
Abstract
Coeliac disease is a common autoimmune inflammatory condition of the small intestine that is triggered by dietary gluten. Symptoms include fatigue, diarrhoea, bloating, and abdominal pain, as well as extra-intestinal symptoms. The only treatment is a strict life-long gluten-free diet. Despite affecting 1% of the UK population, only 36% of those living with the condition are diagnosed. Undiagnosed coeliac disease can lead to complications, including digestive symptoms, malabsorption, osteoporosis and higher risk of small bowel malignancy. This article aims to raise awareness about the condition and highlight common presentations, investigations, management, and follow-up.
Clinical case scenario 1
James, a 34-year-old fit and healthy architect, presents to your face-to-face clinic. He reports a 3-month history of generalised abdominal pain, loose stools and fatigue. He has been putting off going to see the doctor, as he felt his symptoms were related to a trip to India 3 months ago; his colleagues have all been well. He looks pale. He has no past medical history and no family history of inflammatory bowel disease. Abdominal examination is normal. Full blood count shows microcytic anaemia and faecal immunochemical testing is negative.
Epidemiology
Coeliac disease is an autoimmune condition that affects 1% of the United Kingdom (UK) and European population (Coeliac UK, 2022). Currently, only 36% of those living with the condition in the UK are diagnosed, and the average length of time from the onset of symptoms to diagnosis is 13 years (Coeliac UK, 2022). Coeliac disease may present at any age with variable symptoms. It most commonly diagnosed between the ages of 50 and 69 years, however, the prevalence of paediatric coeliac disease is increasing in the UK (BMJ Best Practice, 2022; Schuppan and Dieterich, 2022). Those at increased risk of coeliac disease include first- and second-degree relatives of patients with coeliac disease, as well as individuals with type 1 diabetes, autoimmune thyroiditis, Down syndrome and Turner syndrome.
Clinical presentation
Adults
Coeliac disease is a systemic autoimmune disorder triggered by gluten peptides and is characterised by mucosal inflammation, crypt hyperplasia and villous atrophy in the small bowel. Presentation of coeliac disease is variable. Common gastrointestinal symptoms include diarrhoea (may be foul-smelling), bloating, abdominal pain or discomfort and weight loss. Extraintestinal manifestations of coeliac disease include fatigue, dermatitis herpetiformis and atrophic glossitis. Other common clinical presentations in adults are iron, vitamin B12 or folate deficiency anaemia and osteopenia as a consequence of malabsorption. The main indicators for coeliac disease testing are outlined in Table 1.
Indicators for coeliac disease testing as per Coeliac UK; adapted from NICE guidelines (2010).
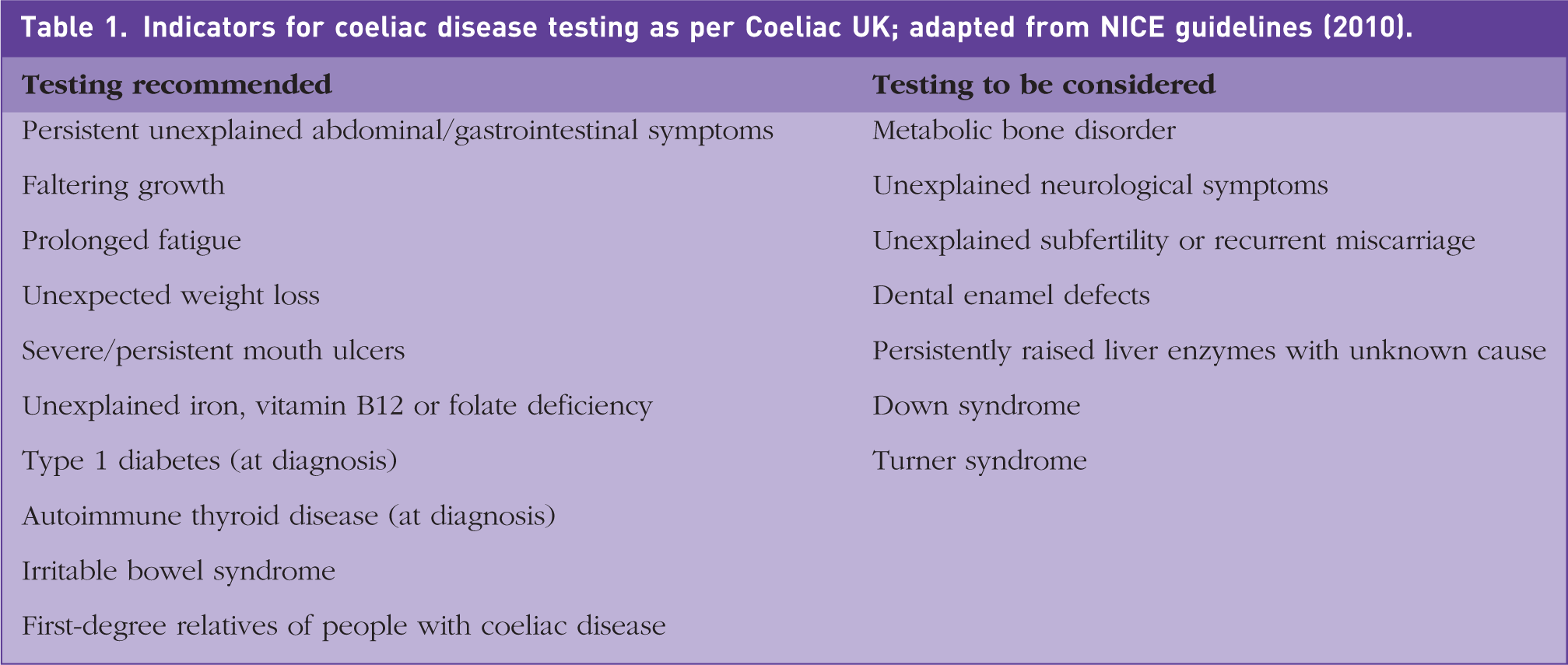
It is important to note that at least 20% of patients are asymptomatic (BMJ Best Practice, 2022). Therefore, National Institute for Health and Care Excellence (NICE) guidelines also recommend considering a diagnosis of coeliac disease with a number of unexplained or refractory conditions, such as depression or anxiety, peripheral neuropathy or ataxia, miscarriage or subfertility, persistently raised transaminases on liver function tests, dental enamel defects, osteoporosis and hyposplenism. Any patient with these symptoms may benefit from coeliac serology testing as part of their primary care investigations.
Infancy
Children may have similar presentations to adults, as well as presenting with suboptimal growth or delayed puberty. Rarely, children may present with haemodynamic and metabolic consequences of severe dehydration, referred to as a coeliac crisis.
Women
The reproductive period for female patients with coeliac disease is shorter than average, as the mean age for menarche is higher than average and early menopause is common (Sher, and Mayberry, 1994). Post-menopausal women diagnosed with Coeliac disease are at a particularly high risk of low bone mineral density, and therefore, osteoporosis (Coeliac UK, 2022). Clinicians should consider coeliac disease when investigating female patients for subfertility.
Investigations
Serology testing
The first-line investigation in suspected coeliac disease is serum immunoglobulin (Ig)A tissue transglutaminase antibody (tTGA). Higher values of IgA-tTGA have increased positive predictive value, but may not correlate with severity of symptoms. Concurrent testing of quantitative IgA may be helpful to assess for IgA deficiency, which may cause IgA-tTGA to be insensitive. Second-line testing is serum IgA endomysial antibody (EMA), in cases where IgA-tTGA is unavailable or weakly positive. IgA-EMA has greater specificity, but lower sensitivity, than IgA-tTGA. If there is evidence of IgA deficiency, consider checking serum IgG EMA, IgG deamidated gliadin peptide, or IgG-tTGA. Interpretation of results and indication for referral is outlined in Fig. 1.
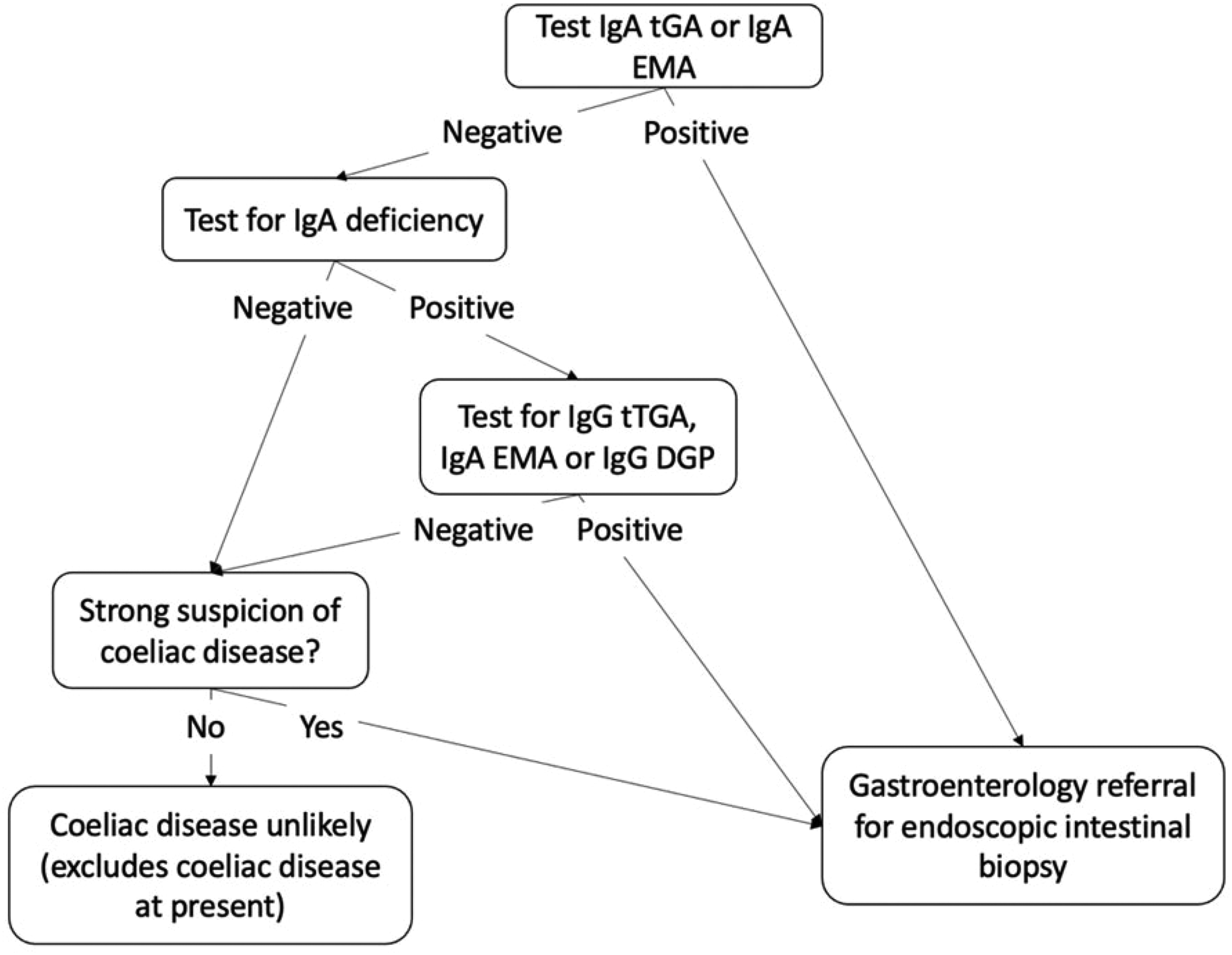
Interpreting coeliac disease serology results as per NICE guidelines.
In order to provide an accurate diagnosis, coeliac serology testing requires the patient to eat gluten-containing foods beforehand. Wheat, barley or rye must be consumed in at least two meals a day for a minimum of 6 weeks before testing is performed. As coeliac disease can present at any age, re-testing is indicated despite previous negative serology if a person presents with new symptoms of coeliac disease.
Endoscopy
All patients with positive serology should be referred to gastroenterology for endoscopy. Patients with negative serology, but a high clinical suspicion of coeliac disease or significant risk factors as described above, should still be referred. Ideally, endoscopy should be completed within 6 weeks of referral. In some cases, specialist diagnosis may be confirmed by repeating serology without the need for endoscopy.
Endoscopic features suggestive of coeliac disease include visible atrophic mucosa with loss of folds, evidence of fissures or nodularity, scalloping and prominent submucosal vascularity. However, these have low sensitivity and appearance may be normal in up to a third of cases at diagnosis (BMJ Best Practice, 2022; Schuppan and Dieterich, 2022).
Small bowel biopsy
The gold standard test to establish diagnosis is small bowel histology. In most centres a duodenal biopsy will be performed at the same time as endoscopy. As with serology testing, duodenal biopsy should be performed while on a gluten-containing diet and multiple biopsies are recommended to confirm the diagnosis.
Skin biopsy
Dermatitis herpetiformis is pathognomonic for coeliac disease. Any patient who presents with skin lesions suggestive of dermatitis herpetiformis (see Fig. 2) requires a skin biopsy initially. Results have high sensitivity and specificity, where direct immunofluorescence showing granular deposits of IgA at the dermal papillae of both the lesion and the skin surrounding the lesion indicates a positive result. One-in-four patients with coeliac disease will have dermatitis herpetiformis (Pelowski and Viera, 2014).

Dermatitis herpetiformis.
Clinical case scenario 2
Ellie is a 3-year-old girl brought to the GP by her parents due to her becoming a picky eater and complaining of abdominal discomfort. They notice she has been passing foul-smelling stools and has stopped gaining weight after previously growing along an appropriate height and weight centile. Blood tests show a raised level of IgA tissue transglutaminase antibodies and her parents have cut out gluten from her diet. They would like more information regarding further testing, additional diet plans and whether her parents and her siblings will need to get tested as well.
Management
Diet
The only treatment for coeliac disease is a life-long gluten-free diet. This should not be started until diagnosis is confirmed by a gastroenterologist, in order to allow for full testing to be completed. Patients should be referred to a dietitian specialising in coeliac disease for appropriate dietary counselling and to assess for nutritional deficiencies. Patients with coeliac disease need to abstain completely from consuming gluten-containing foods, typically those based on wheat, barley and rye. This includes bread, cereals, pasta, biscuits, cakes and pastries. Many foods may have gluten-containing products as fillers or flavouring, such as ready meals, soups, sauces and sausages. Other foods may be contaminated with gluten during processing or packaging, such as when gluten-containing foods are fried in the same oil as gluten-free products or when products such as beer are malted.
Prescribing gluten-free products
Gluten-free staples were previously prescribed for patients in the UK. Recent changes have been made, reducing NHS funding of gluten-free products, due to increasing availability in supermarkets. In England, prescriptions are restricted to gluten-free bread and flour mixes, though many local authorities do not fund gluten-free food prescriptions at all. In Scotland, Wales and Northern Ireland prescriptions may include other staple foods such as pasta or cereal (NHS England, 2018). Prescription is based on a monthly allocation of units depending on age, gender and pregnancy/breastfeeding status. Each food item, based on weight, counts as a certain number of units and prescribers are given a recommended number of units per month for each age group. More information regarding prescribing can be found on the Coeliac UK website, including a weekday prescribing helpline.
Follow-up
Patients with confirmed coeliac disease should have an annual review that includes assessment of any persistent or recurrent symptoms, as well as the patient’s adherence to their diet. (NICE 2020) Further monitoring includes body mass index, screening for associated depression and or anxiety and assessing for nutritional deficiencies. Clinicians should consider offering annual blood test monitoring for coeliac serology to confirm the reported adherence to a gluten-free diet, full blood count and ferritin to rule out anaemia and its causes, liver and thyroid function tests for associated autoimmune liver and or thyroid disease and calcium and vitamin D for deficiency due to malabsorption. Another consideration in adults is the risk of osteoporosis requiring a dual-energy x-ray absorptiometry scan. Patients should be referred to a specialist or dietitian if there are any concerns about intentional or inadvertent exposure to gluten, unexplained symptoms of coeliac disease despite treatment or suspected nutritional deficiencies.
Complications
Diagnosis and appropriate treatment of coeliac disease is imperative to prevent long-term complications. As well as the previously mentioned consequences of coeliac disease, such as malabsorption or osteoporosis, undiagnosed coeliac disease can lead to ulcerative jejunitis, functional hyposplenism and recurrent pancreatitis. People with untreated coeliac disease also have an increased risk of upper gastrointestinal carcinomas and small bowel and extra-intestinal lymphomas.
Vaccinations
There is no consensus national guideline regarding vaccinations. However, Coeliac UK recommend patients should have annual influenza vaccination, as well as 5-yearly pneumococcal vaccine boosters due to a higher risk of hyposplenism in coeliac patients. Meningococcal vaccination should also be considered.
Clinical case scenario 3
Juan is 45 years old and experiencing regular bloating, abdominal discomfort and loose stools. He is known to have type 1 diabetes mellitus and irritable bowel syndrome. Testing for inflammatory bowel and coeliac disease, including small bowel biopsy, was negative 5 years ago. Although a change in diet was initially helpful, he feels his symptoms have become worse over the last few months, even with strict adherence to a diet low in fermentable carbohydrates. On examination he is found to have abdominal bloating and clusters of small blisters on his back and knees. Full blood count shows a macrocytic anaemia. His sister was recently diagnosed with coeliac disease. Juan asks whether there are any other investigations or treatments for his symptoms.
Key points
Coeliac disease affects an estimated 1% of the UK population It is currently underdiagnosed; only 36% of those living with the condition in the UK are formally diagnosed Undiagnosed coeliac disease can lead to malabsorption, osteoporosis, ulcerative jejunitis, functional hyposplenism and increased risk of malignancies If a patient presents with new symptoms of coeliac disease, re-testing is indicated despite previous negative serology and must be done with patients on a gluten-containing diet Refer to a specialist dietitian upon diagnosis in order to improve diet adherence Annual check-ups are recommended for assessment of symptoms, adherence to a gluten-free diet, nutritional deficiencies and need for vaccinations