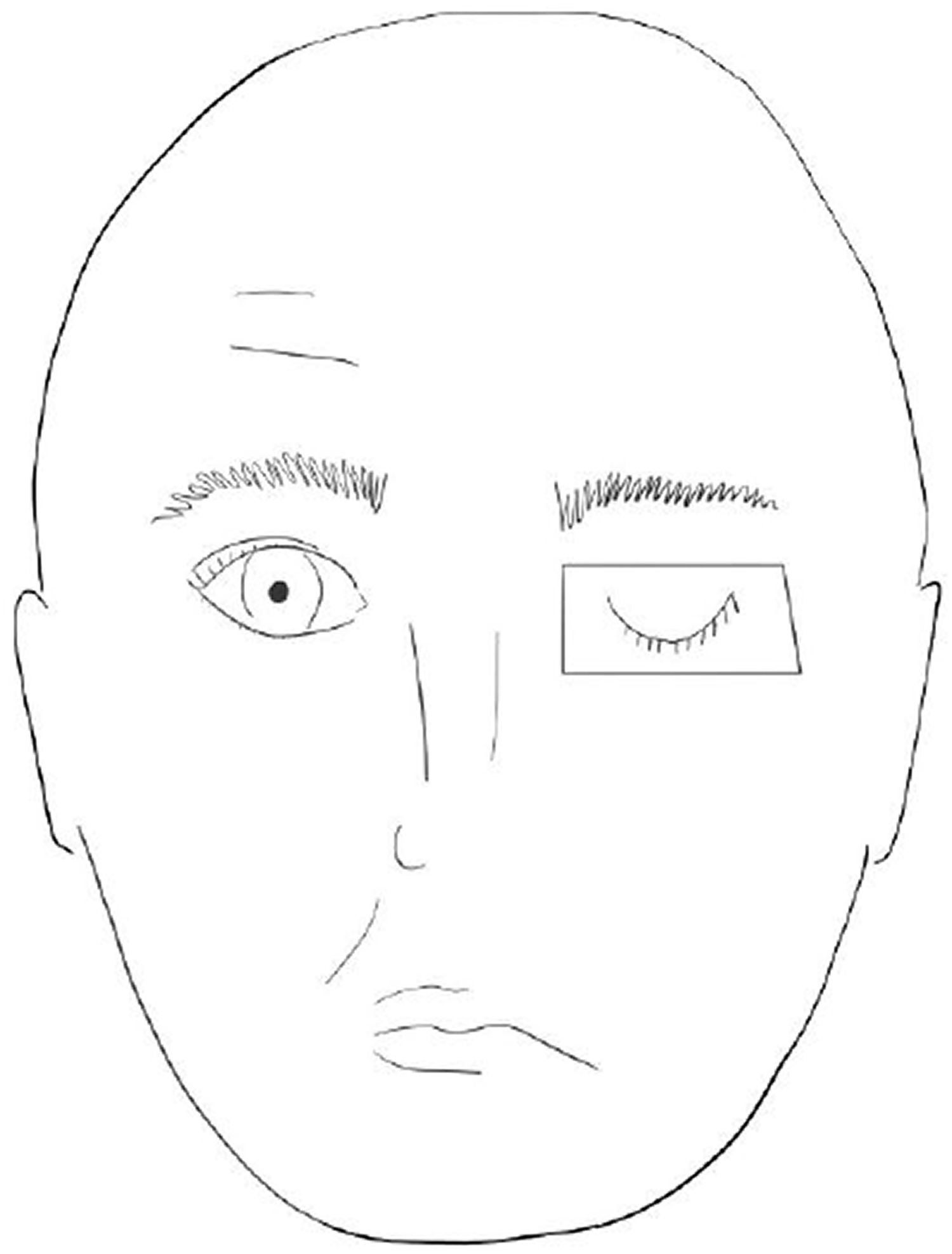
Mouth closure can be affected, which can make talking and eating difficult, and may be embarrassing for patients. The buccal mucosa may also be at risk of trauma from the teeth when chewing. If eating or drinking is affected, a softer diet and use of straws may be helpful (Eviston et al., 2015; NICE, 2019).
Resources
Patient resources.

Prognosis
Poor prognostic indicators.
The literature definition of ‘early’ recovery, in this instance, ranges from 2 weeks to 3–4 months. Those who show some improvement within weeks have an improved chance of full recovery (likely within months). Those who show signs of improvement after 3–4 months are thought to be those who undergo nerve regrowth and reinnervation. This group is less likely to experience a return to entirely normal function: findings at 6 months are a good indicator of long-term prognosis. In around 7% of sufferers, palsy is a recurrent event, usually with years between episodes (Holland and Weiner, 2004; Eviston et al., 2015; NICE, 2019; Peitersen, 2002).
Complications
Complications of Bell's palsy.
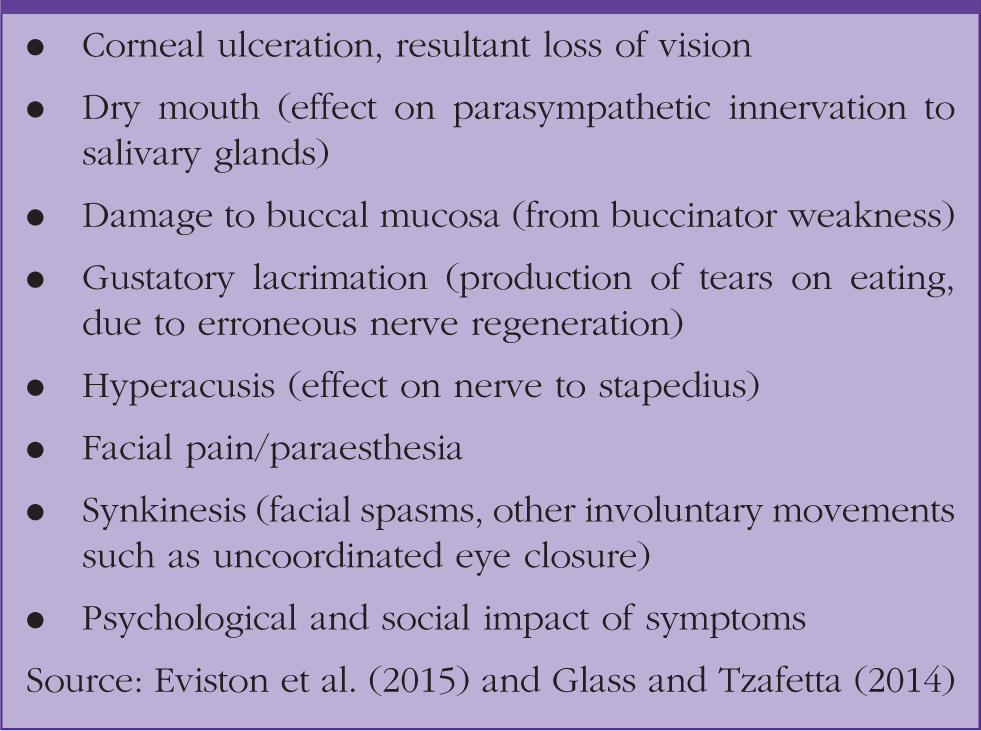
Review patients within a month and refer those without improvement at 3–4 weeks (Mettias et al., 2019; NICE, 2019). For patients with longstanding symptoms, a number of treatment options exist, under the care of a multidisciplinary team. Examples include botulinum injections, which can restore a more symmetrical appearance or reduce synkinesis, and surgical options for facial reanimation, which can offer functional and aesthetic improvements. Nerve conduction studies may be undertaken to assess suitability for surgery. Facial rehabilitation may help in managing symptoms such as synkinesis and in achieving more symmetrical expressions. Speech and language therapy can benefit those with ongoing difficulty in phonation or mastication. NHS provision of treatments such as botulinum toxin injection can demonstrate regional variation (Facial Palsy UK, 2019; Wessex Facial Nerve Centre, 2019).
Bell's palsy in special groups
Children
Bell's palsy is a less common cause of facial weakness in children than in adults, so careful consideration of other causes is required before making the diagnosis. A full physical and neurological examination should be undertaken, including blood pressure to exclude hypertension. Ear infections are common in children and must be excluded. Red flags must also be considered including those for malignancy, infection or undeclared trauma. Lyme disease may underlie half of paediatric cases of facial weakness in endemic areas, including in the UK (Holland and Weiner, 2004; Wessex Neurosciences Clinical Network, 2020).
Regional guidance varies in the UK, but assessment of facial palsy is generally assumed to be undertaken in the acute paediatric setting, rather than in general practice. Some regions stipulate full blood count, blood film, Lyme serology and/or ENT review as part of paediatric facial palsy assessment, as well specific pharmacological approaches in cases of Bell’s palsy (El-Hawrani et al,, 2005; Norfolk and Norwich University Hospitals, 2020; Wessex Neurosciences Clinical Network, 2020). Always consult guidance local to your practice. NICE does not offer guidance on the treatment of Bell's palsy in children under 16 years in age, and there is no clear agreement from the limited evidence base on pharmacological treatment in children (Karatoprak and Yilmaz, 2019; Yoo et al., 2018). North American guidance states that early oral steroids may be considered in children with Bell's palsy (Baugh et al., 2013). Prognosis is better than in adults even without steroids. Other advice, such as eye care, remains important, and should be ensured wherever the child goes, for example at school, and at night-time.
Pregnant women
Pregnant women are more likely to suffer from Bell's palsy than the general population and may have a worse prognosis in complete paralysis. It can be associated with other conditions such as hypertension, diabetes and preeclampsia, so these should be considered and monitored for. Corticosteroids are used in the treatment of other conditions in pregnancy and should be considered. An individualised approach is recommended, so discussion of risk/benefit ratio with the patient is paramount. Specific cases may warrant specialist discussion (Baugh et al., 2013; Hussain et al., 2017).
KEY POINTS
Bell’s palsy is an idiopathic unilateral LMN paresis/paralysis of cranial nerve VII and is always a diagnosis of exclusion Maintain a high index of suspicion for alternative serious aetiology such as acute stroke, systemic or neurological conditions, intracranial malignancy, head and neck cancer, trauma and infection Prompt diagnosis and treatment of Bell’s palsy with corticosteroid therapy improves the chance of full recovery In adults, antivirals with corticosteroids may be considered in severe palsies, but antivirals should never be prescribed without steroids Advise lubricant drops and horizontal lid taping to prevent serious complications such as corneal ulcers and subsequent visual loss Failure to improve within 3–4 weeks, despite appropriate treatment, should prompt urgent referral to ENT
ORCID iD
Miss Frith Cull https://orcid.org/0000-0002-4683-1227