
Abstract
Swallowing is a complex interplay of nerves, muscles and protective reflexes which involves both involuntary and voluntary phases. Difficulty swallowing can occur due to a variety of underlying pathologies, but can broadly be differentiated into high (oropharyngeal) and low (oesophageal) dysphagia. Using case scenarios this article will highlight common dysphagia presentations encountered in general practice and their appropriate history, examination, investigation and management.
Clinical case scenario 1
A 62-year-old man presents with a 3-week history of difficulty swallowing. He describes a sensation of food ‘getting stuck’ at the level of the sternum. He has no dysphagia to liquids. He gives a long history of retrosternal burning discomfort after foods – particularly spicy meals and alcohol – which he usually manages with Gaviscon. He does not describe any significant weight loss. He is a current smoker with a 15-pack year history. Oropharyngeal, neck and abdominal examination is unremarkable.
The GP suspects he may have underlying gastro-oesophageal reflux disease (GORD), but as per National Institute for Health and Care Excellence (NICE) guidelines he is referred for an urgent 2-week wait endoscopy. His scope and subsequent biopsies reveal a benign oesophageal stricture and several areas of Barrett’s oesophagus.
Introduction
The process of swallowing is complex and involves co-ordination of a number of different muscles, nerves and involuntary/voluntary reflexes. For this reason, dysphagia can be a difficult presenting complaint to investigate and manage, with a plethora of potential differential diagnoses. This article will outline the physiology of swallowing and common underlying pathologies related to the phase of swallowing, ‘red flag’ symptoms and appropriate investigation and management strategies for the dysphagic patient.
Physiology of swallowing
‘Swallowing’ describes the continuous passage of a food bolus or liquid through the mouth, oral cavity, pharynx and oesopahgus to the stomach. The swallow is split into three phases: oral (preparatory and proper), pharyngeal and oesophageal. The main difference between the phases is that the oral phase is voluntary, whereas the pharyngeal and the oesophageal phase are involuntary. Table 1 gives a description of the components of the normal swallow along with the muscles and nerves responsible for the processes within each phase.
A summary of the phases of swallowing and the muscles and nerves involved with each stage.
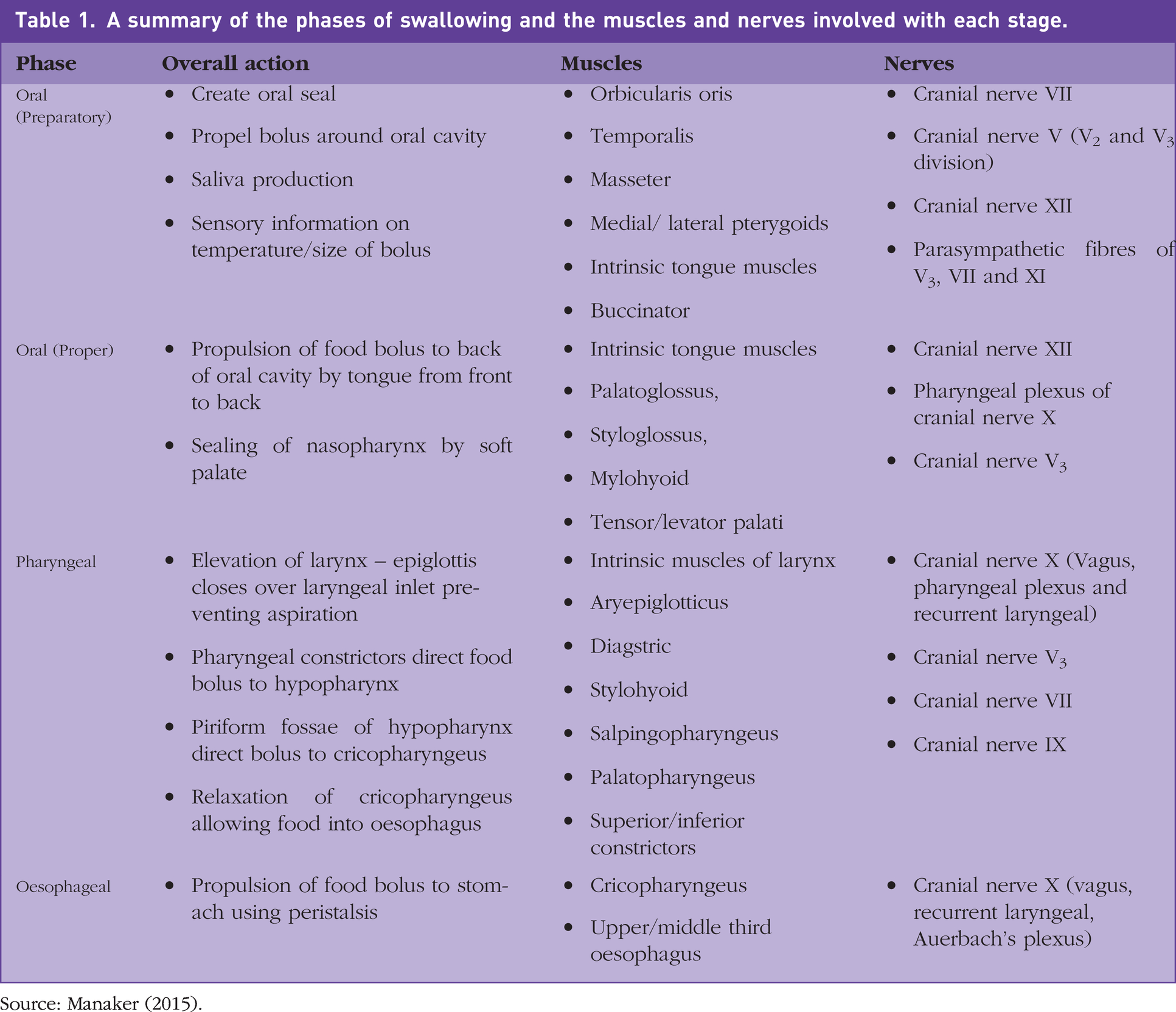
Source: Manaker (2015).
It is worth noting that each of these phases can vary in duration and efficiency for each individual, and can be affected by factors that are not directly related to pathology (age of the patient, nature of the food bolus, state of dentition). For example, presbyphagia is a broad term used to describe the (usually asymptomatic) change to an individual’s swallow with age. These changes are usually multi-factorial and can affect any phase of the swallow. Contributing factors may be iatrogenic (for example, polypharmacy leading to an elderly patient taking a number of different drugs such as anti-hypertensives, anti-cholinergics, angiontensin converting enzyme inhibiters that can predispose a patient to xerostomia), poor dentition/poorly fitting dentures, or normal physiological/neurological degeneration and loss of functional reserve leading to a prolonged or inefficient swallow. Even in the absence of pathology, most people can recall a time when something has become ‘stuck in their throat’ or ‘gone down the wrong way’ as a consequence of eating too quickly or ingesting a large, dry food bolus. Older patients, in particular, can report problems with the latter, with commonly referenced items including bread, rice and large tablets. Peas and other legumes with shells may also cause some gagging as swallow becomes more inefficient and skins of the vegetables stick to the posterior pharyngeal wall.
Protective reflexes
Given the involuntary nature of the pharyngeal and oesophageal phase and the close anatomical relationship between the larynx and the oesophagus, the pharyngeal phase of swallowing is when there is a risk of aspiration of the food bolus. As well as a series of co-ordinated movements of the palate and the larynx (sealing of the nasopharynx and contraction of the suprahyoid to cover the laryngeal inlet with the epiglottis), the swallow also has three protective reflexes to help prevent accidental aspiration. These include the gag reflex, the cough reflex and laryngospasm. The gag reflex can be identified in most cranial nerve or oropharyngeal examinations (if the tongue depressor touches the posterior pharyngeal wall). This is designed to regurgitate large food boluses that are at risk of obstructing the laryngeal inlet. The cough reflex acts to protect the airway from small amounts of fluid, and the laryngospasm reflex helps to protect the airway from larger fluid quantities. It is sometimes referred to as the ‘anti-drowning reflex’. Loss of any of these reflexes can be a sign of a neurological cause for dysphagia and should always be investigated.
Differential diagnoses
The differential diagnoses for dysphagia are listed in Table 2. Broadly speaking, dysphagia can be divided into oropharyngeal ‘high’ dysphagia and oesophageal ‘low’ dysphagia. In oropharyngeal dysphagia patients typically report food sticking in the throat, difficulty in preparing the food bolus or issue with transporting the bolus through the oral cavity and initiating the involuntary phase of swallow. For example, neurological causes of dysphagia may lead to palsy of the glossopharyngeal, vagus or hypoglossal nerve. Any of these could lead to weak palatal elevation, poor tongue coordination and pharyngeal constriction.
Differential diagnoses for dysphagia.
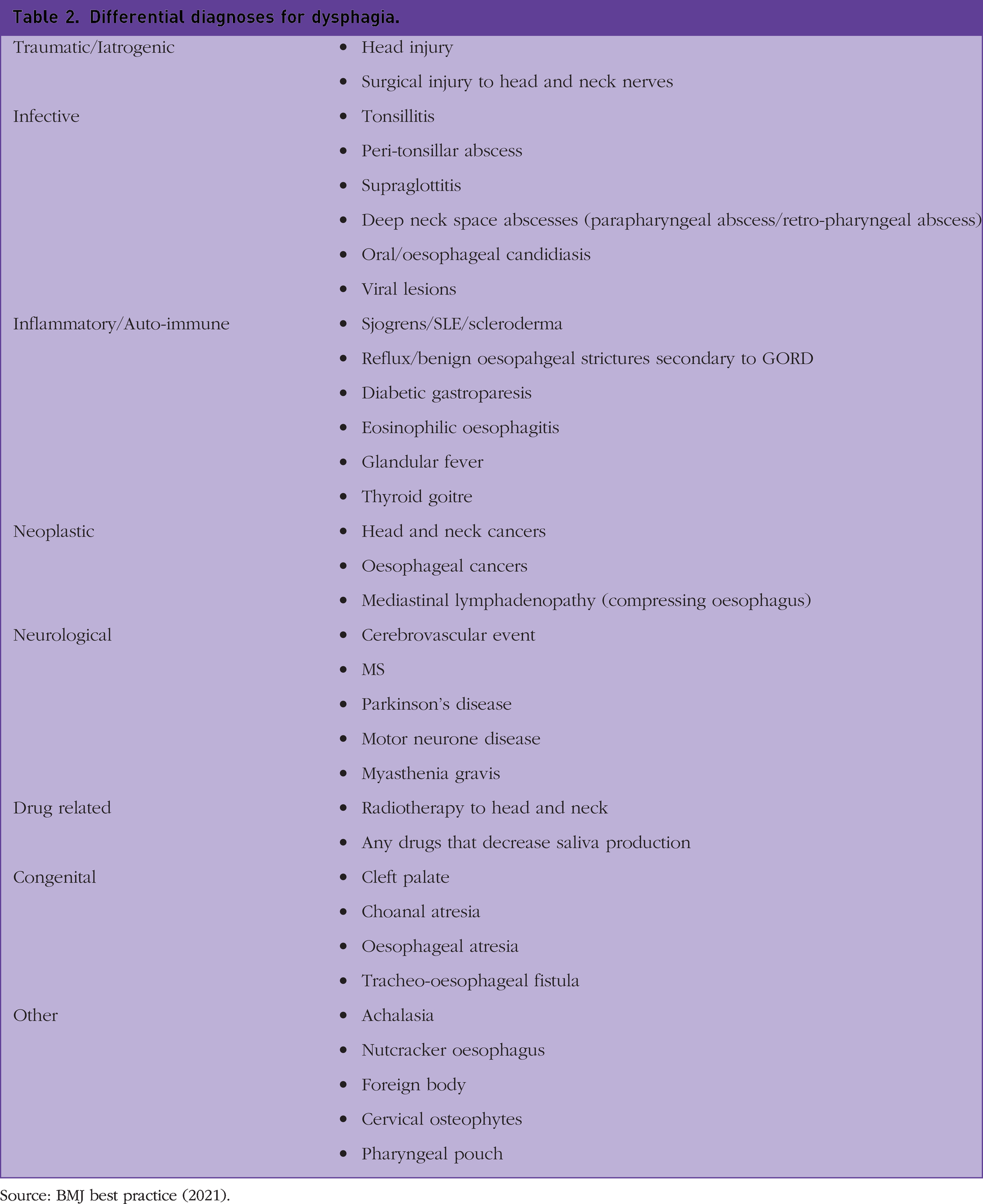
Source: BMJ best practice (2021).
In oesophageal dysphagia patients usually complain of food sticking lower down in the neck with retro-sternal discomfort. In contrast with oropharyngeal dysphagia, patients are more likely to give a history of progressive dysphagia that begins with difficulty swallowing solids, but eventually progresses to dysphagia to liquids.
Oropharyngeal causes for dysphagia
Infective ear nose and throat (ENT) causes for dysphagia are some of the more common presentations to general practice. They are often acute in onset and are usually accompanied by systemic features of inflammation, for example pyrexia and tachycardia.
Clinical case scenario 2
A 17-year-old female presents with a 3-day history of a sore throat and pain on swallowing. She suffers with tonsillitis regularly, but today describes the pain as predominantly right sided, and she has difficulty swallowing both solids and fluids. She has significantly limited mouth opening and a ‘hot potato’ voice. Examination is difficult, but the reviewing GP thinks they can see that her uvula is deviated towards the left tonsil and there is a right peri-tonsillar fullness. She has bilateral cervical lymphadenopathy. She has a fever of 37.9°C and an associated tachycardia. She has been fit and well up until this point.
Case 2 gives a fairly classic history of a quinsy or peri-tonsillar abscess. A peri-tonsillar abscess is not a severe tonsillitis, but rather a complication of tonsillitis. It is a collection of pus sitting superiorly to the tonsil in the peri-tonsillar space, causing restriction of the muscles of mastication, and therefore, the patient will present with trismus. Their pain will be worse on the affected side. It is almost unheard of that a patient will present with a bilateral quinsy. Quinsy needs urgent needle aspiration and is considered an airway risk; therefore, same-day referral is advised. Untreated, the abscess may extend into the parapharyngeal space, potentially causing compression of the airway.
Another common cause of oropharyngeal dysphagia is neurological conditions. Patients with chronic neurological conditions (such as Parkinson’s or multiple sclerosis) tend to describe a history of progressive dysphagia to liquids that progresses to solids. Liquids are fast moving and most difficult to control, and therefore, at highest risk of inadvertent aspiration in neurological weakness.
Clinical case scenario 3
A 75-year-old man presents with a very sudden onset of dysphagia to solids and liquids and associated dysphonia since this morning. He is systemically well. He has had a previous deep vein thrombosis many years ago and has recently been diagnosed with atrial fibrillation, but declined warfarin. On cranial nerve examination he has weak palatal elevation and his tongue deviates to one side. He is obviously dysphonic and when you ask him to take a small sip of water he appears to aspirate.
This man is at very high risk of a cerebrovascular accident (CVA). His symptoms are sudden in onset and abnormalities on cranial nerve examination (hypoglossal and vagus nerve) may point to a brainstem stroke. He needs urgent referral to the on call medical team for investigation.
Oesophageal causes for dysphagia
One of the most common oesophageal causes of dysphagia seen in ENT clinics is reflux. Reflux of stomach acid into the oesophagus causes inflammation of the mucosa leading to retro-sternal discomfort. These patients are typically referred to ENT with a sensation of globus or a ‘lump in the throat’ (due to constriction of muscles) and associated hoarseness of the voice (reflux of stomach acid onto the vocal cords). Some patients report concordant classic ‘heartburn’ symptoms, but others may suffer from silent reflux, with hoarseness and globus being their primary symptoms. Irrespective of chronicity of symptoms, any patients with dysphagia and hoarseness should be referred with urgency to ENT to rule out a laryngeal malignancy with fine nasal endoscopy. Prompt treatment is essential, as prolonged and untreated reflux can lead to Barrett’s oesophagus, which has malignant potential.
Clinical case scenario 4
A 65-year-old man presents to the GP with progressive dysphagia over the last 4 months. Initially he noticed after eating solids that he felt they were getting stuck in his chest with retro-sternal discomfort, which he attributed to heartburn. He has a long history of gastro-oesophageal reflux and is on a proton pump inhibitor, but is finding that they are no longer controlling his symptoms. He is now finding that he is getting the same sensation when drinking fluids. In the last month he has lost 14 kg in weight.
This man’s symptom history is highly concerning for an oesophageal malignancy. Progressive dysphagia to solids and liquids on a background of chronic reflux is suggestive of a malignant stricture and requires a 2-week-wait (urgent suspected cancer) endoscopy referral (Table 3).
Indications for urgent suspected cancer/2-week wait investigations.
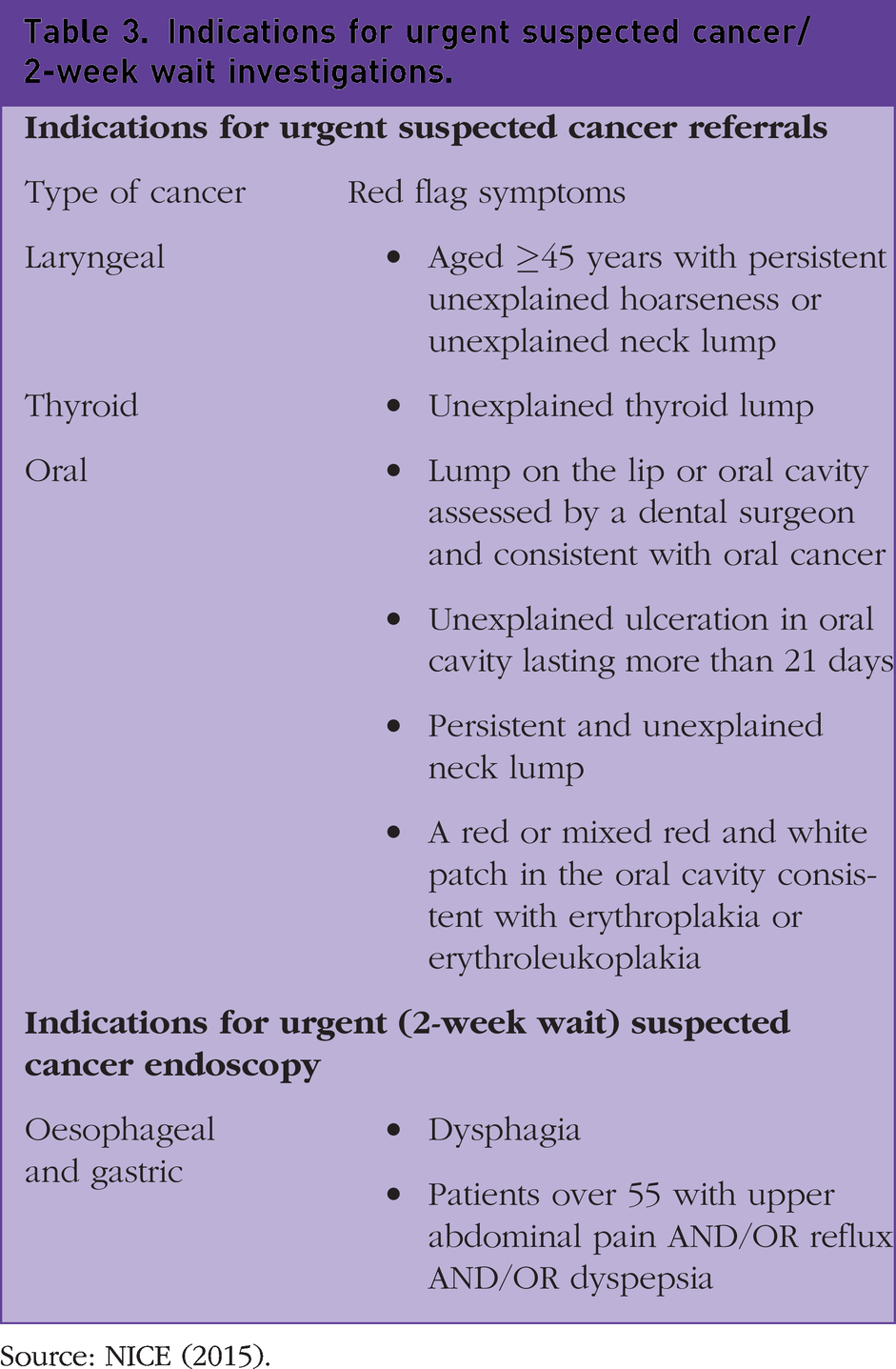
Source: NICE (2015).
In addition to associated symptoms of reflux, patients who describe low dysphagia may also give a history of spasmodic chest pain that is exacerbated by meals, but not by exertion. This can point the clinician towards an oesophageal motility disorder as an underlying diagnosis (once a cardiac cause has been excluded). Oesophageal motility disorders are a spectrum of conditions that are usually diagnosed based on one or more of the following features on oesopahgeal manometery: disorganised oesophageal peristalsis, high-amplitude contractions or increased lower oesophageal sphincter pressure. The two most common oesophageal motility disorders are diffuse oesopahgeal spasm (DOS) and achalasia. DOS is usually a non-progressive dysphagia to solids and liquids and is caused by repetitive, but ineffective, oesophageal peristalsis with normal lower oesophageal sphincter relaxation. The disorganised contraction of the oesopahgus can vary in strength, and so can lead to severe, spasmodic chest pain. In contrast, achalasia is progressive (usually slowly and over a period of many years) that is thought to be caused by degeneration of neurons in the oesophageal myenteric plexus. This leads to ineffective relaxation of the lower oesophageal sphincter and absence of peristalsis in the lower oesophagus. Patients will usually describe more severe dysphagia to solids. As the oesophagus is a muscular tube, systemic auto-immune conditions such as Scleroderma (CREST syndrome) can also lead to oesophageal motility-related dysphagia, due to direct attack of smooth muscle in the oesophagus by auto antibodies. These patients may describe that dysphagia to solids is improved if they swallow fluids at the same time.
Clinical case scenario 5
A 29-year-old male presents to the GP with a 24-hour history of dysphagia. He states he was eating a chicken breast the previous night for dinner and had to stop halfway through as it would not go down. He describes intermittent dysphagia to solid food since childhood that he has usually managed at home, but this time he is regurgitating any water he tries to swallow and cannot eat. He has no past medical history of note, other than asthma and rhinitis, which he states are well controlled with inhalers and topical nasal decongestants and steroids.
Clinical case scenario 5 is highly suggestive of eosinophilic oesophagitis (EO). This condition is caused by eosinophilic infiltration of the oesophageal mucosa leading to direct oesophageal injury and inflammation. The exact trigger of the eosinophilic infiltration is not understood, however, there seems to be a very strong association with concordant allergy (food allergies, asthma, atopic dermatitis). This is a useful diagnosis to consider in younger patients (young adults, adolescents) who give a history of dysphagia that dates back to childhood as incidence and prevalence is on the rise (BMJ, 2021). Patients may also complain of frequent vomiting and associated heartburn. In addition to a history of atopy, risk factors for development of the condition include male sex, a family history of EO and being Caucasian.
History
As a GP, one of the most important tools in the assessment of the patient with dysphagia lies in the history. A focused history will help to establish the level of dysphagia and the urgency with which to refer. Table 3 summarises the ‘red flag’ symptoms identified by NICE that should trigger an urgent suspected cancer referral for head and neck and oesophageal malignancy.
GPs should use focused questions to ascertain the level, onset and duration of the dysphagia, as well as the evolution and progression of symptoms. A good history will also tease out associated symptoms that may better direct the referral to the appropriate secondary speciality.
Symptoms that have been going on for years, or alternatively have presented extremely acutely are less likely to be malignancy related. Patients who have associated systemic features such as pyrexia and tachycardia are more likely to be suffering from an infectious cause of dysphagia. Drug history, past medical history (previous radiation therapy for head and neck cancers, atopy history, or diabetes) and family history (autoimmune conditions, familial malignancy) are also important.
One of the strongest indicators of malignancy is a progressive dysphagia. In head and neck and oesophageal malignancy alike, the classic pattern is dysphagia that begins with solids and progresses to liquids. The symptoms will usually have been present for weeks to months and may feature a sudden deterioration. In head and neck cancers, any change in voice with associated dysphagia should be considered a red flag, particularly in those high-risk patients, for example with a smoking or excess alcohol history. Sudden onset dysphagia and dysphonia in the absence of a systemic inflammatory response may suggest a neurological cause such as pseudobulbar palsy.
Examination
All patients complaining of dysphagia should be brought in for a face-to-face consultation. At initial point of contact, the GP can assess whether the patient appears cachectic or malnourished. As a baseline, any patient presenting with dysphagia should receive an examination of the oropharynx. This will highlight any issues with dentition or dry mucous membranes and any obvious asymmetry of the oropharynx. Examination of the oropharynx may reveal evidence of oral candidiasis.
The assessing clinician should perform a neck examination to assess for any thyroid lumps and palpable lymph nodes. Tender, bilateral lymph nodes are more suggestive of an infective pathology, whereas a painless, fixed, unilateral lymph node is more suggestive of malignancy.
Clinical case scenario 6
A 47-year-old man presents with a 6-week history of mild pain on swallowing. He feels like his food is sticking at the back of the throat, particularly on the right. He has noticed that his voice is more nasal than usual. He has lost a stone in weight in the last month. He is a non-smoker. On examination he has no trismus, but the right tonsil appears to be much larger than the left. There is no associated exudate and the uvula is central. There is a hard, fixed, right cervical lymph node.
This man has no associated infective symptoms and gives a progressive history. With weight loss and oropharyngeal asymmetry in addition to the neck examination findings, this man requires an urgent suspected cancer referral to ENT. These ‘red flag’ findings (Table 3) are suggestive of an oropharyngeal malignancy. Despite a lack of smoking history, this man’s younger age puts him at risk of viral (HPV)-mediated oropharyngeal malignancy.
All patients should receive a cranial nerve examination. The patient may also benefit from an upper and lower neurological examination if the clinical history is suggestive of a neurological cause. If the patient is not describing a potentially unsafe swallow (for example, significant aspiration/coughing/choking) then it may be a good idea to ask the patient to take a sip of water to assess what happens.
Investigations
NICE recommends that the primary investigation of choice in patients with dysphagia should be endoscopy (NICE, 2015). In addition to identifying established malignancy, direct visualisation of the oesophagus can also identify oesophageal pathology with malignant potential (such as Barrett’s oesophagus) and allows biopsy of any suspicious lesions/strictures. The indications for urgent 2-week wait endoscopy are outlined in Table 3. Irrespective of the phase in which the swallow is affected, the purpose of investigation should be to rule out a malignant cause.
Clinical case scenario 7
A 71-year-old gentleman presents with a 4-month history of intermittent dysphagia, mainly to solids. He describes a sensation of the food getting ‘stuck’ in the back of his throat. This has been getting progressively worse; however, in the last month he has noticed he has been regurgitating boluses of undigested food. His family has also remarked that he has halitosis. He finds sometimes food ‘feels like it goes down the wrong way’ and he coughs shortly after eating. He has been treated for three chest infections by the GP in the last 2 months.
The symptoms described in case 7 are classic symptoms of high dysphagia and suggest this gentleman is suffering from a pharyngeal pouch. Classic symptoms include intermittent dysphagia to solids, regurgitation of undigested foods, halitosis, aspiration and weight loss. Although pouches can be left untreated if they are small and not causing problems, this man appears to be suffering with aspiration pneumonia and warrants urgent referral to ENT for consideration of surgical or endoscopic management. The investigation of choice for these patients is a barium swallow.
If a pharyngeal pouch is suspected, a barium swallow may be of benefit while awaiting ENT outpatient assessment. A barium swallow is a study dedicated to assessing the pharynx, oesophagus and gastric fundus of the patient. Barium swallow is usually a well-tolerated test, which involves the patient ingesting a cup of radio-opaque barium. A series of plain film radiographs shows the progression of the barium throughout the alimentary tract. If malignancy is not suspected, this may be a less invasive investigative option in patients with dysphagia. For example, in patients with suspected oesophageal motility disorder, a barium swallow will help to indicate the level of the hold up or the phase of swallow affected or may display other characteristic signs to aid diagnosis such as the ‘corkscrew oesophagus’ seen in diffuse oesopahgeal spasm (BMJ, 2021). It can also identify levels of structuring in the oesophagus/compression of the pharynx and oesophagus by cervical osteophytes, as well as assessing the degree of aspiration/regurgitation.
Although there is no onus on the GP to request interventional investigations in patients with suspected malignancy, it may be helpful for the patient to have some preliminary blood work completed prior to assessment, such as assessment for anaemia and thrombophilia. If a systemic underlying auto-immune cause is suspected auto-immune bloods such as anti-ro, anti-la (Sjogren’s), antinuclear antibodies and anticentromere antibodies could also be requested before specialist referral. It may also be useful to refer a patient to cardiology to rule out a cardiac cause if chest pain is an associated symptom.
Management
Urgent suspected cancer referrals
In the post COVID era, to avoid delay in diagnosis due to significant backlogs in referral times and investigation time-lines, it is incredibly important that red flag symptoms are identified and there is a low threshold for referral as urgent suspected cancer (USC). Any patient presenting with dysphagia and constitutional symptoms (weight loss, night sweats, anorexia) should be referred immediately as USC. Patients with a progressive history of dysphagia (solids to liquids) should always be referred as USC. The secondary speciality to which these patients are referred to for further investigation can be guided by whether the dysphagia is high or low. If the dysphagia is high, the patient should be referred to ENT for rigid oesophagoscopy and microylaryngoscopy. If the dysphagia is mid or low then the patient requires an urgent oesophago-gastro-duodenoscopy. Other NICE recommendations for urgent 2-week wait referrals can be seen in Table 3.
Same-day speciality assessments
If the GP suspects a CVA, then the patient should be referred for same-day medical assessment. ENT same-day assessment should be sought for patients with suspected tonsillitis who cannot tolerate oral fluids/solids, quinsy assessment, concerns surrounding epiglottitis/deep neck space abscesses, and any dysphagia that is associated with stridor.
Clinical case scenario 8
A 45-year-old female presents with a 3-day history of severe sore throat and difficulty swallowing fluids and solids. She is no longer able to swallow oral analgesia and she appears to be spitting into a tissue. She has a fever and is tachycardic, however, on examination of her oropharynx there is nothing significant to see and her tonsils appear normal. She has mild dysphonia, but no stridor. Neck examination is normal.
Case 8 should be referred immediately. Negative oropharyngeal findings with significant dysphagia/odynophagia in an unwell patient warrant flexible nasendoscopy to assess for epiglottitis/supraglottitis. Stridor is a late sign and part of the airway ‘disaster triad’ but can, and may, develop if infections of the supraglottis are left untreated. These patients can deteriorate quickly; therefore, rapid identification and onward referral are imperative.
Irrespective of the underlying cause, same-day assessment should be considered if a patient cannot swallow at all or is visibly malnourished and unable to maintain adequate nutrition and hydration. These patients may need admission for enteral feeding. The secondary speciality to which the patient is referred will be based on the GPs assessment and main differential diagnoses.
Clinical case scenario 9
A 72-year-old attends an emergency GP appointment. She tells the GP that last night she was eating lamb and choked. She still feels like it is stuck in her throat. When asked where the food is stuck, she points to her neck. She has tried to drink water this morning and some fizzy drinks, but she vomited soon after. She is systemically well with no airway compromise, and she is swallowing her own secretions.
This lady in case 9 is describing a soft food bolus. Soft food boluses may resolve on their own, but some are persistent and may need treatment with intravenous anti-spasmodic drugs such as buscopan or in some cases endoscopic removal. A common cause of a soft food bolus is meat including lamb, beef and chicken. Soft food boluses causing obstruction (the patient is unable to eat or drink around the food bolus or shows signs of airway compromise). Any suspicion of ingestion of hazardous foreign bodies such as button batteries, bones or other sharp objects at risk of perforating the pharynx/oesophagus require same-day speciality assessment. The secondary specialty of choice will be based on local trust guidance.
Multi-disciplinary approach
Early referral to speech and language therapists and dieticians in patients presenting with dysphagia will aid in early support and rehabilitation of the patient with dysphagia. Our speech and language colleagues work by providing rehabilitation of the patient’s swallow and also offering useful manoeuvres that may make a patient’s swallow easier and safer. They can also carry out direct video assessment (fluoroscopy) whereby the patient’s dysphagia is assessed with regards to different consistencies of foods and liquids (for example, yoghurts, custards, milk). This can be incredibly useful in helping the patient to maintain a safe swallow and can also facilitate informed decisions between the patient and the GP regarding feeding at risk decisions. Speech and language therapists will usually only see the patient when pathology has been ruled out, so it may be worth checking with your local speech and language therapy department as to the investigations or referrals they like the patient to have undergone before accepting referrals.
The bottom line
Swallowing is a complex process that can be affected by a number of different variables. The huge variation in the factors that can affect each phase between individuals means that an early and thorough multi-disciplinary approach (involvement of our speech and language colleagues, appropriate imaging/investigation and referral to the appropriate speciality for interpretation of those investigations) is essential. This approach is integral to safe management of patients’ symptoms on the way to making the diagnosis and treatment for an identified pathology. This approach also enables management of symptoms when medical intervention is not possible.
Key points
A malignancy is the most important diagnosis to exclude in patients with dysphagia A complete assessment of the patient including a focused history and examination should be used to direct referral of the patient with dysphagia to the appropriate speciality An understanding of the physiology and phases of swallowing can help in the assessment and diagnosis of swallowing problems The primary investigation of choice in most patients with dysphagia is endoscopy If the patient is reporting absolute dysphagia and appears visibly cachectic, same-day admission for nutritional support should be considered Rehabilitation of dysphagia may depend on surgical or medical management, with input from speech and language therapists and, when appropriate, cancer nurse specialists