
Abstract
The seronegative arthritides are a heterogeneous family of rheumatological conditions that are characterised by joint pain and inflammation but without the presence of autoantibodies such as rheumatoid factor and anti-cyclic citrullinated peptide. They feature articular, axial and/or peripheral, and extra-articular manifestations. In this article we will discuss the clinical presentation and management of the seronegative arthritides. We hope to raise awareness of the signs and symptoms of these diseases to permit a timely referral to rheumatology, which should equate to improved outcomes for patients in terms of joint damage, pain, fatigue, loss of function and quality of life.
Clinical case scenario
A 23-year-old male patient presents to his GP with a 6-month history of worsening lower back and buttock pain. He is new to the practice, having moved to the area about 2 months previously in order to take up a place at medical school. His pain is worse in the morning and alternates between both buttocks, and it can take him an hour or so to get going in the morning, due to the associated stiffness. The pain has been waking him up during the second half of the night and he has lost 1.5 kg in weight. He reports feeling generally very fatigued. He believes his symptoms have deteriorated with his more sedentary lifestyle, and he has previously been very active, representing his school in regional athletic competitions. What is your differential diagnosis and how would you manage this case?
An overview of seronegative arthritis
A simple classification of seronegative arthritis is shown in Box 1. Depending upon the distribution of joint involvement the various seronegative spondyloarthropathies fall into one of either of the following groups, though some patients have features from both. The abbreviation SpA refers to the term spondyloarthritis. Types of seronegative arthritis.
Axial spondyloarthritis (radiographic and non-radiographic forms) Psoriatic arthritis Inflammatory bowel disease- associated arthritis Reactive arthritis (aka Reiter syndrome) Undifferentiated spondyloarthritis Less typical forms of seronegative arthritis include:
Juvenile spondyloarthritis
Axial spondyloarthritis
Patients with an axial spondyloarthritis (axSpA) have a disease that predominantly affects the axial skeleton (i.e. the sacroiliac joints and the spine). The group can be further subdivided into a radiographic and a non-radiographic phenotype. Those with radiographic axial spondyloarthritis (also known as ankylosing spondylitis or the abbreviation r-axSpA) have what is commonly referred to as ‘radiographic sacroiliitis’, which is a bit of misnomer and implies inflammatory change of the sacroiliac joints when the reality is that only structural damage, not inflammatory change, is visible on a radiograph. The non-radiographic type (also known as non-radiographic axial spondyloarthritis or nr-axSpA) is a catch-all category for patients without structural abnormality on pelvic radiographs but who have inflammation of the sacroiliac joint(s) on magnetic resonance imaging (MRI) imaging.
It is thought that patients with radiographic and non-radiographic disease are part of a continuum, and the term axial spondyloarthritis refers to the entire disease spectrum. Patients with non-radiographic axial spondyloarthritis may represent an earlier stage of axSpA, which is characterised by inflammation, but is without the obvious radiographic structural damage. Over time some, but not all, of those with nr-axSpA will progress to r-axSpA. Regardless of the two groups to which a patient ultimately belongs (i.e. radiographic or non-radiographic), a preference should be given to using the term axial spondyloarthritis, or axSpA, to refer to all patients.
Peripheral spondyloarthritis
Peripheral spondyloarthritis is inflammatory disease that predominantly involves the peripheral skeleton, i.e. elbows, knees, hands and feet. It is important, however, to remember that many patients with peripheral disease also have axial SpA, and many with axial SpA also have peripheral disease.
The Assessment of the Spondyloarthritis International Society (ASAS) has devised a set of classification criteria to help differentiate the axial from the peripheral spondyloarthropathies. Further details of this can be seen in Box 2 (Rudwaleit et al., 2009). ASAS classification criteria for axial spondyloarthritis (SpA).
Sacroiliitis on imaging1 plus one or more SpA features OR HLA-27 plus two or more other SpA features. SpA feature: Inflammatory back pain Arthritis Enthesitis (heel) Uveitis Dactylitis (sausage-digit) Psoriasis Crohn’s/colitis Good response to non steroidal anti-inflammatories Family history of spondyloarthropathy HLA-B27 Elevated CRP
Arthritis or enthesitis or dactylitis plus One or more SpA features Uveitis Psoriasis Crohn’s/colitis Preceding infection HLA-B27 Sacroiliitis on imaging
Two or more other SpA features Arthritis Enthesitis Dactylitis IBP ever Family history for SpA 1Sacoiliitis on imaging: either definite radiographic sacroiliitis or active inflammation on MRI suggestive of sacroiliitis associated with SpA Based on Assessment of Spondyloarthritis International Society (ASAS) Slide Library 2009: (www.asas-group.org/).
Axial spondyloarthritis
Axial spondyloarthritis (axSpA) is a chronic inflammatory arthropathy. Patients characteristically present with low back pain in their late teens and early twenties, and a complex interplay of immunological, hereditary and environmental factors is thought to contribute to the aetiology. The percentage of patients diagnosed with the non-radiographic form of axSpA is increasing over time as our ability to diagnose it with MRI imaging improves. In 1980, at the time of diagnosis, 100% of patients had the radiographic form of axSpA, whereas 40 years later only 50% of patients qualified for a diagnosis of the radiographic form and the remainder had the non-radiographic version (Benavent and Navarro-Compán, 2021).
In 2015, a group of individuals undertook a cross-sectional cohort study of patients in the UK in order to obtain prevalence figures for axSpA (Hamilton et al., 2015). They applied imaging modalities and modern classification criteria to patients presenting with inflammatory back pain, as the authors were of the opinion that inflammatory back pain is a cardinal symptom of axSpA. The study results appeared to show that estimates of prevalence in a primary care population varied with the diagnostic criteria used. For example, the study estimated the prevalence of axSpA to be 1.2% using the European Spondyloarthropathy Study Group criteria, 0.3% using the ASAS criteria and 0.15% using the modified New York criteria.
Estimates had originally suggested that the ratio of male-to-female patients diagnosed with ankylosing spondylitis (AS) was of the order of 10:1, but by the early 2000s, that ratio was approaching 1:1 (Kennedy et al., 1993). Female patients may have a slightly different disease phenotype when compared with male patients: peripheral arthritis, fatigue, functional impairment, tender points and enthesitis occur more commonly in female patients.
We know comparatively little about the pathogenesis of the axial spondyloarthropathies. The most important genetic risk factor is HLA-B27, but there are other related major histocompatibility complex genetic loci. Exogenous factors such as mechanical stress (Ansell et al., 2016) and infection also play a role alongside endogenous factors such as gut dysbiosis (Watad et al., 2018) and microdamage to entheses and articular connective tissues.
Long delays before diagnosis are associated with a number of less favourable outcomes, including higher risk of work disability or unemployment, higher rates of job loss, and potentially increased healthcare costs (Yi et al., 2020). The National Axial Spondyloarthritis Society (2020) aims to reduce the average diagnostic delay from eight and a half years to just one year. They believe that this ‘Gold Standard Time to Diagnosis’ project will ‘deliver dramatic health and wellbeing improvements for those affected, enabling more patients to access appropriate treatment earlier and improve their health and well-being’. Recent systematic review (Hay et al., 2022), however, appears to suggest that despite improvements over several decades experienced by patients receiving a diagnosis of axSpA, delays remain ‘unacceptably long’. In contrast with previous studies, Hay failed to demonstrate any influence of gender difference on diagnostic delay.
In axApA, depression and other mental health disorders have been shown to be among the most prevalent of the comorbidities that occur (Garrido-Cumbrera et al., 2018). Other comorbidities include osteoporosis and cardiovascular morbidity (including conditions such as hypercholesterolaemia and hypertension). See Box 3 for differential diagnoses of axSpA. Differential diagnosis of axial spondyloarthropathy. Diffuse idiopathic skeletal hyperostosis Chronic (mechanical) lower back pain Fibromyalgia Psoriatic arthropathy Enteropathic arthropathy Rheumatoid arthritis
Psoriatic arthritis
Psoriatic arthropathy (PsA) is a chronic inflammatory arthritis that affects females and males equally. The condition can be seen at any age, though most commonly between the ages of 30 and 50 years, and is associated with multiple comorbidities including cardiovascular disease, metabolic syndrome, obesity, diabetes, uveitis and anxiety.
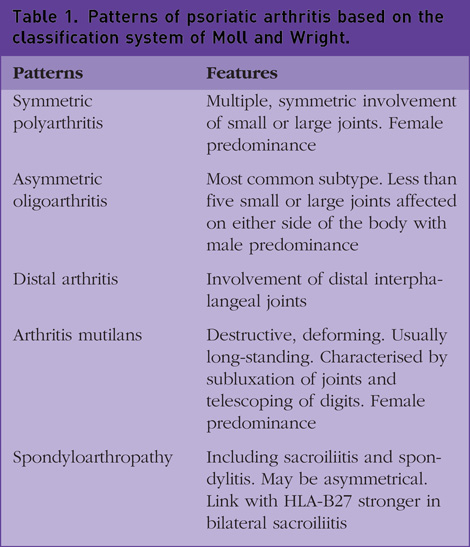
Estimates of the prevalence of PsA range from 6 to 42% of all psoriasis patients where the prevalence of psoriasis quoted is between 2 and 3% of the general population (Zachariae, 2003). It is a heterogeneous condition and can include any combination of nail and skin changes, peripheral arthritis, enthesitis, dactylitis and an axial spondyloarthritis. Moll and Wright (1973) divided PsA into five different patterns, as shown in Table 1. The severity of PsA can vary from a mild form to a very severe erosive arthropathy, known as arthritis mutilans. There is strong evidence that nail psoriasis is a predictor of psoriatic arthritis, and in fact, that a few years can elapse between the appearance of psoriatic nail changes and the onset of the symptoms of psoriatic arthritis (Raposo and Torres, 2015).
Patterns of psoriatic arthritis based on the classification system of Moll and Wright.
Axial PsA has a significant impact on quality-of-life measures and is associated with worse pain than that seen in patients without the axial involvement, as well as more severe skin manifestations and more significantly impaired physical function (Gottlieb and Merola, 2021). Patients with axial involvement also have decreased work productivity with significantly higher proportions of missed work time, overall work impairment and overall activity impairment. Problems with walking and self-care and feelings of anxiety and depression are also common.
The trigger for inflammation in PsA is unknown. There is some early evidence to suggest a role for environmental, genetic and immunological factors including the IL 23/IL-17 pathway.
PsA is a potentially erosive disease, with approximately 50% of patients exhibiting structural damage and functional impairment within 2 years of initial diagnosis (Gottlieband Merola, 2021). Many patients will ultimately experience irreversible joint damage and disability with disease progression making it vital that these patients should be identified as early in their disease course as possible; dermatologists play a crucial role in the early detection of patients with PsA.
A meta-analysis by Villani et al., 2015 suggested that between 10 and 15% of patients in dermatology outpatient clinics have undiagnosed PsA. Delay in diagnosis is associated with a poorer outcome. The National Institute for Health and Care Excellence (NICE) recommends that any patient who is on treatment for their psoriasis should be screened in primary care on an annual basis (NICE, 2013). Differential diagnoses include axial spondyloarthropathy, rheumatoid arthritis, osteoarthritis, gouty arthritis, connective tissue disease, septic arthritis, plantar fasciitis and inflammatory bowel disease (IBD)-related arthritis.
Juvenile idiopathic arthritis
The International League of Associations for Rheumatology has classified juvenile idiopathic arthritis (JIA) into seven heterogeneous subtypes (Petty et al., 2004). For further clarification, see Box 4. Classification of JIA.
50–60% of JIA cases Asymmetric, often large joints affected such as knee, ankle, wrist and elbow Female : male ratio 4:1 Antinuclear antibody (ANA) often positive. Strong association with anterior uveitis in 20%
> 4 affected joints within the first 6 months of illness 20–30% of JIA cases Painless uveitis especially if ANA positive Female : male ratio 4 : 1; onset in adolescence Often asymmetric involving multiple small and large joints
Symmetric, multiple small and large joints. Extra-articular rheumatoid nodules 5–10% of JIA cases Female : male ratio 9:1 Classically affects adolescent girls and is similar to rheumatoid arthritis with similar phenotypic and prognostic features
Arthritis and enthesitis. Asymmetric large joints of axial skeleton affected Symptomatic uveitis in 20%, enthesitis, IBD, aortitis 15% of JIA cases Male to female ratio 9:1 Males are often HLA-B27 positive
Presents as psoriasis and arthritis Asymmetric small and large joints including the hips and especially the distal interphalangeal joints 5–15% of JIA cases Female :male ratio 3:2 Nail changes also seen including dactylitis, pitting, ridging and onycholysis. Uveitis seen in 10%
Symmetric: multiple small and large joints affected Arthritis, rash, fever (‘Still’s disease’) May also present with lymphadenopathy and hepatosplenomegaly 10–20% of JIA cases Female : male ratio equal Can develop macrophage activation syndrome
Does not meet criteria for other JIA subtypes or meets criteria for two or more subtypes Arthritis
Disease onset is prior to 16 years of age with joint stiffness, swelling and/or pain being the underlying symptoms. One-in-six children affected by JIA suffer from anterior uveitis. Eye involvement occurs most commonly in girls with oligoarthritis and the subset of patients with a positive anti-nuclear antibody (Sen et al., 2015). The differential diagnosis includes juvenile rheumatoid arthritis (RA), rheumatic fever, osteomyelitis, septic arthritis, leukaemia, PsA and IBD-related arthritis.
Reactive arthritis
Reactive arthritis comprises a triad of urethritis, conjunctivitis and arthritis. It affects both sexes and occurs most commonly in young adults between 20 and 40 years of age. The disease process is triggered by an infection of the urogenital or gastrointestinal tracts resulting in an autoimmune response.
Typical pathogens affecting the gastrointestinal tract include Salmonella, Shigella, Yersinia, Campylobacter and Clostridium difficile. Pathogens affecting the genitourinary tract include Chlamydia pneumoniae and Chlamydia trachomitis, Escherichia coli, Ureaplasma urealyticum and Mycoplasma genitalium. Microorganisms cannot be cultured from joint samples, as the infection occurs elsewhere in the body and this fact distinguishes it from septic arthritis.
Reactive arthritis typically develops between 2 and 4 weeks after a gastrointestinal or a urogenital infection, and symptoms last around 4–6 months. Approximately one-in-four patients have recurrent episodes and one in ten will develop chronic disease. The arthritis is typically an acute, asymmetric oligoarthritis affecting five or fewer joints and predominantly involving the lower extremities. Pain and swelling of involved joints, including sacroiliitis, may occur.
The differential diagnosis for reactive arthritis includes radiographic and non-radiographic axSpA, PsA and enteropathic arthritis. Other differentials include septic arthritis, crystal arthritis, disseminated gonococcal infection, acute rheumatic fever, IBD, Behcet’s disease, coeliac disease, Whipple’s disease, parasitic infections and various viral infections.
Enteropathic arthritis
Inflammatory arthritis is the most common extra-intestinal manifestation in people with a diagnosis of IBD, with a prevalence of between 6 and 46% (Stolwijk et al., 2013), and is termed enteropathic arthritis. It can be peripheral, axial or both. Axial involvement tends to occur more often in patients who test positive for HLA-B27 and is more common in patients with Crohn’s disease than it is in those with ulcerative colitis (Gionchetti et al., 2015). The differential diagnoses include other spondyloarthropathies; Behcet’s syndrome can also masquerade as an enteropathic arthritis.
Clinical presentation and who to refer
The seronegative arthritides have several features in common, although each disease also has its own individual ‘signature’. Symptoms and signs seen in this patient group are listed below:
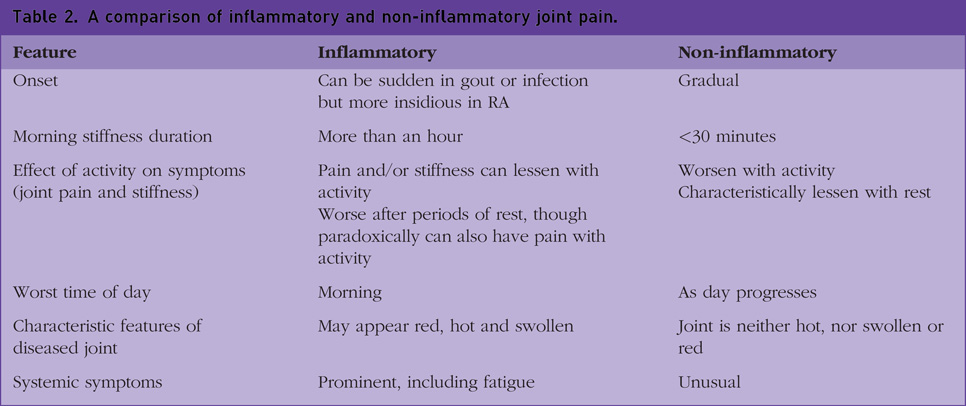
Inflammatory back and joint pain. The pain comes on gradually (i.e. subacute onset) and often awakens the patient during the second half of the night. It is characteristically at its worst in the early morning and is associated with joint stiffness, the latter lasting an hour or more. Pain and/or stiffness can lessen with activity and the pain may respond to treatment with anti-inflammatories. An affected joint may appear red, hot and swollen. Table 2 illustrates the differences between inflammatory and non-inflammatory joint pain Alternating buttock pain Dyspnoea, which can be related to apical lung fibrosis in ankylosing spondylitis, and reduced chest expansion Balanitis, erythema nodosum, keratoderma and pustulosis on palms and soles in reactive arthritis Extra-articular features including psoriasis, psoriatic nail changes, acute anterior uveitis, dactylitis, enthesitis and inflammatory bowel symptoms A comparison of inflammatory and non-inflammatory joint pain.
NICE clinical guidelines outline the circumstances when a patient warrants referral to rheumatology:
A history of low back pain which has lasted more than 3 months and which started prior to their 45th birthday with four or more of the following additional criteria: A history of low back pain with onset prior to their 35th birthday Awakening during the second half of the night as a consequence of their symptoms Buttock pain Pain eased by movement Non-steroidal anti-inflammatory drugs (NSAIDs) help with the pain and often within 48 hours of starting them History of axSpA in a first-degree relative Current or past enthesitis Current or past arthritis Current or past psoriasis If the patient would qualify for a referral but for the absence of one of the additional features, an HLA-B27 should be checked. Any patient with a positive HLA-B27 as well as three of the additional features warrants referral
In anyone in whom clinical suspicion remains, but they do not meet the referral criteria, advise them of any new signs, symptoms or risk factors which should prompt them to re-present to their GP or another healthcare professional; this would be particularly pertinent if the patient has a history of Crohn’s disease, ulcerative colitis, uveitis or psoriasis.
There is no consensus regarding the timeframe for referral of patients with a suspected seronegative inflammatory arthropathy, though an urgent referral would be recommended; the prefix ‘urgent’ is used under the heading ‘psoriatic arthritis and other peripheral spondyloarthritides’ (NICE, 2016).
Investigations
Diagnosis depends upon the clinical presentation plus laboratory and radiological investigations. There is no one investigation that, by itself, can definitively rule in or out the diagnosis of a seronegative arthritis.
Most radiological examinations will be requested by secondary care, as well as possibly some of the more specific blood tests such as anti-cyclic citrullinated peptide , rheumatoid factor (RF) and HLA-B27. It is likely, however, that when the patient initially presents to primary care the GP may wish to undertake some blood tests such as a full blood count, renal function and inflammatory markers like C-reactive protein and erythrocyte sedimentation rate.
Radiological examinations can be very helpful. Peripheral joints, for example, can be imaged with X-ray and ultrasound. Many rheumatologists would opt for an MRI pelvis plus/minus spine as the initial radiographic investigation of choice for all patients with a suspected axial spondyloarthropathy in order to limit radiation exposure and pick up any radiological changes earlier in the patient’s journey. MRI imaging, however, would not ordinarily be something that would be requested in a primary care setting.
Any patient presenting with a history of an acute red eye on a background of a seronegative arthritis, especially where this sounds suspicious of anterior uveitis, warrants an urgent referral to ophthalmology. These patients should undergo a slit lamp examination plus a measurement of their intra-ocular pressures.
Management
The primary treatment goal is to optimise the patient’s health-related quality of life. This will require a combination of the following approaches:
Alleviation of symptoms Prevention of further structural damage due to the underlying disease processes Return to as normal a level of social functioning as possible
The current recommendations from the European League Against Rheumatism (Zangi et al., 2015) are that all rheumatology patients should be actively included in discussions about management of their disease; rheumatology specialist nurses should play a significant role in this process (Bech et al., 2019). All patients should be referred to a specialist physiotherapist for a structured exercise programme and some patients benefit from occupational therapy input.
In terms of pharmacological therapies, NSAIDs are used first line in all of the spondyloarthropathies (NICE, 2016). If no response to a full dose of an NSAID is seen within a 2-week period, then a switch to an NSAID of a different class may be warranted. If the patient is unable to tolerate NSAID treatment or the response is poor, DMARDs (disease-modifying anti-rheumatic drugs) are considered. There are three different categories of DMARD, namely the conventional synthetic DMARDs (or csDMARDs), the biological DMARDs (or bDMARDs) and the targeted synthetic DMARDs (tsDMARDs).
The csDMARDs, which includes methotrexate and leflunomide, are used in the treatment of the peripheral spondyloarthropathies and the bDMARDs, such as the TNF alpha inhibitors and the Il-17 inhibitors, are used for patients with axial disease. The tsDMARDs, such as upadacitinib, are the Janus kinase inhibitors which have garnered increasing attention recently; their use is expanding rapidly and they have the advantage of oral administration. In September 2022, NICE recommended upadacitinib for treating AS in adults who are unable to tolerate the TNF alpha inhibitors or where these molecules do not adequately control the underlying disease (NICE, 2022).
It is important to remember that patients taking DMARDs are at increased risk of serious infection, which can be an important consideration when seeing these patients in the primary care setting.
Key points
The seronegative arthritides are systemic inflammatory diseases characterised by joint pain and inflammation largely without the presence of autoantibodies such as RF and anti-CCP
The spondyloarthropathies are characterised by articular (axial/peripheral) and extra-articular features
Extra-articular features can include fatigue, anaemia, ocular disease, aortic regurgitation, first to third degree heart block and amyloidosis
Management requires a multi-disciplinary approach with occupational therapy, physiotherapy, rheumatology specialists, pain specialists, psychologists and the patient’s GP
Shared decision making between the patient and clinician is an overarching theme, which should play a central role in the management of the seronegative arthritides
NICE recommends NSAIDs first line followed by DMARDs if the patient does not respond to two or more NSAIDs, or is intolerant of treatment with NSAIDs