
Abstract
Musculoskeletal complaints account for approximately 25% of consultations in general practice, with the knee being the second most common cause for consultation after the lumbosacral spine. A robust system for evaluation of knee pain in GP consultations is important for diagnostic and management strategies. The time limitations in primary care mean that a focused history and examination is appropriate. This article will take the form of a consultation, beginning with important points to be covered in history taking, discussing examination techniques and findings before considering diagnostic and management strategies.
Clinical case scenario
Kiran is a fit and well 21-year-old law student. She plays football and tennis regularly for her university teams. She has never had a serious knee injury. During training last weekend, Kiran turned to chase the ball and states ‘her knee went’. She experienced acute pain and was unable to play on. Her knee began to swell immediately. Her teammates helped her off the pitch.
She attended accident and emergency (A&E), an X-ray was performed and a fracture was ruled out. Kiran left after her X-ray and before being seen by a doctor as she had an essay due and felt reassured that there was no fracture.
The injury occurred a week ago and Kiran is still in considerable pain with limited movement. She has been unable to attend lectures this week as she could not walk to the lecture theatre. She is now worried that she did not wait in A&E and is frightened that she has caused irreparable damage.
The consultation
History taking
Pain is defined as ‘an unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage’ (International Association for the Study of Pain, 2020). This definition succinctly encompasses the multi-faceted nature of pain, and as GPs we are more skilled than most at understanding not only the physical effects of pain but also the psychosocial impact.
In the time-pressured world of general practice, use of a mnemonic such as SOCRATES (site, onset, character, radiation, associated features, timing, exacerbating or relieving factors and severity of pain) can be very helpful in ensuring key points have been covered. It also allows us to build a mental image of the possible mechanism of injury, and thus, diagnosis. Patient characteristics make certain conditions more likely, specific conditions are discussed in more detail below.
Sensitive history taking will reveal the psychosocial impact of knee pain; it can limit employment and recreational opportunities, and thus, impact mental health. Activities of daily living may be impeded by severe knee pain, especially in those with associated functional impairment and management must be tailored to the individual’s needs.
Serious knee pathology, though uncommon, can affect individuals of all age groups. The main conditions to consider are malignancy, infection and inflammatory arthropathy. It is important to ensure that history taking includes appropriate systems review to identify individuals presenting with these serious conditions.
Examination
The knee is a complex hinge joint that is comprised of two bony articulations: patello-femoral and tibiofemoral as detailed in Fig. 1. The articular surfaces are incongruent, and so knee stability is provided by a number of knee ligaments and the muscles surrounding the knee (Abulhasan and Grey, 2017).
Examination of a patient with knee pain can begin before the patient has even entered the consulting room. Wherever possible it is helpful to inspect the patient’s gait as they walk to the room and note the presence of an antalgic gait or the use of walking aids. With the knee exposed, one can look for any obvious deformity such as fixed flexion, valgus deformity, bruising or large effusions. Skin complaints such as psoriasis may suggest the possibility of a psoriatic arthropathy, and infection or trauma to the skin overlying the knee is also an important clinical sign to identify.
On palpation, assess for warmth and joint line tenderness. The patellar tap and sweep tests are easily and quickly performed to assess for knee effusion. Palpate for any tenderness along the patellar tendon or a gap in the patellar tendon and the quadriceps tendon, which may indicate tension rupture or tendinopathy.
When assessing movement, check active and passive flexion and extension. Pain and stiffness on flexion and extension are found in a wide range of knee pathologies. An inability to fully extend is an important clinical sign as it may be due to a large meniscal tear. Ask the patient to actively straight leg raise (SLR) to assess for patellar tendon injury. A patient with a severe patellar tendon injury would be unable to SLR.
Special tests
There are many ‘special’ tests employed when assessing the knee. In general practice, it is necessary to be confident in performing collateral ligament testing, the Lachmann and anterior draw test for cruciate ligaments, and the knee hyper-extension test as described in Table 1. Assessing for the posterior sag sign can identify possible posterior cruciate ligament (PCL) injury. As per the National Institute for Health and Care Excellence (NICE) clinical knowledge summary on the assessment of knee pain, McMurray’s test is no longer recommended for routine use in general practice (NICE, 2022a).
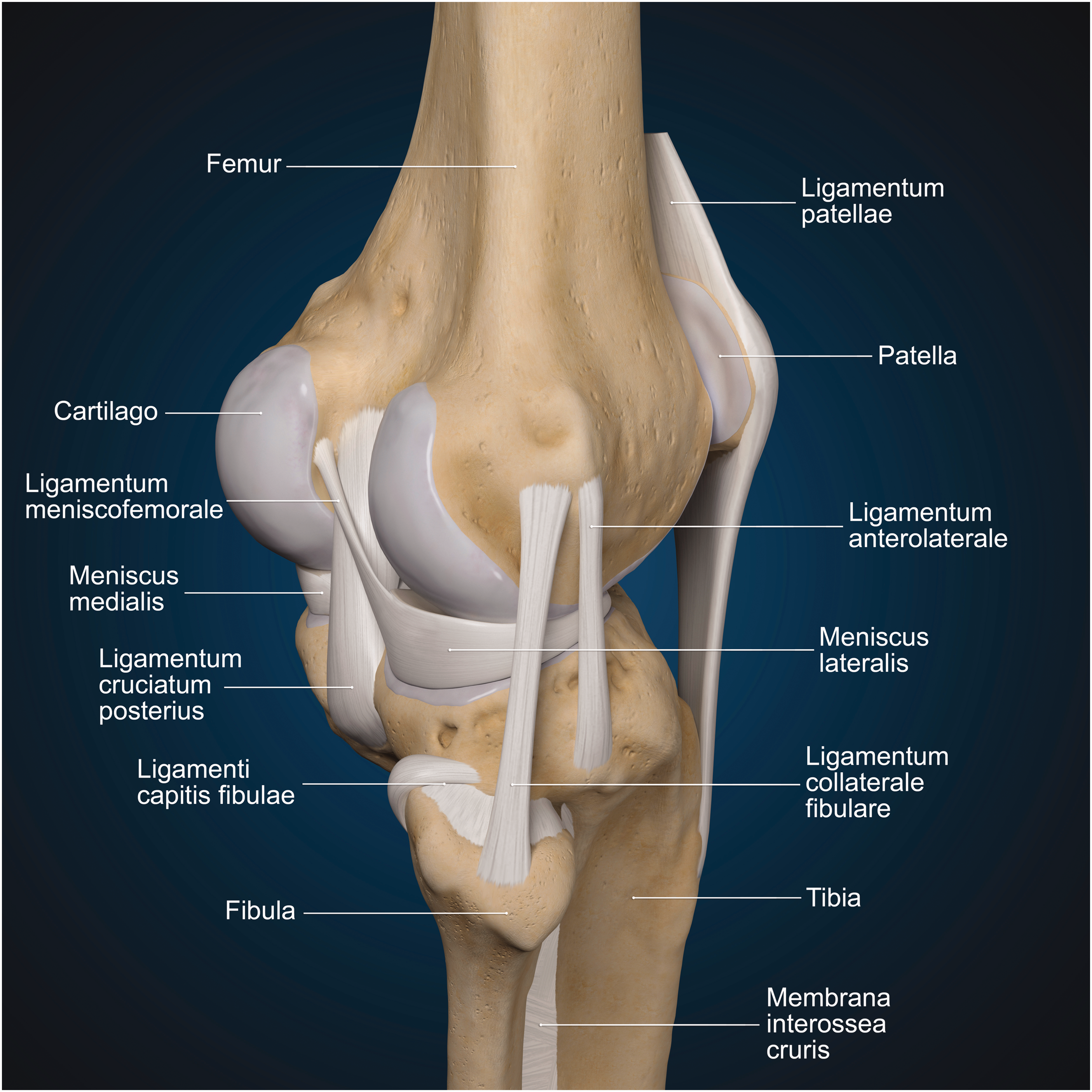
Knee anatomy.
Special tests for knee assessment.
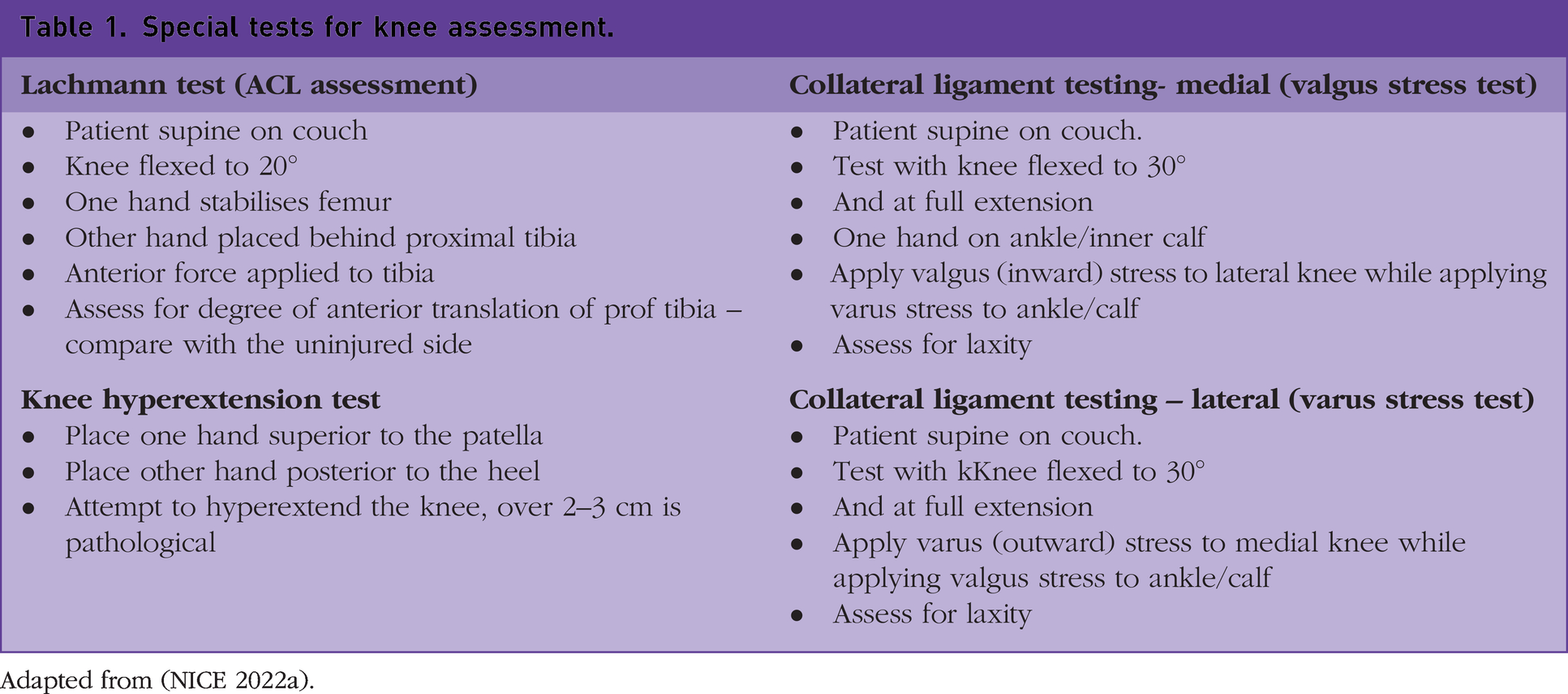
Adapted from (NICE 2022a).
Management
Although the specific management of knee pain depends largely upon the suspected condition, the first priority is to address and treat the patient’s pain. Analgesia should be tailored to best suit each patient and take their individual characteristics into account. Both topical and oral agents are available with risks and benefits of each medication being explained to the patient. It is impossible to cover all causes of knee pain in one article, and so, the most common causes and those warranting urgent orthopaedic referral have been included. The causes of knee pain affecting children and adolescents are not covered in this article.
Osteoarthritis
Osteoarthritis is one of the most common causes of knee pain and tends to present with activity-related knee pain and stiffness. Swelling may be present. According to NICE Quality Standard 87 individuals aged over 45 years and with symptoms typical for osteoarthritis can be diagnosed without imaging (NICE, 2022b). This can be difficult for patients to accept, as they often expect imaging. It is helpful to explain that there is little correlation between the osteoarthritic changes seen on X-ray and the physical symptoms experienced by the patient. X-rays may be indicated if there is diagnostic uncertainty, a rapid change in symptoms or history of acute trauma.
Topical non-steroidal anti-inflammatories (NSAIDs) can be offered in those with knee osteoarthritis. Treatment can be stepped up to oral NSAIDs provided this is appropriate for the patient. Gastric protection with a proton pump inhibitor should be considered (NICE, 2022b). NSAID courses should be kept to the shortest duration possible. Paracetamol and opioids should not be routinely prescribed for those with osteoarthritis. Intra-articular corticosteroid injections for knee osteoarthritis can be considered if pain cannot be controlled and to help improve knee function. Patients must be informed that pain relief tends to be short lived following corticosteroid injection. Serial injections can cause cartilage volume loss and the progression of osteoarthritis and should be avoided when possible (Heidari et al., 2020).
There is high-quality evidence that exercise and weight loss in overweight and obese individuals can improve pain and function in those with knee osteoarthritis (Jamtvedt et al., 2008). It can be helpful to explain to patients how these interventions work, as sometimes individuals feel they are being ‘fobbed off’ or definitive treatment is being deferred.
Exercise is postulated to reduce peripheral sensitisation to pain and local inflammatory responses (Susko and Fitzgerald, 2013). A reduction in body weight will reduce the force being transmitted through weight-bearing joints, such as the knees, and has been proven to improve mobility and reduce self-reported pain secondary to osteoarthritis (Messier et al., 2004).
Websites such as those detailed in Box 1 have online exercise videos specifically designed for those with knee osteoarthritis to follow at home. A multi-disciplinary team approach is useful in supporting all patients, especially the elderly. Physiotherapists, occupational therapists and social workers can assess and optimise the home environment to allow individuals to retain their independence as far as possible. Orthotics can help with aids that may improve patient comfort and function. Failure to improve despite first line management strategies would warrant onward referral. Physiotherapy is beneficial in those with osteoarthritis (Fransen et al., 2001) and patients may be able to self-refer in certain areas.
Helpful resources for patients.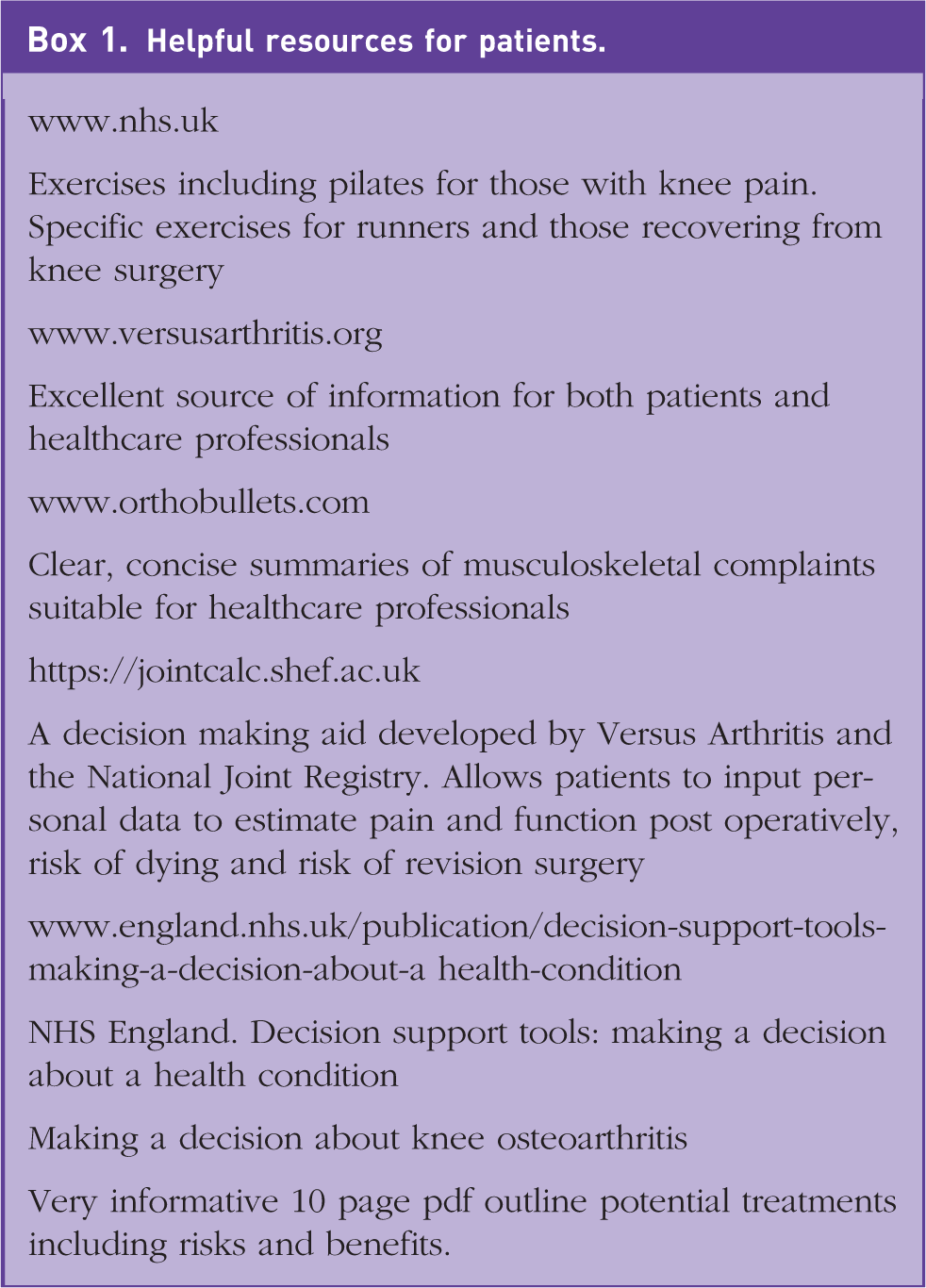
Orthopaedic referral is warranted for those considering definitive treatment, such as partial or total knee replacement. Decision making tools, as included in Box 1, are available online to help support patients with the management of their knee osteoarthritis including whether they feel surgical intervention is acceptable to them.
Low-impact fractures
Low-impact fractures may also present to general practice, they are more common in the elderly age group. Those with previous arthroplasty are at risk of peri-prosthetic fractures. The Ottawa knee rules as shown in Box 2 are highly sensitive at identifying those with knee fractures secondary to trauma (Yao and Haque, 2012). The severity of the pain, nature of the injury and timing of presentation to general practice will dictate whether the radiograph is best performed in an A&E setting or can be safely requested as an outpatient. Ottawa knee rules.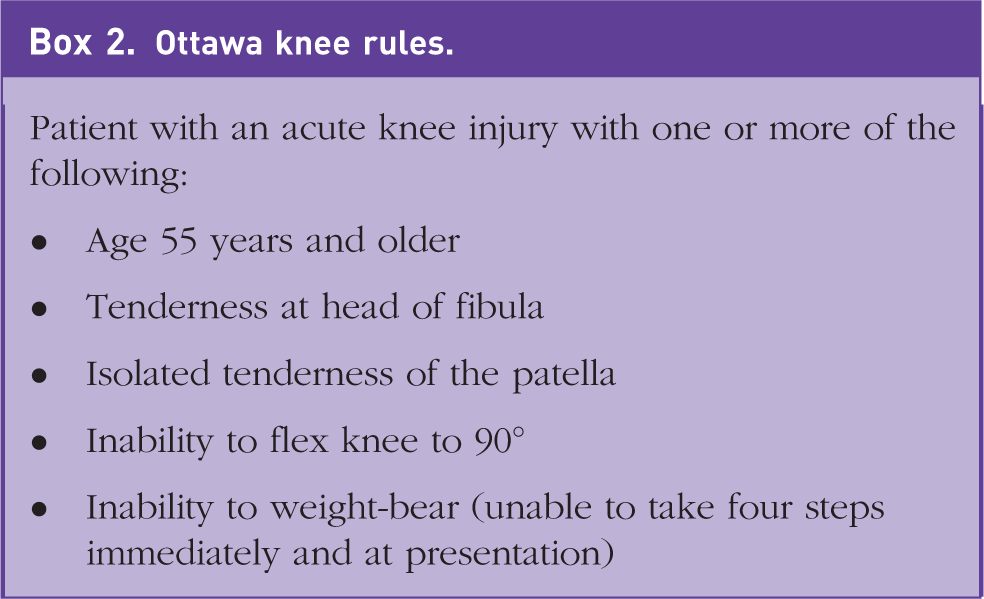
Sporting injuries
Sporting injuries are also common reasons for knee pain, especially for patients in a younger age bracket. Diagnosis of these conditions and referral for timely intervention can be extremely important. The main sports knee injuries seen are anterior cruciate ligament (ACL) injuries, meniscal injuries and collateral ligament injuries. Ligament injuries are commonly referred to as ‘sprains’ and can be graded 1 (a few torn ligamentous fibres with stable joint), 2 (a larger tear with increased joint laxity) and 3 (a complete ligament tear with joint instability). The common scenarios mentioned below refer mainly to higher-grade sprains or complete ligamentous rupture, and it should be remembered that a spectrum of injury can occur involving multiple structures.
ACL injuries
ACL injuries are often non-contact, twisting injuries characterised by an audible pop or crack and a large immediate swelling. Individuals are usually unable to continue their activity and so present to the A&E department. These injuries can be missed if patients do not immediately present or the injury is not recognised in A&E. Patients with a history typical for an acute ACL injury, especially if coupled with a haemarthrosis and an unstable knee, should be assessed by an appropriate specialist within 2 weeks (British Orthopaedic Association, 2020). Urgent referral would not be indicated for those with a relatively stable knee and minimal functional impairment. There are both operative and non-operative treatment options available. PCL injuries are less common and rarely occur in isolation, they usually result from direct impact to the flexed knee, such as a knee hitting the dashboard during a road traffic accident. Subtle PCL injuries may be minimally symptomatic, although there can be swelling and functional impairment, especially if other knee structures such as menisci are involved.
Meniscal injuries
Meniscal injuries can happen as a result of an acute injury or secondary to degenerative changes. Acute injuries tend to be related to a twisting mechanism and present with immediate swelling, though usually to a lesser extent than that produced by ACL injury. Bucket handle meniscal injuries are particularly worrisome and occur when there a tear or separation involving over 25% of the meniscus (British Association for Surgery of the Knee (BASK), 2019). These injuries tend to present with a ‘locked knee’ and an urgent referral for consideration of arthroscopic surgery is advised (BASK, 2019). Degenerative meniscal tears develop more progressively and are common amongst the general population. They tend to present with intermittent locking, catching, swelling and sharp pain. The role of meniscectomy in degenerative tears, especially when coupled with osteoarthritis, has become increasingly controversial. Non-operative interventions such as analgesia, physiotherapy and exercise should be considered, although if symptoms persist for more than 3 months, referral would be indicated (BASK, 2019).
Collateral ligament injuries
Collateral ligament injuries tend to be caused by a direct blow to the side of the knee, as may occur in contact sports such as football or rugby. Patients experience pain, swelling and the knee may feel unstable. The medial collateral ligament is injured more frequently than the lateral collateral ligament. Laxity may be found on collateral ligament testing. Treatment is usually non-operative, although fracture clinic referral for fitting of a knee brace would be appropriate.
Patellar tendon rupture
Patellar tendon rupture is an uncommon injury that tends to occur after sudden quadriceps contraction in a flexed knee position. A typical history would be acute pain during jumping sports such as basketball, patients may also report hearing a ‘pop’. There is usually acute swelling, inferior aspect knee pain and difficulty weight-bearing. An urgent referral is warranted, as immediate repair produces superior results (Greis et al., 2005). Pathways will differ between regions, but often a direct referral to fracture clinic or a virtual fracture clinic is available.
Quadriceps tendon injuries
Quadriceps tendon injuries are more common in those aged over 40 years and may occur after forced contraction of the quadriceps muscle such as missing a step while descending the stairs. As with patellar tendon rupture, risk factors include existing tendinopathy, steroid use and systemic diseases such as diabetes. Pain is localised to the insertion site of the quadriceps tendon, and as with patellar tendon injuries, there may be a palpable gap and absent SLR. Although surgical intervention is not always necessary, an urgent orthopaedic opinion is advised, as knee immobilisation may be required (McKean, 2021).
Imaging has not been discussed for suspected ligamentous or meniscal injury, as individual clinical commissioning groups will have their own guidelines for primary care access to further imaging modalities such as magnetic Resonance imaging, and it is important that GPs are familiar with these situations. In general, acute knee pain after trauma that persists for over 6 weeks in a previously non-symptomatic joint is an indication for further imaging.
Knee pain can also occur without any clear precipitating trauma. Patellofemoral pain is experienced often in young female patients (Callaghan and Selfe, 2006). The aetiology of this pain is not well understood and has been attributed to a range of conditions including patello-femoral cartilage injury, patella maltracking, hyper mobility and patello-femoral dysplasia. Patients present with anterior knee pain exacerbated by activities such as using the stairs or squatting. This finding may be reproducible on examination. Physiotherapy is a suitable treatment modality for those presenting with patella-femoral pain. If there is a clear precipitating activity, avoidance of it should be advised while the condition is causing pain. In those with patellar-femoral instability, physiotherapy aims to correct the biomechanics of maltracking patellae. Onward routine referral is appropriate should patients fail to respond adequately to conservative measures or to a 3-month course of physiotherapy (NICE, 2022a)
Tendinopathies
Tendinopathies of various insertion sites can occur, with patellar tendinopathy being most common. Patients tend to present with pinpoint tenderness at the site of the tendon insertion. Pain is worse with activity and certain movements such as jumping and landing. This presentation tends to be secondary to repetitive micro-trauma. Adaptation of aggravating activities, analgesia and graded exercise programmes are first line management steps.
Prepatellar bursitis
Prepatellar bursitis is the most common site of bursitis in the knee, the majority of cases occurs in males aged between 40 and 60 years of age (Baumback et al., 2014). It presents with knee pain, especially on kneeling and mild swelling over the anterior aspect of the knee overlying the patella. There will usually be a history of excessive kneeling, for example, those working as roofers, gardeners or carpenters. Aseptic prepatellar bursitis is usually managed conservatively with analgesia, compression and immobilisation. A history of rapid increase in bursa size, surrounding erythema and an immunocompromised patient make a septic bursitis more likely. Examination may reveal signs of trauma or skin damage overlying the bursa. Antibiotics are required and a same-day orthopaedic referral advised. Regular follow up is important for those with bursitis to ensure symptoms are resolving. Routine referral would be indicated for aseptic bursitis if there was no response to conservative treatment within 2 months (NICE, 2021).
Osteonecrosis of the knee
Osteonecrosis of the knee (also known as avascular necrosis) presents with pain that is insidious in onset, it may not be activity related and can occur at night. It tends to affect the medial femoral condyle and so pain may be felt in this area. It is more common in females, those over 60 years in age and with risk factors including steroid use, alcohol excess and sickle cell disease (Karim et al., 2015). This finding may be identified on radiographs requested by primary care. Initial management is conservative and includes analgesia and physiotherapy to improve quadriceps strength.
Both primary and secondary malignancy can affect bone. Of the primary bone malignancies, osteosarcoma is the most common with 550 new cases each year according to Cancer Research UK (2021). The lower limb is a commonly affected site in the body, specifically the distal femur and proximal tibia. Secondary malignancy is more common with prostate, breast and lung being the most common primary sites (Cancer Research UK, 2021). Points in the history that would raise alarm for malignancy and warrant an urgent 2-week wait referral are persistent knee pain at rest or during the night, systemic symptoms such as weight loss or night sweats and a previous history of malignancy (NICE, 2022a).
Septic arthritis and osteomyelitis
Septic arthritis and osteomyelitis are conditions that carry significant morbidity and mortality risks.
Acute onset pain with severe restriction of movement and evidence of a warm or erythematous knee would suggest a possible septic arthritis and warrants an urgent same-day admission to the orthopaedic team. This condition is much more common in those with inflammatory arthritis being treated with biologics (Galloway et al., 2011). Systemic symptoms may also be present.
The involvement of multiple joints with evidence of warmth and swelling could indicate an inflammatory arthropathy. Pain and stiffness are typically worse first thing in the morning and after periods of rest. Referral to rheumatology is required and patients should be seen within 3 weeks of referral (NICE, 2020). Referral policies will differ between departments, with some requesting that baseline bloods including rheumatoid factor and anti-cyclic citrullinated peptide (CCP) are performed prior to referral. Reactive arthritis is a form of inflammatory arthritis that occurs 1–4 weeks after certain genitourinary or gastrointestinal infections, namely Chlamydia, campylobacter, shigella and salmonella. It typically affects those aged 20–50 years, with men more commonly affected than women. Early stages are treated with NSAIDs, though it can become chronic requiring disease-modifying anti-rheumatic drugs (American College of Rheumatology, 2021).
In conclusion, knee pain is a common reason for presentation to general practice. There are a wide range of conditions that can cause knee pain, but a focused history and examination help establish a diagnosis, and thus, allow patients to receive the most appropriate care.
Key points
Knee pain is a very common presentation in general practice
Osteoarthritis is the most common cause of knee pain in general practice
Acute knee pain can be secondary to ligamentous and meniscal injury
A thorough history and careful examination can differentiate likely causes, although ligamentous and meniscal injuries share some clinical features
Patients with acute knee injuries, especially with marked effusion, instability and functional impairment, usually require urgent orthopaedic referral
Septic arthritis, primary and secondary malignancies, and inflammatory arthropathies can affect the knee and should be screened for in the history