
Abstract
Many thousands of patients present each year to general practice with breast symptoms. Patients are often concerned that their symptoms might indicate cancer; however, the majority represent benign breast disease. On average, a full-time GP will diagnose one or two cases of breast cancer a year. It can be difficult to distinguish between potentially malignant and benign conditions in the GP setting, as well as manage patient anxiety and expectations. This article aims to cover pathology, diagnosis and management of benign breast disease and improve confidence in managing patients diagnosed with benign disease. The article will not cover the topics of breast cancer or breast pathology in pregnancy and male patients.
Clinical case scenario
Saba, a 33 year old mother of two, presents to her GP because she has found a lump in her left breast just the day before. She is very anxious as a close friend has breast cancer. She is otherwise fit and well and takes no medications. There is no family history of breast disease. She recently stopped breastfeeding and has returned to work as an accountant. Your examination reveals a 1 cm mobile mass with smooth edges in her left breast. She has no lymphadenopathy or any skin or nipple changes. You explain that, while the examination findings are reassuring, you would like to refer her to secondary care using the suspected cancer pathway for an appointment within 2 weeks.
Breast development
Initial breast development is called thelarche, which typically occurs between ages 8.5 and 13 years old and lasts 4–4.5 years (Javed and Lteif, 2013). Oestrogen is vital for pubertal breast development and stimulates both duct growth and fat deposition. Growth hormone, cortisol and insulin are also responsible for ductal development. Progesterone does not appear to be involved in early pubertal breast growth or development, but is reported to mediate the lobular alveolar development in pregnancy, facilitating lactation (Borenstein and Friedman, 2020). Asymmetrical breast growth during thelarche is very common and usually evens out by full maturation. Breast buds are normal lumps felt under the nipple in 8–12 year old girls, often indicating the start of puberty. Patients and their parents can be reassured that this is a normal stage of development.
The female breast consists of fatty tissue, connective tissue and glands. The mammary glands are made up of a series of ducts and around 15–20 secretory lobules where milk is produced for lactation. Each lobule has many alveoli which are drained by lactiferous ducts that converge at the nipple. Surrounding the mammary glands is connective stromal tissue, which condenses to form suspensory ligaments of Cooper that support the breast tissue. The rest of the breast consists of fatty tissue. Each breast has a ‘tail’ of tissue extending up into the axilla.
The male breast structure is almost identical to the female breast. Male breast tissue lacks the secretory lobules, since there is no physiological need for milk production.
The lymphatic drainage of the breast is clinically important in relation to breast cancer and infection. Breast tissue drains into three groups of lymph nodes: the axillary nodes (75%), parasternal nodes (20%) and posterior intercostal nodes (5%). The skin drains to the axillary, inferior deep cervical and infraclavicular nodes, and the nipple and areola drain into the subareolar lymphatic plexus.
Assessment in primary care
Assessment in primary care should assess risk and consider diagnosis and management, including referral to secondary care when appropriate. This section outlines aspects of the history and examination.
Ask the patient about their symptoms, including lumps, pain, nipple discharge, and skin changes. Breast pain is not a common feature of breast cancer, and is often related to menstruation or hormonal therapy. Nipple discharge is also an uncommon symptom, found in only 5% of breast cancer cases. Discharge is more frequently secondary to papillomas or duct ectasia with a spontaneous and/or bloody discharge. Family history of cancer and age of diagnosis is important, as it may lower the threshold for referral to secondary care and warrant genetic testing. A family history of breast cancer in relatives less than 50 years old and affecting more than one first-degree relative is significant. If a patient has a personal history of benign disease, for example a cyst, it should not be assumed that the current presentation is simply a recurrence. Ask about prescribed and over-the-counter medications, including hormonal therapies, and smoking history (smoking is a risk factor for developing periductal mastitis). Enquire about symptoms of weight loss and bone pain if considering malignancy.
It is important to discuss patients’ ideas, concerns and expectations. Patients will often feel anxious and receive negative stories from friends, family or online. This is a chance to educate patients, encourage them to continue checking their breasts, challenge their health beliefs and provide support.
Examination should be performed on both breasts for comparison. Patients may feel uncomfortable, so consider the examination environment and provide a chaperone.
First, inspect the breasts, specifically looking for symmetry, nipple inversion, skin dimpling or changes, previous scars and any visible masses. The patient should sit on the side of the couch and the clinician should inspect the breast while the patient is relaxed with hands on their thighs, hands pushed into the hips and then with hands behind their head and leaning forwards. Always check under the breasts. For palpation, the patient is best examined lying on the couch at 45° with one arm behind their head. Palpate with the flats of the fingers. Often patients can point to where they feel the lump. There are various breast examination techniques, and all are appropriate if performed correctly:
Spiral method: Starting at the nipple working outwards in a concentric spiral motion Clock face method: Viewing the breast as a clock face and examining each ‘hour’ from outer breast edge to the nipple Quadrant method: Divide the breast into quarters and examine each area
In addition to these methods it is important to remember to examine the axillary tail of the breast.
If a mass is felt, then ascertain whether it is smooth or irregular, tethered or mobile, painful or painless, the size and shape, if firm or fluctuant and any overlying skin changes. If the patient presents with nipple discharge they may compress the areolar tissue and the clinician can inspect or even collect a sample. It may be helpful to know that microscopic blood in nipple discharge can be checked using a urine dipstick.
An examination of the lymph nodes should be performed, even if you suspect benign disease. Examination of axillary lymph nodes is best performed with elevation of the patient’s arm at 90° and their flexed forearm resting on the examiner’s forearm, to create the axillary fold where the lymph nodes would be present if enlarged. The supraclavicular nodes should be examined. If enlarged, feel for cervical and infraclavicular nodes.
Clinical guidelines
The National Institute for Health and Care Excellence (NICE) (2021a) outlines guidance on secondary care referral:
Refer people using a suspected cancer pathway referral (for an appointment within 2 weeks) for breast cancer if they are
Aged 30 and over and have an unexplained breast lump with or without pain Aged 50 and over with any of the following symptoms in one nipple
^ Discharge or ^ Retraction or ^ Other changes of concern
Consider a suspected cancer pathway referral (for an appointment within 2 weeks) for breast cancer in people
With skin changes that suggest breast cancer Aged 30 and over with an unexplained lump in the axilla
Consider non-urgent referral in people aged less than 30 years with an unexplained breast lump with or without pain.
Breast clinics aim to see all referrals within 2 weeks, whatever the urgency pathway selected. Triple assessment, consisting of clinical examination, imaging (mammography or ultrasonography) and needle biopsy (if appropriate) is performed.
It can be challenging for GPs to provide adequate reassurance. It is often not possible to make an accurate diagnosis from history and examination alone. Familiarity with the referral criteria and explaining the low threshold for referrals can relieve anxiety for both the clinician and patient. Explanations of what to expect at assessment in secondary care can further relieve anxiety. Many patients will be diagnosed with a benign condition.
Breast lumps
Most breast lumps are benign and do not require treatment. Many benign breast presentations can be categorised as abnormalities of normal involution and development and occur during the three phases of breast growth: development (under 25 years old), cyclical changes (25–45 years old) and involution (over 35 years old). As per NICE guidance, new or persisting discrete breast lumps require further investigation either via the suspected cancer pathway or as a non-urgent referral, and almost all will require biopsy.
Fibroadenoma
A fibroadenoma is a painless, unilateral, benign growth of the stromal breast tissue. They are common. It is estimated that 10% of the world's female population will have a fibroadenoma in their lifetime (Ajmal et al., 2021). The cause of fibroadenomas is thought to be hormonal. This theory is supported by the higher prevalence in younger people, those taking oral contraceptives or hormonal therapies and the observation that fibroadenomas grow in pregnancy and shrink in the menopause.
Masses are firm and rubbery. They vary in size, are painless and most commonly occur in the upper outer quadrant of the breast. They can grow, sometimes to large sizes quite quickly, which is alarming for patients.
Mammography may demonstrate a discrete dense mass. Involuting fibroadenomas, typically in post-menopausal women, may contain macrocalcifications often producing a classic ‘popcorn calcification’ image. Ultrasound may reveal a solid mass with regular borders.
NICE (2021a) recommends that patients under 30 years old with an unexplained breast lump are referred non-urgently to breast services. Patients can be reassured that a firm, mobile, regular-bordered mass is unlikely to be malignant and fibroadenomas often shrink over time with no long-term cancer risk. If the mass is larger than 4 cm it should be considered for removal, due to compression of surrounding breast tissue which can cause pain and patients may be concerned about cosmetic appearance of a large mass.
Clinical case scenario (continued)
Four weeks later, Saba returns to see you having been seen in the breast clinic. She was relieved to find out she has a fibroadenoma. She says the assessment was more invasive than she thought and she did not realise she would have a biopsy that day. When she received the phone call with the histology results, she was anxious and forgot what the specialist said about how to manage her breast lump. She has attended today to ask if she can have it removed and if she is likely to get more of them.
You read the letter from the breast clinic which states examination findings were reassuring, ultrasound revealed a solid mass with smooth borders, and biopsy confirmed a fibroadenoma. You reflect on how consultations have changed since the Covid-19 pandemic; more patients are receiving results over the phone, with an impact on how much information is retained by patients and their ability to ask questions. You consider the possibility that the lump had been present for some time and that changes in the breast tissue during breastfeeding could have made it more difficult to feel.
You explain that, as her lump is small, not causing her any discomfort and likely to shrink over time, surgical removal is unnecessary. You encourage her to remain breast aware and return if there are any changes in lump size or any new lumps.
Lastly, as Saba was surprised to have a biopsy during her breast clinic visit, you reflect on how to explain the ‘Triple Assessment’ better for patients in the future.
Fat necrosis
Fat necrosis is an inflammatory process within the adipose tissue which can be secondary to trauma, radiotherapy, biopsy, lumpectomy or a breast infection (Genova and Garza, 2021). Larger breasts with more adipose tissue are at greater risk. Following injury to the breast tissue, haemorrhage leads to induration and scarring; patients may present with a lump, skin erythema, nipple inversion and occasionally lymphadenopathy. These clinical signs will lead to referral to secondary care services as they provide cause for concern. Simple analgesia and wearing supportive bras can help manage the pain. Surgery is not usually required unless it causes significant pain or distortion to the breast.
Phyllodes tumour
Phyllodes tumours are rare stromal tumours. They account for less than 1% of breast tumours (Tan et al., 2016). They most commonly follow a benign course, but some are malignant and can metastasise. A benign phyllodes tumour presents clinically and radiologically like a fibroadenoma and can present at any age. They usually present as a rapidly growing breast lump; in some patients a lesion may have been apparent for years but only recently has grown in size. These tumours can occur in any breast quadrant, and up to 20% of patients have axillary lymphadenopathy. The aetiology is unclear.
As these tumours present with an unexplained lump, sometimes with lymphadenopathy, patients should be referred urgently to secondary care. Management of benign phyllodes tumours requires excision.
Benign fibrocystic change
There are many synonyms for benign fibrocystic change, such as fibroadenosis or nodularity. It is the most common type of benign breast presentation in young women, with 70% of women developing these changes during their lives. Peak incidence is between 35 and 50 years old, and it is rare in under 25 year olds. The term covers a spectrum of histological changes characterised by overgrowth of fibrous stroma and ducts and lobules, in varying proportions. These changes should be considered as a divergence from normal breast development and involutions, not a disease process. The aetiology is thought to involve overproduction of oestrogen and suppression of progesterone; this theory supported by typical improvement after the menopause (unless the patient takes hormone therapy).
Patients present with a variety of symptoms. It may manifest as changes in breast size, lumpiness of tissue or breast pain. Symptoms are frequently bilateral and related to the menstrual cycle, with a worsening of symptoms pre-menstrually and resolution at onset of menses. Young ‘lumpy’ breasts, rather than discrete breast lumps, may be appropriate for a ‘watch and wait’ approach before considering a referral.
It is important to manage patient expectations and reassure that symptoms are part of normal breast development. However, due to the increased density of the breast tissue it is more difficult to feel new lumps. Therefore, patients should be encouraged to regularly check their breasts and get used to what their ‘normal’ feels like.
It can be frustrating for patients with benign fibrocystic changes as their symptoms can be recurrent and painful. Patients can be advised to wear well-fitting supportive bras, apply heat compresses and use pain relief (such as topical or oral ibuprofen and oral paracetamol). Some women have reported that reducing caffeine and fat intake improves symptoms, but there is no scientific evidence for this observation.
If patients present with large cysts or lumps that persist beyond menstruation they should be referred (NICE, 2021a). Large simple cysts can be aspirated in secondary care and treatment considered complete. Rapidly reforming and complex cysts on imaging are suggestive of malignancy and will be followed up by breast services (Kowalski and Okoye, 2021).
Hamartoma
Hamartomas account for almost 5% of benign breast tumours. Histologically they consist of disorganised ducts, lobules, stroma and adipose tissue, which can be difficult to differentiate from a fibroadenoma. They are most common in patients between 30 and 50 years old and present as a painless, well-circumscribed mobile mass (Kuerer, 2010). Up to 60% are not palpable and are found incidentally on imaging (Ruiz Tovar et al., 2006). Mammography shows a defined dense mass encapsulated within the fatty breast tissue. Lobulated densities may be dispersed with the capsule creating the ‘slice of salami’ image. Ultrasound usually reveals a well-circumscribed solid dense mass that is compressible. If no cell atypia is seen histologically they can be managed conservatively with observation alone.
Nipple discharge
Nipple discharge is common, especially in the reproductive years. Patients may present if it impacts on daily life or with concern about a potentially serious cause. Most often the cause is benign, often physiological. Physiological discharge can be various colours, originating from multiple ducts, and occurs when provoked; it will not leak spontaneously and one should not attempt to express it. The other mammary causes of nipple discharge will be discussed in this section. It is also important to consider extra-mammary causes of nipple discharge, including taking a medication history and checking serum prolactin.
Intraductal papilloma
Intraductal papillomas are warty, benign lesions located in the ducts behind the areola. This condition is most commonly seen in 30– 50 year olds, and 50% are single lesions (Kuerer, 2010; Li and Kirk, 2021). When the lesions are located near the nipple they typically present with spontaneous bloody or clear nipple discharge. Due to proximity to the nipple, pressure around the areola will elicit discharge in most cases, but do not squeeze the nipple bud itself. Rarely, they are palpable or detected incidentally on imaging. Although most are benign, it is considered a high-risk precursor lesion for cancer, but they make up less than 1% of malignant breast tumours (Karadeniz et al., 2016). Any patient with unilateral nipple discharge requires an urgent suspected cancer pathway referral (NICE 2021a). Due to the risk of malignancy, it is advised they are excised.
Mammary duct ectasia and periductal mastitis
Mammary duct ectasia (MDE) and periductal mastitis (PDM) are often terms used interchangeably, however, it is still debated whether they are separate entities or a single disease on a spectrum.
Histopathologically, MDE is characterised by focal dilation of lactiferous ducts, due to reduced elastin and inflammatory infiltrates. In severe cases, fibrosis and granulation tissue might fill and obstruct the ducts, causing further inflammation. The exact aetiology is still unclear; some researchers consider it part of age-related involutional change, but the factors that initiate the disease process are still unknown (Jiang et al., 2020). It is mainly seen in peri-menopausal women, but has been seen in younger patients, including men. MDE is frequently asymptomatic, but often presents with unilateral nipple discharge, which is usually white or green and thick in consistency. Occasionally, a small mass in the subareolar or peri-areolar region can be felt, sometimes associated with some discomfort or redness, caused by the dilated and sometimes blocked ducts. Mammographic findings in MDE include micro-calcifications, retro-areolar duct dilation and masses, which can appear worrisome and prompt a biopsy. Ultrasound can reveal duct dilation. In mild symptomatic cases, after excluding other causes, MDE can be treated conservatively and often resolves within 2 weeks. Surgical intervention is required if the symptoms do not improve.
PDM on histology shows cell metaplasia, which extends deep into the duct system. This results in severe periductal reactive inflammation leading to collagen formation and interstitial fibrosis. Again, the aetiology is not clearly understood, but smokers are three times more likely to experience PDM (Rahal et al., 2005). PDM primarily affects young female patients, but cases have been described in men. Patients present with nipple discharge, which can be bloody, breast masses behind the areolar, with or without pain, and peri-areolar abscesses. Repeated infections increase the fibrotic changes behind the nipple-areola complex and can lead to distortion or retraction (Guray and Sahin, 2006). When presenting with a flare, patients may also have lymphadenopathy. Those with features of malignancy require biopsy and often have lesions removed surgically as diagnosis and removal can be achieved at the same time. Patients with recurrent symptoms may be offered surgical intervention. Patients with mild symptoms can be treated with antibiotics covering for the most common causative organism, Staphylococcus aureus, and gram-negative organisms. The most important management intervention for PDM is smoking cessation; even with surgical removal of lesions PDM can recur if patients continue smoking.
Breast pain
Breast pain, mastalgia, is common, affecting approximately two thirds of women during their reproductive lives (Tahir and Shamsudeen, 2021). Mastalgia alone is not a criterion for urgent referral, with a positive predictive value of less than 3% for breast cancer (NICE, 2015). However, due to the number of patients that experience mastalgia, and the anxiety surrounding breast symptoms, it is important to understand the causes and management.
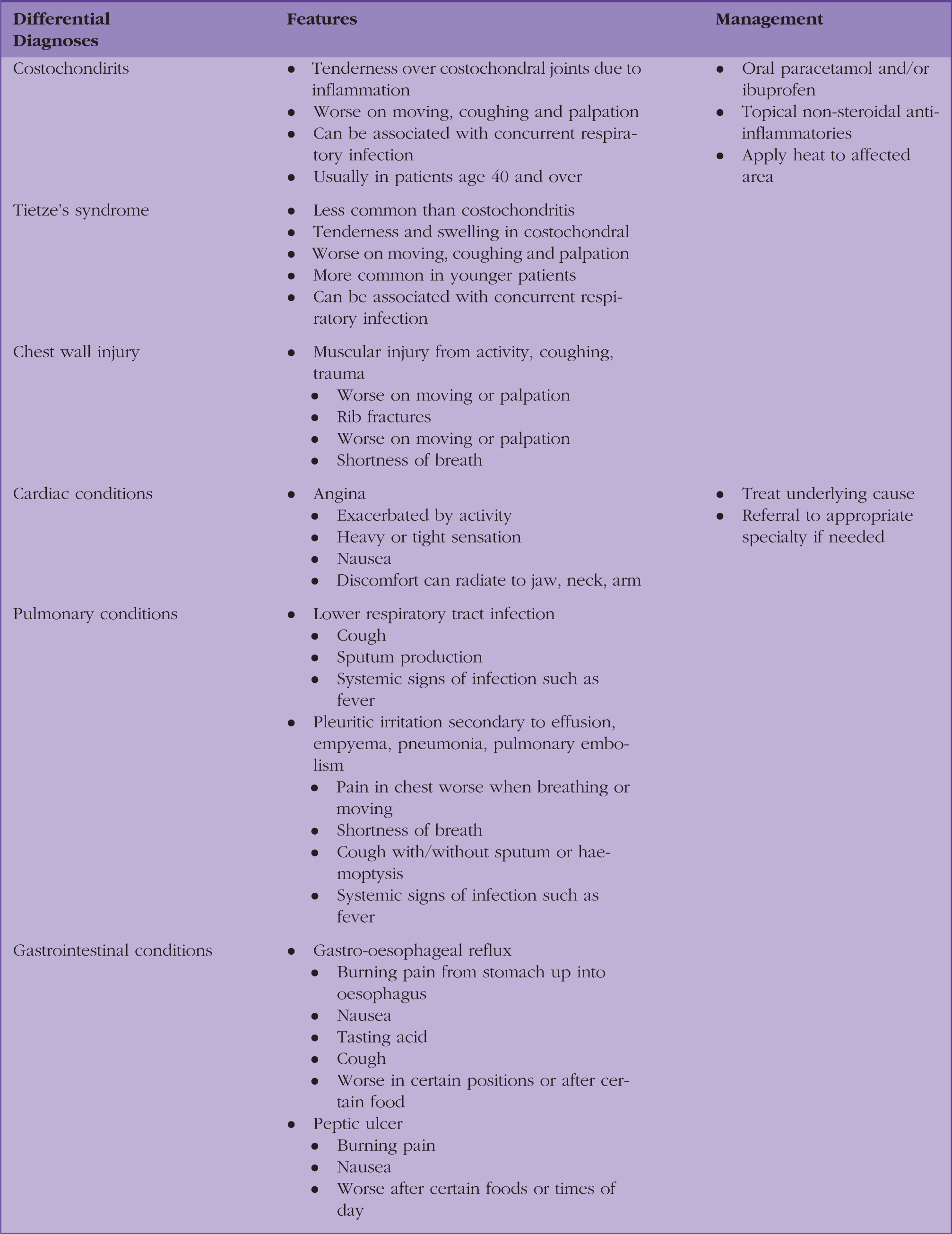
Causes of breast pain can be classified as extra-mammary and mammary. Mammary causes, outlined below, are further divided into cyclical and non-cyclical relating to menstruation. Table 1 outlines the extra-mammary causes, key features and management.
Extra mammary causes of breast pain.
Cyclical mastalgia
The breasts are active organs and change throughout the menstrual cycle. They begin to enlarge under the influence of oestrogen and, later in the cycle, progesterone and prolactin. Patients experience bilateral tenderness, most severe in the outer quadrants, and nodularity in the premenstrual phase, which resolves with the start of menstruation. The aetiology of cyclical mastalgia is poorly understood and thought to be most likely secondary to hormonal changes, again because it is most common in the reproductive years and fluctuates with the menstrual cycle. Nevertheless, studies have demonstrated that women with cyclical mastalgia have similar hormone levels to those who do not experience it. It has been suggested that, rather than differing levels of hormones, it is an increased sensitivity to hormones that may explain cyclical breast pain.
Patients can be reassured that this is a common and benign presentation. Patients are often relieved that they are not suffering alone and there are ways of managing the symptoms if needed; for some women reassurance is enough.
NICE advises oral paracetamol and/or ibuprofen or topical non-steroidal anti-inflammatories as first-line management (NICE, 2020). Lifestyle changes such as regular exercise and wearing well-fitting supportive bras can help. Studies surrounding the effectiveness of avoiding caffeine remain conversional, but it is often recommended due to other health benefits. Vitamin E supplements are anecdotally effective, but have not been proven in high-level research. A long course (more than 4 months) of Evening Primrose Oil (EPO) has been demonstrated to reduce cyclical mastalgia in up to 70% of patients, in placebo-controlled trials (Millet and Dirbas, 2002; Pruthi et al., 2010). The recommendation is to take around 300 mg of Gamma Linolenic Acid content (an omega 6 fatty acid) within the EPO for 2–3 months. It is important to explain what EPO is, that it takes a few months to take effect, and unfortunately might not help all patients.
If first-line treatments do not improve symptoms and patients are experiencing severe pain, then referral or discussion with secondary care should be considered for specialist treatments.
Non-cyclical mastalgia
Symptoms do not follow the menstrual pattern and are more likely to be unilateral and vary in location. Again, patients can be reassured that there are many benign causes.
Breast cysts are common and can present as mastalgia. They are part of the benign process of fibrocystic change. If a discrete mass is felt, the patient will be referred for Triple Assessment in secondary care. Small cysts may come and go and patients might be happy to watch and wait to see if their symptoms improve. Larger cysts are often more painful and may benefit from needle aspiration. Recurrent cysts should be further investigated in secondary care, as should complex cysts.
For women who are breastfeeding, breast pain is one of the most common reasons to present to medical professionals, with nipple and/or breast pain being the second most common reason for mothers to stop breastfeeding (Berens, 2015). There are a variety of causes including engorgement, infectious and non-infectious mastitis, nipple damage and galactoceles. The scope of this article does not provide an in-depth review of breast presentations related to pregnancy and breastfeeding, but patient resources are included in the further information section below.
Infections in the breast can cause pain associated with inflammation. Infectious processes most commonly occur in lactating women, but can occur in those who are not lactating.
Mastitis and breast abscesses usually present unilaterally and can be associated with systemic signs of infection. The most common causal organisms are S.aureus, enterococci and anaerobes (NICE, 2021b). Examination of the breast often reveals a wedge-shaped area of redness which is hot, firm and tender. Abscesses may be felt as a fluctuant lump with overlying skin inflammation. Mastitis without signs of sepsis is managed with simple analgesia, heat application, advice to continue breastfeeding or expressing (including from the affected breast, if possible), and antibiotics. Antibiotics are indicated in lactating patients if there is no improvement after 12–24 hours of conservative measures, and antibiotics are required in all cases of non-lactating mastitis (NICE 2021b). Breast abscesses require urgent diagnostic confirmation with ultrasound and drainage via needle aspiration or incision. The abscess fluid should be sent for culture to guide antibiotic choice. A persistent mass should be referred on the suspected cancer pathway to be seen within 2 weeks.
Cellulitis of the breast is more common in overweight patients, larger breasts, and patients who have had previous surgery or radiation. It presents as a unilateral, tender, hot area of skin with no associated mass. It should be managed with antibiotics. Patients with recurrent breast cellulitis should be referred to secondary care.
Lastly, trauma to the breast or areolar tissue can cause pain. Trauma can be secondary to surgery, radiation, injury or piercings. Symptoms are localised and can be treated with analgesia and wound care if appropriate.
Extra-mammary mastalgia
It is important to consider that, while patients may present with pain in their breasts, the pathology may not be in their breast tissue. It can be caused by musculoskeletal pain, cardiac pathology such as ischemic heart disease, lung disease, or be a part of a pain syndrome. Examples of extra-mammary causes and key features are outlined in Table 1. The appropriate management of extra-mammary mastalgia lies in the exclusion of mammary causes, correct diagnosis, and treatment of the underlying cause, which may involve referral to another specialty.
Key points
Benign breast disease is common; affected patients frequently present to general practice and often need to be referred for accurate diagnosis A full-time GP will diagnose, on average, one or two cases of breast cancer a year; it can be difficult to distinguish between malignant and benign conditions in general practice Patients often experience significant anxiety and GPs need strategies for management and, where appropriate, reassurance Thorough history and examination are important and should be informed by knowledge of breast disease and red flags for cancer GPs should refer suspected cancer using the 2-week wait pathway and help patients understand what to expect from Triple Assessment GPs should promote self-examination and breast screening, as well as providing relevant resources to patients