
Abstract
Teaching and training are integral to the different, core roles of a trainee. Therefore, there is a shift in the medical profession towards credentialing teaching and training skills. Postgraduate qualifications in medical education are likely to be more important for professional development. In recent years, the number of medical education awards and training programmes has increased rapidly. This pluralism, however, may become a source of confusion for those considering enrolment on such programmes. This article summarises the nomenclature, awarding bodies, levels of qualification, programmes and positions available for those wishing to advance their educational practice. The article will focus on opportunities available to UK-based doctors and particularly for doctors in training.
Case scenario
Fernando is commencing his GPST2 year. He enjoys supervision and teaching. He hopes to work within his local deanery as a medical student and trainee supervisor when he becomes a GP partner. He currently has no formal qualifications in medical education. He decides to undertake a Certificate in Medical Education to add to his portfolio.
He makes enquires at the local university where he graduated 4 years ago. The Postgraduate Certificate in Medical Education involves distance learning and costs around £5000. His study budget for the year is £600. To pay the balance would use all his savings. Short staffing due to the COVID-19 pandemic means that he will only be able to take a few days of study leave. He is currently volunteering as a problem-based learning tutor for medical students in the local undergraduate faculty.
What options are available to demonstrate his interest in medical education? How might he get some formal training in supervision?
Background
The last decade has seen rapid expansion of courses in medical education, not only in the UK but also globally. These range from a ‘continued professional development’ day course in teaching through to educational research leading to a PhD. Medical education is now firmly established as a specialty with bespoke societies, journals, professional standards and qualifications (Eitel et al., 2000). Medical education now incorporates a multitude of disciplines including empirical research, student support, international development and much more (Cristancho and Varpio, 2015). In 2016, the General Medical Council (GMC) formalised undergraduate and postgraduate training standards in ‘Promoting Excellence: Standards for Medical Education and Training’, and made the ‘Trainer Recognition Framework’ mandatory for all registered medical trainers (GMC, 2016). This followed a 2009 study showing that of 98% of consultants with one or more such training roles, only 6% had an educational qualification (Schofield et al., 2009). This statistic is changing. Educational training is becoming a feature of consultant interviews and of specialty training selection criteria. Medical educators are now more likely to see themselves as ‘professional experts’ and ‘enthusiasts’, and to belong to a community of practice (Ghataoura and Acharya, 2016; Nikendei et al., 2015; Sethi et al., 2015). Nevertheless, some scepticism persists about this training. Medical postgraduate training already costs an estimated £17 114, this includes an average figure for self-funding of courses of £1875 (Association of Surgeons in Training, 2007; Jaques, 2011; Waters and Wall, 2008).
Entry-level courses include:
Train the trainer/teach the teacher Massive open online courses (MOOC)
The Royal Colleges of Surgeons of Edinburgh (RCSEd), Glasgow (RCPSG), England (RCSEng), Royal College of Obstetricians and Gynaecologists (RCCOG) and the Northern Ireland Medical and Dental Training Agency (NIMDTA) run regional 1 and 2 day ‘Training the Trainer’ courses, with others available by private medical training companies and medical schools throughout the year. Training for Trainers is medical education’s most accessible credential.
The online equivalent of an entry-level course, the MOOC has expanded the reach of universities beyond the classroom (Chen et al., 2019).The University of Glasgow’s Teaching Healthcare Professionals micro-credential achieved through an online platform called Futurelearn, carries 10 credits towards further learning. The same online platform offers four modules in clinical supervision from the University of East Anglia. Futurelearn’s American counterpart Coursera runs health education courses from the University of Michigan. The distance learning arena is likely to grow considerably in the coming decade, facilitated by globalisation and the after effects of the COVID-19 pandemic.
Academy of Medical Educators, Higher Education Academy, and other university opportunities
The Academy of Medical Educators (AoME) sets professional standards, giving members professional recognition and providing best practice standards in a similar way to the respective Royal Colleges, but for educators in medicine, dentistry, veterinary medicine and beyond. Founded in 2006, its 2009 professional standards framework (PSF) describes core values and areas of educational activity expected of a clinician-teacher (AoME, 2014). Membership and fellowship categories exceed the minimum GMC requirements for clinical trainers and its framework has been adopted by both the GMC and course providers internationally. This means that AoME-accredited courses (although not only AoME-accredited courses) meet the GMC Trainer Recognition framework for GMC Registered Medical Trainers, a pre-requisite for senior GP or specialist posts. Membership of the AoME (MAcadMEd) is by submission of a portfolio of recent continuing professional development activities in education, a peer-review of educational practice, a reflective submission and a supervising reference. Educators in all grades of health sciences and disciplines are eligible for membership and fellowship.
Formal training of university staff has been shown to increase student-centeredness, itself a driver of deep learning and other higher cognitive outcomes (Gibbs and Coffey, 2004). The UK’s PSF is a voluntary scheme that stratifies relative competencies for university-level teachers within the UK and increasingly abroad. It outlines the professional values and core knowledge it expects across all areas of practice of a teacher in higher education in all disciplines, not only medicine and has established international currency in higher education expertise (Bell and Brooks, 2016; Newton and Gravenor, 2020). The four levels of the Higher Education Academy (HEA) are: Associate Fellow (AFHEA), Fellow (FHEA), Senior Fellow (SFHEA) and Principal Fellow (PFHEA) (HEA, 2011). Associate Fellow status is broadly equivalent to MAcadMEd. Fellowship level equates broadly to a postgraduate certificate (PGCert) in education and aligns with the expected proficiency of a substantive academic role. Fellowship categories can be obtained by applying directly to the HEA, thus clinicians can credit for yet unaccredited prior expertise and scholarship.
There are multiple entry-level university run courses at the Master’s level that serve as an introduction to medical education and can be completed over 4–10 weeks. These can be later used towards further degrees and are aimed to be flexible with a working schedule. The University of Bristol offers a ‘Teaching and Learning for Healthcare Professionals’ 30-credit online module, whereas Warwick University runs a similar 20-credit module that can be used towards continuing education (Postgraduate Certificate and Diploma Programmes equate to 60 and 120 credits, respectively). Others, such as the University of Cambridge Foundation Programme for Clinical Educators and University of Edinburgh Clinical Educator Programme for staff from local trusts are free and accredited by the HEA and AoME. The Association for Medical Education in Europe has an Essential Skills in Medical Education online course lasts 12 weeks and is accredited by four universities for Accreditation of Prior Learning (APL).
University courses at Postgraduate Certificate, Postgraduate Diploma and Master’s level
For doctors affiliated to a university through the teaching of its undergraduates, and/or pursuing further research degrees, there are many similar options. Most universities run a PGCert in Higher Education/Academic Practice for staff, the equivalent of the PGCert in Medical Education, often conveying Fellowship of the HEA. These can be cost-free, even for faculty members without substantive roles. Similar shorter ‘entry-level’ certificate courses for teaching assistants and demonstrators (Introduction to Academic Practice, First Steps in Teaching, and Introduction to Teaching in Clinical Settings) are usually accredited at AFHEA. Designed to increase levels of accreditation within a mobile workforce, these courses are open to accreditation of Prior Learning. Similarly, universities will often support teachers in achieving HEA Fellowship status or offer their own unique brand of four equivalent awards which mirror the PSF.
The number of Master’s courses in medical education in the UK have increased markedly from one in 1998, eight in 2009, 20 in 2012 to 36 in 2022 (Figure 1) (Cohen et al., 2005; Cusimano and David, 1998; Tekian and Harris, 2012). This rapid increase in courses has raised concerns around quality, as well as the teaching and assessment of qualitative methods that have hitherto not featured in training (Al-Subait and Elzubeir, 2012; Pugsley et al., 2008). The option to leave at PGCert or PGDip level is often taken up. Most part time programmes span 1–4 years, and include flexible options such as taking breaks, completing standalone modules and APL. APL is an attractive option, as programmes overlap in content with already completed courses. With fees exceeding £5000 per PGCert, entry into the programme at a more advanced stage can be very cost-effective. Year 1/PGCerts typically focuses on basic pedagogical theory, with coursework offering feedback on teaching practice and reflective exercises; Year 2/PGDip frequently offers sub-specialist modules in education such as simulation, curriculum design, research techniques, quality improvement and leadership. The final Master’s year requires a research project.
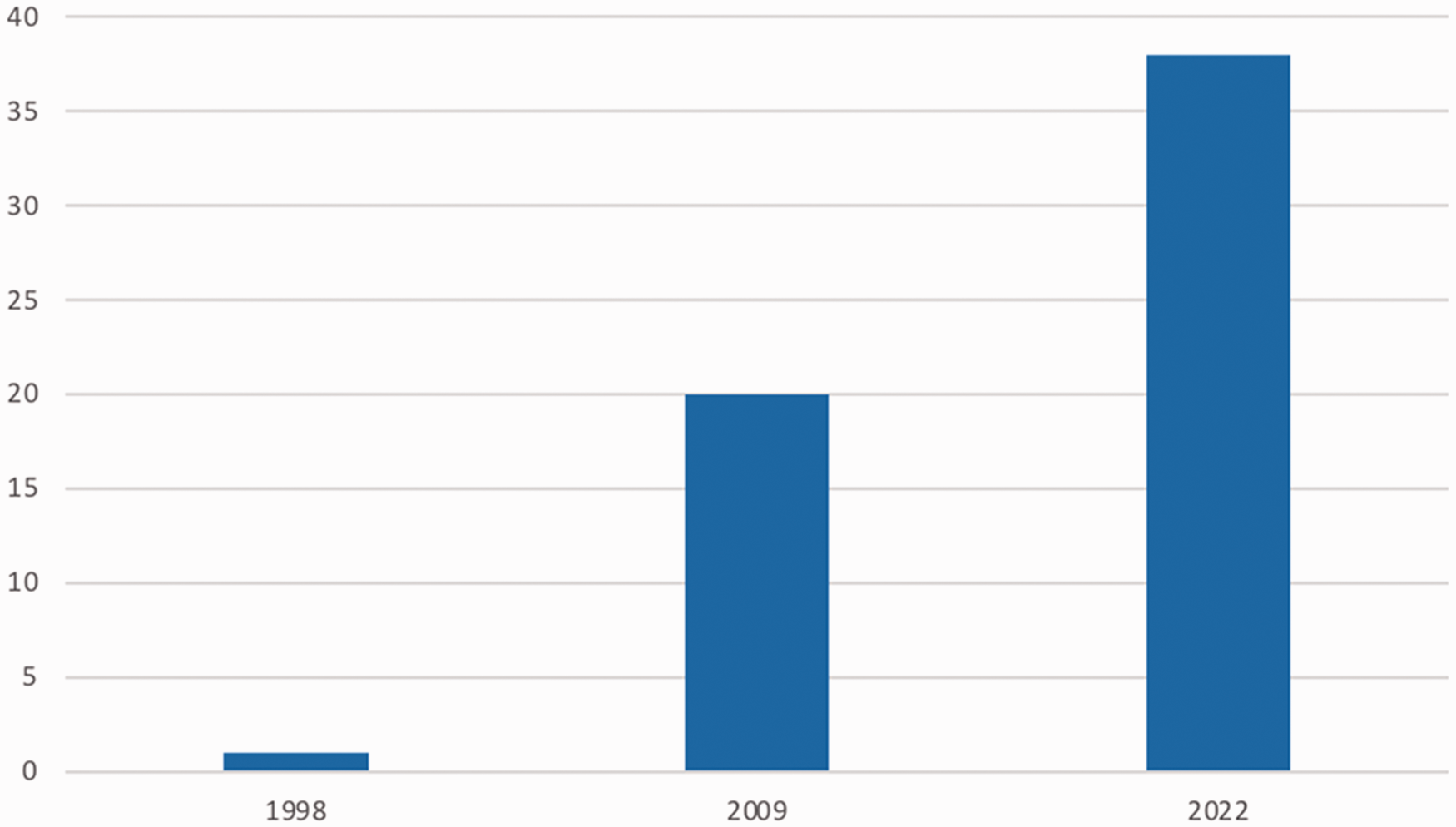
Number of Master’s courses in Medical Education in the UK per year 1998–2012.
Mentoring
Mentoring is a supportive relationship whereby one individual benefits from the experience, perspective, and encouragement of another. It is increasingly promoted by organisations within and outside of medicine to develop healthy trainees, and ultimately, leaders. The Faculty of Medical Leadership and Management, the British Medical Association, and many Royal Colleges run mentorship schemes, supplemented by many grassroots and more informal schemes within deaneries and health trusts. A formal role as a mentor, verified by official documentation from one of these institutions, demonstrates vision for excellence and aims to cultivate the next generation of leaders.
Other options
The Resuscitation Council (UK) trains around 900 generic instructors each year. There is potential to specialise, for instance in Paediatric Life Support, and these well-regulated courses are internationally acknowledged. Advanced Trauma Life Support developed by the American College of Surgeons provides an international standard of training, with students with instructor potential being invited to pursue facilitator training.
Similarly, official appointments to visiting or honorary positions at universities are available to most clinicians engaged in teaching in some capacity. Ranging from honorary teacher roles to lecturers and fellows, such roles demonstrate ongoing commitment to an institution and may be linked to other research capacities. These grant access to university library facilities, a university email account and internal professional development opportunities.
Conclusion
The medical education landscape is complex and growing, but with many opportunities for training, both to improve skills and gain credentials for professional career development. This time of change is also a time of challenge: the specialty of medical education is a social science populated by empiricists, currently reconciling schools of thought less than 50 years old with ‘trial and improvement’ or questionnaire feedback alone (Leif et al., 2019; Norman, 2003; Reid et al., 2018). While there are more opportunities for accreditation than ever before, educators face challenges borne out of the speed of change and an increasingly outcome-driven domain (Seiffge-Krenke and Weitkamp, 2019; Southgate, 2019). Clear guidelines on which qualifications are appropriate for each stage of training with standardisation of qualifications will help UK doctors benchmark their practice both locally and internationally. It is hoped that professional development will standardise best practice and increase the enthusiasm which has driven the development of medical education. It must be hoped that patients will ultimately benefit.
Key points
The specialty of medical education is increasingly organised and professionalised
There are now more accessible and accredited courses in medical education
A range of activities can demonstrate a commitment to medical education, ranging from day courses to a spectrum of higher degrees
Understanding the interface between medical education and higher education can ensure that study achieves dual accreditation
The cost of courses can be a major deciding factor when choosing courses and inevitably some courses offer better value than others
A variety of lecturing and mentoring activities can be used as experience towards a higher degree or as accredited roles, apart from the more traditional degree courses
Supplemental Material
sj-pdf-1-ino-10.1177_17557380221135081 - Supplemental material for Becoming an accredited medical teacher in the UK
Supplemental material, sj-pdf-1-ino-10.1177_17557380221135081 for Becoming an accredited medical teacher in the UK by Dr Matthew F Flynn, Dr Peter J Eves and Professor Ahmed Rashid in InnovAiT
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.